
Abstract
Increasing number of students struggle with test anxiety. Evidence based, online, affordable, and accessible solutions for test anxiety are scarce. The purpose of this study was to evaluate an online delivered, assisted intervention (REST-TA) in a randomized controlled trial.
Participants (N = 178) were recruited through a university course and were randomized into a treatment group and waitlist control group. The treatment group completed an 8-week program which consisted of relaxation, skill training and cognitive behavioral methods. Both treatment and control group filled out a battery of questionnaires (TAMC-SF, STAI, DASS, MBI-SS, Resilience) pre and post-treatment.
According to our results there was a significant reduction in test anxiety between pre and post intervention. We found a significant increase in trait anxiety, negative affectivity, and burnout in the control group, while no change or slight decrease in these scores in the treatment group. Our analyses also yielded a significant increase in resilience scores in the treatment group while resilience scores did not change for the control group.
We conclude that REST-TA was successful at reducing test anxiety. Moreover, it helped to maintain the subjective well-being of students, while increasing resilience. Online solutions are a scalable option for universities to implement, therefore programs such as REST-TA could be of great help to improve the mental health of university students.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
According to a widely accepted concept, we can think of test anxiety as a situational personality trait. This refers to one’s tendency of excessive worry, intrusive thoughts, mental disorganization, tension and psychological arousal in situations that involve evaluation (Spielberger & Vagg, 1995). Importance of testing is quite obvious, since it provides comparable information for making fast, yet well founded decisions. Traditions of testing started centuries ago, and the practice of it spread first through Europe, then in America. The first oral exam was performed at the University of Bologna and the first written test was used at Cambridge University in 1972. As the testing of our students becomes even more frequent, test anxiety is becoming a mental health issue (Bassetti et al., 2011). Early studies usually reported the prevalence of test anxiety between 10 and 30%. Kondaš (1967) for example found that 10% of students struggle with test anxiety, while Nottelmann and Hill (1977) report a 25–30% prevalence. More recent studies report similar or even higher numbers: Turner and colleagues (1993) estimated the prevalence of test anxiety among African American students around 41%. Kavakci and colleagues (2014) found 48% of students with high test anxiety. Recently Thomas and colleagues (2017) reported test anxiety in approximately 25% of undergraduate students. Roughly 50% of anatomy students were found to be test anxious in a different study (Bischofsberger et al., 2021).
There is moderate (estimated between 0.4 and 0.6) association between test and trait anxiety (Hodge et al., 1997). The strength of this association between the two constructs leaves enough room to give grounds for distinguishing the two concepts (Newbegin & Owens, 1996; Sarason, 1959).Test anxiety not only affects the mental wellbeing of students, it is inversely associated with test performance (Chapell et al., 2005; Sommer & Arendasy, 2015; von der Embse et al., 2018). Although the direction of association is not clear, the students’ belief that test anxiety has an adverse effect on performance may be enough to perform less than desirable (Hong & Karstensson, 2002). Highly test anxious students often process and store information ineffectively, which can lead to low performance and bad grades (Naveh-Benjamin et al., 1987; Culler & Holahan, 1980). Besides connection with academic performance, test anxiety is also related to college dropout rates (Krispenz et al., 2019). For example, Spielberger (1962) found that only 6% of students with low test anxiety dropped out of college, while 20% of highly test anxious students failed to finish their studies.
Classical theories indicate that test anxiety has two main components (affective and cognitive). These were first identified by Liebert and Morris (1967), who based their study on the Test Anxiety Questionnaire (TAQ: Mandler & Sarason 1952). The emotional factor includes certain behavioral reactions to the situation (e.g., nervousness, clicking with a pen, checking the time regularly) and the fight or flight response of the sympathetic nervous system. These are the relatively easily measurable and observable signs of test anxiety. Worry is the cognitive desperation regarding the consequences of a failed exam. According to Sarason, factors contributing to the emergence of worry are students’ capacity, difficulty of the test, fear of bad grades, and lack of preparedness (Sarason et al., 1990). Morris & Liebert (1970) found that worry has a stronger relationship with performance than with emotional reaction. More recent theories include behavioral components for example, inadequate learning strategies and self-destructive behaviors, such as procrastination, or avoidant behavior (Zeidner, 2010). Other approaches (which consider some types of anxiety as beneficial) separate test anxiety into 6 factors: 5 test anxiety factors and one facilitating anxiety factor. This comprehensive approach builds on a wide range of studies and theories (Lowe, 2019). According to this model the following factors define test anxiety: cognitive interference, physiological hyperarousal, social concerns, task irrelevant behaviors, worry and facilitating anxiety.
Students often report difficulties accessing help for anxiety or perceive available options as inconvenient. The demand for psychological help is often too big, to keep up with, for campus communities (Lattie et al., 2019; Mowbray et al., 2006). For example, in a survey, almost all college counseling center directors expressed that the number of students with psychological problems was a growing concern in their institute (Mistler et al., 2012). Those students who attend university full time may have a harder time accessing help from a psychologist during regular business hours (Mistler et al., 2012). Additionally, there is a high cost that is associated with seeking help from a psychologist, which in many cases is out of the financial reach of students. This “campus mental health crisis” (Xiao et al., 2017) requires evidence-based, easily accessible alternative options for mental care.
