
Abstract
This study explores the prevalence of physical, sexual and emotional intimate partner violence in Myanmar, attitudes towards violence, and the association between wealth and intimate partner violence. We analysed a nationally representative sample of 3425 married women aged 15–49 years from Myanmar Demographic and Health survey 2015–2016. In this cross-sectional study, data was collected by in-person interviews using a standardized questionnaire. Wealth was operationalized into five groups depending on how much the household owns. Intimate partner violence was measured based on the standard methods of Demographic and Health Survey. The overall prevalence of intimate partner violence (physical, sexual and emotional) was 20.6% (95% confidence interval (95% CI) 18.9–22.3). Less severe physical intimate partner violence was reported by 14.8% (95% CI 13.5–16.3), while 4.4% (95% CI 3.8–5.2) reported severe physical violence. The prevalence of sexual and emotional violence were 2.8% (95% CI 2.2–3.6) and 13.1% (95% CI 11.7–14.6), respectively. Many women believed that a husband has the right to beat his wife if she acts inappropriate, with the highest prevalence at 43% of the women justifying beating if the wife neglects her children. In logistic regression analysis, low wealth as compared with higher wealth, was associated with a higher prevalence of intimate partner violence. The results reveals that intimate partner violence against ever-married women in Myanmar is present, that many women justify beating, and that wealth and intimate partner violence is associated.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The United Nations defines intimate partner violence (IPV) as “Any behavior within an intimate relationship that causes physical, psychological or sexual harm to those in the relationship” (Garcia-Moreno et al. 2012a). IPV is a worldwide problem that has no religious, ethnical or cultural constraints, and all forms (both physical, emotional and sexual violence) affect the health of the victim (Garcia-Moreno et al. 2012). Some of the known consequences are injuries, depression, anxiety, unwanted pregnancies and sexually transmitted diseases (Garcia-Moreno et al. 2012b).
Myanmar may differ from other countries at the same development level, because of their political history. In 2010, Myanmar went from more than 50 years of military-rule to a military-backed civilian government. The military-rule had isolationist policies that lead to little western influence. Their history has made the country one of the poorest in Asia. Myanmar has weak infrastructure and health services (Central Intelligence Agency [CIA] 2018), and lack a law that criminalizes IPV (Gender Equality Network 2013; Thu Thu Aung 2019). Twenty six percent of population live below the poverty line (Central Intelligence Agency [CIA] 2018). The current government aim at increasing the health budget, which is among the lowest in the world (Latt et al. 2016). In order to establish the current status and needs that will help improve the health services, Myanmar is in need of surveys of its health situation, which is scarce from before the election in 2010 (Parmar et al. 2014). Important questions are therefore, what do we know about the presence of intimate partner violence in Myanmar? Does Myanmar differ from the neighboring countries and how are the rates in Myanmar compared to the rest of the world? Does the poverty of Myanmar attribute to high rates of violence?
A study from 2005, of 286 married women aged 18–59 years old from five wards (a subdivision of an urban township) in Myanmar, showed that the prevalence of IPV was 69% (Kyu and Kanai 2005). Sixty nine percent of the responders had experienced psychological aggression, and 27% of the responders reported physical assault. The same study found no significant correlation between household income and intimate partner violence. However, results may have been distorted due to an overrepresentation of low and middle-income participants.
The neighboring countries of Myanmar show great variation in prevalence of intimate partner violence. The prevalence ranges from 15% of Thai women reporting having experienced partner violence (Chuemchit et al. 2018), to 49% of ever-married women in Bangladesh reporting having experienced physical IPV (based on data from Bangladesh Demographic and Health Survey) (National Institute of Population Research and Training [NIPORT], Mitra and Associates,, and Macro International 2009).
In 2013, the World Health Organization (WHO) did a systematic search (García-Moreno and Pallitto 2013) in a number of databases to gather information about violence against women. Global and regional presence of physical and sexual intimate violence were estimated. According to WHO (García-Moreno and Pallitto 2013), IPV has a worldwide prevalence of 30% for women. The highest prevalence of IPV was in Africa, Eastern Mediterranean and South East Asia at 37%. The high-income regions had the lowest prevalence of IPV at 23%. This research had some weaknesses, for example, some countries had no cross-country data on intimate partner violence, and were therefore not included in the estimates. They also did not include emotional IPV in their estimated prevalence of global and regional intimate partner violence (García-Moreno and Pallitto 2013).
