
Abstract
Telemedicine and teleconsultation can be powerful and useful tools for patients to hamper the physical barriers to access to health care services during COVID-19 pandemic. We describe the teleconsultation (TC) model in the Lazio Region. It uses a hub-and-spoke network system on geographic regional basis using a web based digital platform, termed ADVICE with the aim to connect regional Emergency Departments (EDs) and Infectious Diseases (ID) acute and critical care settings for patients with acute ID syndrome. Between January 2020 and June 2021, the ADVICE platform received 18.686 TCs: of them, 10838 requests (58%) were for ID TCs in 7996 patients, followed by 2555(13%) requests for trauma, 2286(12%) for acute complex syndrome and 1681 (8%) for Stroke TCs. Three quarter of ID TCs were requested for SARS-COV-2 infection, followed by sepsis management in 7% and tuberculosis in 6%. In 5416 TCs, 68%, diagnostic investigations and therapeutic prescriptions were recommended before admission, in 1941 TCs, 24%, the recommendation was patient admission and in 608 TCs, 7%, was to discharge patient at home. Telemedicine have ensured high-profile consultations for ID patients and during COVID-19 the use of this resource optimized clinical patient management.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
During the COVID-19 outbreak, telehealth technology has been recognized to play a key role in the global response to the spread of SARS-CoV-2 infection. Indeed, it allowed physicians to deliver, via information technologies (IT), health services to patients with limited access to health care services during the quarantine [1].
Telemedicine is the use of telecommunications technology for medical diagnosis and patient care [2]. It is possible to organize specialized advice from a distance by planning an electronic consultation (e-consult). In the emerging field of telemedicine, teleconsultation (TC) is defined as synchronous or asynchronous consultation using information and communication technology to omit geographical and functional distance. Its goals are for diagnostics or treatment between two or more geographically separated health providers [2]. Referring providers send a consultation request to specialists, who may respond by answering the consult question, requesting additional information, and/or indicating diagnostic and therapeutic prescriptions [3]. For a novel infection such as COVID-19, where natural history and optimal clinical management are rapidly evolving, information must be rapidly synthesized, and Infectious Disease (ID) consultations can provide support by performing case-by-case evaluations [4].
The Lazio region is one of the 20 administrative regions of Italy and is in the central peninsular area of the country and comprises a land area of 17,242 km2. It has 5,864,321 inhabitants, most of them (4,353,738) resident in the metropolitan city of Rome. Rome incorporates the small enclave of Vatican City [5]. In 2010, a Lazio regional law established the legal framework of the regional network of ID units, but only in December 2015, at the time of the last catholic Jubilee, the regional health authorities officially instituted a network of all the 47 regional Emerging Departments (EDs) with the eight ID units operating by a hub-and-spoke network system on a geographic basis (Fig. 1). Since January 2019, regional health authorities have provided all regional EDs with a web-based telemedicine platform system termed ADVICE to obtain remote teleconsultations [6,7,8,9]. Through the ADVICE system is possible to ask for different specialist TCs: trauma and polytrauma, complex acute syndromes for poly-pathological patients (CASPP) demanding for multidisciplinary medical services, neurological clinical disorders requiring an urgent assessment by a stroke unit, cardiological emergencies requiring cardio surgical evaluation and pediatric emergencies.

Model of the Infectious Disease emergencies Network in Lazio Region
The aim of this report is to describe the experience of telemedicine using the ADVICE digital platform for ID TC service in all EDs of the Lazio region during the COVID-19 outbreak between January 2020 and June 2021.
Material and methods
We analyzed ID TC requests sent by EDs of peripheral hospitals through ADVICE web-platform, during the period between January 2020 and June 2021. We collected data regarding ED of origin, gender, age of patient, reason for physician request, outcome of counseling, and time between request and release of counseling.
Briefly there are three major ID units operating on call, 24 h per day and 7 days per week, play the role of primary hubs: the Sapienza University Hospital, the Agostino Gemelli Catholic University Hospital and the Lazzaro Spallanzani National Institute for Infectious Disease (INMI), all based in Rome, Italy (Fig. 1). The INMI Hub plays the role of the clinical coordination of the network and the INMI ID physician on call is the bed manager of the regional ID network.
The general data protection officer of the Lazio region and of the Italian data protection authority approved the use of the ADVICE platform for sharing clinical data among health care workers.
