
Abstract
The main objective of this study was the preparation and evaluation of the primary reagents for the liquid phase human chorionic gonadotropin-radioimmunoassay (HCG-RIA) kit. Polyclonal antibody is specific and valid; monoclonal antibodies are more specific. In HCG-RIA technique, polyclonal antibodies for βHCG subunits with high binding and displacement % were used. 125I-HCG radioactive tracer was prepared with high yield 71.58 ± 0.92%, purity 99.2 ± 0.05%, and specific activity 170.42 ± 1.65 µCi/µg using chloramine T method, βHCG polyclonal antisera and HCG standards in assay buffer matrix were locally prepared. In-house HCG-RIA was developed with high sensitivity 0.5 mIU/ml, specificity (99%), precision (CV% < 6.4 and < 8.3 for intra-and inter-assay, respectively), and accuracy (recovery range 96.4–104.3%) could be used for quantitative estimation of HCG in human sera for monitoring pregnancy and diagnosis of gestational trophoblastic diseases.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The earliest documented pregnancy hormonal signal is human chorionic gonadotropin (HCG). The blastocyst (fertilized egg) start to produce HCG before implantation, then the syncytiotrophoblast generate HCG exponentially after blastocyst implantation [1]. Blood HCG levels are detectable at considerable levels ten days after conception. Between weeks 10 and 11, the placenta generates the most HCG, and then the rate of production drops until week 12 when it stabilizes. HCG facilitates the corpus luteum's rescue and maintains progesterone production [2, 3].
HCG levels are elevated in all cases of gestational trophoblastic diseases (GTDs), making it an ideal tumor marker. GTDs are pregnancy disorders including a spectrum of diseases, ranging from the potentially premalignant hydatidiform mole to the highly aggressive choriocarcinoma. HCG is produced by all trophoblastic tumors, and monitoring of therapy is largely based on the determination of HCG in serum [4].
Total HCG in GTDs is the best example of a tumor marker because it has about 100% sensitivity and specificity for trophoblast malignant tissues. The amount of hydatidiform mole or tumor tissue is directly proportional to the blood level of total HCG. Hyperglycosylated HCG is a definitive tumor marker of invasion and malignancy in invasive moles and choriocarcinomas [4, 5]. High concentrations of HCG variants have been detected in human tumors that do not develop from trophoblastic tissue, including testicular, ovarian, bladder, kidney, lung, breast, and gynecological cancers [6]. These findings imply that HCG variants play a significant role in almost all human malignancies, and the production of specific antibodies against them can be exploited in cancer therapy [7].
The problem with automated laboratory HCG tests using an antibody to βHCG C-terminal peptide as the capture or tracer antibodies is that, it prevents detection of circulating HCG variants lack C-terminal peptide epitope. Using these antibodies severely restrict the specificity of the HCG assays [8]. To measure all HCG variants, the HCG-RIA only requires one polyclonal antibody to core β-subunit-1 or β-subunit-2. The GTDs Centre in the UK continues to monitor patients receiving treatment for GTDs using an in-house radioimmunoassay of this kind [9]. HCG-RIA has the advantage of detecting the major forms of HCG both in serum (i.e., HCG and βHCG) and in urine (HCG, HCGβ, and HCGβcf) in a fairly equimolar fashion [10].
In this study, purified HCG was optimized for labeling with radioactive iodine-125 to produce 125I-HCG tracer with high purity and specific activity, then used to prepare HCG standard solutions. All these reagents along with polyclonal β HCG antibodies can be used to develop a sensitive, precise, and accurate method for HCG estimation as a useful tool for pregnancy monitoring and diagnosis of GTDs.
