
Abstract
Purpose: The aim was to investigate the feasibility and optimal stimulation parameters for supramaximal stimulation of muscle recorded transcranial electrical stimulation motor evoked potentials (mTc-MEP). Methods: Forty-seven consecutive patients that underwent scoliosis surgery were included. First, the feasibility of supramaximal stimulation was assessed for two settings (setting 1: pulse duration 0.075ms, interstimulus interval (ISI) 1.5ms; setting 2: pulse duration 0.300ms, ISI 3ms). Thereafter, three mTc-MEP parameters were considered for both settings; (1) elicitability, (2) amplitude, and (3) if supramaximal stimulation was achieved with ≥ 20 V below maximum output. Finally, ISIs (1ms–4ms) were optimized for setting 1. Results: Nine patients (19.15%) were excluded. Of the remaining patients, supramaximal stimulation was achieved in all patients for setting 1, and in 26 (68.42%) for setting 2. In one patient, mTc-MEPs were elicitable in more muscles for setting (1) Amplitudes were not significantly different. Stimulation voltage could be increased ≥ 20 V in all 38 patients for setting 1 and in 10 (38.46%) for setting (2) Optimal ISI’s differed widely. Conclusion: We recommend using setting 1 when monitoring mTc-MEPs with supramaximal stimulation, after which an individualized ISI optimization can be performed. Moreover, when using supramaximal stimulation, short ISI’s (i.e. 1ms or 1.5ms) can be the optimal ISI for obtaining the highest mTc-MEP amplitude.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
For the past three decades, intraoperative neurophysiological monitoring (IONM) has been used to detect and prevent neurologic injury during high-risk spinal surgery [1, 2]. The sensory tracts can be monitored using somatosensory evoked potentials (SSEPs) [3], while the integrity of motor tracts can be determined using muscle recorded transcranial electrical stimulation motor evoked potentials (mTc-MEPs) [4]. The combined use of SSEPs and mTc-MEPs has become an essential tool for detecting and preventing surgically induced neurological injury during scoliosis surgery [1, 5].
Various mTc-MEP monitoring methods and corresponding warning criteria can be used to determine impending neurological damage. Three main methods have been described. These are: the threshold level method [6, 7], the waveform method [8], and the amplitude reduction method [9]. Langeloo et al. concluded that, even though all three methods can successfully be used for monitoring, the amplitude reduction method is the most sensitive predictor of neurological damage during spinal surgery [10]. Depending on the type of surgery, a decrease of 50 to 100% from the baseline mTc-MEP amplitude is considered a warning [4, 11, 12].
The amplitude reduction method can be applied using either submaximal stimulation or supramaximal stimulation. In submaximal stimulation, the stimulation voltage is usually increased to 20–30% above the threshold stimulation voltage [13]. In supramaximal stimulation, the voltage is increased beyond the voltage necessary to evoke the maximum amplitude of the mTc-MEPs [10, 14]. An advantage of performing supramaximal stimulation is that it yields less variability between consecutive mTc-MEP amplitudes than submaximal stimulation, as has been reported in a case example by Journée et al. [12] A lower variability between measurements could help decrease the number of false positive warnings [15, 16].
When mTc-MEPs are monitored, the responsible neurophysiologist should ideally select a stimulus location and values of the stimulation parameters that generate optimal mTc-MEPs. In addition to the stimulation voltage, other stimulation parameters that can be varied include: stimulus duration, inter-stimulus interval, and number of pulses per train. Although multiple studies have tried to determine the optimal values of these stimulation parameters for eliciting mTc-MEPs, few studies have investigated the optimal stimulation parameters for performing supramaximal stimulation [12, 14, 17]. However, the feasibility of supramaximal stimulation for different stimulation parameters and the optimal stimulation parameters for performing supramaximal stimulation have not been vigorously investigated.
Therefore, the aim of this retrospective study was to investigate the feasibility of supramaximal stimulation for different stimulation parameters, and the optimal stimulation parameters, consisting of pulse duration and ISI, for performing supramaximal stimulation in patients undergoing scoliosis correction surgery.
2 Materials and methods
2.1 Study design
This is a retrospective observational study. Since the data analyzed in this study were collected during routine clinical care, the ethical committee of University Medical Center Groningen (UMCG) waived the requirement for full ethical committee review in accordance with the terms of the Dutch Act on Medical Research on Human Subjects (Wet Medisch-Wetenschappelijk Onderzoek, or ‘WMO’).
2.2 Patients
The study data were collected from May 2018 until May 2019. Forty-seven consecutive patients undergoing scoliosis correction surgery with IONM were included.
