
Abstract
Purpose
Many countries have developed clinical decision-making support tools, such as the smart work injury management (SWIM) system in Hong Kong, to predict rehabilitation paths and address global issues related to work injury disability. This study aims to evaluate the accuracy of SWIM by comparing its predictions on real work injury cases to those made by human case managers, specifically with regard to the duration of sick leave and the percentage of permanent disability.
Methods
The study analyzed a total of 442 work injury cases covering the period from 2012 to 2020, dividing them into non-litigated and litigated cases. The Kruskal–Wallis post hoc test with Bonferroni adjustment was used to evaluate the differences between the actual data, the SWIM predictions, and the estimations made by three case managers. The intra-class correlation coefficient was used to assess the inter-rater reliability of the case managers.
Results
The study discovered that the predictions made by the SWIM model and a case manager possessing approximately 4 years of experience in case management exhibited moderate reliability in non-litigated cases. Nevertheless, there was no resemblance between SWIM’s predictions regarding the percentage of permanent disability and those made by case managers.
Conclusion
The findings indicate that SWIM is capable of replicating the sick leave estimations made by a case manager with an estimated 4 years of case management experience, albeit with limitations in generalizability owing to the small sample size of case managers involved in the study.
Implications
These findings represent a significant advancement in enhancing the accuracy of CDMS for work injury cases in Hong Kong, signaling progress in the field.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Prolonged worker absence from work due to injury is a global concern that has been on the rise in recent years. From 2010 to 2020, the number of days lost due to work-related injuries increased by 42% in 64 surveyed countries, totalling approximately 62.5 million days [1]. From 2010 to 2016, the number of days lost in Hong Kong remained relatively stable at approximately 300,000 days per year [1]. In 2021, there were 30,185 non-fatal occupational injuries in Hong Kong [2]. This phenomenon of enormous loss of days has led to lost wages, lower productivity, and higher permanent disability. In addition, work injuries have created a public health concern [3] and have indicated the need for injury prevention or health and safety reinforcement for workers in the future.
In Hong Kong, protracted waiting periods for medical consultations and rehabilitation interventions, especially with orthopedic specialists at public hospitals, significantly impede the recuperation of injured employees. This delay in obtaining essential medical care aggravates the consequences of injuries. Furthermore, the escalating demand for rehabilitation services exerts pressure on the public healthcare system, complicating the provision of prompt and sufficient assistance to injured workers. In response to these challenges, various rehabilitation initiatives, including the Volunteer Rehabilitation Programme (VRP) [4], the Multi-disciplinary Orthopaedics Rehabilitation Empowerment (MORE) program [5], and the Pilot Rehabilitation Programme for Employees Injured at Work [6], have been established to mitigate these issues. These initiatives prioritize case management and early intervention strategies to guarantee swift and efficient delivery of rehabilitation services.
Case Management in Hong Kong
Case management has a rich history dating back to 1863 in the United States [7]. In 1995, Martin described case management as “a systematic approach to coordination of services to suitable clients through efforts of assessing providers, treatments, and developing treatment plans which improve quality and efficacy while controlling costs and monitoring outcomes” [8]. The case management model has been effective in reducing the number of lost days, medical costs, and claim costs [9], and importantly, it enhances continuity of case management and promoted efficient reintegration of employees into the workplace [10]. Therefore, over the last 20 years, many employers and insurers in Hong Kong have adopted the case management approach in managing work injury cases to reduce work disability in terms of sick leave days and permanent disability percentage (PD%). In Hong Kong, case management encounters obstacles stemming from a high rate of staff turnover and a deficiency of seasoned case managers. Consequently, this situation leads to novices, lacking formal training or qualifications, managing complex cases.
