
Abstract
This research was carried out to identify the relationship between the spiritual well-being and caregiver burden in caregivers of patients with breast cancer. The study was conducted with family caregivers of patients with breast cancer who presented to the oncology clinic of a university hospital for treatment. The study sample included a total of 138 family caregivers who met the criteria for participation and agreed to participate in the study. The data were collected using a participant information form, caregiver burden scale and three-dimensional spiritual well-being scale. The caregivers have a moderate level of caregiver burden and their spiritual well-being was quite high. The caregiver burden of female caregivers was found to be significantly higher than that of male caregivers (p = 0.040). There is a negatively significant relationship between caregiver burden and spiritual well-being (p = 0.000, r = − 0.357). The caregiver burden is significantly higher among the 24-h caregivers compared to that among the 3-h and 4–6-h caregivers (p = 0.003). The spiritual well-being of the caregivers who provide care between 3 h and 4–6 h a day was significantly higher than that of those who provide 24-h care (p = 0.001). Increasing spiritual well-being may help to reduce caregiver burden in caregivers of those with breast cancer.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Breast cancer in women is one of the most common cancers all over the world. With 2,261,419 new cases in 2020, the incidence rate of breast cancer is 11.7% (World Health Organization, 2020). Breast cancer can be treated using methods such as surgery, chemotherapy, radiotherapy and immunotherapy. The side effects of these treatments increase the care needs of patients (Baider, 2014). Caring for a patient with breast cancer can often strain family caregivers psychologically, socially and financially, leading to negative consequences called caregiver burden (CB). CB is defined as ‘‘a multidimensional response to the physical, psychological, social and financial stress factors associated with the caregiving experience’’ (Zarit et al., 1980).
Breast cancer patients are now treated on an outpatient basis without the need for hospitalisation. Care needs are often provided by voluntary family caregivers (Schulz et al, 2020). Caregivers help patients with their daily work, provide medication and manage symptoms (Sun et al, 2019). In this process, caregivers' CB and needs are often unnoticed, and the treatment process is often shaped by the needs of the patient (care recipient) (Jite et al., 2021). Caregivers often receive neither adequate education nor social support (Adelman et al., 2014). Studies on CB have reported a moderate CB (Jite et al, 2021; Lee et al., 2018; Vahidi et al., 2016; Yusuf et al., 2011; Zuo et al., 2020). However, some studies report advanced CB (Garcia et al., 2020). The CB of those who provide care for patients with cancer is affected by many factors. One of them is spiritual well-being (SWB). SWB is an expression of spirituality and a measure of a person's spiritual health (Spatuzzi et al., 2019).
Spiritual well-being is a feeling of one's contentment defined as “the affirmation of life in a relationship with God, self, community and environment that nurtures and celebrates wholeness.” (National Interfaith Coalition on Aging, 1975). Various studies show that people who are spiritually strong feel more positive about their roles and communicate better when caring for their patients (Newberry et al., 2013; Sankhe et al., 2017; Spazutti et al., 2019; Tan et al., 2015; Vigna et al., 2020). The International Council of Nurses has included spirituality in nursing codes. ‘Spiritual distress’ and ‘risk for spiritual distress’ diagnoses are included in the nursing diagnosis list of the North American Nursing Diagnosis Association (Wilkinson & Barcus, 2016). Nurses are responsible for identifying CBs that may affect the health of caregivers and SWBs that are known to be associated with CBs as well as for providing care. SWB can be used as a cost-effective and effective intervention to reduce the CB of caregivers of patients with breast cancer. In line with this information, our research was carried out to define the relationship between the SWB of caregivers of patients with breast cancer and their CB.
Study Questions
-
What is the level of CB of caregivers of patients with breast cancer?
-
What is the level of SWB of caregivers of patients with breast cancer?
-
Is there a relationship between the SWB of caregivers of patients with breast cancer and their CB?
Method
Study Design
It is a descriptive and correlational study.
