
Abstract
This review aims to identify and evaluate digital interventions for social participation in the growing population of adults with long-term physical conditions. Articles were sourced from MEDLINE, EMBASE, CINAHL and PsycINFO databases using subject headings and keywords related to “social participation” and “digital technology”. Studies that adopted digital technology interventions to improve social participation in adults with long-term physical conditions were included. Data on study methodology, participant and digital intervention characteristics, and findings related to social participation were extracted. The search yielded a total of 4646 articles and 14 articles met criteria for final review with five randomized controlled trials, two non-randomized clinical trials and seven one-group pretest–posttest clinical trials. Studies were organized based on the digital intervention strategy implemented to improve social participation: group support (n = 4), individual skill training or counseling (n = 6), education and support (n = 3), and mixed intervention (n = 1). The group support interventions developed a social network among participants through videoconference, app, or virtual reality platform. Three studies reported positive improvements in different aspects of social participation. Individual skill training or counseling mainly utilized phone calls to help participants cope with activity participation and interpersonal relationship issues. Only two studies demonstrated benefits for social participation. The education and support intervention, which used messages and website information to increase participants’ knowledge and provide support, showed positive findings in three studies. This review suggests digital interventions for improving social participation in adults with long-term physical conditions are feasible and the effectiveness of different strategies may vary.
Registration: This review was prospectively registered on the International Prospective Register of Systematic Reviews (PROSPERO) (registry number: CRD42021254105).
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Worldwide, long-term physical conditions are the leading cause of disability and account for a majority of total deaths, including cardiovascular diseases (32%), cancer (17%) and respiratory diseases (7%) in 2017 [1]. In the United States, hypertension and high cholesterol are the most common long-term physical conditions. It is reported that 60% of adults have at least one long-term condition and 42% of adults have multiple long-term conditions [2]. Additionally, people with long-term conditions represent a growing share of health care spending. In 2016, the total cost of health care reached $3.3 trillion in the United States, with 33% spent on direct treatment of long-term conditions [3, 4]. It is estimated that the cost for long-term conditions will increase to $4.2 trillion in 2023, with the growing number of people with long-term physical conditions financially straining the health care system [5].
Long-term physical conditions are associated with a gradual decrease in physiological functions that lead to physical impairments and social limitation [6, 7]. Compared to physical impairments, social limitations are less recognized in hospitals and become more significant when people with long-term physical conditions return to communities [8, 9]. As one of the most important factors in social health, social participation has a direct relationship with physical health, mental well-being, and quality of life [10,11,12,13]. Despite a lack of consensus on the definition of social participation, it has been widely accepted that social participation consists of involvement in social activities and engagement in social relationships with a focus on interacting with people [10, 14, 15].
Previous studies have shown that people with long-term physical conditions experience different degrees of social participation challenges [16, 17]. Moreover, mental health problems developing after long-term physical conditions may exacerbate social participation limitations [18, 19]. Interventions for improving social participation are usually delivered in person and require long-term and ongoing reinforcement [20, 21]. Common barriers of access to these interventions include living in rural areas without local resources, conditions limiting ability to travel, transportation difficulties and time constraints [22]. It is also possible that people who experience stigma related to their conditions are less likely to engage in face-to-face interventions [23, 24].
As technologies improve, it becomes possible to connect with people anywhere and anytime. In the United States, adults with a smartphone rapidly increased from 35% in 2011 to 85% in 2021. Similarly, American adults using the Internet increased from 52% in 2000 to 93% in 2021 [25]. A majority of smartphone owners (62%) in the last year used their phone to search for health-related information. Additionally, there is an increasing trend to use mobile devices to track health [26, 27]. A study reported that more than half of respondents with chronic diseases are interested in using digital technology to receive health care [28]. A growing number of studies support the use of digital technology to deliver different health care services, with encouraging results indicating that digital interventions have the potential to improve health outcomes and be accessible to a broad population [29, 30].
In view of the increasing prevalence of long-term physical conditions and emerging use of digital interventions for social participation, there is a need to summarize current evidence to guide future clinical practice. By systematically reviewing the literature on the use of digital interventions for social participation in adults with long-term physical conditions, this review aims to examine quantitative evidence and summarize characteristics of different intervention strategies in these populations.
