
Abstract
Purpose
This phase 3, multicenter, open-label, randomized, two-period, crossover bioequivalence trial evaluated the safety, tolerability, and pharmacokinetics of intravenous immunoglobulins (IVIGs) Gammaplex 5% and Gammaplex 10% in 33 adults and 15 children with primary immunodeficiency diseases (PIDs).
Methods
Eligible adults received five Gammaplex 5% infusions followed by five Gammaplex 10% infusions, or vice versa, stratified by a 21- or 28-day dosing regimen. Pediatric subjects received five Gammaplex 10% infusions only.
Results
The primary objective, to demonstrate the bioequivalence of Gammaplex 10% and Gammaplex 5% at the 28-day dosing interval, was met based on the Gammaplex 10%/Gammaplex 5% ratio of area under the concentration versus time curve (AUC0–28) values. Throughout the study, total immunoglobulin G trough levels were well maintained, with total values generally ≥600 mg/dL (minimum level for study inclusion). At the dosing schedules and infusion rates used in this study, safety and tolerability were comparable and acceptable in adult and pediatric PID subjects treated with Gammaplex 10% and 5%.
Conclusions
In this study, the first direct comparison of 5% IVIG and 10% IVIG products in PID subjects, the pharmacokinetic analysis demonstrated bioequivalence of Gammaplex 10% and Gammaplex 5% at the 28-day dosing interval. The Gammaplex 10% formulation was safe and well tolerated in pediatric and adult PID subjects. Based on the results from this bridging study in PID subjects, Gammaplex 10% could be expected to have a therapeutic effect similar to the licensed Gammaplex 5%, which has demonstrated efficacy and tolerability in patients with PID and idiopathic thrombocytopenic purpura.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Primary immunodeficiency diseases (PID) comprise a diverse range of disorders, most of which are characterized by defects in antibody production and increased susceptibility to infection [1]. Replacement therapy with immunoglobulin G (IgG) purified from human plasma has been the standard of care since the early 1950s. By the 1960s, IgG products were administered intramuscularly, but efficacy was limited by the relatively small quantities that could be administered by that route due to discomfort and painful local side effects [2, 3]. In the 1980s, intravenous immunoglobulin (IVIG) became available in the USA and became the most common treatment for PID patients with impaired humoral immunity [4,5,6]. Currently, IVIG is available at concentrations of 3%, 5%, 6%, 9%, 10%, and 12%, with more products available at 10% than at any other concentration [7, 8].
Gammaplex® 5% is a highly purified human IgG liquid product intended for intravenous (IV) administration (Bio Products Laboratory Ltd., Elstree, UK) and approved for use in the USA and the UK for PID and immune thrombocytopenic purpura (ITP) [9, 10]; Gammaplex 5% is also licensed in Brazil, Brunei, Israel, Lebanon, and Malta. Previous studies of Gammaplex 5% demonstrated efficacy in preventing serious acute bacterial infections (SABIs) and demonstrated tolerability both in patients with PID [11, 12] and those with ITP [13]. Like Gammaplex 5% (Gammaplex [5%] 5 g in 100 mL), Gammaplex 10% (Gammaplex [10%] 10 g in 100 mL) is a ready-prepared solution for IV administration containing the active ingredient human normal IgG. Both products are manufactured using the same process, but Gammaplex 10% is more concentrated, with an IgG concentration of 100 g/L, and is stabilized with glycine, whereas Gammaplex 5% is stabilized with sorbitol. This study evaluated the bioequivalence of the currently licensed formulation (Gammaplex 5%) and the new formulation (Gammaplex 10%), as well as pharmacokinetics (PK), safety, and tolerability of Gammaplex 10%, in adult and pediatric subjects with PID. This article is the first report of a clinical study of Gammaplex 10% and of the first direct comparison between a 5% and a 10% IVIG product in PID patients.