In our era, in which there is a rising demand to perform better on tests coupled with less spare time to spend on mental health, self-help interventions become more important. With technological advancement, a growing number of interventions have become accessible, helping people to get the help they need. Several systematic reviews and meta-analyses have demonstrated the efficacy of computerized and internet-delivered self-help programs (Griffiths et al., 2010; Lewis et al., 2012; Christensen et al., 2014). These methods proved to be effective in treating different anxiety disorders (panic disorder, social phobia, PTSD, generalized anxiety disorder) and depression. In many cases, face-to-face therapy did not differ from online delivery of cognitive behavioral therapy (e.g. Cuijpers & Cuijpers et al., 2009), and adherence to the program was also comparable to other forms of psychotherapy (Christensen et al., 2014).
To the authors’ knowledge there are only two other online programs that focus specifically on test anxiety. Orbach and colleagues (2007) designed a 6-module online intervention for test anxiety based on cognitive behavioral therapy, skill training and progressive muscle relaxation. This program was successful in reducing test anxiety and the reduction was correlated with initial test anxiety. The strengths of this study are the use of a placebo control group and randomization. Unfortunately, Orbach and colleagues did not measure other aspects of students’ subjective wellbeing such as burnout, resilience, or negative affect which may have been affected by their program.
Reiss and colleagues (2019) have designed an online platform aiming to reduce test anxiety. This 5-week program is based on a combination of CBT, skill training and positive imagery. Their program was successful in reducing test anxiety and improving other aspects of subjective wellbeing. Their platform is available in the university (where the study was conducted) for students. One of the weaknesses of the study design is that it did not use a control group and had a low number of participants.
Both of the above-mentioned studies combined different methods such as skill training, CBT, positive imagery. Orbach and colleagues (2007) acknowledge that a mixture of different methods may work better at reducing test anxiety than only using one specific method. This thinking is also echoed in the meta-analysis of Ergene (2003), who found that those interventions are the most effective at reducing test anxiety that combine different methods.
The aim of the present study is to evaluate an online delivered program aiming to reduce test anxiety. It is based on the combination of relaxation and skill training, mixed with positive, guided imagery, suggestions and CBT methods (REST-TA). We hypothesized that students in the treatment condition would show a significant reduction in test anxiety compared to the waitlist control group. The elements in the program may also affect a wider aspect of subjective well-being, thus we also hypothesized that trait anxiety measured by the State and Trait Anxiety Inventory (STAI) and negative affectivity measured by the Depression, Anxiety and Stress Scale (DASS) would also show a significant difference between the two groups. Other measures related to students’ mental health such as the scores obtained on the burnout questionnaire (MBI-SS) and Resilience scale would also differ between the two groups.
Method
Procedure
Participants (N = 178) were recruited through a university course and participated in the study for course credit. Students participated in an online session at the beginning of the course.
During that session they were given detailed information about the study. After the online session, they were randomized into treatment and waitlist control group, and they were asked to fill out a battery of questionnaires online. Some of the students also attended a 30-minute session where their electrodermal activity was assessed. Results regarding this aspect of the experiment will be reported elsewhere. The wait list control group was promised access to the program at the end of the study. Participants in the treatment condition completed a protocol containing 8 modules (detailed description of the modules are below), using a website that was designed specifically for this study. When students completed all modules, they were asked to fill out the same battery of questionnaires that they completed before intervention. At this time the students in the control group were also asked to fill out the battery of questionnaires. Once the questionnaires were filled out the control group was granted access to the website.
Description of the modules
Throughout 8 weeks, participants had access to 8 modules, all of them containing a skill training or a suggestive communication-based relaxation module. Two modules (module 2 and 8) had a combined structure, with relaxation and skill training in the same module. One module per week needed to be completed, and we rated completion rates based on whether the necessary self-reflection exercise was sent to the assigned research assistant. Self-reflection exercises were designed to help participants adhere to treatment. Students could only progress to the following part of the online program once they listened to all content in the previous module. Each module was 30–60 min in length.
Relaxation exercises
All relaxation exercises started with a guided relaxation induction. This was followed by positive imagery, suggestions and visualization of different themes that included: self-confidence and self-acceptance; increase the sense of competence; facilitate emotional stability, promote sleep and learning processes; promoting positive self-image finally trust and confidence in one’s intuition and abilities.
Skill training
Skill training (ST) modules included psychoeducation on stress and test anxiety and associated lifestyle factors; adaptive and maladaptive coping mechanisms; time management; learning and test writing strategies; and cognitive-behavioral therapy-based exercises. After each ST educational phase, a short version of progressive muscle relaxation was taught.
Measures
TAMC-SF is a 24 item self-report test anxiety questionnaire, which was developed from the 43 item TAMC questionnaire (Lowe, 2021). It’s a relatively new, modern questionnaire based on the most recent test anxiety theories. Items are rated on a four-point Likert scale, which ranged from (1,) never, to (4,) almost always. It measures six factors of test anxiety: social, worry, cognitive interference, task irrelevant behavior, psychophysiological hyperarousal, facilitating anxiety (Lowe, 2021).