Methods
Data source and search strategy
MEDLINE, EMBASE, CINAHL and PsycINFO were searched to identify a broad scope of relevant literature [31,32,33]. The MEDLINE strategy was first developed using Medical Subject Headings (MeSH) and keywords related to “social participation” and “digital technology” and was adapted to the syntax and subject headings for the other databases [34]. All search strategies were reviewed by a librarian with expertise in systematic review searching. Studies were limited to those published in English between January 2010 and May 2021 with corresponding search filters applied for each database (Appendix 1). This review was guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and the protocol was prospectively registered on the International Prospective Register of Systematic Reviews (PROSPERO) (registry number: CRD42021254105) [35].
Inclusion and exclusion criteria
Selection of studies was based on the following criteria. Inclusion criteria: 1) Adult participants (> = 18 years) with single or multiple long-term physical conditions based on International Classification of Diseases (ICD)-10 criteria [36, 37]; 2) Interventions for improving social participation delivered via phones, computers, or other digital technologies; 3) Randomized controlled trials, non‐randomized controlled trials, controlled before‐after studies, interrupted time series studies or one-group pretest–posttest studies. Exclusion criteria: 1) Participants with mental illnesses or intellectual disabilities as primary diagnoses; 2) Digital technology used to assess participants or collect information only; 3) Intervention without at least one component specifically for improving social participation.
Titles and abstracts of the retrieved studies were first screened. Full texts of any potential eligible studies were independently assessed by two authors. Discrepancies were resolved by discussion or involving a third author. Reference lists of the included studies were reviewed to identify additional relevant articles.
Quality assessment and data synthesis
The study quality was evaluated using the Levels of Evidence from the Oxford Centre for Evidence-Based Medicine (OCEBM) [38]. For intervention studies, a randomized controlled trial with narrow confidence interval is rated as “1b”, a cohort study or a low-quality randomized controlled trial is rated as “2b”, a case–control study is rated as “3b”, and a case-series study or a low-quality cohort or case–control study is rated as “4”.
In this review, each included study reported intervention outcomes. However, the outcome measures and participant groups varied greatly thereby not enabling meaningful data pooling for meta-analysis. Data on study methodology, participants and interventions characteristics, and findings related to social participation were extracted. Studies using similar intervention strategies were grouped together and presented in tables.
Results
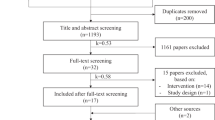
The search yielded a total of 4646 articles. After removing duplicates, titles and abstracts of 3585 articles were screened and full texts of 158 articles were reviewed. A total of 14 articles met all criteria and were included. The study flow diagram documents details of the selection process (Fig. 1).

Study flow diagram
Study characteristics
Table 1 shows the general characteristic of the included studies. There are five randomized controlled trials [39,40,41,42,43], two non-randomized clinical trials [44, 45], and seven one-group pretest–posttest clinical trials [46,47,48,49,50,51,52]. Of the 14 included studies, four studies focus on stroke [39, 43, 47, 50], two studies on cancer [42, 52], two studies on human immunodeficiency virus [40, 51], two studies on systemic lupus erythematosus [48, 49], one study on chronic pain [45], one study on cardiovascular disease [46], one study on neuromuscular disease [44], and one study on spinal cord injury [41]. Sample sizes vary from 19 [47] to 409 [42] with age from 18 to 81 years, while intervention durations range from four weeks [43] to 10 months [41] (Table 2).
Digital interventions for social participation
Regarding OCEBM level of evidence for the included studies, five studies were rated as “2b” and nine studies were rated as “4”. Of the 14 included studies, 11 reported rates of participants that completed the digital intervention, ranging from 83% [43] to 93% [50].
Three types of intervention strategies were identified to improve social participation: 1) group support intervention developed a social network among affected people to increase social interaction and support; 2) education and support intervention sent participants personalized information to increase their knowledge and provide support for social participation; 3) individual skill training or counseling helped participants cope with activity participation and interpersonal relationship issues.
Group support intervention
Four studies utilized group support intervention. Martínez et al. reported significant improvements in “getting along with people”, “life activities”, “participation in society”, “social interaction”, and “psychosocial domain” for people with neuromuscular diseases after seven group support sessions using videoconference [44]. Sakakibara et al. attempted to encourage social connection through a mobile app, which grouped six to nine people with cardiovascular diseases into a “Circle-of-Friends” for 10 weeks to interact with group members and exchange information [46]. Their results showed significant changes in “social support” and “social integration”. The remaining two studies focused on people with aphasia after stroke and each of their group support interventions was based on a topic such as “living with aphasia”. One study using videoconference demonstrated significant improvements in domains of “participation”, “environment”, “socialization and activities” and “roles and responsibilities” [47]. However, the other study used a virtual reality platform and failed to observe any difference in social participation measures between intervention and control groups [39].