Case managers play a vital role in estimating reserves for work injury cases. A reserve is defined as funds set aside by an insurance company to meet future obligations as they become due. These obligations include liabilities for unearned premiums and the estimated costs of unpaid claims [10]. Insurance companies earmark reserves to guarantee ample funds are available for policyholders' claims. The precision of these estimates’ hinges on the case manager's competence in evaluating the number of sick leave days and the percentage of permanent disability (PD%). Lack of experience among case managers can compromise the accuracy of reserve estimations and influence the formulation of rehabilitation plans. The distinct reserving guidelines of insurance companies, coupled with the varied quality and experience of case managers, further affect the accuracy of reserves. Additionally, an accurate disability prognosis is pivotal in work injury cases, as it shapes decisions regarding medical interventions, allocation of resources, and the compensation reserved by insurers for such events [11, 12]. An inaccurate estimation of the prospective outcome of an injury can negatively affect the worker's recovery trajectory [13]. Artificial intelligence-powered clinical decision tools for disability forecasting enhance consistency and mitigate the risk of inaccurate medical assessments [14, 15].
Clinical Decision-Making Support Tools
Clinical decision-making support (CDMS) tools, widely used in various medical areas, have shown potential for improving outcomes such as ambulatory/primary care [16] and genetics healthcare [17]. Nevertheless, further studies are needed to evaluate the results and to determine effective implementation. However, their application in work injury rehabilitation remains limited. A few predictive models have been developed in the industry, but these models have not yet been widely used. Predictive models the Work Assessment Triage Tool (WATT) [18, 19] the gradient boosting machine (GBM) [20] offer potential but need further validation. The Smart Work Injury Management (SWIM) system, developed in Hong Kong, utilizes artificial intelligence to predict return-to-work trajectories and provide advice on medical care and interventions [21, 22]. Unfortunately, there has been no validation study to show its accuracy. Therefore, the objective of this study is to evaluate the accuracy of SWIM as a clinical decision support tool for forecasting work disability in injured workers. By juxtaposing predicted values with estimations made by case managers, the study seeks to gauge SWIM's suitability for industry application and pinpoint its limitations.
Method
Designs
This study used the severity model of the SWIM system (version 1.0) (Fig. 1) to predict sick leave days, PD%, Medical Assessment Board (MAB) days, whether a case requires high-level management (HLM), and return-to-work (RTW) days. The study only used the sick leave days and PD% results for analysis. SWIM requires five mandatory data points to produce a prediction: age, gender, injured body part, nature of injury, and cause of injury. Other optional information that can be inputted includes industry, position, and salary. Physical demand level, alertness, and frequency of manual handling operations are preset and appear on the mandatory data input. These preset fields can be adjusted manually on the basis of the particular situation of a case. In this study, we compared the sick leave days and PD% predictions of the SWIM system with the estimations of three case managers (CMs) with different levels of case management experience and backgrounds: CM-A, a female with 4 years of work injury case management experience and an academic background in marketing; CM-B, a female with 9 years of case management experience and a registered nurse; and CM-C, a female with approximately 20 years of experience and a legal background. CM-B and CM-C were working in the same company at the time of the data collection (Table 1). Since the total number of cases used was 442, only three case managers agreed to participate voluntarily in the study due to the long length of time required for the estimations. Case managers were provided with data for 442 cases in an Excel format, which included an index number starting from 1 to 442, occupation, physical demand level, age at the date of the accident, gender, alertness, injured body part, nature of the injury, cause of injury, and the frequency of Manual Handling Operation for estimating sick leave and PD% (permanent disability percentage). The directive given to the three case managers was to assess each case as if it were newly reported, and to estimate the initial sick leave in months and the PD% that might be awarded following a medical assessment by the Employees’ Compensation (Ordinary Assessment) Board in Hong Kong. No further discussions or surveys were conducted by the case managers.

User interface of SWIM
Participants
The data were extracted from the claims database of an insurance company in Hong Kong. A total of 546 claims covering the period between 2012 and 2020 were initially identified; 104 of these cases were not valid and were excluded because they were either fatal cases, cases with no claim form, or cases with insufficient information. The remaining 442 work injury cases (mean age = 45.9; male = 397 and female = 55) were adopted for this study. The data contained the following information about the cases: the demographic information (occupation, age at the date of accident, and gender) of the injured workers (Table 2), information on physical demand level, alertness, injured body part, nature of the injury, cause of injury, frequency of manual handling operations, actual sick leave, and actual PD%. PD% data were available for 267 of the 442 cases, and all cases contained data on the actual sick leave days taken by the injured workers. At the time of the data collection, these cases were at different stages. A total of 332 out of the 442 cases involved employees’ compensation litigation proceedings and 110 were non-litigation cases.