Study Setting and Sample
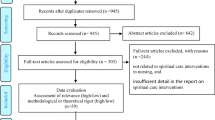
The study was conducted in the inpatient unit of a university hospital oncology clinic and in the outpatient chemotherapy unit. The study conducted with family caregivers of patients with breast cancer who applied to a university hospital oncology clinic for treatment. A total of 138 family caregivers who met the criteria for participation in the study and agreed to participate in the study constituted the study sample.
Study Power
Gpower 3.1.9.2 was used in calculating the sample size (Faul et al., 2009). The mean care load score of caregivers of cancer patients in the study by Bahrami et al. (2014) was used for calculating the sample size. With a 95% confidence (1 − α), 95% test power (1 − β), d = 0.333 effect size and two-way t-test, the sample size for this study was determined as 133 people. The study was completed with 138 people. The posthoc power of the research is 0.957.
Inclusion Criteria for Participants in the Study
Being ≥ 18 years of age, being a family member responsible for the care of a patient diagnosed with breast cancer, being referred to by the caregivers themselves or the patient as a primary care provider, not having any health problems, not having a cancer diagnosis or neurological cognitive disorder, being able to communicate in Turkish, and being a caregiver for ≥ 3 months.
Exclusion Criteria for Participants
Wanting to withdraw from the research for any reason while the research is in progress and being < 18 years of age.
Data Collection Technique and Tools
Data were collected using the participant information form, caregiver burden scale and spiritual well-being scale.
Participant Information Form
It is a form prepared by the researchers, consisting of a total of 16 questions related to the age, socio-demographic status and employment status of the participants (Spatuzzi et al., 2019; Vigna et al., 2020).
Caregiver Burden Scale (CBS)
It is a scale used to evaluate the CB of those who care for a person or elderly in need of care (Zarit et al., 1980). ‘‘The Turkish validity and reliability of the scale was assessed by İnci and Erdem. The reliability coefficient of the scale is between 0.87 and 0.99. The scale consists of 22 statements. It is a 5-point Likert type scale (never, rarely, sometimes, frequently, and nearly always). A minimum score of 0 and a maximum score of 88 points can be obtained on the scale. In this study, scale scores were evaluated as no/little burden (0–20 points), moderate burden (21–40 points), severe burden (41–60 points) and very severe burden (61–88 points)’’ (İnci & Erdem, 2010). The Cronbach’s α value of this study is 0.92.
Three-Factor Spiritual Well-Being Scale (SWBS)
The validity and reliability of this scale was assessed by Ekşi and Kardaş (Ekşi & Kardaş, 2017; Kardaş, 2019). Three-factor Spiritual Well-being Scale in Turkish was given in Table 1 (Ekşi and Kardaş 2017; Kardaş 2019), spiritual and social dimensions of a person's life and to determine the quality of this process. It is a 5-point Likert type scale. The transcendency subscale consists of items 1, 4, 5, 8, 9, 12, 13, 16, 17, 20, 21, 24, 25, 27 and 29; the harmony with nature subscale consists of items 2, 6, 10, 14, 18, 22 and 28 and the anomie subscale consists of items 3, 7, 11, 15, 19, 23 and 26. When a total score is desired, reverse scoring is applied for the items in the anomie subscale. The Cronbach's α value of the scale was determined as 0.763’’ (Ekşi & Kardaş, 2017; Kardaş, 2019). The Cronbach’ alpha value of this study is 0.81.
Data Collection
The data of the study were collected between August 2021 and October 2021. The data were collected through face-to-face interviews with caregivers of patients with breast cancer. The data collection took approximately 10–15 min. Due to the ongoing coronavirus disease-19 pandemic, the interviewers and interviewees wore masks and maintained social distance during the interview.
Ethical Principles
Ethics committee approval was obtained before starting the research (App. Date/ No: 07.07.2021/ 2021–12-63). Institutional permission was obtained from the hospital (E-14567952–900-71,409). Oral and written consents of the participants were obtained. The research was carried out according to the principles of the Declaration of Helsinki.