The State and Trait Anxiety Inventory is a 40 item self-report anxiety questionnaire. STAI is frequently used to measure both state (STAI-s) and trait (STAI-t) anxiety. Items are rated on a four-point Likert scale from ‘never applies to me’’ to “almost always applies to me” (Spielberger et al., 1970).
The Depression, Anxiety and Stress scale (DASS-21) is a 21 item Likert scale questionnaire assessing 3 dimensions of negative emotional states: depression, anxiety and stress. Items are rated from 0 to 3, “0” meaning never applies to me and “3” meaning almost always applies to me. Items in the depression scale include examples like: “I couldn’t seem to experience any positive feeling at all.” Items in the anxiety scale include questions such as this: “I experienced trembling (eg, in the hands)”. Finally, items in the stress scale include questions such as the following: “I found myself getting agitated”. Each scale includes 7 items and the DASS-21 gives a total score and a score for each scale (Henry & Crawford, 2005).
The Maslach burnout inventory student survey (MBI-SS) was derived from the Maslach burnout inventory general survey (MBI-GS) by Schaufeli et al. (2002), which is a 15 item Likert scale questionnaire, designed to explore student burn out. Items are rated from 0 to 6 on a 7-point Likert scale. The survey gives a total score and explores 3 factors of burnout. It measures emotional exhaustion (e.g. “I feel exhausted by the end of university day”), cynicism (e.g.“I feel more cynic about applying my lessons”),, academic efficacy (e.g.“In my opinion I am a good student.”) (Hazag et al., 2010).
The resilience scale is a one factor 10 item questionnaire derived from the Connor– Davidson 25 item resilience scale. Items are rated on a 4-point Likert scale ranging from “never” to “almost always”. It measures resilience with questions such as “think of myself as a strong person” or “able to adapt to change” (Járai et al., 2015).
Results
Dropout rate
According to the results, out of the 89 participants that were randomized to the treatment group 87% filled out the pre-intervention battery of questionnaires, 80% started intervention, and 71% finished the program. REST-TA had a dropout rate of 12.5% which was calculated based on the number of participants who started the treatment and finished it. In the control group, out of the 89 participants 85% filled out the pre-intervention battery of questionnaires and 72% of the participants filled out the post-intervention battery of questionnaires (Fig. 1).

Flow diagram of the procedure
Baseline (pre-treatment comparisons)
Participants’ age and gender distribution in the treatment and control group is displayed in Table 1. The independent sample t test yielded no significant differences between the two groups regarding age t(2, 125) = 0.17, p = .869. Chi squared analysis revealed no significant differences between the two groups regarding gender distribution χ2(1,127) = 0.32, p = .570.
There were no significant differences between the two groups on the STAI-T, DASS, MBI-SS and Resilience measures. On the TAMC-SF there was a significant pretreatment difference between the groups on the social and cognitive interference factor. There were no other significant differences between the two groups. Data is presented in Table 3. Reliability of the used measures is presented in Table 2.
Pre-treatment and post-treatment comparisons between conditions
Mixed ANOVA was conducted with the within subject variable of time (pre-treatment and post-treatment) and the between subject variable of group (treatment or control) on all outcome variables. Means and standard deviations are displayed in Table 3.
Results of the TAMC-SF
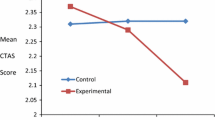
Our analysis resulted in a main effect of time on the TAMC-SF total score F(1,126) = 20.64, p < .001, η2 = 0.14, the mixed ANOVA yielded a significant interaction effect of time and group on the TAMC-SF total score F(1,126) = 6.76, p = .010, η2 = 0.05 (Fig. 1).
Furthermore we found a significant between subject effect on the total score of the TAMC-SF, F(1,126) = 8.70,p = .004, η2 = 0.05. The TAMC-SF total score fell between pre and post-treatment in both groups, while the scores in the treatment group fell significantly more than in the control group resulting in significant between subject differences.
Further examination of the factors of the TAMC-SF
Analysis of the TAMC-SF social score yielded a main effect of time F(1,126) = 4.23, p=0.042, η2 = 0.03. We found no interaction effect of time and group and it resulted in a between subject effect F(1,126) = 6.51,p = .012, η2 = 0.05. The TAMC-SF social score fell overall between pre and post-treatment in both groups, resulting in more salient between subject differences.
Examination of the cognitive interference factor of the TAMC-SF yielded no significant main or interaction effects. It resulted in a significant between-subject effect, F(1,126) = 6.97,p = .009, η2 = 0.05.
The analysis of the worry factor of the TAMC-SF resulted in a main effect of time F(1,126) = 104.07, p < .001, η2 = 0.45, an interaction effect of time and group F(1,126) = 6.65, p=0.011, η2 = 0.05. There were no other effects. The TAMC-SF worry scores fell in both groups over time, but it fell significantly more in the treatment group compared to the control group.
The mixed ANOVA on the psychophysiological hyperarousal factor of the TAMC-SF yielded no significant effects.
When Analyzing the task irrelevant behavior factor of the TAMC-SF we found no main effect. Our analysis resulted in an interaction effect of time and group F(1,126) = 4.26, p = .032, η2 = 0.04 and a significant between subject effect F(1,126) = 6.02,p = .015, η2 = 0.05. Scores of the task irrelevant behavior factor fell over time in the treatment group and increased in the control group, resulting in significant between subject differences.
