
Abstract
Purpose
The purpose of this study is to examine the effect of the Estonian active labor market reform in 2016, which introduced a new policy concerning vocational rehabilitation services. As a research question, we investigate how such services may have affected the employment outcomes of people with mental and/or physical impairments.
Methods
Our sample includes 9244 people from 2016 to 2020, with a mean age of 46 years. Due to multiple entries to the services, we have more than 11,000 cases with over 100,000 monthly observations. We use propensity score matching in combination with fixed effects panel regressions to analyze how the completion of the scheduled rehabilitation plan affected monthly employment duration.
Results
Our findings indicate that completing the rehabilitation service results on average in 2.6 months longer post-rehabilitation employment, compared to matched individuals who discontinued the service. This effect was larger when already employed and male participants entered the service, while weaker effects were observed in the case of individuals with only mental disabilities.
Conclusions
Overall, we conclude that while completing the scheduled rehabilitation plan has a positive effect on employment outcomes, still maintaining employment status seems to remain a challenge, based on the relatively modest effect sizes. Thus, we question the economic arguments behind the reform.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
There is a belief that active labor market reforms are based on the premise where having a job is fundamental to human well-being [1]. Unemployment, high depression, anxiety disorders and alcohol abuse [2, 3] may lead individuals to assess their quality of life or self-esteem as lower than employed people [4,5,6]. Thus, it seems that the social benefits from job placement are the core of the active labor market reforms. However, the active labor market reform rhetoric is more related to economic incentive arguments than social cost arguments [7]. The economic cost–benefit concerns of the reform are in the current case mostly related to the employment outcomes, including tax revenues from the latter. In this study, we ask, whether the economic arguments of the 2016 Estonian active labor market reform, introducing vocational rehabilitation services, were justified.
Therefore, this study examines the effect of vocational rehabilitation services reform on the employment outcomes of people with various sensory/communication, physical and mental impairments in Estonia. The reform in 2016 transferred working-age individuals with reduced working capacities from social services and passive labor market policies to active labor market policies, which included different rehabilitation services. It was triggered by the ideological shift from welfare provision, via unemployment benefits and early retirement pensions, to the active provision of labor market services, which support work life. The reform concerned approximately 100,000 people with special needs or disabilities. For describing and organizing information on functioning and disability, the seven-category International Classification of Functioning, Disability and Health (ICF) is implemented, which is referred to as impairments hereinafter (and synonymously used with the term disabilities).
For investigating the effect of rehabilitation services on employment outcomes, we used a register database of over 9000 clients, who received services, such as physiotherapy, psychological counseling and speech therapy, among other services. All of them can be considered as treated clients and the caveat of the data is that there is no control group neither in terms of those who have a legal right for the services and did not apply nor those who applied but were not approved. Propensity score matching (PSM) is applied to overcome the self-selection bias. Month fixed effect regressions are applied to the matched data.
Reform Agenda: From Theory to Empirical Strategies
Reform in 2016
In most countries, increasing employment among the most vulnerable social groups is recognized as a major political challenge related to labor markets and welfare. However, in Estonia and other post-soviet countries, where the dominant political ideology is liberal and the presence of labor unions tends to be smaller, active labor market policies (ALMPs) are relatively new. By using the typology of Bonoli [8], Toots and Lauri [9] argue that among four types of labor market policies, Estonia belongs to the strong–weak category—‘Employment assistance’ type, concentrating ALMPs on placement services, job subsidies, counseling and job search programs. Also, it is argued that from a practical stance, the employment of the disabled in most post-soviet countries is generally categorized as a health and safety concern, instead of a matter related to equal opportunities [10]. The ALMPs are typically associated with low public expenditure, especially in the Nordics, when compared to the OECD average, which thereby justifies the ‘economic incentives’ ideology (see also [7]). Thus, as a part of the OECD policy evaluation package, Estonia has been long time criticized for both low public expenditure on old social risks (i.e., traditional welfare policies) and rudimental active labor market policies [11].