Briefly, the ED physician requesting the consultation at spoke peripheral level, produces a brief electronic report including medical history, vital signs and respiratory data, blood tests and radiological images of the patient throughout the ADVICE platform, and eventually, providing additional details by phone, upon request. The ID specialist at hub level is committed to provide an evidence-based, standardized diagnostic and therapeutic approach to patients with acute infectious syndrome, suggesting appropriate infection control measures, referring patients to the acute or critical care ID unit, or, alternatively, discharging them home or in an outpatient setting. The ID specialist formally notifies the ED physician of the closure of the consultation. Eventually, INMI is one of the leading Italian COVID-19 reference centers and, since March 2020, weekly web platform COVID-19 seminars on epidemiologic, clinical, and diagnostic topics have been scheduled for all regional ED physician, intensive care and acute ID consultants.
Finally, this is a cross-sectional survey with no prospective longitudinal data.
Results
In the interval period between January 2020 and June 2021, the ADVICE platform collected 18.686 requests for TCs from all 47 regional EDs. The 58% (10.834) were ID TCs while the remaining 6726 (42%) were related to patients with non-ID acute syndromes, among them 38% (2555) were trauma TCs followed by 2286 (34%) CASPP TCs, 1681 (25%) Stroke Unit TCs, followed by few remaining cardio surgical and pediatrics TCs.
Of the 47 regional EDs, 37 (78%) actively used the ADVICE platform to ask for an ID consultation, for a total of 10.838 requests (58%) related to 7966 patients.
Regarding the ID TCs, the 75% (8125) of them, were referred to 10 major regional hospitals: 7 of them, located in Rome and 3 in the Latium provinces. Globally, the provinces accounted for the 26% (2.176) of ID TC requests. Table 1 showed the features of ID TCs.
Patients who underwent ID TCs were mostly male 62% (4938), with a median age of 64 y.o. (min–max, 18–103). The ADVICE platform use progressively increased coinciding with COVID-19 epidemic peaks. This increase was directly related to the increasing number of COVID-19 cases, and particularly, to the different wave peaks of COVID-19 cases in the Lazio region (Fig. 2). A median 497 ID TC (range 17: 2124) per month was reported all over the 18-month period.

Infectious Disease Teleconsultations and number of COVID-19 in Lazio region trends during the observation period
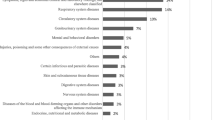
ID TCs were mostly requested for patients with acute respiratory syndromes by COVID-19 (6054 clinical cases, 76%). The remaining TCs (797 cases, 7%) were requested for the management of sepsis, followed by tuberculosis (478 cases, 6%), HIV infection/AIDS 398, 4%), tropical infections or central nervous system acute syndromes (239, 3%) as reported in Table 1.
In 5416 out of 7966 cases (68%), further diagnostic investigations and therapeutic prescriptions were recommended by TCs immediately before admission, whereas in 1941 ID TCs (24%), the clinical recommendation was to admit the patient to the ID unit of the hub-and-spoke network system or, in 608 ID TCs, 7%, to discharge the patient to home. The average time for taking charge of the request and for releasing the ID TC was 73 min.
Discussion
The hub-and-spoke model afford a unique opportunity to maximize efficiencies and effectiveness: from this perspective, telemedicine is a key tool in supporting this model [10,11,12]. In our region few medical hub responsible for advanced medical services are located in the center of the city while primary care medical services are peripherally spread across an extensive network of secondary spoke sites.
Immediately before the beginning of the 2020 COVID-19 pandemic, the Lazio regional network implemented an ID TC service for all regional EDs, particularly in hospitals with no ID professionals. The use of this web platform during the COVID-19 pandemic has presented an opportunity for implementing telemedicine.
The 78% of the Lazio region spokes have asked for ID consultation and the main reason of TC request was the SARS-CoV-2 infection management, followed by the sepsis management.
This could be probably because the clinical management of COVID patients is constantly evolving and being aware of the state-of-the-art treatments can be challenging for ED physicians and that sepsis is a medical emergency and a significant public health problem that affects millions of people worldwide, representing one of the leading causes of death.
The great number of teleconsultations requests reflect the broadmindedness of ER physicians towards innovative technological tools and the clinical support that having an ID specialist consultation could provide to ED physicians, especially in peripheral areas hospitals. This telemedicine approach has allowed the patient to receive the best clinical management in slightly more than 1 h from the ID TC request. This significantly improved the quality and the reliability of clinical care based on scientific evidence. Moreover, ID teleconsultations allowed the patient to be referred in a short time to hospitalization, to further investigations or to home discharge, ensuring a shorter stay in the ED and thus avoiding crowding.