Data Analysis
Data analysis was performed using Statistical Package for Social Science 22.0 package program. Descriptive data were evaluated using percentile, mean, standard deviation, minimum and maximum values. The conformity of the data to the normal distribution according to the groups was determined by the Kolmogorov–Smirnov/Shapiro–Wilk test. The one-way analysis of variance, independent samples t-test and post-hoc Tukey’s test were used for the analysis of the data. The relationship between the total scale scores was determined using Pearson’s correlation analysis. P < 0.05 was accepted as the level of statistical significance.
Results
The descriptive characteristics of the patients are given in Table 2.
The total SWBS scores and CBS scores are given in Table 3 based on the descriptive characteristics of the caregivers. The CBS of female caregivers were significantly higher than those of male caregivers (p = 0.040). A statistically significant difference was observed between the duration of care and SWB (p = 0.001) and CB (p = 0.003) scales mean scores. According to the post-hoc Tukey’s test, caregivers who provide 24-h care had a significantly higher CBS score than the score of those who provide care for 3 h (p = 0.044) and 4–6 h (p = 0.012). According to the post-hoc Tukey’s test results, the total SWB scores of caregivers who provide care between 3 hours (p = 0.014) and 4–6 hours (p = 0.006) a day were significantly higher than those who provide care for 24 hours a day. A statistically significant difference was observed between the SWBS scores of those who received education about the disease and those who did not (p = 0.007). The SWBS scores of those who did not receive education were significantly higher (Table 3).
Caregivers' total CB scale, total SWB and subscale scores are given in Table 4. The caregivers had a moderate CB, whereas their SWB was quite high.
Table 5 demonstrates the negatively significant relationship between CB and SWB (p = 0.000, r = -0.357). There was no significant relationship of disease duration, disease stage, caregiver’s age and SWB with CB (Table 5).
Participants reported no/little burden (27%), moderate burden (36%), severe burden (30%) and very severe burden (7%).
Discussion
This research aimed to identify the CB and SWB of family caregivers of patients with breast cancer and the relationship between them. As breast cancer is the most common cancer, the research was conducted with the caregivers of these patients.
A total of 50.7% of the patients of the caregivers participating in this study had stage 4 breast cancer. Due to the increased care needs of advanced cancer patients as a result of treatments such as chemotherapy and radiotherapy, many family caregivers have a high CB (Roij et al., 2021). In this study, the CB of female caregivers was significantly higher than that of male caregivers. According to the literature, women are at a higher risk of having a high CB than men (Han et al., 2013; Jansen et al., 2018). This may be due to the fact that women, whose responsibilities are already excessive in daily life, are also the caregivers of an individual with cancer. As the responsibilities of a caregiver increase, the care process becomes tiring, dependent and long. According to our research results, the CB of those who provide 24-h care is significantly higher than those who care for 3 h and 4–6 h. Similarly, caregivers who provide care for more than 6 h a day have the highest CB (Zuo et al., 2020). Providing intensive and uninterrupted care leads to an increase in the CB (Vigna et al., 2020). For this reason, caregivers should be supported socially, psychologically and economically as the duration of care increases. Caregivers should be supported with practical support, better case management and greater recognition of the role of caregivers (Heath et al., 2018).
In this study, the SWB of those who did not receive education about the disease was significantly higher than that of those who received education. In Turkey, patients diagnosed with cancer and their caregiver family members are informed about the stage of the disease, its treatment, side-effects of the treatment and emergency situations. The educational contents are prepared in a standard manner by the healthcare professionals of the hospital education unit. However, each individual's educational needs are different. The education should be tailored to the educational needs of the patients and caregivers.
The caregivers who participated in this study had a moderate CB. Studies on CB reported moderate CB (Jite et al., 2021; Zuo et al., 2020) as well as severe CB (Garcia et al., 2020). Excessive CB may cause the care receiver to receive inappropriate and unsafe care (Lafferty et al., 2016). Increased CB is associated with depression and anxiety in patients (Dionne et al., 2016). At the same time, CB negatively affects the patient's quality of life (An et al., 2019). The needs of caregivers may change at different times during the care process (Treanor, 2020). Basically, caregivers with a high level of CB are at risk for a continued increase in CB in the following years (Jansen et al., 2021). In the present study, 36% of the participants had moderate care burden. Similarly Asadi et al. reported 39.5% moderate burden (Asadi et al., 2019).