Most Nordics focused policies toward Welfare-to-Work already in the early 2000s, while Estonia implemented a reform in 2016. From a working-age population of over 900,000 [12], the reform targeted more than 100,000 people with disabilities/impairments in Estonia, which make up at least 10% of the country’s working-age population [13]. In the Estonian case, the target group is larger than the OECD average of 6% [14].
Before the reform, these ‘disability-pensioners’ (i.e., people with reduced working capacity) were the recipients of welfare benefits only. The new program transferred the funds for aiding these people from the budget of the Social Ministry to the budget of the independent public institution called the Estonian Unemployment Insurance Fund (agency hereinafter), which is responsible, among other ALMPs, of a diagnostic evaluation, counseling, training and planning of rehabilitation services. However, the reform was partly financed by the European Social Fund as well.
The introduced ALMP—vocational rehabilitation—is a new service implemented by the reform. The assignment to the service is initiated by the client, however, the case is managed and supervised by the agency case manager, who initiates the rehabilitation plan. The latter includes the following steps: (a) assessment of reduced working capacity (based on the International Classification of Functioning, Disability and Health, ICFFootnote 1 and the client´s vocational profile) by a rehabilitation team of at least three specialists (such as a social worker and other experts); (b) work out of an individual rehabilitation plan with clearly defined objectives; (c) mediating rehabilitation services between local service providers and clients; (d) final assessment of the outcomes. However, it is important to note that the assignment of individuals to rehabilitation programs is not disability-specific since the topics covered in these programs include methods of employment-related aid, which are of a universal nature and suitable for different target groups.
In most cases, the rehabilitation service will last for a maximum of 6 months, which includes all phases from the application to the final evaluation of the service. As we observe from the data, the programs are short in length and often the payments to the contractor have been disbursed for a period of 1 or 2 months. The maximum fee for the single service can reach up to 1800 euros, with certain exceptions. However, the total cost of the reform is unknown to the authors.
The programs that are primarily procured from the for-profit sector consist of vocational services and certain medical treatments/therapies (as part of vocational rehabilitation). These medical services aim to address in general mental and/or physical health conditions, which include services such as physiotherapy, occupational therapy, speech therapy and medical counseling by a doctor or a nurse. On the other hand, the purpose of vocational services is to aid individuals more specifically with reduced working capacity in the labor market. For instance, this includes job training, job placement assistance and support to help the individual maintain employment. Altogether, these rehabilitation services aim to increase motivation to work or study, including engagement in the job search. This is also reflected in the legal definition by the Estonian Labour Market Services and Benefits Act, in § 231 (1): “Occupational rehabilitation is a labour market service provided to a person for preparation for working life and commencement or continuation of employment which involves rehabilitation activities established on the basis of § 57 of the Social Welfare Act.” [15]. Moreover, as indicated by the decree of the agency, the ultimate goal is the employment of the individuals.
However, the assessment of the efficacy or (cost–benefit) efficiency of the reform has not been implemented. In policy documents (e.g., [16]) we see that the reform targets macroeconomic indicators such as poverty rate and (long-run) unemployment, but also micro-level outcomes such as increasing employment probability, employability (e.g., skills, job readiness), job quality and productivity. The latent nature of the latter makes evaluation methodologically complex.
What are the Expectations of the Reform?
Counseling is an essential part of rehabilitation services and it is believed that it can positively impact job satisfaction and employment outcomes. However, only two main mechanisms have been argued to channel or mediate this positive effect (see also [17]). Firstly, there is a so-called good working relationship or working alliance—the client’s affective relationship with the therapist, which is, indicating the client's motivation and ability to set goals and agree with the plan [18, 19]. Secondly, promoting self-efficacy is shown to be the mechanism generating positive treatment effects of rehabilitation [20]. It has been long reported that participants with a greater degree of self-efficacy are more likely to attain employment compared with the rest (e.g., [21]). Thus, Bandura’s [22] vocational self-efficacy theory has found support, which is based on four major tasks of vocational rehabilitation: verbal persuasion, emotional arousal, vicarious experience and performance accomplishments.