Procedures
All mandatory and available optional data were inputted into SWIM. The predicted sick leave days and PD% were recorded for the 442 cases as the experimental group. The same set of data was given to CM-A, CM-B, and CM-C, without knowing the results from SWIM, as the control group. The case managers estimated the sick leave days and the PD% on the basis of the case information provided. Then, the SWIM projected values were compared with the estimations made by the case managers and the actual cases.
The analysis was separated into a group of 110 non-litigated cases and a group of 332 litigated cases. There were 442 cases with data on sick leave days and 273 with PD% data. A litigated case was defined as a case where the injured worker had filed a civil litigation claim against their employer. First, the Shapiro–Wilk test was used to assess the normality of the dataset using Statistical Package for the Social Science (SPSS) version 28 [23]. The test indicated that the sick leave days and PD% data were not distributed normally. Therefore, the Kruskal–Wallis post hoc test with Bonferroni correction was utilized to assess the significant difference between the actual cases, SWIM, and the case managers. The Kruskal–Wallis test is the non-parametric equivalent of a one-way ANOVA and is used for testing whether samples originate from the same distribution [24]. The test was followed by the post hoc Dunn–Bonferroni test to identify the pairwise significant difference from each group by adjusting the alpha level in reducing the type 1 error [25]. Dunn’s test has proved popular over the past two decades, and the test is frequently used with multiple comparison adjustments [24]. Thirdly, the intra-class correlation coefficient (ICC) was selected to test the inter-rater reliability of the predictions across different case managers. ICCs with 95% confidence intervals were calculated using IBM SPSS version 28.0.0.0 (190) based on a mean-rating (k = 3), absolute agreement, 2-way mixed-effects model (model 3) [25]. The ICC is a value between 0 and 1, where values below 0.5 indicate poor reliability, values between 0.5 and 0.75 indicate moderate reliability, values between 0.75 and 0.9 indicate good reliability, and any value above 0.9 indicates excellent reliability [26, 27]. Further analysis will be conducted for the distribution of sick leave days and PD% by the nature of injury.
Results
Sick Leave Days
Kruskal–Wallis Test
The Shapiro–Wilk test showed that the distributions were statistically significantly (p < 0.001) non-normal for all the data, including both sick leave days and PD%. Therefore, the Kruskal–Wallis test was used to assess the similarity between the actual data, SWIM predictions, and the estimations produced by the three case managers. The null hypothesis for the Kruskal–Wallis test is that the population medians of the groups are equal. A non-rejection of the null hypothesis signifies that two or multiple groups are significantly similar. Post hoc test with Bonferroni adjustment was adopted for making pair-wise comparisons [24]. The evaluation targeted two distinct groups: (1) non-litigated cases and (2) litigated cases, with the findings displayed in Table 3. For the non-litigated cases, the Kruskal–Wallis test indicated that three pairwise comparisons did not reject the null hypothesis, thereby suggesting that the populations of these pairs were statistically significantly equivalent: (1) CM-A & SWIM (p = 0.507); (2) CM-B and the actual data (p = 0.109); and (3) CM-C and CM-B (p = 0.215). For the litigated cases, only CM-B and CM-C failed to reject the null hypothesis (p = 0.153).
Intraclass Correlation Coefficient (ICC)
Using the ICC, the inter-rater reliability of the SWIM predictions was tested across different case managers for sick leave days (Table 4). The test showed moderate reliability between SWIM and CM-A (ICC = 0.637, p < 0.001), CM-A and CM-C (ICC = 0.642, p < 0.001), and CM-A and CM-B (ICC = 0.581, p < 0.001) for non-litigated cases. CM-B and CM-C demonstrated good reliability for both non-litigated and litigated cases respectively (ICC = 0.837, p < 0.001; ICC = 0.845, p < 0.001).