Methods
Study Design
This bridging study was a phase 3, multicenter, open-label, randomized, two-period, crossover bioequivalence trial to evaluate the PK, safety, and tolerability of Gammaplex 10% in PID (ClinicalTrials.gov, NCT01963143; EudraCT, 2013-002290-21) versus the PK, safety, and tolerability of Gammaplex 5% [12]. Approximately 1 to 3 days before the first planned infusion (visit 1), eligible adult subjects were randomized (1:1) to the following treatment sequences and stratified by dosing regimen (21 or 28 days): either five infusions of Gammaplex 5% followed by five infusions of Gammaplex 10% (sequence 1), or five infusions of Gammaplex 10% followed by five infusions of Gammaplex 5% (sequence 2). Pediatric subjects received five infusions of Gammaplex 10% only. The enrollment of the pediatric cohort was delayed until acceptable safety and tolerability had been demonstrated in ≥5 adult subjects. Samples for PK profiling were collected at specified times for the final infusion of each treatment (visits 5 and 10 for adult subjects; visit 5 for pediatric subjects).
Gammaplex 5% and Gammaplex 10% were dosed at 300–800 mg/kg per infusion every 21 or 28 days. The selected dose was the same as the dose of IVIG administered during the 3 months prior to study entry. Subjects were to be adequately hydrated prior to infusion, but a pre-infusion hydration step was not required for either product. To provide an initial equivalent protein dose, the initial infusion rates were 0.01 and 0.005 mL/kg/min for Gammaplex 5% and Gammaplex 10%, respectively, for the first 15 min. Subjects who tolerated the first infusion with minimal adverse reactions could begin subsequent infusions at 0.02 mL/kg/min (Gammaplex 5%) and 0.01 mL/kg/min (Gammaplex 10%) (Table 1). For each infusion, the rate was increased incrementally at 15-min intervals, reaching a maximum infusion rate for both Gammaplex 5% and Gammaplex 10% of 0.08 mL/kg/min, depending on the subjects’ ability to tolerate slower infusions. Additional infusions were permitted to ensure that subjects received five infusions of Gammaplex 10% or Gammaplex 5% at the same dose and were on stable treatment prior to the PK sampling. Infusion visits were scheduled every 21 or 28 days, depending on the subject’s cycle of infusions during prior IVIG treatment. Individual infusions could be administered ±3 days of the planned schedule. Subjects returned to the clinic 6 to 7 days after the first infusion of either treatment to assess safety (after visit 1 for pediatric subjects; after visits 1 and 6 for adult subjects). Subjects returned for an end-of-study visit 28 days after the final study infusion. The total study duration (screening to end-of-study visit) was 38–48 weeks for any given adult subject and 23–28 weeks for any given pediatric subject, depending on the subject’s frequency of infusion.
Compliance with Ethical Standards
The protocol for this study was approved by an institutional review board or independent ethics committee for each of 16 study centers in the USA (13 centers), the UK (2 centers), and Hungary (1 center). This study was conducted in accordance with the ICH Harmonised Tripartite Guidelines for Good Clinical Practice [14], and each study participant (or their parent/guardian, if applicable) provided written informed consent to participate in the study. Assents were obtained according to local regulations.
Subject Selection
Study candidates met the following eligibility criteria: aged 16–55 years inclusive (adult cohort) or aged 2–15 years inclusive and body weight ≥10 kg (pediatric cohort); diagnosis of PID with hypogammaglobulinemia; currently receiving a licensed (or investigational stage 3 or 3b) IVIG at a dose that had not changed by ±50% of the mean dose for ≥3 months before study entry and was 300–800 mg/kg per infusion, with an infusion interval of every 21 or 28 days; and trough IgG level of ≥6 g/L (600 mg/dL), with ≥1 documented trough level available from the 3 months before screening.