The evaluation of the outcomes of the rehabilitation services is not that scarce, however, a significant proportion of the quasi-experimental research have a US-centric orientation [23]. Furthermore, the number of studies specifically focused on Europe, such as those examining ALMPs [24] or providing a comprehensive review of methodologically rigorous studies, which include Germany and Norway [25], is relatively limited. Individual studies with quasi-experimental designs can be found in case of Germany [26,27,28], Canada [29] and Sweden [30].
While vocational rehabilitation services are triggered by the evidence-based practice movement in medicine and social sciences (see [17]), it is argued that implementation of a randomized control study is virtually impossible (see [31]). This is because clients self-selectively enter the service and their legal rights for rehabilitation services can vary across countries. In Estonia such legal right to receive these services has been granted to permanent residents of the country, employers and to others staying in the country (under specific circumstances), according to §3 in the Estonian Labour Market Services and Benefits Act [15]. The latter also states that a person is not eligible for rehabilitation in case of no work ability and/or retirement (§ 91). Overall, self-selection and country-specific regulations do not allow randomization across control and treatment groups. Thus, alternative methods and model identification strategies are needed to disentangle the major barrier in deducting rehabilitation treatment effects in the complex environment.
Most correlational/observational studies have applied logistic regressions [32,33,34,35,36,37] and revealed a positive significant effect of the treatment on the increased probability of employment. Also, some heterogeneous effects are found, e.g., gender-specific or service-specific effects (i.e., Kaya [37] indicates that some services may reduce employment and similar is shown also in the case of educational services [38]). However, we have found only a handful of causal identification studies. They have applied machine learning tools such as nonparametric CHAID [39, 40], experimental [41] or quasi-experimental techniques, namely propensity score matching [42] and a comparative meta-analysis assessment studies of vocational rehabilitation [43] or ALPMs in general [24]. In addition to the positive effect found on perceived workability [41], the positive long-run effect has been documented as well [25, 43]. The latter study indicated that schemes with enhanced services, including job-search assistance and training programs, have positive employment effects from 6 to 36 months.
In general, the evidence seems to suggest that vocational rehabilitation has a positive effect on employment outcomes [17, 23, 24, 32], yet few studies demonstrate robust effects [38, 41, 43] and their duration. In addition, there is limited evidence of economic cost-efficiency on it, however, some earlier studies indicate significant positive returns [17, 38, 44].
Results: From Descriptive to Inferential Analysis
Descriptive Analysis
Our register-based longitudinal dataset consists of individual-level observations of vocational rehabilitation for the entire population in the Estonian social service register, from January 2016 to October 2020, which was matched with the employment data in the Estonian working register,. People are eligible for vocational rehabilitation services if they are meeting all the following criteria: (a) age 16 until retirement age (63 in Estonia, gradually increasing towards 65); (b) diagnosis of impairment/disability, indicating reduced working capacity; (c) employed or unemployed as registered job seekers. The database matches the entire population of vocational rehabilitation clients to their employment data from the employment registry and other registers of social and medical services based on the unique ID of each person.
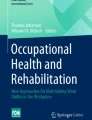
The number of unique individuals is 9244 and nearly 80% of them used rehabilitation only once (see Table 1). The registry is not providing information on the specific services, however, the unique ID of the person allows the identification of multiple entries (more than one service) and 16% of clients have received two services or the same service twice, while only a negligible part has received more than two services. Vocational rehabilitation appears to be a female-dominated service (see Fig. 1), in total 70% of the clients were females and female entrants tend to be employed more often (see Table 2). In general, around 42% of clients are employed and the more middle-aged or higher educated they are the more they enter the service as workers who need support.