Previous studies are inconsistent when attending the question on whether there is an association between wealth and intimate partner violence. Wealth is an indicator of socioeconomic status, and thus among the social determinants for health, “the conditions in which people are born, grow, work, live, and age, and the wider set of forces and systems shaping the condition of daily life” (World Health Organization n.d.). A study from Bangladesh in 2012 found, in bivariate analysis, that women from lower wealth quintile or with lower educational level were more likely to be exposed to intimate partner violence (Ziaei et al. 2014). In the study “Intimate partner violence in the United States – 2010” authors reported that women with a current combined household income under 50,000 US dollars had a significantly higher prevalence of rape, physical violence or stalking by their current partner than those with a household income above 50,000 US dollars. This indicates an association between income and IPV (Basile et al. 2014). On the other side, a study from Ghana using data from Ghana Demographic and Health Survey (Tenkorang et al. 2013) found that wealth status was not a significant predictor for IPV. Similar to Ghana, Myanmar is a Lower Middle Income Country, according to the World Bank (The World Bank Group 2019), but Myanmar is also listed among the world’s least developed countries (Organisation of Economic Co-operation and Development 2020). An interesting question is, if there is an association between wealth and IPV in Myanmar, where most of the population belongs to the low social class and 26% are living under the poverty line (Central Intelligence Agency [CIA] 2018). Myanmar has faced many problems and stressors over the past decades, which could negatively affect people’s attitudes and behavior towards IPV. These factors include military rule (1962–2011), natural disasters, economic crisis, violence, wars and migration (Stokke et al. 2018). Financial stress often affects both individuals and the couple (Mason and Smithey 2012), and is a commonly cited antecedent to IPV perpetration (Byun 2012; Neff et al. 1995; Slep et al. 2010). In a study of the association between financial stress and different forms of IPV perpetration (only minor; only severe; minor and severe; minor, severe, and causing injury; compared with no perpetration), it was shown that both the number of stressors experienced and several types of financial stressors were associated with perpetrating each type of IPV (Schwab-Reese et al. 2016). The findings of an association between financial stressors and interpersonal violence was recently confirmed in analyzes with adjustment for three dopamine genes (DAT1, DRD2, and DRD4) which have been associated with interpersonal delinquency, aggression, and violence when individuals experience adverse environmental exposures (Schwab-Reese et al. 2017).
A report from Myanmar Demographic and Health survey 2015–2016 (MDHS) has given a brief overview on IPV in Myanmar (Ministry of Health and Sports Nay Pyi Taw 2017). With access to the MDHS original data set, this article aim at describing in more detail the occurrence of intimate partner violence, both physical, sexual and psychological, as well as attitudes towards intimate partner violence, and the association between wealth and intimate partner violence.
Methods
Ethical Considerations
An independent ethics committee, the ICS Institutional Review Board (IRB), has approved the research methods and the Demographic and Health survey (DHS) standard questionnaires (IRB). In addition, The Ethics Review Committee on Medical Research including Human Subjects in the Department of Medical Research of the Ministry of Health and Sports approved the Myanmar Demographic and Health Survey. The project was approved by Norwegian Regional Committees for Medical and Health Research Ethics, REK 2016/1195: Domestic violence, mental health and maternal health in Yangon Region, Myanmar. There was taken special considerations when questions about IPV were asked. The domestic violence questionnaire complied with The World Health Organization’s guidelines from 2001 on how to interview about IPV (Guedenet 2009). These guidelines includes that only one eligible woman per household was randomly selected for the domestic violence questionnaire, the staff were specially trained for interviewing about IPV, the informed consent was reiterated and the interview was only conducted if privacy could be kept through the domestic violence questionnaire. This way, nobody else in the household knew the sensitivity of the issues reported. (Ministry of Health and Sports Nay Pyi Taw 2017). Some of the respondents of the domestic violence questionnaire were given the number to a hotline of female law experts, information about One Stop Crisis Center (OSCC) for gender based violence, and some severe cases were given information to contact Myanmar maternal and child welfare association, Myanmar Women’s Affairs Federation and Department of Social Welfare. Myanmar maternal and child welfare association, Myanmar Women’s Affairs Federation are present in all states and regions.
Data Collection
In this study we have analyzed data from Myanmar Demographic and Health Survey, conducted in 2015–2016. The survey was initiated by the Ministry of Health and Sports of Myanmar, and funded by United States Agency for International Development and Three Millennium Development Goal Fund. MDHS data was collected through the standard procedures, methodologies, and manuals of the DHS-program. First, this included preparation of the survey and questionnaire design to meet the needs of Myanmar. Second, field staff were trained, and eligible households and individual respondents were identified and interviewed in their homes. The interviews of women were conducted by female interviewers. The third stage consisted of data processing. This took place simultaneously as the second stage so that they could control the quality of collected data, in terms of missing data (Demographic and Health Survey [DHS] n.d.-c). For the questions about IPV the interviewers were provided additional training on administering the questions, dealing with crisis situations, avoiding further endangering of the respondents, and preparing themselves emotionally (Demographic and Health Survey [DHS] n.d.-b). A pretest was performed by 22 interviewers in one urban and two rural locations of Mandalay. After the test there was a debriefing, and the questionnaires were modified thereafter. The DHS method has been used by many countries to report the country’s health situation, and to explore health trends when studies have been repeated, though many countries has chosen to not include the domestic violence questions (Demographic and Health Survey [DHS] n.d.-a, n.d.-d).