The mixed ANOVA on the facilitating anxiety factor of the TAMC-SF yielded a significant main effect of time F(1,126) = 3.98,p = .048, η2 = 0.03. There were no other significant main or interaction effects that resulted from the analysis. Facilitating anxiety scores increased in both groups overtime.
Results of the STAI-trait
The mixed ANOVA yielded no significant main effect. It resulted in a significant interaction effect of time and group F(1,125) = 12.63, p = .001, η2 = 0.09 and a significant between subject effect F(1,125) = 5.06,p = .026, η2 = 0.05. There was a rise in the scores in the control group and a slight decrease in scores in the treatment group between pre and post treatment.
Results of the DASS-21
The analysis of the DASS-21 total score resulted in a significant main effect of time F(1,125) = 5.70, p = .018, η2 = 0.04, a significant interaction effect of time and group F(1,125) = 9.01, p = .003, η2 = 0.07 and a significant between subject effect F(1,125) = 5.32, p = .023, η2 = 0.04. Scores rose overall between pre and post treatment, however scores fell in the treatment group and significantly rose in the control group resulting in significant between subject differences.
The Mixed ANOVA on the anxiety factor of the DASS-21 yielded a marginally significant main effect of time F(1,125) = 3.92, p = .05, η2 = 0.03. Anxiety scores rose overall, however this rise may be contributed to the significant pre-post rise in the control group.
The analysis of the stress factor of the DASS-21 resulted in a main effect of time F(1,125) = 11.74, p = .001, η2 = 0.08, an interaction of time and treatment group F(1,125) = 12.10, p=0.001, η2 = 0.08 and a significant between subject effect F(1,125) = 4.16,p = .043, η2 = 0.03. Stress scores rose significantly in the control group between pre and post treatment. In contrast scores fell in the treatment group, resulting in significant between subject differences.
The mixed ANOVA on the depression factor of the DASS-21 yielded no main effect, it resulted in an interaction effect of time and group F(1,125) = 4.56,p = .0.035, η2 = 0.03 and a significant between subject effect F(1,125) = 7.22, p = .008, η2 = 0.06. There were no other significant main or interaction effects. Scores rose in the control group, while fell in the treatment group between pre and post-treatment resulting in significant between subject differences.
Results of the Resilience scale
The mixed ANOVA yielded a significant main effect on the scores of the Resilience questionnaire F(1,126) = 4.06, p = .046, η2 = 0.03, a significant interaction effect of time and group F(1,126) = 10.39, p = .002, η2 = 0.08. There were no other effects. The resilience score increased between pre and post treatment overall. Furthermore, there was an increase in resilience scores in the treatment group and a slight decrease in the resilience scores of the control group.
Results of MBI-SS
The mixed ANOVA on the total score of the MBI-SS yielded a main effect of time, F(1,125) = 16.50, p < .001, η2 = 0.12, a significant interaction effect of time and group, F(1,125) = 8.90, p = .003, η2 = 0.07. Scores rose overall, however scores of the control group rose significantly more than scores of the treatment group between pre and post-treatment.
The analysis of the emotional exhaustion factor of the MBI-SS yielded no main effect.
It resulted in an interaction effect of time and group F(1,125) = 6.63, p = .011, η2 = 0.05, and no other effects. Emotional exhaustion scores decreased in the treatment group and increased in the control group overtime.
The analysis of the cynicism factor of the MBI-SS resulted in no significant effects.
The examination of the academic efficacy factor of the MBI-SS resulted in a significant main effect of time F(1,125) = 74.91, p < .001, η2 = 0.38, and an interaction effect of time and group, F(1,125) = 7.29, p = .008, η2 = 0.06. There were no other significant effects. Scores rose overall, however, they did so significantly more in the control group between pre and post treatment than in the treatment group.
Discussion
REST-TA is a comprehensive online delivered solution, aiming to reduce test anxiety in university students. It is based on relaxation, positive suggestions, imagery, skill training and CBT methods. In a randomized study, we compared the treatment group to a waitlist control group, and according to our results the online treatment successfully reduced test anxiety in university students. Moreover, it positively affected trait anxiety and scores associated with negative affectivity. Furthermore, the program prevented the increase of burnout rate in the treatment group and helped raise resilience. This online delivered program is now available for students at the University.
Test anxiety as measured by the TAMC-SF total score was markedly reduced between pre and post treatment in the treatment group, and test anxiety was significantly reduced in the treatment group compared to the control group. Previous studies also showed test anxiety reduction in an online setting with similar or higher effect sizes to the present study (Orbach et al., 2007; Warnecke et al., 2020). Both of those studies had CBT methods as a core component of the program. REST-TA may be improved by implementing more CBT techniques in the future.