First entries to the vocational rehabilitation services by years and gender (n = 9244, numbers below the bars indicate yearly entrances to the service)
Figure 2 reveals the age profile has not considerably changed over time and the mean age for entry is 46 years. Panel (b) indicates a right skew of the age distribution, hence, the median age is 50. Also, there are some gender differences—males are less heterogeneous (respectively 50% of observations from men are between 39 and 57 and women between 32 and 55 and t tests reveal significant differences in mean age by gender). During the Covid-19 period in 2020, we witness a decrease in clients above the median age. Furthermore, in Fig. 3 and Table 2 the ICF 5-point category scores (from 0 to 4) [45] are used to classify impairments, in case the score is at least 1. Under physical impairments, the following are classified: mobility, manual activity and adaptation. Under mental impairments, the following are classified: learning and applying knowledge, communication, self-care and interpersonal interactions. Impairments were not classified using ICF if a client was entering the service at the early stage of the reform. We see from Fig. 3 that more than 50% of clients enter the service with only physical impairments, followed by both mental and physical ones. The category of only mental impairments is the rarest, however, mental impairments are more pronounced in the case of young males.

Age profile of the clients: rehabilitation is an old-age service: a Mean age of clients, b Distribution of the age of clients (n = 9244, mean age by years indicated above each bar)

Impairments of the clients by gender (n = 6788, number of cases included under each bar)
We can also assess the severity of the impairments. For this, we constructed a standardized score based on the ICF classification described above. ICF scores (measured on a 5-point scale, from 0 = “no problem” to 4 = “complete problem”) are combined as composite scores; physical impairments are composed by using the scores of mobility, manual activity and adaptation; mental impairments are composed using the scores of learning and applying knowledge, communication, self-care, as well as interpersonal interactions. These compound scores, indicate the severity of the impairment by summing up scores for physical (from 0 to 12) and mental (from 0 to 16) impairments. Thus, the standardization of the scores (mean = 0 and s.d. = 1) is applied. Correlation analysis (see Fig. 4) reveals that the severity of mental and physical impairments are relatively strongly and negatively associated, while the severity of mental impairments is negatively and physical impairments is positively correlated with age.

The Pearson correlation coefficients between age and severeness of physical and mental impairments (n = 6788, standardized scores)
Figure 5 describes the treatment by indicating that the duration of the service depends on the employment status—on average the employed participated a few days longer in the service than the unemployed (the difference is statistically significant, p < 0.01), the average duration of the service is 25 days and in rare cases, it is longer than 2 months. At the same time, there are significant differences in days depending on the completion of rehabilitation service. In cases, where the service was not completed, the average number of days was only 11.6 days, while service completion was attributed to a mean of 29.5 days.

Number of days spent on vocational rehabilitation service by: a employment status at entry (n = 9244, 42% entered as employed); b service completion status (n = 9244, 73% completed rehabilitation)
Estimation Strategy
For subsequent analysis, a matched sample is generated to investigate the effect of completing rehabilitation services on post-rehabilitation employment. Comparable pairs of people, who completed and who discontinued the service, are created by applying propensity score matching (PSM). The latter was implemented via nearest-neighbor matching without replacement in R by using the MatchIt software package.
To minimize heterogeneity between pairs, PSM was conducted with a caliper of 0.03. Deciding the caliper involves a trade-off between the similarity of the pairs and the number of matches [46]. Smaller calipers yield a greater similarity of pairs, while the number of matches will decrease. A common practice is to obtain its optimal value via a trial and error process [47], which we apply here. Another analytical decision involved removing missing cases,Footnote 2 resulting in 5,141 remaining individuals. Thereafter, PSM is applied with the following model:
where the subscript i denotes an individual, β0 is the constant and \(\epsilon\) is the error term. The dependent variable Completed is 1 in case rehabilitation was completed, otherwise 0 (service discontinued). Other covariates include Gender (male or female), Age (birth year), Education (0 = no education, 1 = primary, 2 = secondary or 3 = higher education), WorkingCapacity (reduced or permanent incapacity) and Residence (regional dummy of Estonian counties). Lastly, Disability referred to the severity of impairment (0 = absent, 1 = slight, 2 = medium, 3 = severe, 4 = complete) in case of mobility, manual activity, adaptation, learning and applying knowledge, interpersonal interactions, self-care, as well as communication. Also, it is important to note that the latter, which is based on ICF scores, does not primarily refer to the working context but rather more broadly to different contexts of an individual´s life. On the other hand, the covariate WorkingCapacity includes the evaluation of a person´s impairment (in terms of the ICF categories), as well as an expert assessment of the resulting constraints to work, provided by the agency. Overall, the matching result of PSM, based on the defined covariates is shown in Table 3.