SWB is a protective factor against psychological and physiological diseases. (Delgado-Guay et al., 2014). SWB is an important factor in coping with the difficulties that caregivers experience during the care of patients with cancer. SWB is a concept that includes both religion and spirituality (Akkuş et al., 2022). More religion or spirituality was associated with lower depressive symptoms and less personality disorder (Power & McKinney, 2014), less post-traumatic stress and perceived stress (Arévalo et al., 2008) also this may affect caregiver burden. In this study, the SWB of the caregivers was found to be quite high. SWB is an important factor that can affect CB and the physical health of caregivers (Spatuzzi et al., 2019). Individuals with high spirituality feel less CB (Vigna et al., 2020). Some studies show that spirituality and religious beliefs reduce distress in caregivers (Hosseini et al., 2016; Koenig, 2015) and also this may be used as coping strategies for stressful situations (Torabi Chafjiri et al., 2017).
The most important result of this research is that as the SWB of caregivers increases, their CB decreases. Similarly, there are studies reporting that SWB is negatively related to CB, and that spirituality can be used as an effective and low-cost intervention to reduce the CB (Rafati et al., 2020). Caregivers with low levels of spirituality are at higher risk of CB, anxiety and stress (Newberry et al., 2013). In this study, the total SWB scores of the caregivers who provide care between 3 h and 4–6 h a day are significantly higher than the scores of those who care for 24 h a day. This finding also supports the negative relationship between SWB and CB.
Due to the increase in the elderly population and in the number of chronic and fatal diseases, the number of individuals who need care and the number of caregivers increase every year. The CB of caregivers of women with breast cancer, one of the most common types of cancer, also increases in this process. Caregivers should be supported in terms of treatment, care and financial issues to eliminate the negative effects of CB on both the caregiver and the patient.
Limitations
The first limitation of the study is that the data were collected only from a single hospital. Therefore, the results of this study should be cautiously generalized to other settings. It is recommended to conduct longitudinal design studies. Many factors affecting the concept of spiritual well-being, such as psychosocial characteristics of caregivers, perceptions of social support, and attachment patterns, were not considered.
Conclusion and Recommendations
According to our results, caregivers have a moderate level of CB and their SWB is quite high. There is a negative relationship between CB and SWB. Nurses, whose main role is to provide care, have important duties in reducing the CB of family caregivers. Follow-up of patients with breast cancer who are cared for at home should be provided by primary health care services. Family physicians and nurses should be in frequent contact with caregivers to reduce the CB and develop coping strategies. Caregivers of patients with breast cancer should be provided effective health counselling, psychosocial care and moral support following the diagnosis of cancer. Since female caregivers have a high care burden, they should be supported more and protected from burnout. Caregivers with longer daily care periods have a higher CB and lower SWB. It is recommended that caregivers with long daily caregiving periods are supported by social services in their care activities. Spirituality can be an important factor influencing the role of a caregiver. As spirituality has different meanings and roles in different cultures and religious beliefs, its relationship with CB may vary. Therefore, conducting more studies in different countries is recommended.
Data Availability
The data that support the findings of this study are available on request from the corresponding author.