The scores of the social factor and worry factor of the TAMC-SF were reduced between pre and post measures in the treatment group and worry scores fell significantly more in the treatment group compared to the control group. Several factors could explain these changes. Firstly, the worry factor of the TAMC-SF describes concerns over exam failure and the social factor pertains to fear of negative evaluation (Lowe, 2019a, b). Both fear of failure and fear of negative evaluation is closely connected to perfectionism (Lowe, 2019a). Looking into the modules of REST-TA, we find that it specifically addresses perfectionism multiple times and explicitly considers worry in the modules. Secondly, REST-TA addresses self-efficacy, self-esteem, and specific skills of successful testing. A decrease in perfectionism coupled with an increase in self-efficacy, self-confidence and increased skills in testing could very well explain the effects of the intervention on these test anxiety factors. Interestingly, we also found a significant reduction in TAMC-SF worry scores in the control group. Participants were not instructed against seeking help for test anxiety, this may explain the reduction in their worry scores. Furthermore, during the semester they may also have become more efficient at coping with tasks by gaining confidence through repeated trials of tests and essays. Thus, their worry pertaining to failing or not performing at the desired level on an exam may have eased. The control group was also aware that they will receive the intervention before the exam period. Thoughts of getting some help before exams could possibly help with worrying thoughts of failure.
There were no effects of the intervention on the cognitive interference factor and the psychophysiological hyperarousal factor of the TAMC-SF. The cognitive interference factor assesses ability to concentrate and the presence of self-critical, distracting thoughts during exams. Although REST-TA has one module that focusses on concentration and memory enhancement, it may benefit from the implementation of CBT methods aiming to reduce the impact of intrusive self-critical thoughts which could interfere with concentration. The psychophysiological hyperarousal factor measures sympathetic overdrive during testing situations. Progressive muscle relaxation (PMR), aiming to reduce symphatetic arousal, is part of REST-TA, however it seems, that it had no transferable effects to exam situations. This is in contrast to others who found significant effects of PMR on test anxiety (Zargarzadeh & Shirazi, 2014). It is possible that the limited number of PMR practice sessions were not enough to exert effects during exams. REST-TA could be complimented by adding more PMR sessions, or biofeedback training could be implemented in it. Biofeedback may prove beneficial by giving students control or perceived control over their unwanted or unpleasant physical sensations, which interfere with testing. Indeed, studies reported improved performance and reduced anxiety among students who used biofeedback (Mccraty et al., 2000; Prato, 2009). Biofeedback protocols based on electrodermal activity target the symphatetic nervous system, therefore they present a good option to reduce arousal brought about by a testing situation.
Scores of the task irrelevant behavior factor of the TAMC-SF fell in the intervention group and rose in the control group. This factor evaluates mainly avoidance behavior. Increasing self-efficacy and self-confidence is discussed in multiple modules in the program. Since, self-efficacy is related to avoidance behavior (Ng & Lovibond, 2020), increased self-efficacy may have resulted in lower avoidance.
We found a reduction in trait anxiety (STAI-t) in the treatment group between pre and post intervention. This is compared to the significant trait anxiety score increase between pre and post treatment in the control group. Referring to Table 3, our sample consisted of participants with an average STAI-t score over 40. According to Spielberger (1983) scores over 40 on the STAI-t mark significant anxiety. The increased anxiety in the control group may be attributed to the fact that post intervention data collection took place at the end of the spring semester close to the exam period. The data collection period also coincided with COVID-19 quarantine and restrictions that may have increased overall anxiety levels. The results of the STAI trait scores nicely underpin the results regarding test anxiety reduction and show the effectiveness of REST-TA at reducing overall anxiety.
Our analysis also shows a reduction in the DASS-21 scores for the treatment group and an increase in the scores of the control group. The DASS-21 scores in our sample compared to the norms provided with the DASS-21 showed moderate anxiety and depression in both groups at pretest. The online program was successful not only in reducing test anxiety but reducing or preventing an increase in negative affect during the semester. Results of the DASS-21 also support results obtained by both the TAMC-SF and the STAI trait supporting the effectiveness of the online intervention.
The scores obtained on the burnout questionnaire (MBI-SS) are higher than scores reported in 2014 by Hazag and colleagues. This discrepancy may be due to the prolonged quarantine situation caused by the COVID-19 pandemic. Nevertheless, results of the MBI-SS and resilience scale show the same pattern of positive effect for the treatment group as the anxiety related measures. These results underline the fact, that the online intervention not only improved test anxiety and negative affect, but also the subjective wellbeing of the participants. The question may be raised, how burn-out and resilience was affected by the intervention. Both resilience and burn out is associated with anxiety (Lyu et al., 2022). Anxiety is thought of as an attribute of a higher order factor negative affect (Watson & Clark, 1984). Since, previous research reported, that burn-out has a significant positive correlation with negative affect (Bikar et al., 2017) and resilience is also associated with affectivity (Robinson et al., 2014), it is plausible, that reduction in negative affect is behind the intervention’s effect on burn-out and resilience. Negative affect is predicted by high self-esteem and low perfectionism (O’Brien & Page, 1994). The focus of REST on raising self-efficacy and self-esteem and lowering perfectionism may have had the effect of reduced negative affectivity, which in turn influenced reported levels of burn-out and resilience.
According to a meta-analysis, those interventions that combined skill training with cognitive behavioral elements or those that combined skill training with hypnosis or mindfulness seemed to have the most effect in reducing anxiety (Ergene, 2003). This is the reason the present intervention was designed, so it includes relaxation, visualization and positive suggestions combined with skill training and CBT methods. Undoubtedly not every intervention works for every person, which takes us to personalized solutions in anxiety management. We need to cut the ropes of the current paradigm which is aiming to detangle what are the most useful components of an intervention. We suggest that deciphering what makes different methods work for different people is the next challenge in the field.