Thus, PSM paired 883 individuals in both treatment and control groups, which could be considered identical in terms of the specified numerical characteristics, according to independent t tests (see Table 3, panel a). Also, the representations of genders and residence were proportionally similar (see Table 3, panels b and c, respectively) across the two groups. However, in terms of working capacity, the pairs included only individuals with reduced working capacity and none with permanent incapacity. Thus, the working capacity was identical in both groups in the sample, with no variations between them regarding this covariate. Such a matched sample is used in the following regression model:
where EmploymentDuration denotes the length of employment in months after receiving rehabilitation services for individual i at time t, while it takes the value of 0 in periods during and before the rehabilitation. Furthermore, Completed refers to the treatment variable (operationalized in Eq. 1). Di = [EmployedEntry, Gender, OnlyMental, OnlyPhysical] denotes a vector of four dummy variables: EmployedEntry (1 = employed while entering to service), Gender (1 = male), OnlyMental (1 = has only mental impairments), OnlyPhysical (1 = has only physical impairments). These dummies are used for estimating interactive effects with the treatment variable Completed.
Furthermore, for controlling unobserved heterogeneity, the model is specified with αi and σt, which denote fixed effects of individuals and months, respectively. The latter enabled to control for the potential distortions in the labor market due to the Covid-19 pandemic in 2020. However, we were unable to include any directly observable control variables since most of our data consisted of time-invariant factors, which fixed effects omit. For the same reason, the dummy variables could be included only as interactions in the models.
Results
Table 4 revealed a treatment effect on post-rehabilitation employment by 2.6 months. This effect is positively moderated by employment status, i.e., initial employment upon the first entry to the service resulted in about 4 months longer post-rehabilitation employment (when compared to individuals that discontinued the service). Moreover, the first entry into the treatment as unemployed is associated with greater post-rehabilitation employment only by 1.1 months (when compared to the individuals that discontinued the service). In contrast, other dummy variables produced smaller moderation effects.
The findings in Table 4 indicate that treated males experienced nearly 1.2 months longer post-rehabilitation employment than females. However, individuals, who had only mental disabilities, experienced about 1.3 months shorter employment, while physical disabilities resulted in positive, yet merely weakly significant findings (p < 0.1).
Discussion and Conclusions
In the current study, we were seeking evidence that would support economic arguments for vocational rehabilitation services, implemented by the 2016 active labor market reform in Estonia. This reform affected more than 100,000 people with disabilities/impairments and transferred them from welfare to supported work services related to job placement.
In our dataset, we had data for more than 9000 clients of vocational rehabilitation services from 2016 to 2020, including their socio-demographic profile type and severity of impairment, as well as prior employment status (more than 40% were employed). We saw from the data that vocational rehabilitation service clients are mostly females, with a median age of 50. Physical impairments are the main cause of disability, followed by combined disability—both mental and physical. Clients with mental disabilities are relatively young compared with clients with physical impairments.
Although many studies have evaluated the probability of employment after the service, we can build evidence on the duration of the latter. The findings revealed that while completing the vocational rehabilitation service had a positive effect on post-rehabilitation employment, its effect size tends to be relatively small. Thus, although the service can facilitate becoming employed, maintaining employment status seems to remain a challenge. Furthermore, longer post-rehabilitation employment occurred when upon the first month of entry into the service the individual was employed and was male. In contrast, individuals, who had only mental disabilities, experienced shorter employment compared to similar people who discontinued the service, while physical disabilities resulted in a positive effect with only marginal significance (compared to the control group).