Education and support intervention
All three studies showed some positive findings after education and support intervention. A six-month intervention through a website significantly improved “social functioning” for people with cancer [42]. Daily education and support text or email messages over four weeks helped stroke participants achieve their “participation goals” but did not improve their “social integration and support” and “usual activities” [43]. While a three-month education and support intervention increased “social support” for people with human immunodeficiency virus [51].
Individual skill training or counseling
Individual skill training or counseling were implemented in six studies. For people with human immunodeficiency virus, a significant decrease was shown in “interpersonal problems” after receiving nine interventional phone calls [40]. Similarly, Cruice et al. found significant increases in “social contacts”, “life participation”, and “quality of life” for people with stroke after 16 intervention sessions using videoconference [50]. However, four studies reported the following insignificant or negative findings for individual skill training and counseling: less effective than face-to-face interventions to help return to work for people with chronic pain [45]; not different from standard care to improve community participation for people with spinal cord injury [41]; and no significant improvement in interpersonal issues for people with systemic lupus erythematosus [48, 49].
Only one study adopted a mixed intervention strategy, which sent cancer participants e-messages with a link for online learning resources and group discussions [52]. The results showed that “employment concern” significantly increased after the three-month intervention despite improvements in physical health.
Assessment scales for social participation
A total of 22 different assessment scales were used with items of measuring different aspects of social participation (Appendix 2). A majority of the scales assessed quality of life such as the Lupus Quality of Life Questionnaire and Stroke and Aphasia Quality of Life Scale. Only three assessment scales were used in two studies, and included the Assessment for Living with Aphasia [47, 50], Health Education Impact Questionnaire [43, 46] and Social Support Survey [46, 49].
Discussion
Adults with long-term physical conditions commonly experience social participation challenges. To our knowledge, this is the first systematic review to examine digital interventions for social participation in adults with long-term physical conditions. Results suggest that using digital interventions for social participation is feasible and that there are differences in effectiveness among the strategies of group support, education and support, and individual skill training or counseling.
In this review, the group support intervention showed more positive improvements in different aspects of social participation than the other two intervention strategies. During the group support intervention, participants with long-term physical conditions shared their experience, developed trusting relationships, and received support from their peer group. These strategies potentially increased social interactions and practiced building social relationships. This was consistent with findings from previous studies outside of the area of long-term physical conditions. A systematic review by Tobin et al. reported that group support interventions benefitted social participation in the adult Autism population [53]. Likewise, another review by Webber et al. summarized different approaches to improve social participation in persons with mental health problems [20]. Their results showed that group support interventions increased participants’ social connections and strong evidence was reported for engagement in community activities. Social interactions with diverse people not limited to peers may be more similar to real-world social interactions and thus produce more benefits. Given the lack of studies comparing different sources of group support in this review, it is unclear whether there is a difference in effectiveness or results between peer support and support from a diverse social network. Nevertheless, previous studies in the elderly and adolescents with chronic disabilities have shown that social media use is associated with increased social participation and have demonstrated the accessibility of diverse social connections with the use of digital technology [54, 55]. Further investigation of different social networks’ effects on social participation may help guide future clinical practice.
Among the three types of digital interventions, the education and support intervention is the most flexible for time and location. Therefore, participants’ motivation for engaging in this intervention plays a key role in ensuring effectiveness. All three studies demonstrated that providing personalized resources and support by identifying participants’ needs and goals facilitated purposeful and active engagement in the intervention [42, 43, 51]. The importance of personalized content was also highlighted in the previous studies adopting message-based interventions for behavior change [56, 57]. A recent study by Graham et al. further explored different factors’ influencing adherence to a 3-month online course for smoking cessation. Their results showed that a dynamic tailoring method, which continuously sent participants feedback about their course usage and promoted different course functions, was the most powerful factor associated with participation in the online intervention [58]. Additional strategies were suggested for digital interventions in a systematic review by Milward et al., which included sending reminders, using multiple media medium, and involving peers or therapists [59]. These findings also indicate that the flexibility and convenience of receiving digital interventions simultaneously make it easy to participate as well as drop out of the intervention. Future research is warranted to address retention in digital interventions and explore strategies to keep people engaged in such studies.