References
Adelman, R. D., Tmanova, L. L., Delgado, D., Dion, S., & Lachs, M. S. (2014). Caregiver burden: A clinical review. JAMA, 311(10), 1052–1060. https://doi.org/10.1001/jama.2014.304
Akkuş, Y., Karacan, Y., Ünlü, K., Deniz, M., & Parlak, A. (2022). The effect of anxiety and spiritual well-being on the care burden of caregivers of cancer patients during the COVID-19 pandemic. Supportive Care in Cancer : Official Journal of the Multinational Association of Supportive Care in Cancer, 30(2), 1863–1872. https://doi.org/10.1007/s00520-021-06611-0
An, Y., Fu, G., & Yuan, G. (2019). Quality of life in patients with breast cancer: the influence of family caregiver’s burden and the mediation of patient’s anxiety and depression. The Journal of Nervous and Mental Disease, 207(11), 921–926. https://doi.org/10.1097/NMD.0000000000001040
Arévalo, S., Prado, G., & Amaro, H. (2008). Spirituality, sense of coherence, and coping responses in women receiving treatment for alcohol and drug addiction. Evaluation and Program Planning, 31(1), 113–123. https://doi.org/10.1016/j.evalprogplan.2007.05.009
Asadi, P., Fereidooni-Moghadam, M., Dashtbozorgi, B., & Masoudi, R. (2019). Relationship between care burden and religious beliefs among family caregivers of mentally ill patients. Journal of Religion and Health, 58(4), 1125–1134. https://doi.org/10.1007/s10943-018-0660-9
Bahrami, M., & Farzi, S. (2014). The effect of a supportive educational program based on COPE model on caring burden and quality of life in family caregivers of women with breast cancer. Iranian Journal of Nursing and Midwifery Research, 19(2), 119–126.
Baider, L., & Surbone, A. (2014). Universality of aging: family caregivers for elderly cancer patients. Frontiers in Psychology, 5, 744. https://doi.org/10.3389/fpsyg.2014.00744
Delgado-Guay, M. O. (2014). Spirituality and religiosity in supportive and palliative care. Current Opinion in Supportive and Palliative Care, 8(3), 308–313. https://doi.org/10.1097/SPC.0000000000000079
Dionne-Odom, J. N., Hull, J. G., Martin, M. Y., Lyons, K. D., Prescott, A. T., Tosteson, T., Li, Z., Akyar, I., Raju, D., & Bakitas, M. A. (2016). Associations between advanced cancer patients’ survival and family caregiver presence and burden. Cancer Medicine, 5(5), 853–862. https://doi.org/10.1002/cam4.653
Ekşi, H., & Kardaş, S. (2017). Spiritual well-being: scale development and validation. Spiritual Psychology and Counseling, 2, 73–88. https://doi.org/10.12738/spc.2017.1.0022
Faul, F., Erdfelder, E., Buchner, A., & Lang, A. G. (2009). Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behavior Research Methods, 41(4), 1149–1160. https://doi.org/10.3758/BRM.41.4.1149
García-Torres, F., Jabłoński, M. J., Gómez Solís, Á., Jaén-Moreno, M. J., Gálvez-Lara, M., Moriana, J. A., Moreno-Díaz, M. J., & Aranda, E. (2020). Caregiver burden domains and their relationship with anxiety and depression in the first six months of cancer diagnosis. International Journal of Environmental Research and Public Health, 17(11), 4101. https://doi.org/10.3390/ijerph17114101
Han, Y., Yuan, J., Luo, Z., Zhao, J., Wu, J., Liu, R., & Lopez, V. (2013). Determinants of hopelessness and depression among Chinese hospitalized esophageal cancer patients and their family caregivers. Psycho-Oncology, 22(11), 2529–2536. https://doi.org/10.1002/pon.3315
Heath, A., Carey, L. B., & Chong, S. (2018). Helping carers care: an exploratory study of factors impacting informal family carers and their use of aged care services. Journal of Religion and Health, 57(3), 1146–1167. https://doi.org/10.1007/s10943-018-0593-3
Hosseini, S., Chaurasia, A., Cooke, M., & Oremus, M. (2016). Effect of religious involvement on cognition from a life-course perspective: protocol for a systematic review and meta-analysis. British Medical Journal Open, 6(9), e011301. https://doi.org/10.1136/bmjopen-2016-011301
İnci, F., & Erdem, M. (2010). Bakım verme yükü ölçeği’nin Türkçe’ye uyarlanması geçerlilik ve güvenilirliği. Anadolu Hemşirelik Ve Sağlık Bilimleri Dergisi, 11(4), 85–95.