2.3 mTc-MEP monitoring
Intraoperative mTc-MEP monitoring was performed using a constant-voltage stimulator (NIM-Eclipse E4 IONM system, Medtronic BV, The Netherlands). Motor evoked potentials were measured using biphasic transcranial electrical stimulation [18]. For transcranial electrical stimulation, corkscrew electrodes (Medtronic, Xomed, Jacksonville, FL) were placed at location Cpl1-Cpl2 (1 cm posteriorly, 1 cm laterally from C1 resp C2) altered from the international 10–20 EEG System. Motor evoked potentials were recorded using surface electrodes (20 × 27 mm, adhesive surface pad electrodes, Medtronic, Xomed, Jacksonville, FL) from the left and right tibialis anterior muscle (TA), and the left and right abductor hallucis muscle (AH).
After anesthetic induction but before incision, mTc-MEPs were measured using two different settings. Setting 1 consisted of a pulse duration of 0.075ms and an ISI 1.5ms, while setting 2 consisted of a pulse duration of 0.300ms and an ISI 3ms. The maximum current output for was ± 1000mA for setting 1 and ± 180mA for setting 2, which are within the IEC safety limits [19]. The stimulation parameters are shown in Table 1.
2.4 Feasibility of supramaximal stimulation
For both setting 1 and setting 2, the feasibility of supramaximal stimulation was evaluated. To assess whether supramaximal stimulation was feasible, voltage intensity curves were produced by increasing the voltage in predefined steps of 10-20 V. Voltage intensity curves were determined per patient for both stimulation settings, and all four muscles separately (AH left and right, TA left and right). The mTc-MEP amplitudes were log-transformed and fitted to Sigmoidal-Boltzmann curves using GraphPad Prism (version 8.4.2, GraphPad Software, San Diego, California USA).
Two independent researchers (SED, GD) subsequently evaluated all curves to determine if supramaximal stimulation was achieved. Supramaximal stimulation was considered to have been achieved if the graph displayed a typical sigmoidal pattern with a plateau at the end of the curve.
The voltage intensity at which supramaximal stimulation was achieved was defined as the voltage necessary for the second log-amplitude on this plateau, in which it was verified that the log-amplitudes did not increase with higher voltage intensities (Fig. 1 A).

Example Sigmoidal Boltzmann curves for setting 1 (A) and setting 2 (B)
The x-axis denotes the stimulation voltage used for eliciting the mTc-MEP amplitude. The y-axis denotes the logarithm of the mTc-MEP amplitude in µV. The graphs are altered from real data
(A) supramaximal stimulation was achieved for setting 1 since a plateau was reached (green). In blue, the voltage intensities with the possibility to increase the voltage intensity with ≥ 20 V is shown
The red dots represent the voltage motor threshold and the voltage intensity at which supramaximal stimulation was achieved (the second log-amplitude of the plateau). (B) Supramaximal stimulation was not reached for setting 2. It was not possible to increase the voltage above 110 V since the maximum current output was reached. The voltage intensity at which the maximum current output was reached differed between patients
Vth Voltage threshold
Supramaximal stimulation might not be feasible for certain stimulation settings, considering the maximal stimulator output of the equipment used for measuring mTc-MEPs, due to the safety limit according to the International Electrotechnical Commission (IEC), which is 50 mJ through 1 kΩ resistance [19]. In Fig. 1B an example is shown in which supramaximal stimulation was not achieved for setting 2 since the maximum current output was reached.
The interobserver variability was calculated using Cohens Kappa. The disagreements were resolved by discussion between the two authors (SED, GD).
Due to the retrospective design of the study, in some patients, supramaximal stimulation was not achieved with one of the stimulation settings, although the maximal current output of the equipment was not yet reached. These patients were excluded from the analysis, as the possibility that supramaximal stimulation could have been achieved cannot be excluded.
2.5 mTc-MEP parameters
After evaluating if supramaximal stimulation was achieved, three mTc-MEP parameters were considered of importance; (1) elicitability of muscles, (2) amplitude, and (3) if supramaximal stimulation was achieved with ≥ 20 V below maximum output to be able to address for anesthetic events. These three parameters were compared for both settings in all patients in which supramaximal stimulation was achieved.
Thereafter, we determined the optimal settings, taking into consideration whether supramaximal stimulation was achieved ánd the three abovementioned parameters together.
2.5.1 Number of elicitable muscles
A muscle was considered elicitable if a reproducible mTc-MEP amplitude could be observed at a display gain of 50µV. The elicitability of the TA muscles left and right and AH muscles left and right was evaluated after induction but before incision in all patients in which supramaximal stimulation was achieved for both settings separately.
2.5.2 mTc-MEP amplitude
The first mTc-MEP amplitudes of the TA and AH muscles that were measured after reaching supramaximal stimulation, were collected for both settings in all patients. The amplitudes were compared between setting 1 and 2.