Study Population and the Process of Selecting Households and Women for the Domestic Violence Module
Myanmar conducted the DHS survey for the first time in 2015–2016. The sampling frame consisted of 76,990 primary sampling units (PSUs) across the country. A PSU is either a census enumeration area (EA) from the 2014 Myanmar census, or a ward or village tract in a sensitive area not enumerated during the census. For example, 1.09 million Rohingyas in Rakhine State, bordering to Bangladesh, were not enumerated in the 2014 census, but were a part of the sampling frame in the present study. In order to end up with a final sample of women who have responded to the women questionnaire and the domestic violence (DV) module, a number of stages and procedures were followed. The first stage involved selecting clusters consisting of census enumeration areas (EAs) or ward/village tracts. For each PSU information about state/region and district, urban or rural location and number of households were known. A master sample of 4000 primary sampling units (PSUs) were randomly selected from the sampling frame. This sample was selected proportional to the population size of the states and to the proportion living in urban wards (approximately 30%) vs. rural villages (approximately 70%). From the master sample, 442 clusters (123 urban and 319 rural) were randomly selected from the master sample. At the second stage, a fixed number of 30 households was selected from each of the selected clusters, using equal probability systematic sampling. A total of 13,238 households were selected, and among them, there were 12,780 households with persons. Out of them, 12,500 households were interviewed. A household questionnaire was used to identify all eligible men and women aged 15–49 years who stayed in the household the night before the survey, and to collect information at household level.
The woman’s questionnaire was given to all eligible women aged 15–49 years, in all households. The men’s questionnaire was given to all eligible men aged 15–49 years, in half of the households. The domestic violence questionnaire was given to one woman, aged 15–49 years, in the subsample of households selected for the men’s survey.
Of the interviewed households, 13,454 women were identified as eligible for women questionnaire, and 12,885 (95.8%) were successfully interviewed. In the subsample of one half of the households, 5218 men were identified as eligible for individual interview, and among them, interviews were completed in 4737 men (90.8%).
In total, 4563 women received the domestic violence questions, and 4517 (99%) were successfully interviewed. Reasons for non-response were mainly no privacy established. Out of the 4517 women, 3425 were ever married, and thus, constituted the final sample (Fig. 1).

Flowchart of women included in analysis
The interviewers of the Woman’s Questionnaire, and the Domestic Violence Questionnaire, were females. Prior to administering the domestic violence questions the informed consent from the participant was reiterated. Also privacy was ensured, and the interview would not be continued if privacy was not reobtained (Demographic and Health Survey [DHS] n.d.-b). For further information about the methods used, see the Myanmar DHS report (Ministry of Health and Sports Nay Pyi Taw 2017).
Measures
The questionnaires have been translated from English to Myanmar language, and back-translated. Also a pilot study was conducted. The questionnaires, developed for the worldwide DHS program, were revised to accord with Myanmar culture as well as to reflect some country-specific health issues.
Measures of Violence
Ever experienced any IPV was in the MDHS data divided into four domains: ever experienced any less severe violence by husband/partner (physical), ever experienced any severe violence by husband/partner (physical), ever experienced any emotional violence by husband/partner and ever experienced any sexual violence by husband/partner. Less severe physical violence includes the women’s experience of actions such as ever having been pushed, shook or had something thrown at her, slapped, punched, gotten arm twisted or hair pulled by husband/partner. Severe physical violence was measured by the women’s report of ever having been kicked or dragged, strangled or burnt, or threatened with knife/gun or other weapon by husband/partner. Emotional violence includes ever having been humiliated, threatened with harm, been insulted or made to feel bad by husband/partner. Sexual violence was measured by the women’s report of ever having been physically forced into unwanted sex by husband/partner, forced into other unwanted sexual acts by husband/partner or physically forced to perform sexual acts respondent didn’t want to. The questions were answered with dichotomous response options (“yes” or “no”). We analyzed these four domains separately and constructed a combined (“ever experienced any IPV”) with “yes” or “no” as the possible outcomes.
Measure of Wealth
In MDHS the household wealth is represented in a wealth index. The wealth index was constructed by MDHS, through the following process: Wealth of the household was operationalized into five groups of poorest, poorer, middle, richer, richest. The index was created by giving each household an asset score based on consumer goods they owned as well as housing characteristics. Consumer goods could range from a mobile phone to a bicycle or car, and housing characteristics could include source of drinking water, toilet facilities, and flooring materials. These scores are derived using principal component analysis. The wealth quintiles at national level are compiled by giving the household score to each household member. Then the participants are ranked by their score, and then divided into five equal categories (quintiles), each with 20% of the participants. Since our study has not used the national sample, but a subsample of ever-married or partnered women, our subgroups of the wealth index are not equal in number. Further information about the wealth index and how it is created is written elsewhere (Demographic and Health Survey; Rutstein n.d.).