Regarding different intervention strategies demonstrated in this review, three studies implementing group support interventions and three studies adopting education and support interventions showed positive improvements in social participation. However, only two of the six studies using individual skill training or counseling reported positive contributions to social participation. There are some possible reasons for these results. First, five studies used phone calls to deliver individual skill training or counseling. Compared with other digital technologies such as videoconferencing, phone calls lack access to facial expressions and body language that potentially affects building therapeutic rapport and limits the skill training or counseling effects [60]. Additionally, some therapeutic interventions, such as return to work training, rely on visual guidance and may not be best suited for verbal delivery by phone calls [45]. Given that digital technology is a prerequisite for successful digital intervention and technology related problems commonly occur, it is essential to choose a digital technology with effective content delivery and easy user adoption [47]. It is also recommended to provide technology training and assistance for participants during the intervention. Finally, peer mentors led individual skill training or counseling in three studies that failed to improve social participation [41, 48, 49]. Although the mentors received a short-term training prior to the intervention in these studies, a lack of systematic training and practical experience may reduce the effects of this intervention and limit the ability to achieve predetermined outcome goals [61]. To perform effective peer mentoring, clear role responsibilities, ongoing professional trainings and supported environments are recommended to be addressed in future studies [62, 63].
Cost is one of the major concerns influencing participants’ choice of an intervention. In 2015, 16.9% of American adults with multiple long-term conditions delayed or refused necessary medical care due to cost [64]. This problem is more significant in developing countries with limited health care resources [65]. In this review, only two studies reported the cost of digital interventions. Their results showed that a 6-month group support intervention cost an average of $2,000 USD per participant and the significant portion of cost was training facilitators [39]. Another 12-week study of individual skill training or counseling spent an average of $1292 USD per participant, with the major cost being participant compensation [48]. Their results also reported a benefit–cost ratio of 18.13 in the long run and suggested the intervention’s cost-effectiveness. In 2002, Whitten et al. questioned the cost-effectiveness of digital interventions due to lack of good evidence [66]. However, growing studies indicate that digital interventions have the potential to address the health care burden in a cost-effective way [67, 68]. With its increasing use in different fields such as mental health [69,70,71] and disease self-management [72,73,74], and the rapidly growing demand during the COVID-19 pandemic [75], digital interventions show the potential to change the landscape of health care through novel intervention delivery and broad access. At the same time, digital interventions pose new challenges for building and supporting a digital health care system, including establishing policies to protect personal privacy and technical support to ensure service quality and data security [76,77,78].
There are several limitations for this review. First, the overall quality of included studies is limited with five randomized controlled trials, two non-randomized clinical trials and seven one-group pretest–posttest clinical trials. Selection bias also exists in studies by preferably recruiting participants, who have access to or are familiar with digital technology, into an experimental group that may overrate the intervention effects. Future studies are recommended to follow the guideline to report digital interventions for health care [79]. Second, the large variety in social participation measures limits the ability to perform a meta-analysis. This limitation has been reported in previous reviews about social participation interventions [20, 80]. Given the growing importance of social participation as a health outcome, there is a need for consensus on the assessment of social participation. Third, the included studies are limited to pre-post experimental designs. Thus, digital interventions reported in descriptive and qualitative studies are excluded from this review. Fourth, eight different long-term physical conditions were explored in the included studies. The effectiveness of intervention strategies may differ based on physical condition. Future studies may explore the optimal intervention strategy with matching to specific physical conditions and personal characteristics.
Social participation is an important component of health and wellness as well as role adjustments for those living with long-term physical conditions. With the increasing use of digital interventions to facilitate the management of long-term physical conditions and improve social participation, it is important to identify trends in these interventions. Additionally, the recent COVID-19 pandemic has highlighted a growing need to provide interventions in a safe and effective manner, with increased utilization of digital interventions. This review demonstrates digital intervention strategies including group support, education and support, and individual skill training or counseling. It highlights the effectiveness of group support for diverse aspects of social participation, the importance of personalized intervention contents for education and support, and the necessity of technology support and peer mentor training for individual skill training or counseling. Meanwhile, there remains a need for future studies to assess the cost-effectiveness of digital interventions, develop practice guidelines for improving social participation, and build supportive environment for a sustainable digital health care system.
Data availability
Not applicable.
References
Ritchie, H., Spooner, F., & Roser, M., Causes of death. Our World in Data, 2018.
Buttorff, C., Ruder, T., Bauman, M., Multiple chronic conditions in the United States. Rand Santa Monica, CA, 2017.
Waters, H., Graf, M., The costs of chronic disease in the US. The Milken Institute: Santa Monica, CA, 2018.
Hartman, M., Martin, A. B., Espinosa, N., Catlin, A., The national health expenditure accounts T. national health care spending in 2016: spending and enrollment growth slow after initial coverage expansions. Health Aff. (Millwood). 37(1):150-60, 2018.