Experimental
All the chemical reagents are of analytical grade. Chorionic gonadotropin human: C1063; Chorionic Gonadotropin, Human Urine, Standard Grade: 230734; Bovine serum, adult: B9433; Bovine Serum Albumin (BSA): A7888; Freund’s adjuvant complete (FAC): F-5881; Freund’s adjuvant incomplete (FAI): F-5506; polyethylene glycol 8000 (PEG): P4463; chloramine-T: C9887; sodium metabisulphite: S1516; potassium iodide: P2963; Sephadex G-25: G2580; sodium azide: S2002, were purchased from Sigma Chemical Co. USA of high quality and purity; sodium iodide –125 (125I Na) radioactive concentration 3700 MBq/ml was purchased from Izotop, Hungary. Microprotein determination kit: AGAPPE diagnostic, Switzerland GmbH. HCG Kit: AIA-PACK kit, TOSOH, Japan.
Preparation of HCG
HCG; was purified in our labs from pooled urine of pregnant women at the 10th week of gestation with high purity of 98.2% and biological activity (10,811 IU/mg) using alcohol precipitation, anion exchange, and gel chromatography according to our recently published method [11]. Polyclonal βHCG antisera; were produced from rabbits with high titer (1/104) and displacement (84.8%) using purified βHCG subunits according to our recently published method [11].
Preparation of 125I- HCG tracer
The immunologically active HCG molecule is composed of 237 amino acids containing seven tyrosine residues that can be radiolabeled using the optimized chloramine-T technique [12]. The labeling reaction was optimized by investigating some effects such as pH, Chloramine-T content, substrate (HCG) content, and the reaction time. The iodination reactions were carried out in the following sequence (in polystyrene eppendorf tube, 10 µl 0.25 M phosphate buffer pH 7.4, 10 µl HCG containing 2.0 µg (w/v), 10 µl Na125I (500 µCi), the reaction started by adding 5 µl chloramine- T solution containing 25 µg (w/v), then mixed by gentle vortexing for one minute, and the reaction was quenched by adding 6 µl sodium metabisulfite containing 30 µg (w/v), and 10 µl potassium iodide was added as a carrier) [13], then 3 µl was taken from the reaction mixture, and then applied on paper chromatography[14], and placed vertically in saturated jar contain 1 ml 70% methanol as a mobile phase. After approximately one hour, the mobile phase had reached the end line, the paper was allowed to air dry and spliced into 1 cm fractions, which were counted as (CPM) using a gamma counter. The iodination yield was calculated by measuring the radioactivity of all the fragments, dividing the radioactivity (CPM) at the spotting site (radiolabelled protein peak) by the total radioactivity (CPM) on the whole paper (the first peak and the second free iodide peak), and multiplying by 100.
Factors affecting the iodination of HCG
-
a.
Effect of pH The pH value of the labeling reaction was optimized by studying the effect of different pH values (5.5, 6.5, 7.5, 8.5, and 9.5) of 0.25 M phosphate buffer, while all other parameters remained constant. After that, the iodination yield was calculated for each pH value.
-
b.
Effect of Chloramine T content The chloramine-T content and molar ratio of Chloramine-T to HCG content was optimized by studying the effect of different chloramine-T concentrations (10, 25, 50, 75, and 100 µg), while all other parameters remained constant. Then, the iodination yield was calculated for each oxidizing agent concentration.
-
c.
Effect of Substrate (HCG) content The optimum substrate (HCG) concentration was determined by studying the effect of different HCG concentrations (0.5, 1.0, 2.0, 4.0, and 8.0 µg), all other parameters were held constant. Then the iodination yield was calculated for each substrate concentration.
-
d.
Effect of Reaction Time The reaction time of labeling was optimized by repeating the labeling reaction at different times (15, 30, 60, 120, and 300 s), while all other reaction parameters remained fixed, and the iodination yield was calculated for each reaction time.
Purification of the radio-iodinated 125I-HCG tracer
Following labeling reaction optimization, the reaction was carried out at these optimum conditions, and the reaction mixture was immediately applied to a Sephadex-G25 column pre-equilibrated with assay buffer (0.05 M phosphate buffer pH 7.4 containing 0.4% BSA, 0.9% sodium chloride and 0.1% sodium azide) [15]. 0.5 ml fractions were collected at a flow rate of 0.5 ml/min and counted in units of a micro curie (μCi) by using a dose calibrator. In general protein peak is used for the specific activity check, relevance of second peak analysis.