One of the difficulties of online interventions is to increase adherence and patient retention. Prior research has suggested minimal phone contact with therapists to encourage program completion (Newman et al., 2011). Telephone interviews, text messages and emails are common and convenient ways to keep people engaged in e-health interventions and supervise therapeutic progress. In REST-TA students had to write a guided self-reflection after the completion of each module which was answered by a trained psychology undergraduate research assistant. This procedure kept the treatment group engaged in the process, which was reflected in the low dropout rate (12.5%). Reiss and colleagues (2019) reported a similarly low dropout rate of 15%. In their study a weekly communication with a counselor was implemented. These low dropout rates are in contrast with the 28% percent dropout rate that was reported by Orbach and colleagues (2007), who did not utilize regular communication. However, the mediating factors of counsellor involvement affecting treatment efficacy still need to be researched thoroughly. Importantly in REST-TA the self-reflections were answered by trained research assistants, who were supposed to provide no more than an empathetic response. This makes REST-TA a scalable option for universities, because any number of students may participate in the program without the extra cost of a therapist.
Limitation
The limitations of the study include the gender homogeneity of our sample. Most of the participants were female with only a few male participants, thus gender differences were not explored in the study. The other limitation of the study is that participants were not blind to what group they were randomized into, and this might have affected their responses. Further limitation is that there were baseline differences between the two groups on two of the factors of the TAMC-SF (Social and the Cognitive interference factors). The Hungarian version of the TAMC- SF is currently under validation. Thus, any conclusion based on results concerning the TAMC- SF should be taken with caution.
Conclusion
The REST-TA program is the first empirically tested relaxation and skill training based online solution to tackle test anxiety. We conclude that REST-TA is effective in reducing test anxiety, improving overall subjective wellbeing and negative affect of university students. This study provides evidence that an 8-week program that requires only about 30–60 min engagement a week is helpful to students. The low dropout rate suggests that regular communication with the students promotes adherence. To improve mental health of students we must take steps to provide solutions to help cope with test anxiety.
Although there is an abundance of self-help online based programs to reduce anxiety, most of those programs are not evidence based. It is paramount that we provide students with evidence based easily accessible structured programs to deal with this pressing issue.
Availability of data and materials
A home-based approach to reduce test anxiety using a combination of methods: a randomized controlled trial.
References
Bassetti, C., Gulino, M., Gazzaniga, V., & Frati, P. (2011). The old roots of the italian health legislation. Mediterranean Journal of Social Sciences, 2(2).
Bikar, S., Marziyeh, A., & Pourghaz, A. (2017). Affective structures among students and their relationship with academic burnout. New Educational Review, 50(4), 47–55. https://doi.org/10.15804/tner.2017.50.4.04.
Bischofsberger, L., Burger, P. H. M., Hammer, A., Paulsen, F., Scholz, M., & Hammer, C. M. (2021). Prevalence and characteristics of test anxiety in first year anatomy students. Annals of Anatomy, 236. https://doi.org/10.1016/j.aanat.2021.151719
Chapell, M. S., Blanding, B., Takahashi, Z., Silverstein, M., Newman, M. E., Gubi, B., A., & McCann, N. (2005). Test anxiety and academic performance in undergraduate and graduate students. Journal of Educational Psychology, 97(2), https://doi.org/10.1037/0022-0663.97.2.268.
Christensen, H., Batterham, P., & Calear, A. (2014). Online interventions for anxiety disorders. Current Opinion in Psychiatry, 27(1), 7–13.
Cuijpers, P., Marks, I. M., van Straten, A., Cavanagh, K., Gega, L., & Andersson, G. (2009). Computer-aided psychotherapy for anxiety disorders: A meta-analytic review. Cognitive Behaviour Therapy, 38(2), 66–82.
Culler, R. E., & Holahan, C. J. (1980). Test anxiety and academic performance: The effects of study-related behaviors. Journal of Educational Psychology, 72(1), 16.
Ergene, T. (2003). Effective interventions on test anxiety reduction: A meta-analysis. School Psychology International, 24(3), https://doi.org/10.1177/01430343030243004. hatósági.pdf. (n.d.).
Griffiths, K. M., Farrer, L., & Christensen, H. (2010). The efficacy of internet interventions for depression and anxiety disorders: A review of randomised controlled trials. Medical Journal of Australia, 192, S4-S11.
Hazag, A., Major, J., & Ádám, S. (2010). A hallgatói kiégés szindróma mérése. A Maslach kiégés-teszt hallgatói változatának (MBI-SS) validálása hazai mintán. Mentalhigiene Es Pszichoszomatika, 11(2), 151–168. https://doi.org/10.1556/Mental.11.2010.2.4. heart_activity.pdf. (n.d.).
Henry, J. D., & Crawford, J. R. (2005). The short-form version of the Depression anxiety stress scales (DASS-21): Construct validity and normative data in a large non-clinical sample. British Journal of Clinical Psychology, 44(2). https://doi.org/10.1348/014466505X29657
Hodge, G. M., McCormick, J., & Elliott, R. (1997). Examination-induced distress in a public examination at the completion of secondary schooling. British Journal of Educational Psychology, 67(2). https://doi.org/10.1111/j.2044-8279.1997.tb01236.x
Hong, E., & Karstensson, L. (2002). Antecedents of state test anxiety. Contemporary Educational Psychology, 27(2), https://doi.org/10.1006/ceps.2001.1095.