Bodenheimer, T., Chen, E., Bennett, HD., Confronting the growing burden of chronic disease: can the US health care workforce do the job? Health Aff. 28(1):64-74, 2009.
Egger, G., Dixon, J., Beyond obesity and lifestyle: a review of 21st century chronic disease determinants. Biomed. Res. Int. 2014:731685, 2014.
Grover, A., Joshi, A., An overview of chronic disease models: a systematic literature review. Glob. J. Health Sci. 7(2):210-27, 2014.
Megari, K., Quality of life in chronic disease patients. Health Psychol. Res. 1(3):e27, 2013.
Stanton, A. L., Revenson, T. A., Tennen, H., Health psychology: psychological adjustment to chronic disease. Annu. Rev. Psychol. 58:565-92, 2007.
Douglas, H., Georgiou, A., Westbrook, J., Social participation as an indicator of successful aging: an overview of concepts and their associations with health. Aust. Health Rev. 41(4):455-62, 2017.
Puts, M. T., Shekary, N., Widdershoven, G., Heldens, J., Lips, P., Deeg, D. J., What does quality of life mean to older frail and non-frail community-dwelling adults in the Netherlands? Qual. Life Res. 16(2):263-77, 2007.
Hornby-Turner, Y. C., Peel, N. M., Hubbard, R. E., Health assets in older age: a systematic review. BMJ Open. 7(5):e013226, 2017.
Santini, Z. I., Jose, P. E., Koyanagi, A., Meilstrup, C., Nielsen, L., Madsen, K. R., et al., Formal social participation protects physical health through enhanced mental health: A longitudinal mediation analysis using three consecutive waves of the Survey of Health, Ageing and Retirement in Europe (SHARE). Soc. Sci. Med. 251:112906, 2020.
Levasseur, M., Richard, L., Gauvin, L., Raymond, E., Inventory and analysis of definitions of social participation found in the aging literature: proposed taxonomy of social activities. Soc. Sci. Med. 71(12):2141-9, 2010.
Piskur, B., Daniels, R., Jongmans, M. J., Ketelaar, M., Smeets, R. J., Norton, M., et al., Participation and social participation: are they distinct concepts? Clin. Rehabil. 28(3):211-20, 2014.
Klein, T. M., Andrees, V., Kirsten, N., Protz, K., Augustin, M., Blome, C., Social participation of people with chronic wounds: A systematic review. Int. Wound J. 18(3):287-311, 2021.
Griffith, L. E., Raina, P., Levasseur, M., Sohel, N., Payette, H., Tuokko, H., et al., Functional disability and social participation restriction associated with chronic conditions in middle-aged and older adults. J. Epidemiol. Community Health. 71(4):381-9, 2017.
Scott, K. M., Lim, C., Al-Hamzawi, A., Alonso, J., Bruffaerts, R., Caldas-de-Almeida, J. M., et al., Association of Mental Disorders With Subsequent Chronic Physical Conditions: World Mental Health Surveys From 17 Countries. JAMA Psychiatry. 73(2):150-8, 2016.
Kvaal, K., Halding, A. G., Kvigne, K., Social provision and loneliness among older people suffering from chronic physical illness. A mixed-methods approach. Scand. J. Caring Sci. 28(1):104-11, 2014.
Webber, M., Fendt-Newlin, M., A review of social participation interventions for people with mental health problems. Soc. Psychiatry Psychiatr. Epidemiol. 52(4):369-80, 2017.
Obembe, A. O., Eng, J. J. Rehabilitation Interventions for Improving Social Participation After Stroke: A Systematic Review and Meta-analysis. Neurorehabil. Neural. Repair. 30(4):384-92, 2016.
Mohr, D. C., Siddique, J., Ho, J., Duffecy, J., Jin, L., Fokuo, J. K. Interest in behavioral and psychological treatments delivered face-to-face, by telephone, and by internet. Ann. Behav. Med. 40(1):89-98, 2010.
Collins, K. A., Westra, H. A., Dozois, D. J., Burns, D. D., Gaps in accessing treatment for anxiety and depression: challenges for the delivery of care. Clin. Psychol. Rev. 24(5):583-616, 2004.
Molero, F., Recio, P., Garcia-Ael, C., Perez-Garin, D., Consequences of perceived personal and group discrimination against people with physical disabilities. Rehabil. Psychol. 64(2):212-20, 2019.
Pew Research Center, Mobile fact sheet 2022. Available from: https://www.pewresearch.org/internet/fact-sheet/mobile/. Accessed 14 Jan 2022.
Smith, A., McGeeney, K., Duggan, M., US smartphone use in 2015. 2015.