Excluded subjects were those with a history of anaphylactic reaction to blood or blood-derived products; abnormal liver and/or renal function; selective immunoglobulin A (IgA) deficiency, history of reaction to products containing IgA, or history of antibodies to IgA; cellular or innate impaired immunity; evidence of an active infection at the time of enrollment; currently receiving or had received any investigational agent other than an IVIG product within the prior 3 months; pregnant or nursing; positive HIV-1 and HIV-2, hepatitis C virus, or hepatitis B surface antigen testing; history of deep vein thrombosis or thrombotic complications of IVIG therapy; or intolerance to any component of Gammaplex. The use of local anesthetics, antipyretics, antihistamines, analgesics, and antiemetics prior to infusion was allowed, but routine long-term use of corticosteroids (apart from oral and parenteral steroids if average daily dose was <0.15 mg of prednisone equivalent/kg/day) was not permitted.
Outcomes
As this was a bridging study to evaluate the bioequivalence and compare the safety and tolerability of the two formulations of Gammaplex, no formal efficacy analyses were performed. The primary analysis was the bioequivalence assessment of Gammaplex 10% and Gammaplex 5% in adult subjects at their final infusion (PK infusion) on a 28-day treatment schedule. The primary outcome was area under the concentration versus time curve from time=0 to time=28 days (AUC0–28; calculated by the linear trapezoidal rule). Secondary outcomes included a bioequivalence assessment of Gammaplex 10% and Gammaplex 5% using area under the concentration versus time curve from time=0 to time=21 days (AUC0–21; calculated by the linear trapezoidal rule) determined in adult subjects on a 21-day treatment schedule at the final infusion in each treatment period (PK infusion).
Additional PK parameters measured during and after the PK infusion included maximum observed concentration (C max), time at which C max was apparent (t max), systemic clearance (CL, calculated as dose/AUC0–τ [where τ is the dosing interval]), apparent volume of distribution at steady state (V ss, calculated as CL·MRT; MRT, the mean residence time at steady state, was calculated as AUMC0–τ + τ·AUCτ–∞/AUC0–τ − T/2 [where AUMC is the area under the first moment curve, T is the infusion duration, and τ is the dosing interval]), apparent terminal half-life (t 1/2), and trough IgG levels. Trough levels of total IgG were measured before every infusion and at end of study, and trough levels by IgG subclass and of IgG antibodies to specific antigens (Haemophilus influenzae type b and Streptococcus pneumoniae) were measured before the first infusion of each Gammaplex formulation and at end of study. Baseline IgG levels for each formulation were defined as those prior to the first study dose of Gammaplex. At the end of each treatment period, IgG levels were assessed within 10 min before the end of the infusion and at the following times after the end of the infusion: 60 min; 3, 6, 24, and 48 h; and 4, 7, 14, and 21 days (and at 28 days for subjects on the 28-day regimen).
Safety assessments included the number and percentage of adverse events (AEs; defined as those events with onset between the first infusion date and 28 days after the last infusion); number and percentage of product-related AEs (defined as AEs in which the relationship to the study drug was recorded as “possible,” “probable,” or “very likely/certain,” or in which information regarding the relationship to the study drug was unavailable); number and percentage of adverse reactions (ARs; defined as AEs [irrespective of causality] that occurred during the infusion or within 72 h after completion of the infusion, any product-related AEs, or any AEs with unknown causality); vital signs; clinical laboratory tests (including tests for hemolysis); transmission of viruses; and physical examination.
Safety variables were determined for Gammaplex 10% in all adult and pediatric subjects and for Gammaplex 5% in all adult subjects. AEs were coded using the Medical Dictionary for Regulatory Activities (version 17.0).