Permanent Disability Percentage
The SWIM system’s predictions on PD% had no similarity across all groups, irrespective of whether the cases were litigated or non-litigated (Table 5). However, the actual data were similar when compared with CM-A (p = 0.289) and CM-B (p = 0.158) for non-litigated cases and with CM-C (p = 0.324) for litigated. The PD% among CM-A, CM-B, and CM-C was significantly similar in their respective comparisons: (1) CM-A & CM-B (p = 0.289); (2) CM-A & CM-C (p = 0.052); CM-B & CM-C (p = 0.112). CM-B and CM-C are similar to each other for both type of cases (p = 0.112 non-litigated; p = 0.119 litigated).
Other Results
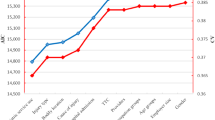
Table 6 presented the average number of sick leave days and the percentage of permanent disability (PD%) by different case types. Additionally, Fig. 2 elucidated that Case Manager B (CM-B) and Case Manager C (CM-C) estimated a higher average number of sick leave days for non-musculoskeletal injuries, such as burns, concussions, or electric shocks, and for severe injuries, including amputations, dislocations, and multiple injuries. The distribution further revealed that the estimations deviated from the actual data in the sequence of CM-C, CM-B, SWIM, and CM-A. The proximity distribution for SWIM and CM-A, as well as CM-B and CM-C, aligned with the findings of this study.

Average sick leave days by nature of injury across actual data, SWIM, CM-A, CM-B, and CM-C
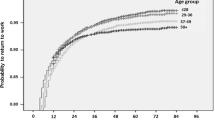
Subsequently, Fig. 3 illustrated that the average PD% predicted by SWIM remained relatively consistent across different types of injuries, corroborating the Kruskal–Wallis test result that it exhibited no similarity across all groups. The boxplot in Fig. 3 was based on the Actual PD%.

Average permanent disability percentage by nature of injury across actual data, SWIM, CM-A, CM-B, and CM-C
Discussion
The evaluation of the SWIM system's accuracy within this study revealed that its predictions for sick leave days were comparable to those made by Case Manager A (CM-A) for non-litigated cases, with the inter-rater reliability analysis indicating moderate reliability among these comparisons. Moreover, the assessments provided by Case Manager B (CM-B) and Case Manager C (CM-C) showed significant similarity and demonstrated robust reliability for both non-litigated and litigated cases. When it comes to predicting the percentage of permanent disability (PD%), SWIM's forecasts exhibited significant divergence from all groups, when dealing with types of injuries for which the AI has not been sufficiently trained. This discrepancy highlights the importance of a comprehensive training dataset for AI systems like SWIM, ensuring they are well-equipped to accurately predict outcomes across a wide range of injury types. The limitations in SWIM's predictive accuracy for less common or more complex injuries suggest that enhancing the AI's training with a broader spectrum of case types could improve its utility and reliability in clinical decision support. Although the study's generalizability may be impacted by the small number of case managers involved, the findings represent a significant progress in improving the accuracy of CDMS for handling work injury cases in Hong Kong. This advancement is critical for enhancing the support and rehabilitation process for injured workers, contributing to more efficient and effective case management practices in the region.
The similarity between the average number of sick leave days estimated by Case Manager A (CM-A) and SWIM underscores a key outcome of this study: SWIM's predictions of sick leave days were closely aligned with those made by CM-A, who possessed approximately 4 years of case management experience. This correlation was not observed with Case Manager B (CM-B) and Case Manager C (CM-C), who have 9 and 20 years of experience, respectively. All three case managers performed their assessments without prior knowledge of whether a case was non-litigated or litigated, relying solely on the same dataset as SWIM. This approach highlighted a significant variance among the case managers, with CM-A's estimations paralleling SWIM's, whereas CM-B and CM-C's estimates diverged. This disparity may be attributed to several factors, including differences in years of experience, academic backgrounds, and the companies for which they work. A notable factor could be the divergent reserving guidelines adopted by their respective companies. CM-B and CM-C were employed by the same company, likely utilizing a consistent set of guidelines and estimation approaches, whereas CM-A worked for a different firm with unique reserving criteria. Such internal guidelines can vary significantly, affecting the weighting of case information and the overall estimation process. Additionally, the methodology applied in adhering to these guidelines may further contribute to variability in estimates. The observed differences in estimation patterns for non-musculoskeletal injuries between “SWIM and CM-A” versus “CM-B and CM-C” suggest distinct algorithmic approaches or considerations between these groups. Yet, the study does not specify the algorithms or methodologies used by each group. This ambiguity underscores the need for further research to elucidate the various considerations case managers might employ in their initial estimates, particularly for non-musculoskeletal injuries, and to explore the implications of these findings for the development and implementation of AI tools like SWIM in clinical and insurance settings.