Jansen, L., Dauphin, S., De Burghgraeve, T., Schoenmakers, B., Buntinx, F., & van den Akker, M. (2021). Caregiver burden: an increasing problem related to an aging cancer population. Journal of Health Psychology, 26(11), 1833–1849. https://doi.org/10.1177/1359105319893019
Jansen, L., Dauphin, S., van den Akker, M., De Burghgraeve, T., Schoenmakers, B., & Buntinx, F. (2018). Prevalence and predictors of psychosocial problems in informal caregivers of older cancer survivors-a systematic review: still major gaps in current research. European Journal of Cancer Care, 27(6), e12899. https://doi.org/10.1111/ecc.12899
Jite, I. E., Adetunji, A. A., Folasire, A. M., Akinyemi, J. O., & Bello, S. (2021). Caregiver burden and associated factors amongst carers of women with advanced breast cancer attending a radiation oncology clinic in Nigeria. African Journal of Primary Health Care & Family Medicine, 13(1), e1–e8. https://doi.org/10.4102/phcfm.v13i1.2812
Kardaş, S. (2019). Erratum: correcting the name of the spiritual well-being scale as the three-factor spiritual well-being scale. Spiritual Psychology and Counseling, 4, 85–85. https://doi.org/10.12738/spc.2019.4.1.0068
Koenig, H. G. (2015). Religion, spirituality, and health: a review and update. Advances in Mind-Body Medicine, 29(3), 19–26.
Lafferty, A., Fealy, G., Downes, C., & Drennan, J. (2016). The prevalence of potentially abusive behaviours in family caregiving: findings from a national survey of family carers of older people. Age and Ageing, 45(5), 703–707. https://doi.org/10.1093/ageing/afw085
Lee, Y. H., Liao, Y. C., Shun, S. C., Lin, K. C., Liao, W. Y., Chang, P. H., Jhang, S. Y., Yu, C. J., Yang, P. C., Hsieh, P. Y., & Lai, Y. H. (2018). Trajectories of caregiver burden and related factors in family caregivers of patients with lung cancer. Psycho-Oncology, 27(6), 1493–1500. https://doi.org/10.1002/pon.4678
National Interfaith Coalition on Aging. (1975). Spiritual wellbeing: a definition. National Interfaith Coalition on Aging.
Newberry, A. G., Choi, C. W., Donovan, H. S., Schulz, R., Bender, C., Given, B., & Sherwood, P. (2013). Exploring spirituality in family caregivers of patients with primary malignant brain tumors across the disease trajectory. Oncology Nursing Forum, 40(3), E119–E125. https://doi.org/10.1188/13.ONF.E119-E125
Power, L., & McKinney, C. (2014). The effects of religiosity on psychopathology in emerging adults: intrinsic versus extrinsic religiosity. Journal of Religion and Health, 53(5), 1529–1538. https://doi.org/10.1007/s10943-013-9744-8
Rafati, F., Mashayekhi, F., & Dastyar, N. (2020). Caregiver burden and spiritual well-being in caregivers of hemodialysis patients. Journal of Religion and Health, 59(6), 3084–3096. https://doi.org/10.1007/s10943-019-00939-y
Sankhe, A., Dalal, K., Agarwal, V., & Sarve, P. (2017). Spiritual care therapy on quality of life in cancer patients and their caregivers: a prospective non-randomized Single-cohort study. Journal of Religion and Health, 56(2), 725–731. https://doi.org/10.1007/s10943-016-0324-6
Schulz, R., Beach, S. R., Czaja, S. J., Martire, L. M., & Monin, J. K. (2020). Family caregiving for older adults. Annual Review of Psychology, 71, 635–659. https://doi.org/10.1146/annurev-psych-010419-050754
Spatuzzi, R., Giulietti, M. V., Ricciuti, M., Merico, F., Fabbietti, P., Raucci, L., Bilancia, D., Cormio, C., & Vespa, A. (2019). Exploring the associations between spiritual well-being, burden, and quality of life in family caregivers of cancer patients. Palliative & Supportive Care, 17(3), 294–299. https://doi.org/10.1017/S1478951518000160
Sun, V., Raz, D. J., & Kim, J. Y. (2019). Caring for the informal cancer caregiver. Current Opinion in Supportive and Palliative Care, 13(3), 238–242. https://doi.org/10.1097/SPC.0000000000000438