Járai, R., Vajda, D., Hargitai, R., Nagy, L., Csókási, K., & Kiss, E. C. (2015). A Connor– Davidson reziliencia kérdőív 10 itemes változatának jellemzői. Alkalmazott Pszichológia, 15(1), 129–136. https://doi.org/10.17627/ALKPSZICH.2015.1.129.
Kavakci, O., Semiz, M., Kartal, A., Dikici, A., & Kugu, N. (2014). Test anxiety prevalance and related variables in the students who are going to take the university entrance examination. Dusunen Adam The Journal of Psychiatry and Neurological Sciences, 27(4), 301.
Krispenz, A., Gort, C., Schültke, L., & Dickhäuser, O. (2019). How to reduce test anxiety and academic procrastination through inquiry of cognitive appraisals: A pilot study investigating the role of academic self-efficacy. Frontiers in Psychology, 10, 1917. https://doi.org/10.3389/fpsyg.2019.01917.
Kondaš, O. (1967). Reduction of examination anxiety and ‘stage-fright’by group desensitization and relaxation. Behaviour Research and Therapy, 5(4), 275–281.
Lattie, E. G., Lipson, S. K., & Eisenberg, D. (2019). Technology and college student mental health: Challenges and opportunities. Frontiers in Psychiatry, 10, https://doi.org/10.3389/fpsyt.2019.00246.
Lewis, C., Pearce, J., & Bisson, J. I. (2012). Efficacy, cost-effectiveness and acceptability of self-help interventions for anxiety disorders: Systematic review. The British Journal of Psychiatry, 200(1), 15–21.
Liebert, R. M., & Morris, L. W. (1967). Cognitive and emotional components of test anxiety: A distinction and some initial data. Psychological Reports, 20(3), 975–978.
Lowe, P. A. (2019a). Exploring cross-cultural and gender differences in test anxiety among
Lowe, P. A. (2019b). Examination of test anxiety in samples of australian and U.S. higher education students. Higher Education Studies, 9(4), https://doi.org/10.5539/hes.v9n4p33.
Lowe, P. A. (2021). The test anxiety measure for College Students-Short Form: Development and examination of its psychometric properties. Journal of Psychoeducational Assessment.39. (2). https://doi.org/10.1177/0734282920962947
Lyu, C., Ma, R., Hager, R., & Porter, D. (2022). The relationship between resilience, anxiety, and depression in chinese collegiate athletes. Frontiers in Psychology, 13(August), 1–14. https://doi.org/10.3389/fpsyg.2022.921419.
Mandler, G., & Sarason, S. B. (1952). A study of anxiety and learning. The Journal of Abnormal and Social Psychology, 47(2), 166–173. https://doi.org/10.1037/h0062855.
Mccraty, R., Atkinson, M., & Lipsenthal, L. (2000). Emotional self-regulation program enhances psychological health and quality of life in patients with diabetes.
Mistler, B. J., Services, H., Reetz, D. R., Services, C., Krylowicz, B., Services, C., & Barr, V. (2012). The Association for University and College Counselling Center Directors Annual Survey. Retrieved from http://www.unccd.int/en/programmes/Event-and- campaigns/Dryland Champions/dryland_champions_2014/Pages/Eritrea.aspx
Morris, L. W., & Liebert, R. M. (1970). Relationship of cognitive and emotional components of test anxiety to physiological arousal and academic performance. Journal of Consulting and Clinical Psychology, 35(3), 332.
Mowbray, C. T., Megivern, D., Mandiberg, J. M., Strauss, S., Stein, C. H., & Collins, K., … Lett R. Campus mental health services: Recommendations for change. American Journal of Orthopsychiatry, Vol. 76. https://doi.org/10.1037/0002-9432.76.2.226
Naveh-Benjamin, M., McKeachie, W. J., & Lin, Y. (1987). Two types of test-anxious students: Support for an information processing model. Journal of Educational Psychology, 79(2), 131–136. https://doi.org/10.1037/0022-0663.79.2.131.
Newbegin, I., & Owens, A. (1996). Self-esteem and anxiety in secondary school achievement. Journal of Social Behavior and Personality, 11(3).
Newman, M. G., Szkodny, L. E., Llera, S. J., & Przeworski, A. (2011). A review of technology- assisted self-help and minimal contact therapies for anxiety and depression: Is human contact necessary for therapeutic efficacy? Clinical Psychology Review, 31, https://doi.org/10.1016/j.cpr.2010.09.008.
Ng, A., & Lovibond, P. F. (2020). Self-efficacy moderates the relationship between avoidance intentions and anxiety. Emotion, 20(6), https://doi.org/10.1037/emo0000594.
Nottelmann, E. D., & Hill, K. T. (1977). Test anxiety and off-task behavior in evaluative situations. Child Development, 225–231.
O’Brien, S., & Page, S. (1994). Self-efficacy, perfectionism, and stress in canadian nurses. The Canadian Journal of Nursing Research = Revue Canadienne de Recherche En Sciences Infirmieres, 26, 49–61.