Figure 2 further elucidates significant discrepancies in the estimated sick leave days between SWIM, CM-A, CM-B, CM-C, and the actual data. The actual data, derived from cases that have been resolved, were utilized retrospectively to assess the accuracy of SWIM. This indicates that the real cases evolved over a certain period, culminating in a longer duration of sick leave than initially predicted. Such differences imply the influence of various factors throughout the case's progression. Numerous studies have identified that, as cases advance, a variety of psychosocial factors emerge, potentially impacting the trajectory of these cases and leading to prolonged sick leave, thereby affecting the return-to-work outcomes [28,29,30,31]. These factors may include cases becoming legal matters [32, 33], the injured employees’ self-perception on employment readiness and maintaining a belief that they were unfit for work [34, 35], developing a compensation-oriented mindset rather than a recovery-oriented [36,37,38,39] or adopting a ‘sick role’ such as the Parsonian Model [40]. It is critical to highlight that the case managers in this study made initial sick leave estimations without accounting for psychosocial factors. They were not provided with information regarding the injured employees' self-perceptions about returning to work, nor whether they had legal representation. The case managers relied solely on their judgment, informed by their background and experience, to assess each case. Moreover, the prognosis estimation often hinges on the case manager's experienced judgment. The identification of high-risk factors might alter the trajectory of individual cases as more information is gathered from the injured employee or as the case evolves. A key responsibility of case managers is to develop a case management plan that outlines the direction and frequency of treatment, aiming to facilitate the injured worker's recovery at the minimum possible cost. The training, experience, and access to information of case managers play a significant role in determining the quality of the case management plan [41] and the selection of skilled nurse case managers also helped facilitate the implementation of a successful case management interventions [42]. The other qualitative study from Yanar et al. noted that case managers’ different perceptions of “early” return to work differed the case trajectory despite the agreement on encouraging return to work [43]. Therefore, a case manager’s experience, knowledge, and further case information contents to be obtained has influence on the case prognosis estimation or psychosocial factors identification. Further research is suggested to find out the potential factors that contributing to this identified difference.
It was unexpected that the SWIM’s prediction on PD% were different (p ≤ 0.001) across the 3 case managers. Nevertheless, the estimations made by the three case managers align closely with the actual data for CM-A and CM-B in non-litigated cases, and for CM-C in litigated cases. Figure 3 provides additional support for this assertion. Injuries such as fractures, contusions and bruises, and amputations were among the most accurately predicted types of injury by these groups, excluding SWIM. This observation, in conjunction with the findings related to sick leave days, suggests that the percentage of permanent disability (PD%) estimated by humans might not be significantly influenced by the progression of the case. However, the duration of sick leave may extend as cases progress through various stages of incidents, a conclusion supported by previous research.
It is essential to acknowledge the diversity of factors that case managers, varying in experience and background, might take into account when predicting the prognosis of an injury. Case management embodies a multifaceted process, entwined with a plethora of human elements and disparate responses from injured workers. Given the distinct nature of each work injury case's rehabilitation trajectory, it underscores the importance of ongoing endeavors to emulate human judgment in this domain. Consequently, enhancing the fidelity of simulations to approximate human estimations more closely is highly recommended to improve outcomes in case management.