Characterization of the tracer
The prepared 125I-HCG tracer was characterized in terms of radioiodination yield, radiochemical purity, specific activity (µCi/µg), immunoreactivity, and stability.
-
(a)
Radioiodination yield (%)
Following purification of 125I-HCG tracer on a Sephadex-G25 column, radioiodination yield was calculated as a percent of activity (µCi) of labeled HCG (125I-HCG) fractions to the total radioactivity (µCi) of all fractions (125I-HCG + free iodide), multiplied by 100.
-
(b)
Radiochemical purity (%)
The radiochemical purity of the purified 125I-HCG tracer was tested by the paper chromatography method using 70% methanol as a mobile phase. Then, the 1 cm fragments were counted using a gamma counter in units of (CPM). Radiochemical purity was measured as a percent of radioactivity (CPM) of labeled HCG (125I-HCG) to the total radioactivity counted.
-
(c)
Immunoreactivity
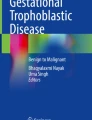
Immunoreactivity of the prepared 125I-HCG tracer was tested in terms of maximum binding (B0%) and nonspecific binding (NSB %) at different dilutions of anti βHCG antisera.
-
(d)
Specific activity
The specific activity of the 125I-HCG tracer, the radioactive iodine content per unit mass of substrate (HCG) was measured by multiplying the radioiodination yield (%) by the total activity(µCi) added in the labeling reaction, and dividing the result by the concentration(µg) of the substrate (HCG) added in the reaction mixture [16]. The specific activity of the prepared 125I-HCG tracer was expressed in units of (µCi /µg).
$$\begin{aligned} {\text{Specific}}{\mkern 1mu} {\text{activity}} = & \left( \begin{gathered} {\text{Radioiodination}}{\mkern 1mu} {\text{yield}}\left( \% \right) \hfill \\ \times {\text{Total}}{\mkern 1mu} {\text{Activity}}{\mkern 1mu} {\text{added}}\left( {\mu Ci} \right) \hfill \\ \end{gathered} \right) \\ & \frac{1}{{{\text{Concentration}}{\mkern 1mu} {\text{of}}{\mkern 1mu} {\text{HCG}}\left( {\mu g} \right)}} \\ \end{aligned}$$(2) -
(e)
Tracer stability
The stability of the prepared 125I-HCG tracer was studied under different conditions (diluted and undiluted), both at different temperatures (− 20 °C, 4 °C and 25 °C). Stability was estimated by measuring the maximum binding (%B0) and non-specific binding (%NSB) through three months of storage period [17].
Preparation of HCG standard solutions
HCG standard grade (3rd IS 75/537) as a lyophilized powder from sigma Aldrich company (2500 IU/vial) was dissolved in 1250 μl of double distilled water containing 0.1% sodium azide and divided into aliquots stored at–20 ºC. The stock HCG solution was estimated in duplicate by commercial EIA (AIA360 automated enzyme immunoassay TOSOH), and the net concentration of stock HCG solution was measured to be 2000 IU/ml. Two sets of standard solutions of HCG were prepared, the first set of standard HCG was prepared in HCG-free bovine serum matrix and the second one was prepared in assay buffer matrix. HCG solution with concentration 4000 mIU/ml was prepared by diluting 2 μl of stock solution with 998 μl of diluting matrix [18]. Furthermore, concentrations (1, 5, 25, 50, 100, 250, 500, 1000, and 2000 mIU/ml) were prepared [19], HCG standards that prepared in both HCG free bovine serum matrix and assay buffer matrix were tested for binding with βHCG specific antisera, then stored refrigerated at 4 ºC or frozen for long time storage at -20 till use.
HCG-RIA optimization
The parameters of the radioimmunoassay system such as incubation time, temperature, sample volume, dilution of βHCG antisera, reaction volume, and separating agents (secondary antibody, non-immunized rabbit serum and PEG 8000), have been optimized by keeping all the parameters constant and focusing the study on each one of them, temperature (4, 25, and 37 °C), incubation time (1, 2, 3, 6, 12 h), sample volume (50,100,200, and 300 µl), reaction volume (300,500 and 1000 µl), secondary antibody (from 1:10 to 1:100), normal rabbit serum (1:100,1:200, 1:300, and 1:400), and PEG 8000 (4, 8, 12%). The optimum parameter is that with the highest binding and displacement percentages were measured.