Orbach, G., Lindsay, S., & Grey, S. (2007). A randomised placebo-controlled trial of a self-help internet-based intervention for test anxiety. Behaviour Research and Therapy, 45(3), https://doi.org/10.1016/j.brat.2006.04.002.
Prato, C. A. (2009). Biofeedback assisted relaxation training program to decrease test anxiety in nursing students.
Reiss, N., Warnecke, I., Tibubos, A. N., Tolgou, T., Luka-Krausgrill, U., & Rohrmann, S. (2019). Effects of cognitive-behavioral therapy with relaxation vs. imagery rescripting on psychophysiological stress responses of students with test anxiety in a randomized controlled trial. Psychotherapy Research, 29(8), 974–985.
Robinson, J. S., Larson, C. L., & Cahill, S. P. (2014). Relations between resilience, positive and negative emotionality, and symptoms of anxiety and depression. Psychological Trauma: Theory Research Practice and Policy, 6(Suppl 1), https://doi.org/10.1037/a0033733.
Sarason, I. G. (1959). Intellectual and personality correlates of test anxiety. Journal of Abnormal and Social Psychology, 59(2), 272–275. https://doi.org/10.1037/h0042200.
Sarason, B. R., Sarason, I. G., & Pierce, G. R. (1990). Traditional views of social support and their impact on assessment. Wiley Series on personality processes. Social support: An interactional view (pp. 9–25). Oxford, England: John Wiley & Sons.
Schaufeli, W. B., Martinez, I. M., Pinto, A. M., Salanova, M., & Bakker, A. B. (2002). Burnout and engagement in university students: A cross-national study. Journal of Cross-cultural Psychology, 33(5), 464–481.
Sommer, M., & Arendasy, M. E. (2015). Further evidence for the deficit account of the test anxiety-test performance relationship from a high-stakes admission testing setting. Intelligence, 53. https://doi.org/10.1016/j.intell.2015.08.007
Spielberger, C. D. (1962). The effects of manifest anxiety on the academic achievement of college students. Mental Hygiene, 46, 420–426.
Spielberger, C. D. (1983). Manual for the State-Trait Anxiety Inventory STAI (Form Y). Palo Alto, CA: Consulting Psychologists Press.
Spielberger, C. D., & Vagg, P. R. (1995). Test anxiety: A transactional process model. Series in Clinical and Community psychology. Test anxiety: Theory, assessment, and treatment (pp. 3–14). Philadelphia, PA, US: Taylor & Francis.
Spielberger, C., Gorsuch, R., & Lushene, R. (1970). STAI manual for the state-trait anxiety inventory. Self-Evaluation Questionnaire. In Lushene Consulting Psychologists Press.
Thomas, C. L., Cassady, J. C., & Heller, M. L. (2017). The influence of emotional intelligence, cognitive test anxiety, and coping strategies on undergraduate academic performance. Learning and Individual Differences, 55, 40–48.
Turner, B. G., Beidel, D. C., Hughes, S., & Turner, M. W. (1993). Test anxiety in African American school children. School Psychology Quarterly, 8, 140–152. https://doi.org/10.1037/h0088835
von der Embse, N., Jester, D., Roy, D., & Post, J. (2018). Test anxiety effects, predictors, and correlates: A 30-year meta-analytic review. Journal of Affective Disorders, 227, https://doi.org/10.1016/j.jad.2017.11.048.
Warnecke, I., Haffinger, L. M., Konradi, H., Reiss, N., Luka-Krausgrill, U., & Rohrmann, S. (2020). Design of a guided internet-delivered counseling intervention for test anxiety. The European Journal of Counselling Psychology, 8(1), https://doi.org/10.5964/ejcop.v8i1.205.
Watson, D., & Clark, L. A. (1984). Negative affectivity: The disposition to experience aversive emotional states. Psychological Bulletin, 96(3), https://doi.org/10.1037/0033-2909.96.3.465.
Xiao, H., Carney, D. M., Youn, S. J., Janis, Hayes, J. A., & Locke, B. D. Are we in crisis? National mental health and treatment trends in college counseling centers. Psychological Services, 14(4). https://doi.org/10.1037/ser0000130
Zargarzadeh, M., & Shirazi, M. (2014). The effect of progressive muscle relaxation method on test anxiety in nursing students. Iranian Journal of Nursing and Midwifery Research, 19(6), 607–612.
Zeidner, M. (2010, January 30). Test Anxiety. The Corsini Encyclopedia of Psychology, pp. 1–3. https://doi.org/10.1002/9780470479216.corpsy0984
Acknowledgements
This work was accomplished with support of the Hungarian Academy of Sciences (through project: LP-2018-21/2018. We are grateful for support of the Faculty of Education and Psychology, ELTE Eötvös Loránd University, Budapest, Hungary.
Funding
Open access funding provided by Eötvös Loránd University.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationship that could be construed as a potential conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Csirmaz, L., Vikor, F., Szekely, A. et al. A Home-based Approach to Reduce Test Anxiety Using a Combination of Methods: A Randomized Controlled Trial. J Rat-Emo Cognitive-Behav Ther 42, 322–338 (2024). https://doi.org/10.1007/s10942-023-00512-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10942-023-00512-3