Limitations
The development of SWIM provides a valuable tool for clinical decision-making in Hong Kong, particularly for predicting work injury rehabilitation and sick leave days in non-litigated cases. However, there is room for SWIM to improve its accuracy in replicating the expertise of more experienced case managers, thereby addressing the resource shortage in the market. Despite the absence of psychosocial factors in the data provided to case managers, these factors are often considered by case managers due to their historical case handling experience. Given the jurisdiction of Hong Kong, it is common for injured workers to file litigation claims, which typically have a significant impact on return to work and compensation. Therefore, it is recommended that clinical decision-making tools in Hong Kong incorporate psychosocial factors, including litigation risk, when devising treatment plans. Medical treatment outcomes are notoriously poor in patients with pending litigation following disability claims, especially those covered by workers’ compensation programs [44]. Consequently, this study suggests further research on work injury rehabilitation predictions, specifically examining or considering psychosocial factors.
Furthermore, the limited number of case managers involved in this study (n = 3) raises concerns regarding the generalizability and scalability of the findings. The modest sample size may not sufficiently represent the wider community of case managers likely to interact with the SWIM system. Case managers hail from varied backgrounds, possess different levels of expertise, and operate within distinct environments, all of which could affect their viewpoints and engagement with the system. Consequently, the system's efficacy and performance might differ when deployed among a more extensive cohort of case managers in real-world scenarios. To corroborate and expand upon the conclusions of this study, future research endeavors should involve a larger and more varied group of case managers.
Conclusion
Work injury rehabilitation is an issue of international importance, and this study aimed to assess the accuracy of the SWIM system, a clinical decision-support tool, in the context of Hong Kong. This tool assists case managers in forecasting the work disability outcomes of injured workers. The findings indicated that SWIM's estimations were comparable to those made by a case manager with approximately 4 years of case management experience. Nonetheless, to confirm the applicability of these results more broadly, further research involving a larger cohort of case managers is necessary. Additional studies are also recommended to investigate the factors that arise during case progression, which could enhance the accuracy of predictions in comparison with those made by more experienced case managers or against actual case outcomes. Despite these limitations, this study marks a significant advancement for Clinical Decision Management Systems (CDMS) developed in Hong Kong. With the demonstrated success of CDMS in predicting disability outcomes for work injury cases, this technology could address the critical needs for accurate case estimations for reserve allocation and the planning of rehabilitation services for injured employees.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
ILOSTAT data tools to find and download labour statistics. In: ILOSTAT. https://ilostat.ilo.org/data/. Accessed 2 Dec 2023.
Legislative Council. Hong Kong’s occupational safety performance in the first half of 2022. https://www.legco.gov.hk/yr2023/english/panels/mp/papers/mp20230221cb2-138-5-e.pdf. 2023. Accessed 2 Dec 2023.
Tompa E, Mofidi A, van den Heuvel S, van Bree T, Michaelsen F, Jung Y, Porsch L, van Emmerik M. Economic burden of work injuries and diseases: a framework and application in five European Union countries. BMC Public Health. 2021;21(1):1.
Labour Department of Hong Kong. voluntary rehabilitation programme for employees injured at work. https://www.labour.gov.hk/eng/public/ecd/WorkInjuries2.htm. Accessed 2 Dec 2023.
Law SW, Szeto GP, Chau WW, Chan C, Kwok AW, Lai HS, Lee RK, Griffith JF, Hung LK, Cheng JC. Multi-disciplinary orthopaedics rehabilitation empowerment (MORE) program: a new standard of care for injured workers in Hong Kong. J Back Musculoskelet Rehabilit. 2016;29(3):503–13.
Pilot rehabilitation programme for employees injured at work. https://www.prp-wiro.gov.hk/tc/index.htm. Accessed 2 Dec 2023.
Kersbergen AL. Case management: a rich history of coordinating care to control costs. Nurs Outlook. 1996;44(4):169–72.
Dees JP, Anderson N. Case management. AAOHN J. 1996;44(8):385–90.
Iles R, Wyatt M, Pransky G. Multi-faceted case management: reducing compensation costs of musculoskeletal work injuries in Australia. J Occup Rehabilit. 2012. https://doi.org/10.1007/s10926-012-9364-2.