However, due to the specificity of the data—we have no control group—only the impact of successful completion can be evaluated. Thus, the main limitations of our results originate from the data specificity—we estimated only the average treatment effect on the treated (ATT) not the average treatment effect (ATE). Furthermore, we did not examine in which services the individuals participated nor did we focus on the occupational background, which may affect employment outcomes as well. Also, even though PSM was applied for mimicking a randomized experimental design, its effectiveness tends to be limited to the selected covariates used for generating the matched sample.
Whether our findings contribute to the case-specific literature or allow us to argue that the positive impact of rehabilitation service is generally relatively small is open to debate. The small treatment effects apply especially in the case of mental impairments. Furthermore, the external validity of our results is dependent on treatment design, meaning that the individual-therapist interaction (working alliance) might hamper the validity of the study. Also, the service is female-dominated, however, male outcomes appeared longer in duration.
Even though the duration of employment is a proxy of latent variables such as employability, job readiness or even productivity and job quality, we have no direct evidence of these psychological well-being metrics. Nevertheless, our study implies that self-efficacy in the case of mental impairments is more difficult to achieve as the main channel for improving labor market outcomes of the clients than in the case of physical impairments. The latter signals more need for targeted services for clients with mental-cognitive impairments. Overall, we conclude that in the case of vocational rehabilitation services, the impact remains shorter than the average impact of employment assistance services and typical cost-efficiency or economic incentive rhetoric does not apply to this reform. Thus, the need for psychological welfare, self-efficacy or similar metrics for identifying the social benefits of the reform remains.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Notes
ICF is a testing tool approved by the World Health Assembly in 2001. The ICF integrates the major models of disability. Seven different impairments are identified: mobility, manual activity, adaptation, learning and applying knowledge, interpersonal interactions, self-care as well as communication. Furthermore, the working capacity assessment (reduced capacity or permanent incapacity) is based on ICF composite scores. However, there are expert opinions included in the assessment, including specifying key indicators dependent on the field of working expertise of the client. Thus, we are unable to directly identify working capacity from ICF scores.
Robustness of this decision was tested with multiple imputations using predictive mean matching. The findings are not significantly different from the ones reported in the current study.
References
Chan F, Leahy MJ, Saunders JL, editors. Case management for rehabilitation health professionals. Aspen Professional Services; 2005.
Popovici I, French MT. Does unemployment lead to greater alcohol consumption? Ind Relations. 2013;52(2):444–466.
French MT, Maclean JC, Sindelar JL, Fang H. The morning after: alcohol misuse and employment problems. Appl Econ. 2011;43(21):2705–2720.
Norström F, Waenerlund AK, Lindholm L, Nygren R, Sahlén KG, Brydsten A. Does unemployment contribute to poorer health-related quality of life among Swedish adults? BMC Public Health. 2019;19(1):1–12.
Hult M, Pietilä AM, Saaranen T. The factors predicting quality of life among unemployed adults: a model based on salutogenic approach. Soc Indic Res. 2020;152(3):1197–1211.
Reitz AK, Luhmann M, Bleidorn W, Denissen JJA. Unraveling the complex relationship between work transitions and self-esteem and life satisfaction. J Pers Soc Psychol. 2022;123(3):597–620.
Van Berkel R, Caswell D, Kupka P, Larsen F, editors. Frontline delivery of welfare-to-work policies in Europe—activating the unemployed. London: Taylor & Francis; 2017.
Bonoli G. The political economy of active labor-market policy. Polit Soc. 2010;38(4):435–457.