2.5.3 Supramaximal stimulation achieved with ≥ 20 V below maximum output
During mTc-MEP spinal cord monitoring, the stimulation voltage or current should ideally not be at the maximum of the equipment used. Should higher anesthetic drug doses, anesthetic fade, or significant blood pressure decreases cause reductions in mTc-MEP amplitudes then it is desirable to increase the stimulation voltage or current [20, 21]. Therefore, we evaluated if there was the possibility to increase the stimulation voltage with ≥ 20 V below maximum output to address for these possible anesthetic events. The values of the voltage intensities and the corresponding current outputs at which supramaximal stimulation was achieved for all four muscles were collected. Thereafter, it was evaluated if it was possible to increase the voltage intensity with ≥ 20 V without reaching the maximum current output of our equipment.
2.5.4 Setting selection
Which stimulation setting would be the optimal setting according to all abovementioned parameters (feasibility, elicitability, amplitude and if supramaximal stimulation was achieved with ≥ 20 V below maximum output) was assessed retrospectively. First it was evaluated if supramaximal stimulation was achieved in all four muscles (AH left and right, TA left and right). If with one setting supramaximal stimulation was not achieved in one or more muscles for which the maximum current output had been reached, then the other setting was regarded as the preferred setting for mTc-MEP monitoring (if supramaximal stimulation was achieved with the other setting).
Thereafter, the number of muscles (AH left and right and TA left and right) in which an mTc-MEP could be elicited were considered. If a stimulation setting provided more elicitable muscles suitable for monitoring, then it was considered the preferred setting. Thirdly, the mTc-MEP amplitudes were compared between both settings. If with one setting the amplitudes were higher in at least 3 muscles, then that setting was considered preferable.
Lastly, we determined whether an increase of ≥ 20 V above that needed for supramaximal stimulation would cause the maximal current output of the equipment to be reached. If the maximal current output was reached for one setting, and was possible with the other, then the other setting was considered the optimal setting. After consideration of all parameters, the preferred stimulation setting was chosen.
2.6 Interstimulus interval
Using a pulse duration of 0.075ms, the ISI that provided the highest amplitude for each of the AH and TA muscles was determined per patient. ISI’s of 1ms, 1.25ms, 1.5ms, 2ms, 3ms, and 4ms were used.
2.7 Anesthesia
All patients underwent total intravenous anesthesia with propofol and remifentanil or sufentanil. Nondepolarizing muscle relaxants were administered judiciously during the induction of anesthesia to facilitate endotracheal intubation while not impeding the intraoperative detection of muscle responses. No other drugs which could interfere with neuromonitoring were administered before or during the measurements. Hemodynamic and respiratory parameters remained within the accepted physiological range in all patients.
2.8 Statistical analyses
The mean and standard deviation (SD) were calculated for the baseline patient characteristics.
To determine if the amplitude of the TA and AH muscles differed significantly between both settings, the most parsimonious linear regression model was identified by testing whether setting (setting 1 vs. setting 2), side (left vs. right), and their interaction significantly improved model fit (p < 0.05) using sequential likelihood ratio tests (ANOVA function in R, R core team 2018, version 3.5.1). Model diagnostics were then performed on the most parsimonious model.
After developing the simple linear regression models, plots of the residuals were examined to determine if they were normally distributed. If they were not normally distributed, the variable was log-transformed using the natural logarithm.
The mean and SD or median and interquartile range (IQR) were calculated for the voltage intensities, current outputs and delivered charge from the last pulse of the train of pulses at which supramaximal stimulation was achieved, depending on whether the data was normally distributed or not. Differences in charge between both settings were analyzed using the Wilcoxon signed rank test.
3 Results
3.1 Patients
From the 47 consecutive patients, 9 (19.15%) were excluded. In four out of the nine excluded patients, measurements were performed with a pulse duration of 0.5ms instead of 0.3ms. One patient underwent surgery twice, therefore the data of the second operation was excluded to avoid clustering of data. In three patients, supramaximal stimulation was not achieved although the subsequent analyses showed that there had still been the possibility to increase the voltage without reaching the maximal current output. These three patients were therefore excluded from the analysis. The last patient was excluded since all four muscles (AH left/right, TA left/right) were not elicitable for both settings. Characteristics of the 38 included patients are listed in Table 2.
3.2 Feasibility of supramaximal stimulation
In total 328 mTc-MEP voltage intensity curves were produced (41 patients, two sides, two muscles, two stimulation settings). Five muscles were not elicitable. Therefore, 323 curves (98.48%) were evaluated. The scores per researcher are shown in supplementary table A. Cohen’s Kappa was 82.54% which is considered ‘almost perfect’.
Supramaximal stimulation was achieved in all patients (100.00%) when stimulation was performed with setting 1. For setting 2, supramaximal stimulation was not achieved in 23 muscles in 12 patients (31.58%) out of 38 patients. The number of patients in which mTc-MEPs were elicitable and the number of patients in which supramaximal was achieved for both setting 1 and 2 are shown per muscle in Table 3.