Dooley Lucenti Insurance reserves: what are they and how do they work? https://dooleylucenti.ca/insurance-reserves-what-are-they-and-how-do-they-work/
Snoeck-Krygsman SP, Schaafsma FG, Donker-Cools BH, Hulshof CT, Jansen LP, Kox RJ, Hoving JL. The perceived importance of prognostic aspects considered by physicians during work disability evaluation: a survey. BMC Med Inform Decis Mak. 2022;22(1):25.
Cancelliere C, Donovan J, Stochkendahl MJ, Biscardi M, Ammendolia C, Myburgh C, Cassidy JD. Factors affecting return to work after injury or illness: best evidence synthesis of systematic reviews. Chiropr Man Ther. 2016;24:1–23.
Trippolini MA, Young AE, Pransky G, Elbers NA, Lockwood K, Cameron ID. Beyond symptom resolution: insurance case manager’s perspective on predicting recovery after motor vehicle crash. Disabil Rehabilit. 2021;43(4):498–506.
Harish V, Morgado F, Stern AD, Das S. Artificial intelligence and clinical decision making: the new nature of medical uncertainty. Acad Med. 2021;96(1):31–6.
American Hospital Association (AHA). How AI is improving diagnostics, decision-making and care. AHA [Internet]. [cited 2024 Jan 16]. www.aha.org.
Bryan CJ, Boren SA. The use and effectiveness of electronic clinical decision support tools in the ambulatory/primary care setting: a systematic review of the literature. Inform Prim Care. 2008;16(2):79–91.
Sebastian A, Carroll JC, Oldfield L, Mighton C, Shickh S, Uleryk E, Bombard Y. Effect of genetics clinical decision support tools on health-care providers’ decision making: a mixed-methods systematic review. Genet Med. 2021;23(4):593–602.
Gross DP, Steenstra IA, Shaw W, Yousefi P, Bellinger C, Zaïane O. Validity of the work assessment triage tool for selecting rehabilitation interventions for workers’ compensation claimants with musculoskeletal conditions. J Occup Rehabilit. 2019;30(3):318–30.
Qin Z, Armijo-Olivo S, Woodhouse LJ, Gross DP. An investigation of the validity of the work assessment triage tool clinical decision support tool for selecting optimal rehabilitation interventions for workers with musculoskeletal injuries. Clin Rehabilit. 2015;30(3):277–87.
Na K-S, Kim E. A machine learning-based predictive model of return to work after sick leave. J Occup Environ Med. 2019;61(5):191–9.
Cheng AS, Ng PH, Sin ZP, Lai SH, Law SW. Smart work injury management (SWIM) system: artificial intelligence in work disability management. J Occup Rehabilit. 2020;30(3):354–61.
Ng PH, Chen PQ, Sin ZP, Lai SH, Cheng AS. Smart work injury management (SWIM) system: a machine learning approach for the prediction of sick leave and rehabilitation plan. Bioengineering. 2023;10(2):172.
King AP, Eckersley RJ. Statistics for biomedical engineers and scientists: how to visualize and analyze data. 1st ed. Cambridge: Academic Press; 2019.
Ostertagová E, Ostertag O, Kováč J. Methodology and application of the Kruskal-Wallis test. Appl Mech Mater. 2014;611:115–20.
EasyMedStat. Dunn-Bonferroni post-hoc test. n.d. https://help.easymedstat.com/support/solutions/articles/77000536997-dunn-bonferroni-post-hoc-test#:~:text=The%20purpose%20of%20the%20Dunn,pairs%20of%20means%20being%20compared
Bobak C, Barr P, O’Malley A. Estimation of an inter-rater intra-class correlation coefficient that overcomes common assumption violations in the assessment of health measurement scales. BMC Med Res Methodol. 2018;18:93.
Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–63.
Besen E, Young AE, Shaw WS. Returning to work following low back pain: towards a model of individual psychosocial factors. J Occup Rehabilit. 2014;25(1):25–37.
Marom BS, Ratzon NZ, Carel RS, Sharabi M. Return-to-work barriers among manual workers after hand injuries: 1-year follow-up cohort study. Arch Phys Med Rehabilit. 2019;100(3):422–32.