Toots A, Lauri T. Nation (re)building through social investment? The Baltic reform trajectories. In: Garritzmann JL, Hausermann S, Palier B, editors. The world politics of social investment the politics of varying social investment strategies, vol. 2. Oxford: Oxford University Press; 2022. p. 159–184.
Foster D, Masso M, Osila L. Work accommodations and sustainable working: the role of social partners and industrial relations in the employment of disabled and older people in Estonia, Hungary and Poland. Eur J Ind Relat. 2021;27(2):149–165.
OECD. Improving the provision of active labour market policies in Estonia, connecting people with jobs. Paris: OECD Publishing; 2021.
Servinski M. How the Estonian labr market has changed during 30 years? Statistics Estonia. 2021. https://www.stat.ee/et/uudised/kuidas-muutunud-eesti-tooturg-30-aasta-jooksul
Statistics [Internet]. The Estonian Chamber of Disabled People. 2021. https://epikoda.ee/en/for-specialists/statistics%0A
Transforming disability into ability. Policies to promote work and income security for disabled people. Pairs: OECD Publishing; 2003.
Labour Market Services and Benefits Act. Riigikogu (Parliament of Estonia); 2005.
ETF. Assessment of the effectiveness of active labour market policies in crisis and post-crisis situation. 2022.
Pruett SR, Swett EA, Chan F, Rosenthal DA, Lee GK. Empirical evidence supporting the effectiveness of vocational rehabilitation. J Rehabil. 2008;74(1):56–63.
Lustig DC, Strauser DR, Rice ND, Rucker TF. The relationship between working alliance and rehabilitation outcomes. Rehabil Couns Bull. 2002;46(1):24–32.
Donnell CM, Lustig DC, Strauser DR. The working alliance: Rehabilitation outcomes for persons with severe mental illness. J Rehabil. 2004;70(2):12–18.
Rosenthal DA, Hoyt WT, Ferrin JM, Cohen ND. Advanced methods in meta-analytic research: applications and implications for rehabilitation counseling research. Rehabil Couns Bull. 2006;49(4):234–246.
Regenold M, Sherman MF, Fenzel M. Getting back to work: self-efficacy as a predictor of employment outcome. Psychiatr Rehabil J. 1999;22(4):361–367.
Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215.
Fleming AR, Del Valle R, Kim M, Leahy MJ. Best practice models of effective vocational rehabilitation service delivery in the public rehabilitation program: a review and synthesis of the empirical literature. Rehabil Couns Bull. 2013;56(3):146–159.
Vooren M, Haelermans C, Groot W, van den Maassen Brink H. The effectiveness of active labor market policies: a meta-analysis. J Econ Surv. 2019;33(1):125–149.
Pereira RMC, Monteiro I. Vocational rehabilitation and return to work: integrative review. Rev Bras Med do Trab. 2019;17(3):441–455.
Echarti N, Schüring E, O’Donoghue C. Effects of vocational re-training on employment outcomes among persons with disabilities in Germany: a quasi-experiment. J Occup Rehabil. 2020;30(2):221–234.
Reims N, Bauer U. Labour market status and well-being in the context of return to work after vocational rehabilitation in Germany. J Occup Rehabil. 2015;25(3):543–556.
Reims N, Tisch A. Employment effects for people with disabilities after participation in vocational training programmes: a cohort analysis using propensity score matching. Work. 2022;72(2):611–625.
Campolieti M, Gunderson MK, Smith JA. The effect of vocational rehabilitation on the employment outcomes of disability insurance beneficiaries: new evidence from Canada. IZA J Labor Policy. 2014;3(1):1–29.
Frölich M, Heshmati A, Lechner M. A microeconometric evaluation of rehabilitation of long-term sickness in Sweden. J Appl Econom. 2004;19(3):375–396.
Bolton B. Counseling and rehabilitation outcomes. In: Chan F, Berven NL, Thomas KR, editors. Counseling theories and techniques for rehabilitation health professionals. New York: Springer; 2004. p. 444–465.