3.3 mTc-MEP parameters
3.3.1 Number of elicitable muscles
Of the 38 patients in whom supramaximal stimulation was achieved when stimulating with setting 1, in 37 patients (97.37%) all four muscles were elicitable. In 25 (96.415%) out of the 26 patients in which supramaximal stimulation was achieved when stimulating with setting 2, all four muscles were elicitable. In this one patient in which not all four muscles were elicitable, the AH left and TA left muscle were not elicitable for setting 2, and in the same patient only the AH left was not elicitable for setting 1.
3.3.2 mTc-MEP amplitude
For all 26 patients in whom supramaximal stimulation was achieved for both settings, the amplitude was compared using linear regression analysis. The amplitude was not statistically different between setting 1 and 2 for the AH muscles (F(1, 100) = 0.70, p = 0.40) or for the left or right side of the AH (F(1, 100) < 0.01, p = 0.97).
For the TA muscles, the amplitude was also not statistically different between setting 1 and 2 (F(1, 101) < 0.01, p = 0.91) or for the left or right side of the TA (F(1, 101) = 0.48, p = 0.49).
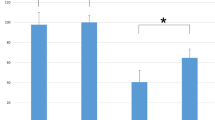
The median amplitudes and IQR per muscle and per setting can be found in Fig. 2.

Median amplitudes per muscle for setting 1 and setting 2
The x-axis denotes the different muscles used for mTc-MEP monitoring, and the y-axis denotes the median amplitude in µV. The median intraoperative mTc-MEP amplitudes for setting 1 (dark grey bars) and setting 2 (light grey bars) are presented of 25 patients for the AH left and 26 patients for the AH right, TA left and TA right. The whiskers represent the interquartile range (Q1-Q3).
AH abductor hallucis muscle, TA tibialis anterior muscle
3.3.3 Supramaximal stimulation achieved with ≥ 20 V below maximum output
In all 38 patients in whom supramaximal stimulation was achieved using stimulation setting 1, the voltage could be increased with ≥ 20 V above that required for supramaximal stimulation without reaching the maximal current output of the equipment. For setting 1, the mean voltage necessary to obtain supramaximal stimulation was 279.21 V (SD 69.06) and the median current was 393.50mA (IQR 348.25mA – 511.75mA).
In 10 (38.46%) out of the 26 patients in whom supramaximal stimulation was achieved using stimulation setting 2, the voltage could be increased with ≥ 20 V above that required for supramaximal stimulation without reaching the maximal current output. Of the 26 patients in whom supramaximal stimulation was achieved, the mean voltage was 102.12 V (SD 14.01) and the median current was 158.00mA (IQR 144.75mA – 178.00mA). The median charge of the last pulse of the train of five pulses after supramaximal stimulation was 29.5µC for setting 1 (n = 38) and 47.4µC for setting 2 (n = 26). The delivered charge was significantly lower for setting 1 (p < 0.001) as evidenced by the Wilcoxon signed rank test.
3.4 Setting selection
3.4.1 Feasibility of supramaximal stimulation
In 12 out of 38 patients (31.58%) in whom supramaximal stimulation was not achieved in all four muscles when stimulating with setting 2, the maximal current output was already reached. Since, supramaximal stimulation was achieved when stimulating with setting 1, it was considered to be the preferred stimulation setting in these 12 patients (Fig. 3).

Overview selection criteria for choosing either setting 1 or setting 2 for monitoring mTc-MEPs using supramaximal stimulation
AH abductor hallucis muscle, TA tibialis anterior muscle
3.4.2 Number of elicitable muscles
In one patient (3.85%), the AH left and the TA left muscle were not elicitable for setting 2, and in the same patient, only the AH left was not elicitable for setting 1. Therefore, for this patient, setting 1 was the preferred setting.
3.4.3 mTc-MEP amplitude
In 12 patients (48.00%) out of the remaining 25 patients, amplitudes were higher in at least 3 of the TA and AH muscles when stimulation with setting 1. In 5 patients (20.00%), the number of muscles that had the highest mTc-MEP amplitudes were equal. In 8 patients (32.00%) setting 2 was preferred considering that the mTc-MEP amplitudes were higher in at least 3 muscles than when stimulating with setting 1.
3.4.4 Supramaximal stimulation achieved with ≥ 20 V below maximum output
For setting 1 it was possible in all 38 patients (100.0%) to increase the voltage with ≥ 20 V above that required for supramaximal stimulation.
In 5 (62.50%) of the 8 patients in whom setting 2 provided higher amplitudes in at least 3 muscles when compared to setting 1, the voltage intensity could be increased with ≥ 20 V above supramaximal stimulation for setting 2. In the remaining 3 patients (37.50%) this was not possible for setting 2. In 1 (20.00%) of the 5 patients (18.52%), in whom the number of muscles that had the highest mTc-MEP amplitudes were equal, the voltage could be increased with ≥ 20 V above supramaximal stimulation for setting 2. In the remaining 4 patients (80.00%) this was not possible.