Statistical Analysis
PK analyses (AUC0–τ , C max, t max, CL, V ss, t 1/2, and trough IgG levels for PK infusions) were performed on the PK population, defined as all subjects who received regular doses of Gammaplex (i.e., assumed to be at steady state) and from whom an appropriate PK profile was obtained over the 21- or 28-day period. Gammaplex PK was based on absolute (unadjusted) and baseline-adjusted (i.e., adjusted for pre-dose concentrations) values and were calculated using a noncompartmental method. All trough IgG levels were analyzed unadjusted. Actual sample times, rather than nominal times, were used to calculate PK parameters. The AUC0–τ on which bioequivalence was based was log-transformed prior to analysis. Adult subjects on the 28-day regimens were analyzed using an analysis of variance model, including fixed effect terms for sequence, subject within sequence, period, and formulation (Gammaplex 10% or Gammaplex 5%). The 90% confidence interval (CI) for the difference between formulations was obtained and back transformed to obtain a CI for the ratio between formulations on the original scale. To show bioequivalence of the two formulations, this back-transformed 90% CI needed to lie between 0.8 and 1.25. Safety parameters (including AEs and adverse reactions) and trough levels of total IgG, IgG subclasses, and IgG antibodies to specific antigens were summarized using the intent-to-treat population, which was defined as all subjects who received ≥1 infusion of Gammaplex 10% or Gammaplex 5%.
Results
Subject Disposition
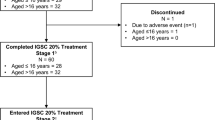
A total of 48 subjects were enrolled in this study; 33 adults were randomized to sequence 1 or sequence 2 over 21-day (n = 14) or 28-day (n = 19) infusion schedules, and 15 nonrandomized pediatric subjects were enrolled to receive Gammaplex 10% over 21-day (n = 7) or 28-day (n = 8) infusion schedules (Fig. 1). Thirty-two of 33 adult subjects completed the study; one adult withdrew during the first infusion due to inconvenience of study visits. Of the 32 adult subjects who completed the study, 30 were eligible for the PK analysis (n = 14 and n = 15 for the 21- and 28-day infusion schedules, respectively). Fourteen of 15 pediatric subjects completed the study; one child was withdrawn from the study after the fourth infusion at the investigator’s discretion due to consistently low IgG trough levels despite a dose increase. Of the 14 pediatric subjects who completed the study, 13 were eligible for the PK analysis (n = 7 and n = 6 for the 21- and 28-day infusion schedules, respectively).

Subject disposition. a Sequence 1 was five infusions of Gammaplex 5% followed by five infusions of Gammaplex 10%. b Sequence 2 was five infusions of Gammaplex 10% followed by five infusions of Gammaplex 5%. c Pediatric subjects received five infusions of Gammaplex 10% only. d One subject withdrew consent. e One subject was withdrawn at investigator discretion
Baseline Characteristics
Upon study entry, the median age of the adult subjects was 42.0 years (range, 17–55 years); the median age of the pediatric subjects was 8.0 years (range, 3–15 years) (Table 2). Most enrolled subjects had a diagnosis of common variable immunodeficiency (30 of 33 adults [91%] and 8 of 15 pediatric subjects [53%]). The remaining subjects had diagnoses of X-linked or autosomal forms of agammaglobulinemia (3 of 33 adults [9%] and 5 of 15 pediatric subjects [33%]) and hypogammaglobulinemia (2 of 15 pediatric subjects [13%]). Both subjects with hypogammaglobulinemia were aged ≥8 years and were therefore too old to have transient hypogammaglobulinemia of infancy. In accordance with study eligibility criteria, all subjects had received IGIV therapy prior to enrollment. One adult had also been treated with a subcutaneous immunoglobulin product prior to receiving IGIV treatment and subsequent study enrollment.