Tan, J. Y., Lim, H. A., Kuek, N. M., Kua, E. H., & Mahendran, R. (2015). Caring for the caregiver while caring for the patient: exploring the dyadic relationship between patient spirituality and caregiver quality of life. Supportive Care in Cancer : Official Journal of the Multinational Association of Supportive Care in Cancer, 23(12), 3403–3406. https://doi.org/10.1007/s00520-015-2920-5
TorabiChafjiri, R., Navabi, N., Shamsalinia, A., & Ghaffari, F. (2017). The relationship between the spiritual attitude of the family caregivers of older patients with stroke and their burden. Clinical Interventions in Aging, 12, 453–458. https://doi.org/10.2147/CIA.S121285
Treanor, C. J. (2020). Psychosocial support interventions for cancer caregivers: reducing caregiver burden. Current Opinion in Supportive and Palliative Care, 14(3), 247–262. https://doi.org/10.1097/SPC.0000000000000508
Vahidi, M., Mahdavi, N., Asghari, E., Ebrahimi, H., EivaziZiaei, J., Hosseinzadeh, M., NamdarAreshtanab, H., & Kermani, I. A. (2016). Other side of breast cancer: factors associated with caregiver burden. Asian Nursing Research, 10(3), 201–206. https://doi.org/10.1016/j.anr.2016.06.002
Van Roij, J., Brom, L., Sommeijer, D., van de Poll-Franse, L., & Raijmakers, N. (2021). Self-care, resilience, and caregiver burden in relatives of patients with advanced cancer: results from the eQuiPe study. Supportive care in cancer : official journal of the Multinational Association of Supportive Care in Cancer, 29(12), 7975–7984. https://doi.org/10.1007/s00520-021-06365-9
Vigna, P. M., de Castro, I., & Fumis, R. (2020). Spirituality alleviates the burden on family members caring for patients receiving palliative care exclusively. BMC Palliative Care, 19(1), 77. https://doi.org/10.1186/s12904-020-00585-2
Wilkinson, J. M., & Barcus, L. (2016). Nursing Diagnosis Handbook (Translate: Kapucu S., Akyar I., Korkmaz F) (11th ed.). Pearson.
World Health Organization. (2020, December). The global cancer observatory reports, International agency for research on cancer number of new cases in 2020, both sexes all ages. Retrieved from Nov 1, 2021 https://gco.iarc.fr/today/data/factsheets/cancers/20-Breast-fact-sheet.pdf.
Yusuf, A. J., Adamu, A., & Nuhu, F. T. (2011). Caregiver burden among poor caregivers of patients with cancer in an urban African setting. Psycho-Oncology, 20(8), 902–905. https://doi.org/10.1002/pon.1814
Zarit, S. H., Reever, K. E., & Bach-Peterson, J. (1980). Relatives of the impaired elderly: correlates of feelings of burden. The Gerontologist, 20, 649–655.
Zuo, Y., Luo, B. R., Peng, W. T., Liu, X. R., He, Y. L., & Zhang, J. J. (2020). Informal caregiver burden and influencing factors in gynaecological oncology patients hospitalized for chemotherapy: a cross-sectional study. The Journal of International Medical Research, 48(11), 300060520974927. https://doi.org/10.1177/0300060520974927
Funding
The authors received no financial support for the research, authorship and/or publication of this article. This research received no specific grant from any funding agency in the public, commercial, or not for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The author declares they have no potential conflict of interest. The authors report no actual or potential conflicts of interest.
Ethical Approval
All procedures in the study performed in accordance with the ethical standards of the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Was obtained from all participants who were included in the study. This study was verbal presented in 10th International Medicine and Health Sciences Researchers Congress, 27–28 August 2022 Ankara /Turkey.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Türkben Polat, H., Kiyak, S. Spiritual Well-Being and Care Burden in Caregivers of Patients with Breast Cancer in Turkey. J Relig Health 62, 1950–1963 (2023). https://doi.org/10.1007/s10943-022-01695-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10943-022-01695-2