3.4.5 Optimal setting
In 32 patients (84.21%) setting 1 was preferred when compared to setting 2 considering the abovementioned parameters. In 1 patient (2.63%), the settings were equally preferable and in 5 patients (13.16%) setting 2 was preferred.
3.5 Interstimulus interval
In 9 (23.68%) out of 38 patients, not all ISI’s were used and they were therefore excluded from this analysis. In Fig. 4, the number of muscles of the optimal ISI’s can be observed. For both the AH left and right, an ISI of 1ms provided the highest amplitude in most patients (n = 9, 31.03%) for both AH left and right). For the TA left and right, an ISI of 3ms provided the highest amplitude in most patients (n = 9, 31.03%) for both TA left and right). However, no clear optimal ISI can be observed per muscle, and were often even different between muscles within a patient.

Distribution of optimal ISI when measuring mTc-MEPs using supramaximal stimulation with a pulse duration of 0.075ms (n = 29)
The x-axis denotes the different muscles used for mTc-MEP monitoring and the y-axis denotes the number of patients. The optimal ISI’s ranging from 1ms to 4ms are presented by the different colored bars for the AH left, AH right, TA left and TA right separately
AH abductor hallucis muscle, TA tibialis anterior muscle
4 Discussion
In this study we investigated the feasibility of supramaximal stimulation for different stimulation parameters, as well as the optimal stimulation parameters, consisting of pulse duration and ISI, for performing supramaximal stimulation in patients undergoing scoliosis correction surgery.
Firstly, our study showed that supramaximal stimulation is most feasible when stimulating with a relatively short pulse duration (0.075ms) when compared to a relatively long pulse duration (0.300ms). Secondly, for selection of optimal stimulation parameters for performing supramaximal stimulation, the maximum stimulator output should be considered, since ideally there has to be the possibility to increase stimulation voltage or current to be able to compensate for anesthetic events. Lastly, our study showed that when monitoring mTc-MEPs using supramaximal stimulation with a pulse duration of 0.075ms, there is broad inter-individual variation in the optimal ISI. This suggests that the optimal ISI should be determined in a per patient basis.
Our study evaluated sigmoidal curves to determine whether supramaximal stimulation was feasible for two different stimulation settings. The mTc-MEP amplitudes of the voltage intensity curves were log-transformed since changes in the amplitude are usually considered in a relative context and described by a ratio rather than by an absolute difference [12]. Two independent researchers (SED, GD) evaluated all sigmoidal curves to determine whether supramaximal stimulation was achieved. We then assessed the agreement between their evaluations and found that the Cohen’s Kappa was 82.54% which is considered ‘almost perfect’ agreement. This high Cohen’s Kappa implies that this is a good method for assessing if supramaximal stimulation was achieved or not.
It is clinically relevant to know if supramaximal stimulation was achieved in all muscles, since this has an influence on the interpretation of the warning criteria. If mTc-MEP monitoring is performed using submaximal stimulation, the potentially large inter-trial variability between mTc-MEP measurements can give false positive warnings. The difference in inter-trial variability when submaximal stimulation and supramaximal stimulation are used requires further investigation, since up till now it has only been shown in one case report [12].
Unfortunately, the equipment used in this study cannot display voltage intensity curves during mTc-MEP monitoring. Therefore, in clinical practice, supramaximal stimulation was assumed if, by visual inspection, the mTc-MEP amplitude did not increase anymore after increasing voltage intensity.
Supramaximal stimulation was feasible in all patients, when stimulating with setting 1. We found that with setting 2, supramaximal stimulation was not achieved in 12 patients (31.58%), since the maximal current output of the stimulator had been reached. Therefore, with longer pulse durations, supramaximal stimulation might not always be possible depending on the limits of the equipment used for mTc-MEP monitoring. If this is also true for constant current stimulators needs to be further explored.
For the patients in whom supramaximal stimulation was achieved for both settings, the elicitability of mTc-MEPs was similar when performing supramaximal stimulation. There was only one patient in whom fewer muscles were elicitable with setting 2 when compared to setting 1.
There were more patients that had higher mTc-MEP amplitudes in at least three of the four recorded muscles when stimulating with setting 1. However, the amplitudes did not differ significantly between the two settings.
When stimulation with setting 2, in most patients, supramaximal stimulation was only achieved with a current at or close to the maximal current output, as can be deduced from the high median current of 162.50mA (IQR 145.00mA – 178.75mA). During surgery, and especially during long operations such as scoliosis correction, it should ideally be possible to increase the voltage intensity to counteract the potential influence of the effects of higher anesthetic drug doses, anesthetic fade, and significant blood pressure decreases on mTc-MEP amplitudes [20,21,22]. Although, the ≥ 20 V cut-off value chosen in this study is arbitrary, in our experience, it was sufficient to counteract for anesthetic events.