Deng, H., Abouzeid, C. A., Shepler, L. J., Slavin, M. D., Taylor, J. A., Mercier, H. W., et al., Using digital phenotyping to characterize psychosocial trajectories for people with burn injury. Burns. 48(5):1262-6, 2022.
Edwards, L., Thomas, C., Gregory, A., Yardley, L., O'Cathain, A., Montgomery, A. A., et al., Are people with chronic diseases interested in using telehealth? A cross-sectional postal survey. J. Med. Internet Res. 16(5):e123, 2014.
Silva, B. M., Rodrigues, J. J., de la Torre Diez, I., Lopez-Coronado, M., Saleem, K., Mobile-health: A review of current state in 2015. J. Biomed. Inform. 56:265-72, 2015.
Fiordelli, M., Diviani, N., Schulz, P. J., Mapping mHealth research: a decade of evolution. J. Med. Internet Res. 15(5):e95, 2013.
Wong, S. S., Wilczynski, N. L., Haynes, R. B. Comparison of top-performing search strategies for detecting clinically sound treatment studies and systematic reviews in MEDLINE and EMBASE. J. Med. Library Assoc. 94(4):451-5, 2006.
Bahaadinbeigy, K., Yogesan, K., Wootton, R., MEDLINE versus EMBASE and CINAHL for telemedicine searches. Telemed. J. e-Health. 16(8):916-9, 2010.
VandenBos, G. R., APA dictionary of psychology: American Psychological Association, 2007.
Sampson, M., McGowan, J., Cogo, E., Grimshaw, J., Moher, D., Lefebvre, C., An evidence-based practice guideline for the peer review of electronic search strategies. J. Clin. Epidemiol. 62(9):944-52, 2009.
Moher, D., Liberati, A., Tetzlaff J, Altman DG, Group P., Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 6(7):e1000097, 2009.
Kampling, H., Baumeister, H., Bengel, J., Mittag, O., Prevention of depression in adults with long-term physical conditions. Cochrane Database Syst. Rev. 3:CD011246, 2021.
World Health Organization, The ICD-10 classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines. World Health Organization, 1992.
Howick, J., Phillips, B., Ball, C., Sackett, D., Badenoch, D., Oxford centre for evidence-based medicine levels of evidence. University of Oxford, Centre for Evidence-Based Medicine, 5, 2009.
Marshall, J., Devane, N., Talbot, R., Caute, A., Cruice, M., Hilari, K., et al., A randomised trial of social support group intervention for people with aphasia: A Novel application of virtual reality. PLoS One. 15(9):e0239715, 2020.
Heckman, T. G., Heckman, B. D., Anderson, T., Lovejoy, T. I., Markowitz, J. C., Shen, Y., et al., Tele-interpersonal psychotherapy acutely reduces depressive symptoms in depressed HIV-infected rural persons: A randomized clinical trial. Behav. Med. 43(4):285-95, 2017.
Mackelprang, J. L., Hoffman, J. M., Garbaccio, C., Bombardier, C. H., Outcomes and lessons learned from a randomized controlled trial to reduce health care utilization during the first year after spinal cord injury rehabilitation: Telephone counseling versus usual care. Arch. Phys. Med. Rehab. 97(10):1793-6.e1, 2016.
Willems, R. A., Bolman, C. A. W., Mesters, I., Kanera, I. M., Beaulen, A. A. J. M., Lechner, L., Short-term effectiveness of a web-based tailored intervention for cancer survivors on quality of life, anxiety, depression, and fatigue: randomized controlled trial. Psycho-Oncology. 26(2):222-30, 2017.
Cadilhac, D. A., Andrew, N. E., Busingye, D., Cameron, J., Thrift, A. G., Purvis, T., et al., Pilot randomised clinical trial of an eHealth, self-management support intervention (iVERVE) for stroke: feasibility assessment in survivors 12–24 months post-event. Pilot and Feasibility Stud. 6(1), 2020.
Martínez, O., Jometón, A., Pérez, M., Lázaro, E., Amayra, I., López-Paz, J. F., et al., Effectiveness of teleassistance at improving quality of life in people with neuromuscular diseases. Span. J. Psychol. 17:E86, 2014.
Sullivan, M. J. L., Simon, G., A telephonic intervention for promoting occupational re-integration in work-disabled individuals with musculoskeletal pain. Transl. Behav. Med. 2(2):149-58, 2012.