In ED setting, the immediate taking care of new suspected or confirmed COVID-19 cases is crucial. Indeed, both early recognition of severe patients and identification of the best heath care settings depending on clinical severity (general or critical care units) make resource allocation more efficient. Moreover, it allows to discharge home pauci- or asymptomatic patients using standardized protocols and, finally, to contain the viral circulation among susceptible subjects. In the context of sepsis, having a short time to set antibiotic therapy and an appropriate treatment regimen is already demonstrated to improve clinical outcome [13].
Monkowski et al. already demonstrated the effectiveness of telemedicine in the the setting of infectious diseases [14], moreover, during the SARS-CoV-2 pandemic telehealth has been developed further. In the province of Shandong in China, an ID consulting service has been established through a digital platform cutting time and expenses, while decreasing the risk of spread of SARS-CoV-2 infection by avoiding close contacts with affected patients [15]. Moreover, ID teleconsultation has been also associated with low ICU mortality and low ICU length of stay in patients with sepsis [16, 17].
In the development of ID telemedicine, however, few concerns are to be considered. The lack of digital literacy can be frustrating, but few sessions of training could help to identify simple digital solutions. The management of personal data must be in line with data protection laws especially in the European Union [18, 19]. A delay in releasing ID teleconsultations occurred when untenable patient volumes overwhelmed EDs. However, the number of available ID professionals has increased in response to the surging demand for ID TCs, particularly on night and during holidays. The use of videoconference system integrated in the ADVICE platform is not widely spread. Easy-to-use and inexpensive technological solutions could be the solution to move towards from ID teleconsultation to a tele visit with the patient remote view. Finally, this is a cross-sectional survey with no prospective longitudinal data. In the future, ADVICE platform database could be linked to the regional health care system platform, fully respecting data protection European regulation.
Finally, apart from pandemic scenarios, it is mandatory to take advantage of new digital technologies in the medical setting, that overcoming physical barriers and supporting general or ED physicians in peripheral hospital to have bedside evidence-based clinical advices.
Implementing a standardized telemedicine intervention model will overcome the increasing limitation of human and technical resources, will save time and costs and will help to maintain a high standard of care even in peripheral district.
Availability of supporting data
Data used to support the findings of this study are available from the corresponding author upon request.
References
Smith AC, Thomas E, Snoswell CL, Haydon H, Mehrotra A, Clemensen J et al (2020) Telehealth for global emergencies: Implications for coronavirus disease 2019 (COVID-19) [Internet]. Vol. 26, Journal of Telemedicine and Telecare. SAGE Publications. p. 309–13. Available from: https://doi.org/10.1177/1357633X20916567
Anthony B Jnr Use of telemedicine and virtual care for remote treatment in response to COVID-19 Pandemic J Med Syst. 2020 Jun 15;44(7):132. https://doi.org/10.1007/s10916-020-01596-5.
Sethuram C, Helmer-Smith M, Karunananthan S, Keely E, Singh J, Liddy C. Electronic consultation in correctional facilities worldwide: a scoping review BMJ Open. 2022 Aug 3;12(8):e055049. https://doi.org/10.1136/bmjopen-2021-055049.
Nguyen CT, Olson G, Pho MT, Lew AK, Pitrak D, Satzman J et al (2020) Automatic ID consultation for inpatients with COVID-19: Point, counterpoint, and a single-center experience [Internet]. Vol. 7, Open Forum Infectious Diseases. Oxford University Press (OUP); Available from: https://doi.org/10.1093/ofid/ofaa318
http://www.regione.lazio.it/statistica/it/lazio-in-numeri/popolazione-e-famiglie/popolazione. Last Accessed Apr 2022
Decreto del Commissario ad Acta N U 58, del 12 .07.2010 “ La rete assistenziale delle Malattie Infettive” Available from https://www.inmi.it/bedmanager. Last Accessed Apr 2022
Decreto del Commissario Ad Acta N U00452, del 29.09.2015 “Piano Regionale per la Sorveglianza e la Gestione di Emergenze Infettive durante il Giubileo Straordinario 2015 – 2016 “.Available from https://www.inmi.it/bedmanager. Last Accessed Apr 2022
Decreto del Commissario Ad Acta N. U00540, del 12.11.2015 “Percorso assistenziale per la gestione dei casi con patologia infettiva primaria o associata a comorbidità “ Available from https://www.inmi.it/bedmanager. Last Accessed Apr 2022
Delibera di Giunta regionale del 30 ottobre 2018, n. 626, “Programma di miglioramento e riqualificazione (art. l, comma 385 e ss. Legge 11 dicembre 2016 n. 232) Intervento 2.1 Telemedicina nelle Reti Ospedaliere dell'Emergenza. Attivazione della piattaforma "ADVICE" per il teleconsulto fra centri "Hub" e "Spoke" delle Reti dell'Emergenza, Tempo-dipendenti e delle Malattie Infettive” Available from https://www.regione.lazio.it/sanità Last Accessed Apr 2022
Elrod JK, Fortenberry JL. The hub-and-spoke organization design: an Avenue for serving patients well. BMC Health Serv Res 2017;17:457
Devarakonda S (2016) Hub and spoke model: making rural healthcare in India affordable, available and accessible. Rural Remote Health. 16(1):1–8.