Another advantage of stimulating with setting 1 was that the median charge from the last pulse of the train of pulses was significantly lower (p < 0.001) when compared to setting 2. One could argue that stimulating with higher voltages and a relatively short pulse duration, compared to stimulating with lower voltages and a relatively long pulse duration, may result in similar amounts of delivered charge. Theoretically, shorter ISIs also result in higher amounts of delivered charge per train of pulses. Our results suggest that setting 1 can achieve supramaximal stimulation of mTc-MEPs more efficiently than setting 2. Unfortunately, the ISIs were not included in the calculations since the precise delivered charge per train was not available from the equipment used in this study.
As mentioned above there was significant inter-individual variability in optimal ISI, and also within patient variability per muscle. Optimal ISI should therefore be determined per patient.
Published data concerning the optimal ISI for mTc-MEP monitoring are conflicting. In general, ISIs between 2 and 5ms are recommended [7, 23,24,25,26,27]. Using methodology similarly to that of our study, Hal et al. also found a bimodal distribution with a first peak at around 1ms, and the second peak at around 3ms for the tibialis anterior muscles. However, it could be argued that the short ISI’s of 1ms might result in stimulation within the absolute refractory period (ARP). The relationship between the ARP and the optimal ISI for providing the highest amplitude is not known. Novak et al. reported that the ARP is shorter (mean 0.82ms) with supramaximal stimulation than with submaximal stimulation (mean 1.47ms) [28]. This might explain why shorter ISI’s than 2ms can be the optimal ISI for supramaximal stimulation, which is contradictory to previous literature [7, 23,24,25,26,27].
The difference between the optimal ISI’s of the TA and AH muscles might be explained by differences of the motor unit properties of the different muscles [28]. Further research is necessary to better understand how mTc-MEP stimulation parameters can be optimized per muscle and how the different motor unit properties of different muscles play a role in mTc-MEP stimulation. Taken together, our data and that of others suggests that optimal ISI will depend on whether supramaximal stimulation or submaximal stimulation is used to elicit mTc-MEPs, and furthermore there is inter-patient variability and within-patient (per muscle) variability in optimal ISI for obtaining the highest amplitude. An individualized optimization of the ISI is therefore still recommended [14].
In our clinical practice, we choose to first obtain supramaximal stimulation, and thereafter optimize the ISI (1ms, 1.25ms, 1.5ms, 2.0ms, 3.0ms and 4.0ms) and choose the ISI that provided the highest mTc-MEP amplitudes in the muscles of most interest.
Although this study is one of the most extensive studies to determine the feasibility of supramaximal stimulation for different stimulation parameters, and the optimal stimulation parameters, consisting of pulse duration and ISI, it has limitations.
Firstly, although we investigated two different stimulation settings, there are still multiple different settings of interest that have to be investigated to get more insight into the optimal setting parameters for supramaximal stimulation. However, due to time constraints in the operating theater and patient safety concerns, at the time of data collection we routinely only used two sets of settings. By understanding more about the range of the different stimulation parameters for optimization of supramaximal stimulation, a more targeted set-up for the baseline measurements can be achieved in the limited time available in the operating room.
Another limitation of supramaximal stimulation might be that it may not be suitable for all types of surgery, since with higher voltage or current stimulation, there will be more patient movement. Supramaximal stimulation might, for example, not be feasible for neurosurgical patients in whom the head is secured in a Mayfield skull clamp.
5 Conclusion
mTc-MEP monitoring using supramaximal stimulation is most feasible when stimulating with a relatively short pulse duration (0.075ms) since with a relatively longer pulse duration (0.300ms) the maximum stimulator output can be reached before supramaximal stimulation is achieved or there is no possibility to increase the voltage intensity to counteract for anesthetic events. Therefore, we recommend using setting 1 when monitoring mTc-MEPs with supramaximal stimulation, after which an individualized ISI optimization can be performed. Moreover, when using supramaximal stimulation, short ISI’s (i.e. 1ms or 1.5ms) can be the optimal ISI for obtaining the highest mTc-MEP amplitude.