Assay design
Following optimization, the HCG-RIA was formulated as follows: in a polystyrene test tube, add 100 µl sample or standard, 100 µl βHCG polyclonal antibodies at a dilution of 1:10,000, and 100 µl radiolabeled 125IHCG tracer at a radioactivity count of approximately 20,000 CPM/100 µl. After gentle vortexing and incubation for three hours at room temperature (25 °C), the following separating agents were added: 100 µl secondary antibody at dilution 1:50, 100 µl NRS (non-immunized rabbit serum) at dilution 1:100, and 500 µl PEG 8000 at concentration 6%. Again, gently vortex the tubes, incubate at RT (25 °C) for 30 min, and centrifuged at 4 °C, 5000 rpm for 15 min, the supernatant was discarded by decantation, the tubes were kept in the inverted position on a blotting paper/ tissue, and the tubes were counted for radioactivity as CPM using a gamma counter.
Calculation of the assay output results
After measuring, the total activity that was added to each tube and the bounded activity that counted after decantation. The data of the radioimmunoassay were represented as maximum binding (B0) for zero standard tubes, and known standard binding (Bs).
Standard curve representation
The standard curve for HCG-RIA was represented by plotting the %B/B0 for each HCG standard value (1, 5, 25, 50, 100, 250, 500, 1000, and 2000 mIU/ml) versus the concentration of individual HCG standards [20].
Validation study of HCG–RIA
Radioimmunoassay validation was achieved by measuring some quality control parameters, such as assay sensitivity, cross-reactivity with related glycoproteins FSH, LH, and TSH, intra-assay and inter-assay precision, and accuracy (recovery and dilution), and finally method comparison with a commercial kit.
Statistical methods
CVs and SD were calculated within and between runs as described by Krouwer and Rabinowitz 1984 [21]. The slope of the calibration curve was calculated after the logit-log transformation of % B/B0 as described by Rodbard 1974 [20].
Results and discussion
Optimization of the iodination reaction
HCG was labeled with iodine-125 using the optimized Chloramine T-method, at chloramine T concentration (25 μg), pH (7.5) of 0.25 M phosphate buffer, HCG content (2.0 μg), and reaction time (60 Sec.) the iodination yield obtained was 71.58 ± 0.92% as shown in Fig. 1 and the specific activity was 170.42 ± 1.65 µCi/µg. The purity of the prepared tracer was measured by paper chromatography method, and the radiochemical purity of the tracer calculated to be 99.2 ± 0.05% as shown in Fig. 2.

Radiochemical yield of 125I-HCG. The mixture of the HCG iodination reaction was applied on sephadex G-25 column, eluted with 0.25 M phosphate buffer pH 7.4 and 0.5 ml fractions were collected at flow rate 0.5 ml/min. The radioactivity in the fractions were counted as (µCi) by dose calibrator instrument

Radiochemical purity of 125I-HCG. 3 µl from the fraction no. 7 containing the radiolabelled HCG tracer was applied on paper chromatography, eluted with 70% methanol and the the 1 cm paper fragments were counted as (CPM) using the gamma counter
Characterization of the prepared 125I- HCG tracer
-
-
Radiochemical yield When the tracer was purified by gel filtration technique using a Sephadex-G25 column (PD-10), the radioactivity of the first peak represented 71.6% of the iodination process, as shown in Fig. 1.
-
-
Radiochemical purity When the tracer was analyzed by paper chromatography technique, the results represented in Fig. 2 showed that the purity of the prepared radio-iodinated HCG tracer is 99.2 ± 0.05%.
-
-
Specific activity The radioactivity content per mass unit of labeled HCG tracer was measured to be (170.42 ± 1.65 µCi/µg), indicating that; the prepared tracer with high specific activity can be used in RIA with a sharp radioactive signal that enhances assay sensitivity.