Measure of Attitudes towards Violence
Women’s attitudes towards wife-beating, included the following MDHS variables: beating justified if wife goes out without telling husband, if wife neglects children, if wife refuses to have sex, if wife argues with husband, if wife burns the food, if wife refuses to use contraception and if wife is involved in too much social activity. These were each answered with “yes” or “no”.
Constructed Variables
New variables were constructed so that age was divided into three groups (15–29,30-39,40–49), and total children ever born into four groups (0, 1–4, 5–8, 9–12). Other MDHS variables included were states and regions (a total of 15), place of residence (urban, rural), highest educational level (no education, primary, secondary, higher), husband/partners educational level (no education, primary, secondary, higher) and respondent currently working (yes, no). Primary education includes grades 1–6, while secondary education constitutes grades 7–11.
Data Analysis
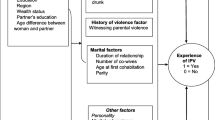
The data was analysed using Stata MP 15. We declared complex survey data by using ‘svyset’, and the survey prefix command ‘svy’ was used in the analysis in order to incorporate the complex survey design. Univariate and bivariate analysis were used to describe the variables of interest. In order to get answers to the research question about the occurrence of IPV, we have used Wald Chi-Squared test for testing differences in IPV between subgroups of the population. The strategy for analyzing data is based on drawing of a directed acyclic graph (DAG) (Textor et al. 2016) (Fig. 2). The graph shows that age, education of both respondent and husband/partner, whether the respondent is currently working or not and frequency of husband/partner being drunk are associated with both the exposure (wealth) and the outcome (intimate partner violence), and are not intermediate variables. They are therefore confounders. In order to get answers to the research question if there is an association between wealth index and IPV, we applied binary logistic regression analyses, estimating odds ratio (OR) with 95% confidence interval (CI).. The rationale for using binary logistic regression is that the outcome has dichotomous response alternatives (experienced any IPV - yes/no). We present the results of the logistic regression as crude OR and OR adjusted for the following confounders: age, respondent is currently working, highest educational level and husband/partner’s educational level. No interaction was found between wealth index and confounders. All the analyses were weighted, so they would be representative at a national and regional level.

Directed acyclic graph (DAG) (Textor et al. 2016) of the association between wealth and intimate partner violence (IPV) among married women in Myanmar, identifying confounders (red) associated with both exposure and outcome and mediators (blue) which are intermediate variables between exposure and outcome
Results
The sociodemographic characteristics of participants are described in Table 1. One-fourth of the population lives in urban areas. The majority of women (77%) had finished primary or secondary school, only 7% had higher education and 15% had no education. The distribution was about the same for their husband or partner. Almost two-thirds of the respondents were currently working.
Intimate Partner Violence
The prevalence of IPV was 20.6% (95% CI 18.9–22.3) (Table 2), and increasing with poorer wealth, from 14% (richest) to 27% (poorest) (Table 1). The prevalence also increased with lower education and with increasing number of children. The prevalence of IPV showed wide variation across the 15 states and regions in Myanmar, being highest in Rakhine State at 40%. Unexpectedly, we found no increase in the prevalence of IPV by increasing age (Table 1).
Physical Violence
The prevalence of less severe physical violence was 14.8% (95% CI 13.5–16.3) (Table 2), which is the highest among all four subgroups. Severe IPV was reported by 4.4% (95% CI 3.8–5.2) (Table 2). The proportion of physical IPV varied a lot between the regions in Myanmar. Rakhine and Taninthayi were the ones with most physical IPV, while women in Shan and Mandalay reported the lowest rates. The share of women who reported physical violence from their husbands increased the poorer the women were. The prevalence of less severe- and severe physical violence, were lower in the richer- and richest wealth-index-groups as compared with the poorest group (less severe physical IPV: 8.6% (95% CI 6.4–11.5) vs. 20.3 (95% CI 17.4–23.6); severe physical IPV: 1.8% (95% CI 1.0–3.3) vs. 6.7% (95% CI 5.1–8.7)) (Table 3). There was no difference in prevalence between urban or rural living. The women with higher educational level than secondary had a lower prevalence of less severe and severe physical abuse than those with less education. Also, when the husband had higher level of education, the lower was the prevalence of physical violence (Table 3).
Sexual Violence
The prevalence of sexual IPV was 2.8% (95% CI 2.2–3.6) (Table 2). The occurrence of sexual IPV was found to decrease with increased wealth index (Table 3). The prevalence of sexual IPV was statistically lower among the richer wealth-group as compared with the poorest group (1.1% (95% CI 0.6–2.0) vs 3.9% (95% CI 2.6–5.9)) (Table 3). Women having a husband with higher level of education, as compared with lower educational level, reported less sexual violence (0.1% (95% CI 0.0–0.5) vs. 3.6% (95% CI 2.1–6.1)) (Table 3). The highest rates of violence was found in the regions Rakhine (12.7%) and Kayah (10.2%), and the lowest prevalence in Mandalay (0.5%) (Table 3).