Abbreviations
- mTc-MEP:
-
muscle evoked transcranial electrical stimulation motor evoked potential
- ISI:
-
interstimulus interval
- AH:
-
abductor hallucis muscle
- TA:
-
tibialis anterior muscle
- IONM:
-
intraoperative neurophysiological monitoring
- SSEP:
-
somatosensory evoked potential
- IQR:
-
interquartile range
- IEC:
-
International Electrotechnical Commission
References
Fehlings MG, Brodke DS, Norvell DC, Dettori JR. The evidence for intraoperative neurophysiological monitoring in spine surgery: does it make a difference? Spine (Phila Pa 1976) [Internet]. 2010 [cited 2019 Aug 28];35:S37-46. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20407350
MacDonald DB, Skinner S, Shils J, Yingling C. Intraoperative motor evoked potential monitoring – A position statement by the American Society of Neurophysiological Monitoring. Clinical Neurophysiology [Internet]. 2013 [cited 2019 Apr 25];124:2291–316. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1388245713010006
MacDonald DB, Dong C, Quatrale R, Sala F, Skinner S, Soto F, et al. Recommendations of the International Society of Intraoperative Neurophysiology for intraoperative somatosensory evoked potentials. Clin Neurophysiol Int Federation Clin Neurophysiol. 2019;130:161–79.
MacDonald DB, Skinner S, Shils J, Yingling C. Intraoperative motor evoked potential monitoring - A position statement by the American Society of Neurophysiological Monitoring. Clinical Neurophysiology [Internet]. International Federation of Clinical Neurophysiology; 2013;124:2291–316. Available from: https://doi.org/10.1016/j.clinph.2013.07.025
MacDonald DB, Janusz M. An approach to intraoperative neurophysiologic monitoring of thoracoabdominal aneurysm surgery. J Clin Neurophysiol Lippincott Williams Wilkins. 2002;19:43–54.
Calancie B. Intraoperative neuromonitoring and alarm criteria for judging MEP responses to transcranial electric stimulation: the threshold-level method. J Clin Neurophysiol. 2017;34:12–21.
Calancie B, Harris W, Broton JG, Alexeeva N, Green BA. “Threshold-level” multipulse transcranial electrical stimulation of motor cortex for intraoperative monitoring of spinal motor tracts: description of method and comparison to somatosensory evoked potential monitoring. J Neurosurg American Association of Neurological Surgeons. 1998;88:457–70.
Quiñones-Hinojosa A, Lyon R, Zada G, Lamborn KR, Gupta N, Parsa AT, et al. Changes in transcranial motor evoked potentials during intramedullary spinal cord tumor resection correlate with postoperative motor function. Neurosurgery. 2005;56:982–92.
Langeloo DD, Lelivelt A, Louis Journée H, Slappendel R, de Kleuver M. Transcranial Electrical Motor-Evoked potential monitoring during surgery for spinal deformity. Spine (Phila Pa 1976). 2003;28:1043–50.
Langeloo D-D, Journée H-L, de Kleuver M, Grotenhuis JA. Criteria for transcranial electrical motor evoked potential monitoring during spinal deformity surgery. Neurophysiologie Clinique/Clinical Neurophysiology. 2007;37:431–9.
MacDonald DB. Overview on criteria for MEP monitoring. Journal of Clinical Neurophysiology. 2017. p.4–11.
Journée HL, Berends HI, Kruyt MC. The percentage of amplitude decrease warning criteria for Transcranial MEP monitoring. J Clin Neurophysiol. 2017;34:22–31.
Hausmann ON, Min K, Boos N, Ruetsch YA, Erni T, Curt A. Transcranial electrical stimulation: significance of fast versus slow charge delivery for intra-operative monitoring [Internet]. Available from: www.elsevier.com/locate/clinph
van Hal C, Hoebink E, Polak HE, Racz I, de Kleuver M, Journee HL. Optimum interpulse interval for transcranial electrical train stimulation to elicit motor evoked potentials of maximal amplitude in both upper and lower extremity target muscles. Clin Neurophysiol. 2013;124:2054–9.
MacDonald DB, Skinner S, Shils J, Yingling C, American Society of Neurophysiological Monitoring. Intraoperative motor evoked potential monitoring – A position statement by the American Society of Neurophysiological Monitoring. Clinical Neurophysiology [Internet]. 2013 [cited 2018 May 13];124:2291–316. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24055297
Yoshida G, Ando M, Imagama S, Kawabata S, Yamada K, Kanchiku T et al. Alert Timing and Corresponding Intervention with Intraoperative Spinal Cord Monitoring for High-Risk Spinal Surgery. Spine (Phila Pa 1976) [Internet]. Lippincott Williams and Wilkins; 2019 [cited 2022 Jun 21];44:E470–9. Available from: https://journals.lww.com/spinejournal/Fulltext/2019/04150/Alert_Timing_and_Corresponding_Intervention_With.8.aspx
Lo YL, Dan YF, Tan YE, Teo A, Tan SB, Yue WM et al. Clinical and physiological effects of transcranial electrical stimulation position on motor evoked potentials in scoliosis surgery. 2010.