-
-
Immunoreactivity The immunoreactivity of the prepared HCG tracer was estimated by examining its binding with the specific anti βHCG polyclonal antisera. Figure 3 shows that the tracer prepared using the chloramine-T method had a high maximum binding percent (%B0 = 84.7%), a high displacement percent (D% = 84.8%), and a very low nonspecific binding percent (%NSB = 2.1%). These results indicate that the prepared tracer is immunologically active and had very specific antibody binding.
Fig. 3 
Immunoreactivity check for the prepared 125I-HCG tracers
-
-
Tracer stability The results of tracer stability studies conducted over two months storage period at different temperatures under diluting and undiluted conditions showed that, the tracer is more stable when stored as a diluted solution in assay buffer matrix at − 20 °C over two months.

As shown in Table 1; the HCG tracer was partially deteriorated when stored undiluted at 4 °C and completely deteriorated when stored for two months at 25°C. On the other hand, when the tracer was preserved at − 20 °C, the binding of the tracer with antibody kept high while the nonspecific binding remained low through the storage period.
Preparation of HCG standards
Two types of standards were prepared: The first in an assay buffer matrix, and the second in a bovine serum matrix.
Both standard sets were used in constructing standard curves for HCG-RIA, and the results shown in Fig. 4 demonstrated that the binding of antigen and antibody was greater when assay buffer was used as a matrix than bovine serum matrix.

Comparative study between the locally prepared HCG standards in assay buffer and HCG free bovine serum matrix
From the obtained results in Fig. 4, high binding was observed when assay buffer was used as a matrix for standard HCG preparation. The prepared HCG standard solutions in assay buffer matrix were selected and characterized by measuring each individual standard with commercial (HCG kit, TOSOH). The results of indigenous and commercial HCG standards were statistically analyzed for linear fit as shown in Fig. 5, the result of the correlation coefficient’r’ = 0.999 revealed a strong positive correlation between them.

Linear regression equation and correlation coefficient “r” between indigenous HCGstandards RIA and commercial HCG standard TOSOH
HCG-RIA optimization
The optimization results per each HCG-RIA parameter are listed below: The optimal reaction time was 3 h, and the binding and displacement percentages were 44.9 and 81.5%, respectively. The optimum temperature for HCG-RIA was 25 °C, with binding and displacement percentages of 44.2 and 80.1%, respectively. The optimal sample volume for HCG-RIA was 100 µl, with binding and displacement percentages of 45.0 and 82.4%, respectively. The optimal tracer radioactivity concentration for HCG-RIA was 20 × 103 CPM, with binding and displacement percentages of 41.3 and 79.6%, respectively. The optimal dilution for the goat anti rabbit secondary antibody in the HCG-RIA separation technique was 1:50, with binding and displacement of 50.6% and 84.2%, respectively. In non-immunized rabbit serum, a dilution of 1:100 produced the best results for HCG-RIA. The recommended PEG-8000 content for HCG-RIA was 6%, with binding and displacement percentages of 58.7% and 78.6%, respectively. Additionally, 300 µl of the HCG-RIA reaction volume yielded the greatest outcomes, with binding and displacement percentages of 43.0 and 79.6%, respectively.
Standard curve for HCG-RIA
The values of % B/B0 for each HCG standard were plotted against the concentration of HCG standards on a logit-log sheet. Figure 6 shows a linear inversed line, implying that as the concentration of HCG increases, the binding of radioactive HCG-tracer with the βHCG antibody decreases, and consequently the radioactive count decrease; from this curve, any unknown sample can be measured. The HCG-RIA range of measures (1, 5, 25, 50, 100, 250, 500, 1000, and 2000 mIU/ml) developed in-house was broad and can detect native HCG in samples up to 2000 mIU/ml.