Sakakibara, B. M., Ross, E., Arthur, G., Brown-Ganzert, L., Petrin, S., Sedlak, T., et al., Using mobile-health to connect women with cardiovascular disease and improve self-management. Telemed. J. e-Health. 23(3):233-9, 2017.
Pitt, R., Theodoros, D., Hill, A. J., Russell, T., The impact of the telerehabilitation group aphasia intervention and networking programme on communication, participation, and quality of life in people with aphasia. Int. J. Speech Lang. Pathol. 21(5):513-23, 2019.
Williams, E. M., Dismuke, C. L., Faith, T. D., Smalls, B. L., Brown, E., Oates, J. C., et al., Cost-effectiveness of a peer mentoring intervention to improve disease self-management practices and self-efficacy among African American women with systemic lupus erythematosus: analysis of the Peer Approaches to Lupus Self-management (PALS) pilot study. Lupus. 28(8):937-44, 2019.
Williams, E. M., Hyer, J. M., Viswanathan, R., Faith, T. D., Voronca, D., Gebregziabher, M., et al., Peer-to-peer mentoring for African American women with lupus: A feasibility pilot. Arthritis Care Res. (Hoboken). 70(6):908-17, 2018.
Cruice, M., Woolf, C., Caute, A., Monnelly, K., Wilson, S., Marshall, J. Preliminary outcomes from a pilot study of personalised online supported conversation for participation intervention for people with Aphasia. Aphasiology. 35(10):1293-317, 2021.
Uhrig, J. D., Lewis, M. A., Bann, C. M., Harris, J. L., Furberg, R. D., Coomes, C. M., et al., Addressing HIV knowledge, risk reduction, social support, and patient involvement using SMS: results of a proof-of-concept study. J. Health Commun. 17(Suppl 1):128-45, 2012.
Nahm, E. S., Miller, K. , McQuaige, M., Corbitt, N., Jaidar, N., Rosenblatt, P., et al., Testing the impact of a cancer survivorship patient engagement toolkit on selected health outcomes. Oncol. Nurs Forum. 46(5):572-84, 2019.
Tobin, M. C., Drager, K. D., Richardson, L. F., A systematic review of social participation for adults with autism spectrum disorders: Support, social functioning, and quality of life. Res. Autism Spectr. Disord. 8(3):214-29, 2014.
Raghavendra, P., Newman, L., Grace, E., Wood, D. ,'I could never do that before': effectiveness of a tailored Internet support intervention to increase the social participation of youth with disabilities. Child Care Health Dev. 39(4):552-61, 2013.
Hasan, H., Linger, H., Enhancing the wellbeing of the elderly: Social use of digital technologies in aged care. Educ. Gerontol. 42(11):749-57, 2016.
Fjeldsoe, B. S., Marshall, A. L., Miller, Y. D. Behavior change interventions delivered by mobile telephone short-message service. Am. J. Prev. Med. 36(2):165-73, 2009.
Naughton, F., Jamison, J., Sutton, S., Attitudes towards SMS text message smoking cessation support: a qualitative study of pregnant smokers. Health Educ. Res. 28(5):911-22, 2013.
Graham, A. L., Papandonatos, G. D., Jacobs, M. A., Amato, M. S., Cha, S., Cohn, A. M., et al., Optimizing text messages to promote engagement with internet smoking cessation treatment: Results from a factorial screening experiment. J. Med. Internet Res. 22(4):e17734, 2020.
Milward, J., Drummond, C., Fincham-Campbell, S., Deluca, P., What makes online substance-use interventions engaging? A systematic review and narrative synthesis. Digit. Health. 4:2055207617743354, 2018.
Oh, C. S., Bailenson, J. N., Welch, G. F., A systematic review of social presence: Definition, antecedents, and implications. Front. Robot AI. 5:114, 2018.
Fuhr, D. C., Salisbury, T. T., De Silva, M. J., Atif, N., van Ginneken, N., Rahman, A., et al., Effectiveness of peer-delivered interventions for severe mental illness and depression on clinical and psychosocial outcomes: a systematic review and meta-analysis. Soc. Psychiatry Psychiatr. Epidemiol. 49(11):1691-702, 2014.
Mancini, M. A., An exploration of factors that effect the implementation of peer support services in community mental health settings. Commun. Ment. Health J. 54(2):127-37, 2018.
Mahlke, C. I., Kramer, U. M., Becker, T., Bock, T., Peer support in mental health services. Curr. Opin. Psychiatry. 27(4):276-81, 2014.
Ward, B. W., Barriers to health care for adults with multiple chronic conditions: United States, 2012-2015. NCHS Data Brief. (275):1–8, 2017.