Bailey TS, Dollard MF, McLinton SS, Richards PA. Psychosocial safety climate, psychosocial and physical factors in the aetiology of musculoskeletal disorder symptoms and workplace injury compensation claims. Work Stress. 2015;29(2):190–211.
Eggert S. Psychosocial factors affecting employees’ abilities to return to work. AAOHN J. 2010;58(2):51–5.
Casey PP, Feyer AM, Cameron ID. Associations with legal representation in a compensation setting 12 months after injury. Injury. 2015;46(5):918–25.
Murgatroyd DF, Casey PP, Cameron ID, Harris IA. The effect of financial compensation on health outcomes following musculoskeletal injury: systematic review. PLoS ONE. 2015;10(2):e0117597.
Li-Tsang CW, Chan HH, Lam C, Lo-Hui KY, Chan CC. Psychosocial aspects of injured workers’ returning to work (RTW) in Hong Kong. J Occup Rehabilit. 2007;17(2):279–88.
Booth-Kewley S, Schmied EA, Highfill-McRoy RM, Sander TC, Blivin SJ, Garland CF. A prospective study of factors affecting recovery from musculoskeletal injuries. J Occup Rehabilit. 2014;24(2):287–96.
Rohling ML, Binder LM, Langhinrichsen-Rohling J. Money matters: a meta-analytic review of the association between financial compensation and the experience and treatment of chronic pain. Health Psychol. 1995;14(6):537–47.
Hall R, Hall R. Compensation neurosis: a too quickly forgotten concept? J Am Acad Psychiatry Law. 2006;34(3):313–25.
Mendelson G. ‘Compensation neurosis’ revisited: outcome studies of the effects of litigation. J Psycosomatic Res. 1995;39(6):695–706.
de Moraes VY, Godin K, dos Santos JB, Faloppa F, Bhandari M, Belloti JC. Influence of compensation status on time off work after carpal tunnel release and rotator cuff surgery: a meta-analysis. Patient Saf Surg. 2013. https://doi.org/10.1186/1754-9493-7-1.
Segall A. The sick role concept: understanding illness behavior. J Health Soc Behav. 1976;17(2):162–9.
Henderson MG, Souder BA, Bergman A, Collard AF. Private sector initiatives in case management. Health Care Financ Rev. 1988;1988:89–95.
Hudon C, Bisson M, Chouinard M-C, Delahunty-Pike A, Lambert M, Howse D, Schwarz C, Dumont-Samson O, Aubrey-Bassler K, Burge F, Doucet S, Ramsden VR, Luke A, Macdonald M, Gaudreau A, Porter J, Rubenstein D, Scott C, Warren M, Wilhelm L. Implementation analysis of a case management intervention for people with complex care needs in primary care: a multiple case study across Canada. BMC Health Serv Res. 2023. https://doi.org/10.1186/s12913-023-09379-7.
Yanar B, Kosny A, Lifshen M. Perceived role and expectations of health care providers in return to work. J Occup Rehabilit. 2018;29(1):212–21.
Bellamy R. Compensation neurosis: financial reward for illness as nocebo. Clin Orthop Relat Res. 1997;336:94–106.
Funding
Open access funding provided by The Hong Kong Polytechnic University. This work was supported by a Project on Start-up Fund for New Recruits of The Hong Kong Polytechnic University under account number BE96.
Author information
Authors and Affiliations
Contributions
Yumiki Yeung wrote the main manuscript text. Peter Chen and Peter Ng responsible for the figures and data analysis. Andy Cheng supervised the whole research. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The author has no relevant financial or nonfinancial interests to disclose.
Ethical Approval
The project has been approved by the PolyU Institutional Review Board (PolyU IRB) (or its Delegate) (Reference Number: HSEARS20230818003).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yeung, Y.Y.K., Chen, P.Q., Ng, P.H.F. et al. Evaluation of the Accuracy of the Smart Work Injury Management (SWIM) System to Assist Case Managers in Predicting the Work Disability of Injured Workers. J Occup Rehabil (2024). https://doi.org/10.1007/s10926-024-10199-7
Accepted:
Published:
DOI: https://doi.org/10.1007/s10926-024-10199-7