Standard curve of HCG-RIA
HCG-RIA validation
According to Andreasson et al. 2015 [22], the results obtained from locally prepared HCG-RIA were validated by measuring the following statistical parameters:
Sensitivity, the lowest concentration of analyte (HCG) that has been demonstrated to be measurable with acceptable levels of precision and accuracy and can be distinguished statistically from zero standards [23], a detection limit of 0.5 mIU/ml was obtained by assaying 20 replicates of zero standards (Table 2) and the binding % B/B0 at 95% probability of true results by the assembly on HCG-RIA standard curve [24], the sensitivity obtained was excellent when compared with the commercial ELISA and EIA kits.
Specificity, the ability of the antibody to recognize an antigen even when the antigen is measured in a medium of similar substances that may be expected to be present [22]. The specificity was tested according to the method of Abraham [25], also called the 50% inhibition method, where specificity was calculated by dividing the concentration of HCG by the concentration of cross-reactant at % B/B0 equal to 50% to HCG standards, and the obtained specificity was 98.8% [11], indicating that the locally prepared polyclonal anti-βHCG specifically binds to HCG and has no cross-reactivity with related glycoproteins.
Precision is the degree to which separate test findings acquired under predetermined conditions accord closely [22]. Three pooled samples of human serum were used to calculate the mean of 10 duplicates in order to estimate the intra-assay (Within-Run) precision for HCG. The three levels of pooled human serum samples had coefficients of variation (% CVs) of 6.3, 6.4, and 5.7%. The statistical analyses were calculated for each sample and the % CVs were 8.3, 7.1, and 7.4% as shown in Table 3. The inter-assay (Run to Run) precision for HCG was derived from the mean of the average of duplicates from 10 independent runs with the same three pooled human sera. The % CV of the intra-assay (within assay variation) should be less than 10%, according to Pillai and Bhandarkar 1998 [26] and El-Kolaly et al. 2001[27], and the % CV of the measured ligand concentration in the case of the inter-assay (between assay variations) should be less than 15% [28]. Collectively the results show that the developed HCG RIA is with acceptable precision.
Accuracy, the degree of agreement between the measured and true values; in this study, the assay accuracy was evaluated using recovery and dilution tests (parallelism).
Recovery test This test compares the concentrations of three samples of human serum from various diagnostic states before and after the addition of a known quantity of HCG. The current study's HCG-RIA recovery test results varied from 96.4 to 104.3%, as reported in Table 4.
Dilution test The linearity of the assay was evaluated using the HCG content in three pooled human serum samples at varying dilutions. The outcomes demonstrated that the current study's method for HCG retained good linearity under dilution. The findings of the dilution test, which are displayed in Table 5, ranged from 91.1 to 107.6%. The recovery statistics from the current investigation for HCG are well-concordant with those reported by Pillai and Bhandarkar in 1998 [26] and Mehany et al. in 2007[29], who stated that the recovery in the RIA method should be 100 ± 15%.
Comparison with reference method
The results of the statistical analysis of the linear correlation between the HCG levels of 50 serum samples measured commercially using the TOSOH immunoassay analyzer and the developed RIA system show that there is a strong linear positive correlation (r = 0.998) between the locally developed HCG-RIA technique and the commercial EIA technique, as shown in Fig. 7.

Linear correlation between results obtained by HCG-RIA method and EIA method
Conclusions
In this research article, purified HCG was radiolabelled with iodine-125 under optimal conditions; 125I-HCG tracer with high yield (71.58 ± 0.92%), high purity (99.2 ± 0.05%), and high specific activity (170.42 ± 1.65 µCi/µg) was obtained. Standard solutions for HCG were prepared and characterized. All HCG-RIA parameters were optimized, formulated, and then characterized by validity testing. The high sensitivity 0.5 mIU/ml of the developed HCG-RIA enables the detection of very low concentrations of HCG in human serum, and the obtained standard curve covers a wide range of detection up to 2000 mIU/ml, the precision and accuracy study revealed a low % CV. The problem of underestimation of HCG measured by automated HCG assays that use monoclonal antibodies for βHCG-CTP could be solved by using polyclonal βHCG antisera along with prepared 125I-HCG tracer and HCG standard solutions in the developed HCG-RIA system. Based on the above study a system can be developed for the estimation of the recently discovered hyperglycosylated-HCG isoform, an invasive molecule which may have a role in spontaneous abortion of pregnancy and the development of several types of human cancers.