Emotional Violence
Thirteen percent (95% CI 11.7–14.6) of the women reported having been exposed to emotional violence from husband or partner (Table 2). The poor and the families with many children, had a higher prevalence of emotional violence than the rich and the ones with fewer children (Table 3). Taninthayi (26.3%) and Rakhine (25.8) had highest presence of emotional violence performed by their intimate partner, while the lowest prevalence was reported in Yangon (6.3%) (Table 3).
Attitudes
Forty-three percent of the women believed that beating the wife is justified if the wife neglects the children (Table 4). Many of the women agree that the husband can beat his wife if she goes out without telling the husband (24%) or if she is involved in too much social activity (15%). If the wife argues with the husband, refuses to have sex with the husband or refuses to use contraception, about 11% of the women legitimize beating. Thirteen percent of the women also believed that beating is allowed if the wife burns the food (Table 4).
Association between Wealth Index and Intimate Partner Violence
In crude (Model 1) and adjusted analysis (Model 2), wealth index showed an association with intimate partner violence (Table 5). Adjustment for confounders (age, respondent is currently working, highest educational level and husband/partners highest educational level) (Model 2) did not change the estimates much from the crude analysis. We found significant associations with IPV for all categories of wealth, as compared with the poorest quintile: poorer wealth (OR = 0.76; 95% CI 0.58–1.00), middle wealth (OR = 0.58; 95% CI 0.43–0.78), rich (OR = 0.56; 95% CI 0.39–0.79) and richest (OR = 0.50; 95% CI 0.33–0.74). The results indicate that the rich experience less IPV than the poor.
Discussion
In this nation-wide study of 15–49 year old women in Myanmar, the prevalence of IPV was 20.6%. We found the prevalence of less severe physical IPV to be 14.8% and severe physical IPV to be 4.4%. Sexual violence was the rarest subgroup of IPV (2.8%), while emotional violence was about as common as less severe physical violence (13.1%). Presence of spousal violence varied considerably between the regions, of which the highest prevalence was found in Rakhine and Taninthayi. Based on logistic regression analyses, we found low wealth to be associated with a higher rate of intimate partner violence. We also found 43% of the women themselves meant beating is justified if the wife neglects the children, and that 13.1% agrees beating is justified if the wife burns the food.
Our Findings Compared to Other Countries
The World Health Organization has estimated a worldwide prevalence of IPV at 30% and a prevalence of 37% in South East Asia. Our study finds an overall prevalence of IPV in Myanmar at 20.6%. The discrepancy might be caused by an actual difference between Myanmar and the other countries. Culture and politics in Myanmar may differ from other countries in South East Asia and lead to lower presence of violence.
However, our findings could be an underestimation of intimate partner violence. In our study, the domestic violence module is added to a larger study that addresses a variety of topics. The reported prevalence of IPV is usually lower with this design than in surveys that only concern violence (Kataoka et al. 2010).
In our study, the data were collected through interviews. As IPV is associated with shame and negative feelings, it is likely that participants underreport their experience of violence. Thus, this is a possible explanation of our findings of a lower prevalence of violence than WHO. Some studies argue that a self-administered questionnaire is a better way to research IPV (Kataoka et al. 2010; Webster and Holt 2004). On the other hand, Myanmar has a rate of literacy of 85% among women (Ministry of Health and Sports Nay Pyi Taw 2017). Therefore, a written self-administered questionnaire would exclude 15% of women in Myanmar from the study. This implies that, even though a self-administered questionnaire might be a better methodology for research on intimate partner violence, this would not apply to Myanmar, caused by the fact that 15% of the women in Myanmar cannot read and could therefore not complete a self-administered questionnaire.
IPV is measured in different ways in other surveys. There is no universal agreement on the definition of- and what should be included in the term IPV (European Institute for Gender Equality [EIGE] 2016). This is likely to influence the results of the studies. WHO’s estimates of violence is based on a systematic review were the authors included any definition of IPV by the different authors. The lower prevalence in our study may be a result of the definitions used. However, Bangladesh, a neighboring country to Myanmar, did the Demographic and Health survey in 2009 with the same domestic violence module as used in our study. 49% of the women in Bangladesh reported ever having experienced physical intimate partner violence (National Institute of Population Research and Training [NIPORT] et al. 2009). The result implies that Bangladesh has a higher prevalence of physical violence than Myanmar. Given that results from Bangladesh are close to WHOs estimates for South East Asia, this may indicate that IPV is lower in Myanmar than the average for the region.
We found an association between wealth index and intimate partner violence. Other studies from Bangladesh, using data from Bangladesh Demographic and Health Survey (Ziaei et al. 2014) and USA (Basile et al. 2014) support our finding of an association between wealth and IPV. However we note, a study from Ghana (Tenkorang et al. 2013), which is also based on a national Demographic and Health survey, did not find a relationship.