Ukegawa D, Kawabata S, Sakaki K, Ishii S, Tomizawa S, Inose H et al. Efficacy of biphasic transcranial electric stimulation in intraoperative motor evoked potential monitoring for cervical compression myelopathy. Spine (Phila Pa 1976) [Internet]. Spine (Phila Pa 1976); 2014 [cited 2022 Nov 25];39. Available from: https://pubmed.ncbi.nlm.nih.gov/24153163/
International Electrotechnical Commission. Medical Electrical Equipmant - Part 2–40: Particular requirements for the safety of electromyographs and evoked response equipment. 1st ed. Geneva: International Electrotechnical 60601-2-40., Commission; 1998. I.
Sahinovic MM, Gadella MC, Shils J, Dulfer SE, Drost G. Anesthesia and intraoperative neurophysiological spinal cord monitoring. Curr Opin Anaesthesiol [Internet]. Curr Opin Anaesthesiol; 2021 [cited 2021 Sep 30];34:590–6. Available from: https://pubmed.ncbi.nlm.nih.gov/34435602/
Dulfer SE, Sahinovic MM, Lange F, Wapstra FH, Postmus D, Potgieser ARE et al. The influence of depth of anesthesia and blood pressure on muscle recorded motor evoked potentials in spinal surgery. A prospective observational study protocol. J Clin Monit Comput. Springer Netherlands; 2021
Ugawa R, Takigawa T, Shimomiya H, Ohnishi T, Kurokawa Y, Oda Y, et al. An evaluation of anesthetic fade in motor evoked potential monitoring in spinal deformity surgeries. J Orthop Surg Res. 2018;13:227.
Bartley K, Woodforth IJ, Stephen JP, Burke D. Corticospinal volleys and compound muscle action potentials produced by repetitive transcranial stimulation during spinal surgery. Clin Neurophysiol [Internet]. Clin Neurophysiol; 2002 [cited 2022 May 16];113:78–90. Available from: https://pubmed.ncbi.nlm.nih.gov/11801428/
Deletis V, Isgum V, Amassian VE. Neurophysiological mechanisms underlying motor evoked potentials in anesthetized humans. Part 1. Recovery time of corticospinal tract direct waves elicited by pairs of transcranial electrical stimuli. Clin Neurophysiol. 2001;112:438–44.
Pelosi L, Stevenson M, Hobbs GJ, Jardine A, Webb JK. Intraoperative motor evoked potentials to transcranial electrical stimulation during two anaesthetic regimens. Clin Neurophysiol. 2001;112:1076–87. Department of Clinical Neurophysiology, University Hospital, Queen’s Medical Centre, NG7 2UH, Nottingham, UK.
Taniguchi M, Cedzich C, Taniguchi M, Cedzich C, Schramm J. Modification of cortical stimulation for motor evoked potentials under general anesthesia: Technical description. Neurosurgery [Internet]. Neurosurgery; 1993 [cited 2021 May 30];32:219–26. Available from: https://pubmed.ncbi.nlm.nih.gov/8437660/
Pechstein U, Cedzich C, Nadstawek J, Schramm J. Transcranial high-frequency repetitive electrical stimulation for recording myogenic motor evoked potentials with the patient under general anesthesia. Neurosurgery [Internet]. Neurosurgery; 1996 [cited 2021 Sep 1];39:335–44. Available from: https://pubmed.ncbi.nlm.nih.gov/8832671/
Novak K, de Camargo AB, Neuwirth M, Kothbauer K, Amassian VE, Deletis V. The refractory period of fast conducting corticospinal tract axons in man and its implications for intraoperative monitoring of motor evoked potentials. Clin Neurophysiol. 2004;115:1931–41.
Acknowledgements
The authors would like to thank technicians Ms. C. Scholtens and Mr. D. W. ten Cate, for their help with the data collection of this study.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
SED, GD, and FL designed and prepared the first draft of the study. All authors critically reviewed the manuscript, substantially revised it, and approved the final version of this manuscript.
Corresponding author
Ethics declarations
Conflicts of interest/Competing interests
ARA reports receipt of unrestricted research funding and/or reimbursement for consultancy for The Medicines Company, Janssen Pharma, Carefusion/BD, Orion Pharma, Ever Pharma, Terumo, PAION and Philips (all for work unrelated to the current study; all payments to institution).
The other authors report no conflicts of interest.
Ethics approval and consent to participate
This study will be conducted in accordance with the Declaration of Helsinki and in compliance with the Medical Research Involving Human Subjects Act. Since the data analyzed in this study were collected during routine clinical care, the ethical committee of University Medical Center Groningen (UMCG) waived the requirement for full ethical committee review in accordance with the terms of the Dutch Act on Medical Research on Human Subjects (Wet Medisch-Wetenschappelijk Onderzoek, or ‘WMO’).
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Dulfer, S.E., Lange, F., Sahinovic, M.M. et al. Feasibility and optimal choice of stimulation parameters for supramaximal stimulation of motor evoked potentials. J Clin Monit Comput 37, 783–793 (2023). https://doi.org/10.1007/s10877-022-00972-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10877-022-00972-5