References
Jurisicova A, Antenos M, Kapasi K, Meriano J, Casper RF (1999) Variability in the expression of trophectodermal markers beta-human chorionic gonadotrophin, human leukocyte antigen-G and pregnancy specific beta-1 glycoprotein by the human blastocyst. Human Reprod (Oxford, England) 14(7):1852–1858. https://doi.org/10.1093/humrep/14.7.1852
Shikone T, Yamoto M, Kokawa K, Yamashita K, Nishimori K, Nakano R (1996) Apoptosis of human corpora lutea during cyclic luteal regression and early pregnancy. J Clin Endocrinol Metab 81(6):2376–2380. https://doi.org/10.1210/jcem.81.6.8964880
Makrigiannakis A, Vrekoussis T, Zoumakis E, Kalantaridou SN, Jeschke U (2017) The role of HCG in implantation: a mini-review of molecular and clinical evidence. Int J Mol Sci 18(6):1305. https://doi.org/10.3390/ijms18061305
Sisinni L, Landriscina M (2015) The role of human chorionic gonadotropin as tumor marker: biochemical and clinical aspects. Adv Exp Med Biol 867:159–176. https://doi.org/10.1007/978-94-017-7215-0_11
Cole LA, Butler S (2012) Hyperglycosylated hCG, hCGβ and Hyperglycosylated hCGβ: interchangeable cancer promoters. Mol Cell Endocrinol 349(2):232–238. https://doi.org/10.1016/j.mce.2011.10.029
Cole LA (2012) HCG variants, the growth factors which drive human malignancies. Am J Cancer Res 2(1):22–35
Cole LA (2012) hCG, the wonder of today’s science. Reprod Biol Endocrinol 10(1):24. https://doi.org/10.1186/1477-7827-10-24
Cole LA (2015) 29-antibodies and hCG tests. In: Cole LA, Butler SA (eds) Human chorionic gonadotropin (HGC), 2nd edn. Elsevier, San Diego, pp 313–321. https://doi.org/10.1016/B978-0-12-800749-5.00029-8
Cole LA (2015) 30-problems with today’s hCG pregnancy tests. In: Cole LA, Butler SA (eds) Human chorionic gonadotropin (HGC), 2nd edn. Elsevier, San Diego, pp 323–334. https://doi.org/10.1016/B978-0-12-800749-5.00030-4
Harvey RA, Mitchell HD, Stenman UH, Blankenstein MA, Nustad K, Stieber P, Stewart W, Savage PM, Seckl MJ, Braunstein GD (2010) Differences in total human chorionic gonadotropin immunoassay analytical specificity and ability to measure human chorionic gonadotropin in gestational trophoblastic disease and germ cell tumors. J Reprod Med 55(7–8):285–295
Elsheikh HM, Hamdy GM, Ebeid NH, Sallam KM, El-Bayoumy ASA, Mehany NL, Fathy SA (2021) Effective purification of human chorionic gonadotropin and production of highly specific polyclonal anti-βHCG as a component of radioimmunoassay kit. J Immunoass Immunochem 43(3):233–249. https://doi.org/10.1080/15321819.2021.1993896
Bolton A, Hunter W (1973) The labelling of proteins to high specific radioactivities by conjugation to a 125I-containing acylating agent. Appl Radioimmunoass Biochem J 133(3):529–538
Law B (1996) Radiolabelling procedures for radioimmunoassay. In: Immunoassay. CRC Press, pp 72–105
Law B (2002) Immunoassay: a practical guide. Taylor & Francis, London
Abu-Bakr El-Bayoumy AS, Hessien Keshta AT, Sallam KM, Ebeid NH, Elsheikh HM, Bayoumy BE-S (2018) Extraction, purification of prostate-specific antigen (PSA), and establishment of radioimmunoassay system as a diagnostic tool for prostate disorders. J Immunoass Immunochem 39(1):12–29. https://doi.org/10.1080/15321819.2017.1392320
Morris BJ (1976) Specific radioactivity of radioimmunoassay tracer determined by self-displacement: a re-evaluation. Clin Chim Acta 73(1):213–216. https://doi.org/10.1016/0009-8981(76)90328-4