Anderson E, Rinne ST, Orlander JD, Cutrona SL, Strymish JL, Vimalananda VG. Electronic consultations and economies of scale: a qualitative study of clinician perspectives on scaling up e-consult delivery Am Med Inform Assoc. 2021 Sep 18;28(10):2165-2175. https://doi.org/10.1093/jamia/ocab139.
Liu VX, Fielding-Singh V, Greene JD, Baker JM, Iwashyna TJ, Bhattacharya J, Escobar GJ. The Timing of Early Antibiotics and Hospital Mortality in Sepsis Am J Respir Crit Care Med. 2017 Oct 1;196(7):856-863. https://doi.org/10.1164/rccm.201609-1848OC.
Monkowski D, Rhodes LV III, Templer S, Kromer S, Hartner J, Pianucci K et al (2019) A Retrospective Cohort Study to Assess the Impact of an Inpatient Infectious Disease Telemedicine Consultation Service on Hospital and Patient Outcomes [Internet]. Clinical Infectious Diseases. Oxford University Press (OUP). Available from: https://doi.org/10.1093/cid/ciz293
Song X, Liu X, Wang C (2020) The role of telemedicine during the COVID-19 epidemic in China—experience from Shandong province [Internet]. Vol. 24, Critical Care. Springer Science and Business Media LLC. Available from: https://doi.org/10.1186/s13054-020-02884-9
Young LB, Chan PS, Lu X, Nallamothu BK, Sasson C, Cram PM (2011) Impact of Telemedicine Intensive Care Unit Coverage on Patient Outcomes [Internet]. Vol. 171, Archives of Internal Medicine. American Medical Association (AMA). Available from: https://doi.org/10.1001/archinternmed.2011.61
Udeh C, Perez-Protto C, Canfield CM, Sreedharan R, Factora F, Hata JS.. Outcomes Associated with ICU Telemedicine and Other Risk Factors in a Multi-Hospital Critical Care System: A Retrospective, Cohort Study for 30-Day In-Hospital Mortality Telemed J E Health. 2022 Mar 16. https://doi.org/10.1089/tmj.2021.0465. Online ahead of print.
https://www.garanteprovacy.it/regolamentoue/formazione/ last Accessed July 2021
Li P, Luo Y, Yu X, Wen J, Mason E, Li W et al (2020) Patients’ Perceptions of Barriers and Facilitators to the Adoption of E-Hospitals: Cross-Sectional Study in Western China [Internet]. Vol. 22, Journal of Medical Internet Research. JMIR Publications Inc.; p. e17221. Available from: https://doi.org/10.2196/17221
Funding
This study was supported by Italian Ministry of Health (Line1 Ricerca Corrente: Studio dei patogeni ad alto impatto sociale: emergenti, da importazione, multiresistenti, negletti).
Author information
Authors and Affiliations
Consortia
Contributions
GM, NB, AC carried out study conception and design; GM,NB, SV, DB wrote the manuscript; GM, NB and VZ have participated in the research and acquisition of data; TC, GS, SR have supported and contributed to the realization of the web platform; COVID Group of the Lazio Region and Bed Manager group INMI Spallanzani have been involved in the clinical management of patients; GI, FNL and EN critically revised the manuscript and approved its final version. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval
Ethical approval was not required since data were truly anonymized.
Informed consent
Not applicable.
Conflict of interest
All authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Maffongelli, G., Bevilacqua, N., Vita, S. et al. Telemedicine During COVID-19 Pandemic: Lesson Learned from the Lazio Region Infectious Diseases and Emergency Department Network. J Med Syst 46, 105 (2022). https://doi.org/10.1007/s10916-022-01887-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10916-022-01887-z