Primary Outcome
For adults treated with Gammaplex 10%, the geometric mean AUC0–τ for the 28-day regimen was 34,900 mg·day/dL for absolute (unadjusted) values and 7830 mg·day/dL for baseline-adjusted (adjusted for pre-dose concentration) values (Supplemental Table S1). For adults treated with Gammaplex 5%, the geometric mean AUC0–τ for the 28-day regimen was 34,800 mg·day/dL for absolute values and 7230 mg·day/dL for baseline-adjusted values. Mean absolute serum IgG concentrations at steady state following repeated IV doses of Gammaplex 10% and Gammaplex 5% (28-day regimen) were almost superimposable (Fig. 2a, b). Based on the ratios (Gammaplex 10%/Gammaplex 5%) of least squares (LS) geometric means for AUC0–τ for the 28-day regimen (ratio for absolute IgG concentrations 1.01 [90% CI 0.98–1.03]; ratio for baseline-adjusted IgG concentrations 1.07 [90% CI 0.93–1.23]), both 90% CIs were within the prescribed bioequivalence range of 0.8–1.25. Thus, based on these results, the two products were bioequivalent.

Mean absolute serum concentrations of immunoglobulin G (IgG) following intravenous infusion of Gammaplex 10% to pediatric subjects, Gammaplex 10% to adults, and Gammaplex 5% to adults: 28-day regimen linear (a) and semi-logarithmic (b) scales; 21-day regimen linear (c) and semi-logarithmic (d) scales. Pre-dose samples were taken up 30 min prior to infusion; samples at time zero were taken within 10 min prior to the end of infusion
Secondary Outcomes
Adult Subjects
For the 21-day dosing interval, geometric means of the AUC0–τ of IgG in adults following repeated IV infusions of Gammaplex 10% (30,000 mg·day/dL) and Gammaplex 5% (30,400 mg·day/dL) were bioequivalent for absolute serum IgG concentrations (ratio of LS geometric means 0.99 [90% CI 0.95–1.02]). Results for baseline-adjusted IgG concentrations were similar (AUC0–τ : Gammaplex 10%, 6980 mg·day/dL; Gammaplex 5%, 6380 mg·day/dL); however, the upper 90% confidence limit for the ratio of geometric mean (1.10 [90% CI 0.96–1.26]) was just outside of the upper prescribed bound of 1.25. Thus, the secondary objective, to demonstrate bioequivalence between the 21-day dosing regimens of Gammaplex 10% and 5%, was met using absolute serum IgG concentrations but just missed the defined bioequivalence bounds for baseline-adjusted IgG concentrations.
Similar to that observed for the 28-day regimen, the mean absolute serum concentrations of IgG among adults at steady state for the 21-day regimen following repeated IV doses of Gammaplex 10% and Gammaplex 5% were almost superimposable (Fig. 2c, d). For each dosing regimen, mean absolute trough IgG concentrations at the end of dosing following repeated (≥5) IV infusions of Gammaplex 10% (28-day regimen, 918 mg/dL; 21-day regimen, 1103 mg/dL) and Gammaplex 5% (28-day regimen, 945 mg/dL; 21-day regimen, 1120 mg/dL) were also equivalent based on ratio of geometric mean data (28-day regimen, 0.98 [90% CI 0.94–1.02]; 21-day regimen, 0.95 [90% CI 0.92–0.99]). Adults treated with Gammaplex 10% had mean total IgG trough levels of 879 mg/dL (28-day regimen) and 1074 mg/dL (21-day regimen) at baseline, with mean changes from baseline to after the last Gammaplex 10% infusion of 58 and 29 mg/dL, respectively (Fig. 3). Adults treated with Gammaplex 5% had mean total IgG trough levels of 891 mg/dL (28-day regimen) and 1074 mg/dL (21-day regimen) at baseline, with mean changes from baseline to after the last Gammaplex 5% infusion of 71 and 46 mg/dL, respectively.

Mean trough (pre-infusion) serum concentrations of immunoglobulin G (IgG) following intravenous infusion of Gammaplex 10% in adults (a), Gammaplex 5% in adults (b), and Gammaplex 10% in pediatric (c) subjects. Threshold at 600 mg/dL (minimum trough serum IgG level for inclusion in study) is indicated by the gray line. SD standard deviation
Throughout the study, total IgG trough levels in adult subjects were well maintained, with total IgG trough levels consistently ≥600 mg/dL (the minimum trough serum IgG level for inclusion in the study) (Fig. 3a, b). Trough levels of IgG antibodies to specific antigens (H. influenzae type b and S. pneumoniae serotypes) were comparable after treatment with Gammaplex 10% or Gammaplex 5%, and no clinically relevant changes from baseline were observed (Supplemental Table S2).