Böttcher HM, Steimann M, Ullrich A, Rotsch M, Zurborn KH, Koch U, et al. Evaluation of a vocationally oriented concept within inpatient oncological rehabilitation. Rehabilitation. 2013;52(5):329–336.
Dutta A, Gervey R, Chan F, Chou CC, Ditchman N. Vocational rehabilitation services and employment outcomes for people with disabilities: a United States study. J Occup Rehabil. 2008;18(4):326–334.
Chiu CY, Chan F, Bishop M, Da Silva CE, O’Neill J. State vocational rehabilitation services and employment in multiple sclerosis. Mult Scler J. 2013;19(12):1655–1664.
Sung C, Sánchez J, Kuo HJ, Wang CC, Leahy MJ. Gender differences in vocational rehabilitation service predictors of successful competitive employment for transition-aged individuals with autism. J Autism Dev Disord. 2015;45(10):3204–3218.
Kaya C, Chan F, Rumrill P, Hartman E, Wehman P, Iwanaga K, et al. Vocational rehabilitation services and competitive employment for transition-age youth with autism spectrum disorders. J Vocat Rehabil. 2016;45(1):73–83.
Kaya C, Iwanaga K, Hsu S, Akpinar EN, Bezyak J, Chen X, et al. Demographic covariates, vocational rehabilitation services, and employment outcomes of working-age adults with anxiety disorders: a multivariate logistic regression analysis. J Occup Rehabil. 2022;32(4):743–752.
Dean D, Pepper JV, Schmidt R, Stern S. The effects of vocational rehabilitation services for people with mental illness. J Hum Resour. 2017;52(3):826–858.
Chan F, Cheing G, Chan JYC, Rosenthal DA, Chronister J. Predicting employment outcomes of rehabilitation clients with orthopedic disabilities: a CHAID analysis. Disabil Rehabil. 2006;28(5):257–270.
Gonzalez R, Rosenthal DA, Kim JH. Predicting vocational rehabilitation outcomes of young adults with specific learning disabilities: transitioning from school to work. J Vocat Rehabil. 2011;34(3):163–172.
Braathen TN, Veiersted KB, Heggens J. Improved work ability and return to work following vocational multidisciplinary rehabilitation of subjects on long-term sick leave. J Rehabil Med. 2007;39(6):493–499.
Langi FLFG, Oberoi A, Balcazar FE, Awsumb J. Vocational rehabilitation of transition-age youth with disabilities: a propensity-score matched study. J Occup Rehabil. 2017;27(1):15–23.
Nivorozhkin A. Overcoming barriers: effects of entering vocational rehabilitation on labour market outcomes. Int J Soc Welf. 2019;28(3):260–270.
Cimera RE. The cost-efficiency of supported employment programs: a literature review. J Vocat Rehabil. 2000;14(1):51–61.
World Health Organization. How to use the ICF: a practical manual for using the International Classification of Functioning, Disability and Health (ICF). Exposure draft for comment. Geneva: WHO; 2013.
Baek S, Park SH, Won E, Park YR, Kim HJ. Propensity score matching: a conceptual review for radiology researchers. Korean J Radiol. 2015;16(2):286–296.
Strawiński P. Dynamic caliper matching. Cent Eur J Econ Model Econ. 2011;2(3):97–110.
Funding
This work was funded by the Ministry of Social Affairs of Estonia.
Author information
Authors and Affiliations
Contributions
A literature review and descriptive analysis were performed by KP. Propensity score matching and regression analysis were conducted by RP. Both authors contributed to revising and editing the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
There are no potential conflicts of interest reported by the authors.
Ethical Approval
The research has been approved by the ethics committee of the Estonian Business School and the Estonian Data Protection Inspectorate.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Pesor, R., Põder, K. Evaluation of Active Labor Market Policy Reform: Employment Outcomes of Vocational Rehabilitation Services. J Occup Rehabil 34, 116–127 (2024). https://doi.org/10.1007/s10926-023-10102-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10926-023-10102-w