Strengths and Limitations
A strength of our study is the inclusion of persons without a citizenship. As described in the methods section, independent household listing operations were performed to include persons who was not included in the 2014 census frame, as the census excluded inhabitants who could not prove a citizenship. This is particularly important in Rakhine State, where a large group of 1.09 million Rohingyas were not enumerated in the census (United Nations Fund for Population Avtivities [UNFPA] 2016). This group represents one third of the state population (Department of Population 2015), and might contribute to the high prevalence of IPV in Rakhine State. It is known being an ethnic minority is a risk factor for IPV (Gerino et al. 2018). Rakhine State border to Bangladesh, and if there is any exchange of culture or behavior across the border, the high prevalence of IPV found in Rakhine is only slightly lower than the prevalence of physical violence of 49% reported in Bangladesh (National Institute of Population Research and Training [NIPORT] et al. 2009).
An important limitation to this study is the lack of testing for validity and reliability. However, some of the following facts may have improved the internal validity of the study and/or reliability of instruments: we applied standard DHS methodology used in many countries; questionnaires were translated from English to Myanmar language, and back-translated; the instruments have been piloted and adjusted to Myanmar culture and fieldworkers have been well trained.
Another limitation in the present study is caused by the cross-sectional design. This design gives a picture of the circumstances during the survey, but the dimension of time is not represented in the data. Although we can find an association between wealth and IPV with binary logistic regression analysis, the study cannot confirm a causal relationship. We can therefore not be sure that an economic lift would lead to less violence, though this is likely.
A third weakness of the analysis is the failure of adjusting for all potential confounders (i.e. unmeasured confounders). For example, “frequency of husband/partner being drunk” could not be included in the analysis, because of missing data for most of the participants on this variable. We did not design the survey, and had no influence over which questions were asked to the participants.
Another limitation is that women were systematically excluded if the interview could not be completed privately, that is to say without husband or partner being present. Because men who perform IPV often have controlling behavior, this likely excluded women who were exposed to IPV (Aizpurua et al. 2017). This means that our results would underestimate the prevalence of IPV. We do not know the reasons why the household response rate was low, but among those who received the DV questions, only 1 % did not respond, the main reason being lack of privacy. Thus, this type of bias would most likely not lead to major changes in the results.
Conclusion and Implications
We find IPV to be prevalent in Myanmar, although less prevalent than in the region. Many women think that their husband has a right to pursue violent methods if the wife acts inappropriately. Our study also finds an association between wealth and intimate partner violence.
Despite the limitations mentioned, the study is an important contribution to mapping women’s experience of violence in Myanmar. We believe information and legal steps could reduce the level of violence. This could include the government of Myanmar, as well as non-governmental organizations. Since 2013, the Gender Equality Network has tried to promote a law in Myanmar criminalizing domestic abuse. However, the implementation of this law keeps getting delayed (Thu Thu Aung 2019). A legal framework, supported by information, could change behavior and attitudes both in men and women in Myanmar. It is necessary not only to address men in this work, but also to address women’s attitudes and norms towards violence. Social acceptance of IPV perpetuates violence. Attitude campaigns, especially if supporting a legal framework, could lead to changes in mindset, and thus lead to less violence. Increasing the wealth of the poor could be a strategy to decrease IPV and concomitant improve the health of women of Myanmar. However, given the limitations of our study, it is still open whether wealth itself, or another factor like educational level of women is the key driver to reduce violence. There is also need for a health system with services that can help victims of IPV, and governmental social and financial support for these women.
We suggest further research to identify effective governmental actions to reducing intimate partner violence. Also research related to the association between wealth and intimate partner violence is welcomed. We should better define a causal relationship between wealth and violence. New surveys are necessary to follow trends in prevalence and risk factors for IPV, providing estimates as unbiased as possible with respect to underestimation of IPV. It will also be important with increased research about why men perpetrate intimate partner violence. Lastly, to the knowledge of the author, there are few surveys worldwide, and no surveys in Myanmar that investigate men as the victim of intimate partner violence. Therefore, this would be intriguing fields to investigate.
References
Aizpurua, E., Copp, J., Ricarte, J. J., & Vazquez, D. (2017). Controlling behaviors and intimate partner violence among women in Spain: an examination of individual, partner, and relationship risk factors for physical and psychological abuse. Journal of Interpersonal Violence, 886260517723744. https://doi.org/10.1177/0886260517723744. (Accession No. 29294888).
Basile, K., Black, M., Breiding, M., Mercy, J., Saltzman, L., & Smith, S. (2014). Intimate partner violence in the United States. Retrieved from Atlanta, Georgia: https://www.cdc.gov/violenceprevention/pdf/cdc_nisvs_ipv_report_2013_v17_single_a.pdf
Byun, S.-H. (2012). What happens before intimate partner violence? Distal and proximal antecedents. Journal of Family Violence, 27(8), 783–799. https://doi.org/10.1007/s10896-012-9464-y.