Ballard P, Stafford LE, Law B (1996) The development and performance of a radioimmunoassay for the analysis of ZM 213,689, the major metabolite of meropenem—a carbapenem antibiotic—in plasma and urine. J Pharm Biomed Anal 14(4):409–417. https://doi.org/10.1016/0731-7085(95)01656-2
Ballard P, Malone MD, Law B (1994) The use of competitive displacement agents to resolve albumin binding problems observed during the development of a radioimmunoassay for ICI 215001. J Pharm Biomed Anal 12(1):47–52
Stenman U-H (2004) Standardization of assays for human chorionic gonadotropin. Clin Chem 50:798–800. https://doi.org/10.1373/clinchem.2003.031013
Rodbard D (1974) Statistical quality control and routine data processing for radioimmunoassays and immunoradiometric assays. Clin Chem 20(10):1255–1270
Krouwer J, Rabinowitz R (1984) How to improve estimates of imprecision. Clin Chem 30(2):290–292
Andreasson U, Perret-Liaudet A, van Doorn Waalwijk L, Blennow K, Chiasserini D, Engelborghs S, Fladby T, Genc S, Kruse N, Kuiperij H, Kulic L, Lewczuk P, Mollenhauer B, Parnetti L, Vanmechelen E, Verbeek M, Winblad B, Zetterberg H, Teunissen C (2015) A practical guide to immunoassay method validation. Front Neurol 6:179. https://doi.org/10.3389/fneur.2015.00179
Lee JW, Devanarayan V, Barrett YC, Weiner R, Allinson J, Fountain S, Keller S, Weinryb I, Green M, Duan L, Rogers JA, Millham R, O’Brien PJ, Sailstad J, Khan M, Ray C, Wagner JA (2006) Fit-for-purpose method development and validation for successful biomarker measurement. Pharm Res 23(2):312–328. https://doi.org/10.1007/s11095-005-9045-3
Rodbard D (1978) Statistical estimation of the minimal detectable concentration (sensitivity) for radioligand assays. Anal Biochem 90(1):1–12
Abraham GE (1976) Radioimmunoassay of steroids in biological fluids. In: Proceedings of the fourth international congress on hormonal steroids. Elsevier, pp 261–270
Pillai M, Bhandarkar S (1998) Radioimmunoassay. Principles and practice head, isotope division, baba atomic research centre, Trombay, Mumbai Thane, India: Devi Printers and Binders
Elkolaly MT, Mehany NL, Ragab MT, El-Mohty AA (2001) Studies on local preparation of double antibody radioimmunoassay for determination of alpha fetoprotein as a tumor marker. Arab J Nucl Sci Appl 34(2):105–116
Shah VP, Midha KK, Dighe S, McGilveray IJ, Skelly JP, Yacobi A, Layloff T, Viswanathan C, Cook CE, McDowall R (1992) Analytical methods validation: bioavailability, bioequivalence, and pharmacokinetic studies. J Pharm Sci 81(3):309–312
Mehany N, El-Kolaly M, Sallam KM, EI-Hashash M (2007) Liquid phase radioimmunoassay system for determination of progesterone in human serum using different radiolabeled tracers. Arab J Nucl Sci Appl 40(1):300–311
Funding
Open access funding provided by The Science, Technology & Innovation Funding Authority (STDF) in cooperation with The Egyptian Knowledge Bank (EKB).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Elsheikh, H.M., Fathy, S.AH., Ebeid, N.H. et al. Development of radioimmunoassay system for determination of human chorionic gonadotropin in human sera. J Radioanal Nucl Chem 332, 581–590 (2023). https://doi.org/10.1007/s10967-023-08797-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10967-023-08797-5