Peters, D. H., Garg, A., Bloom, G., Walker, D. G., Brieger, W. R., Rahman, M. H., Poverty and access to health care in developing countries. Ann. N. Y. Acad. Sci. 1136:161-71, 2008.
Whitten, P. S., Mair, F. S., Haycox, A., May, C. R., Williams, T. L., Hellmich, S., Systematic review of cost effectiveness studies of telemedicine interventions. BMJ. 324(7351):1434-7, 2002.
Jiang, X., Ming, W. K., You, J. H. The Cost-Effectiveness of Digital Health Interventions on the Management of Cardiovascular Diseases: Systematic Review. J. Med. Internet Res. 21(6):e13166, 2019.
De La Torre-Díez, I., López-Coronado, M., Vaca, C., Aguado, J. S., de Castro, C., Cost-utility and cost-effectiveness studies of telemedicine, electronic, and mobile health systems in the literature: a systematic review. Telemed. e-Health. 21(2):81-5, 2015.
Shah, A., Kraemer, K. R., Won, C. R., Black, S., Hasenbein, W., Developing digital intervention games for mental disorders: A review. Games Health J. 7(4):213-24, 2018.
Lau, Y., Cheng, J. Y., Wong, S. H., Yen, K. Y., Cheng, L. J., Effectiveness of digital psychotherapeutic intervention among perinatal women: A systematic review and meta-analysis of randomized controlled trials. World J. Psychiatry. 11(4):133-52, 2021.
Krzyzaniak, N., Greenwood, H., Scott, A. M., Peiris, R., Cardona, M., Clark, J., et al., The effectiveness of telehealth versus face-to face interventions for anxiety disorders: A systematic review and meta-analysis. J. Telemed. Telecare. 1357633x211053738, 2021.
Morrison, D., Wyke, S., Agur, K., Cameron, E. J., Docking, R. I., Mackenzie, A. M., et al., Digital asthma self-management interventions: a systematic review. J. Med. Internet Res. 16(2):e51, 2014.
Samoocha, D., Bruinvels, D. J., Elbers, N. A., Anema, J. R., van der Beek, A. J., Effectiveness of web-based interventions on patient empowerment: a systematic review and meta-analysis. J. Med. Internet Res. 12(2):e23, 2010.
Guo, Y., Albright, D., The effectiveness of telehealth on self-management for older adults with a chronic condition: A comprehensive narrative review of the literature. J. Telemed. Telecare. 24(6):392-403, 2018.
Hau, Y. S., Kim, J. K., Hur, J., Chang, M. C., How about actively using telemedicine during the COVID-19 pandemic? J. Med. Syst. 44(6):108, 2020.
Gurupur, V. P., Wan, T. T. H. Challenges in implementing mHealth interventions: a technical perspective. Mhealth. 3:32, 2017.
Akter, S., Ray, P., mHealth-an ultimate platform to serve the unserved. Yearb. Med. Inform. 19(01):94-100, 2010.
Arora, S., Yttri, J., Nilse, W. Privacy and Security in Mobile Health (mHealth) Research. Alcohol Res. 36(1):143-51, 2014.
Agarwal, S., LeFevre, A. E., Lee, J., L'Engle, K., Mehl, G., Sinha, C., et al., Guidelines for reporting of health interventions using mobile phones: mobile health (mHealth) evidence reporting and assessment (mERA) checklist. Bmj. 352:i1174, 2016.
Baker, S., Warburton, J., Waycott, J., Batchelor, F., Hoang, T., Dow, B., et al., Combatting social isolation and increasing social participation of older adults through the use of technology: A systematic review of existing evidence. Australas. J. Ageing. 37(3):184-93, 2018.
Funding
This work was supported by the Spaulding Research Institute (the Leadership Catalyst Research Fellowship), Stepping Strong Center and National Institute on Disability, Independent Living, and Rehabilitation Research (grant number 90DPBU0001).
Author information
Authors and Affiliations
Contributions
Study conception and design: HD and JCS; literature search, data extraction and screening, study assessment, results interpretation, and the initial manuscript writing: HD, KQV and JRF; study design, results interpretation, and critically revising the manuscript: LJS, CAA, JWH, HWM, JAT, LEK, MDS, CMR, and JCS. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethical approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Conflict of interest
The Authors declare that there is no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Deng, H., Vu, K.Q., Franco, J.R. et al. Digital Interventions for Social Participation in Adults with Long-term Physical Conditions: A Systematic Review. J Med Syst 47, 26 (2023). https://doi.org/10.1007/s10916-023-01914-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10916-023-01914-7