Central Intelligence Agency [CIA]. (2018). Burma - The world factbook. Retrieved from https://www.cia.gov/library/publications/the-world-factbook/geos/bm.html
Chuemchit, M., Chernkwanma, S., Somrongthong, R., & Spitzer, D. L. (2018). Thai women’s experiences of and responses to domestic violence. International Journal of Women’s Health, 10, 557–565. https://doi.org/10.2147/ijwh.s172870.
Demographic and Health Survey [DHS]. (n.d.-a). DHS Model Questionnaires. Retrieved from https://dhsprogram.com/What-We-Do/Survey-Types/DHS-Questionnaires.cfm
Demographic and Health Survey [DHS]. (n.d.-b). Protecting the Privacy of DHS Survey Respondents. Retrieved from https://dhsprogram.com/What-We-Do/Protecting-the-Privacy-of-DHS-Survey-Respondents.cfm
Demographic and Health Survey [DHS]. (n.d.-c). Survey Process. Retrieved from https://dhsprogram.com/What-We-Do/Survey-Process.cfm
Demographic and Health Survey [DHS]. (n.d.-d). Team and partners Retrieved from https://dhsprogram.com/Who-We-Are/About-Us.cfm
Department of Population, M. o. I. a. P (2015). The 2014 Myanmar Population and Housing Census Rakhine State. 3-K. Retrieved from https://myanmar.unfpa.org/sites/default/files/pub-pdf/Rakhine%20State%20Census%20Report%20-%20ENGLISH-3.pdf
European Institute for Gender Equality [EIGE]. (2016). Analysis of national definitions of intimate partner violence. Retrieved from ile:///C:/Users/lisewl/AppData/Local/Packages/Microsoft.MicrosoftEdge_8wekyb3d8bbwe/TempState/Downloads/gbv_natdefn_ipv.pdf.
García-Moreno, C., & Pallitto, C. (2013). Global and regional estimates of violence against women: Prevalence and health effects of intimate partner violence and non-partner sexual violence. Retrieved from Geneva, Switzerland: http://apps.who.int/iris/bitstream/handle/10665/85239/9789241564625_eng.pdf?sequence=1
Garcia-Moreno, C., Guedes, A., Knerr, W., Bott, S., & Ramsay, S. (2012). Understanding and addressing violence against women: overview. Retrieved from http://apps.who.int/iris/bitstream/10665/77433/1/WHO_RHR_12.35_eng.pdf?ua=1
Garcia-Moreno, C., Guedes, A., Knerr, W., Campbell, J., Bott, S., & Ramsay, S. (2012a). Intimate Partner violence. Retrieved from http://apps.who.int/iris/bitstream/handle/10665/77432/WHO_RHR_12.36_eng.pdf;jsessionid=AE43595A138B4E8BB228C5B111D5BCEE?sequence=1
Garcia-Moreno, C., Guedes, A., Knerr, W., Campbell, J., Bott, S., & Ramsay, S. (2012b). Understanding and addressing violence against women: Intimate partner violence. Retrieved from http://apps.who.int/iris/bitstream/10665/77432/1/WHO_RHR_12.36_eng.pdf
Gender Equality Network. (2013). The Case for Anti-Violence Against Women Laws. Retrieved from https://www.burmalibrary.org/docs20/Myanmar_Law+CEDAW-en-red.pdf
Gerino, E., Caldarera, A. M., Curti, L., Brustia, P., & Rollè, L. (2018). Intimate partner violence in the golden age: systematic review of risk and protective factors. Frontiers in Psychology, 9, 1595. https://doi.org/10.3389/fpsyg.2018.01595.
Guedenet, H. (2009). Ethical and Safety Guidelines for Implementing the DHS Domestic Violence Module. Retrieved from https://dhsprogram.com/topics/gender-Corner/upload/DHS_Domestic_Violence_Module_Ethical_Guidelines.pdf
Kataoka, Y., Yaju, Y., Eto, H., & Horiuchi, S. (2010). Self-administered questionnaire versus interview as a screening method for intimate partner violence in the prenatal setting in Japan: a randomised controlled trial. BMC Pregnancy and Childbirth, 10(1), 84. https://doi.org/10.1186/1471-2393-10-84.
Kyu, N., & Kanai, A. (2005). Prevalence, antecedent causes and consequences of domestic violence in Myanmar. Asian Journal of Social Psychology, 8(3), 244–271. https://doi.org/10.1111/j.1467-839X.2005.00170.x.
Latt, N. N., Myat Cho, S., Htun, N. M., Yu Mon, S., Myint, M. N., Aoki, F., et al. (2016). Healthcare in Myanmar. Nagoya Journal of Medical Science, 78(2), 123–134 Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4885812/.
Mason, B., & Smithey, M. (2012). The effects of academic and interpersonal stress on dating violence among college students: a test of classical strain theory. Journal of Interpersonal Violence, 27(5), 974–986. https://doi.org/10.1177/0886260511423257.
Ministry of Health and Sports Nay Pyi Taw, M. (2017). Myanmar Demographic and Health Survey 2015–2016.
National Institute of Population Research and Training [NIPORT], Mitra and Associates, & Macro International. (2009). Domestic violence. In Bangladesh Demograhpic and Health Survey 2007 (pp. 197–214).
Neff, J. A., Holamon, B., & Schluter, T. D. (1995). Spousal violence among Anglos, blacks, and Mexican Americans: the role of demographic variables, psychosocial predictors, and alcohol consumption. Journal of Family Violence, 10(1), 1–21. https://doi.org/10.1007/BF02110534.
Organisation of Economic Co-operation and Development. (2020). DAC List of ODA Recipients. Retrieved from http://www.oecd.org/dac/financing-sustainable-development/development-finance-standards/DAC-List-of-ODA-Recipients-for-reporting-2020-flows.pdf
Parmar, P. K., Benjamin-Chung, J., Smith, L. S., Htoo, S. N., Laeng, S., Lwin, A., Mahn, M., Maung, C., Reh, D., Shwe Oo, E. K., Lee, T., & Richards, A. K. (2014). Health and human rights in eastern Myanmar prior to political transition: a population-based assessment using multistaged household cluster sampling. BMC International Health and Human Rights, 14(1), 15. https://doi.org/10.1186/1472-698x-14-15.
Rutstein, S. O. (n.d.). Steps to constructing the new DHS Wealth Index. Retrieved from https://dhsprogram.com/programming/wealth%20index/Steps_to_constructing_the_new_DHS_Wealth_Index.pdf
Schwab-Reese, L. M., Peek-Asa, C., & Parker, E. (2016). Associations of financial stressors and physical intimate partner violence perpetration. Injury Epidemiology, 3(1), 6. https://doi.org/10.1186/s40621-016-0069-4.
Schwab-Reese, L. M., Parker, E. A., & Peek-Asa, C. (2017). The interaction of dopamine genes and financial stressors to predict adulthood intimate partner violence perpetration. Journal of Interpersonal Violence, 0886260517696841, 1251–1268. https://doi.org/10.1177/0886260517696841.
Slep, A. M. S., Foran, H. M., Heyman, R. E., & Snarr, J. D. (2010). Unique risk and protective factors for partner aggression in a large scale air force survey. Journal of Community Health, 35(4), 375–383. https://doi.org/10.1007/s10900-010-9264-3.
Stokke, K., Vakulchuk, R., & Øverland, I. (2018). Myanmar: A political economy analysis. Retrieved from Norwegian Institute of International Affairs: https://www.nupi.no/en/Publications/CRIStin-Pub/Myanmar-A-Political-Economy-Analysis
Tenkorang, E. Y., Owusu, A. Y., Yeboah, E. H., & Bannerman, R. (2013). Factors influencing domestic and marital violence against women in Ghana. Journal of Family Violence, 28(8), 771–781. https://doi.org/10.1007/s10896-013-9543-8.
Textor, J., van der Zander, B., Gilthorpe, M. S., Liśkiewicz, M., & Ellison, G. T. (2016). Robust causal inference using directed acyclic graphs: the R package ‘dagitty’. International Journal of Epidemiology, 45(6), 1887–1894. https://doi.org/10.1093/ije/dyw341.
The World Bank Group. (2019). Lower Middle Income. Retrieved from https://data.worldbank.org/income-level/lower-middle-income
Thu Thu Aung. (2019). ‘Until her bones are broken’: Myanmar activists fight to outlaw domestic violence. Reuters. Retrieved from https://www.thejakartapost.com/seasia/2019/08/16/until-her-bones-are-broken-myanmar-activists-fight-to-outlaw-domestic-violence.html
United Nations Fund for Population Avtivities [UNFPA]. (2016). UNFPA welcomes release of Myanmar census data on religion. Retrieved from https://myanmar.unfpa.org/news/unfpa-welcomes-release-myanmar-census-data-religion
Webster, J., & Holt, V. (2004). Screening for partner violence: direct questioning or self-report? Obstetrics & Gynecology, 103(2), 299–303. https://doi.org/10.1097/01.AOG.0000110245.83404.3d.
World Health Organization. (n.d.). What are social determinants of health? Retrieved from https://www.who.int/social_determinants/en/
Ziaei, S., Naved, R. T., & Ekström, E.-C. (2014). Women’s exposure to intimate partner violence and child malnutrition: findings from demographic and health surveys in Bangladesh. Maternal & Child Nutrition, 10(3), 347–359. https://doi.org/10.1111/j.1740-8709.2012.00432.x.
Funding
Open access funding provided by University of Oslo (incl Oslo University Hospital).
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Larsen, L.W., Aye, W.T. & Bjertness, E. Prevalence of Intimate Partner Violence and Association with Wealth in Myanmar. J Fam Viol 36, 417–428 (2021). https://doi.org/10.1007/s10896-020-00190-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10896-020-00190-0