Similar results were observed for trough levels of IgG subclasses 1, 2, and 3, whereas trough levels of IgG subclass 4 were slightly lower after the last Gammaplex infusion (mean [standard deviation, SD]: Gammaplex 10%, 8.3 [5.8] mg/dL; Gammaplex 5%, 8.6 [7.8] mg/dL) compared with baseline (mean [SD]: Gammaplex 10%, 13.0 [7.7] mg/dL; Gammaplex 5%, 13.0 [7.6] mg/dL) (Supplemental Table S3). All other PK parameters were similar between Gammaplex 10% and Gammaplex 5% (Supplemental Table S1).
Pediatric Subjects
For the 28-day dosing interval, the geometric mean AUC0–τ for pediatric subjects treated with Gammaplex 10% was 32,600 mg·day/dL for absolute values and 7280 mg·day/dL for baseline-adjusted values (Supplemental Table S1). For the 21-day dosing interval, the geometric mean AUC0–τ was 27,100 mg·day/dL for absolute values and 6000 mg·day/dL for baseline-adjusted values.
Mean absolute serum concentrations of IgG among pediatric subjects at steady state following repeated IV doses of Gammaplex 10% were similar to those of adults receiving Gammaplex 10% and Gammaplex 5% for the 28-day (Fig. 2a, b) and 21-day (Fig. 2c, d) dosing regimens.
Each of the 14 pediatric subjects who completed the study maintained total IgG trough levels of ≥600 mg/dL throughout the study, and total IgG trough levels were well maintained throughout (Fig. 3c). For the pediatric subject who did not complete the study and was withdrawn by the investigator, the total IgG trough level prior to initiating Gammaplex 10% was 507 mg/dL and thereafter ranged from 343 to 470 mg/dL, despite dose increases (infusion 1, 488 mg/kg; infusion 2, 494 mg/kg; infusion 3, 651 mg/kg; infusion 4, 659 mg/kg). Twelve days after infusion 4, and without having received any other IVIG, the total IgG trough level in this subject was 846 mg/dL.
Among pediatric subjects, mean trough levels of total IgG at baseline and after the last infusion were 875 and 908 mg/dL, respectively (Fig. 3c). No clinically relevant changes from baseline were observed in trough levels of IgG subclasses (Supplemental Table S3) or IgG antibodies to H. influenzae and S. pneumoniae antigens (Supplemental Table S2) in pediatric subjects after treatment with Gammaplex 10%. Additional PK parameters of IgG following treatment with Gammaplex 10% in pediatric subjects are shown in Supplemental Table S1.
Safety
Overall, the mean (SD) total duration of exposure to Gammaplex (10% and/or 5%) was 252.2 (56.79) days among adults and 138.5 (30.26) days among pediatric subjects, with median (range) durations of 281.0 (1–316) and 139.0 (97–196) days, respectively. With the crossover study design, the mean (SD) durations of exposure among adults were similar for Gammaplex 10% (132.6 [22.58] days) and Gammaplex 5% (124.6 [27.59] days), with median (range) durations of exposure of 141.0 (97–181) and 140.0 (1–150) days, respectively. For adults, the mean (SD) total dose of Gammaplex 10% was 202.21 (77.732) g, with a mean (SD) dose per infusion of 494.9 (135.95) mg/kg; the mean (SD) total dose of Gammaplex 5% was 190.01 (67.094) g, with a mean (SD) dose per infusion of 485.6 (145.68) mg/kg. Among pediatric subjects, the mean (SD) total dose of Gammaplex 10% was 111.91 (52.988) g, with a mean (SD) dose per infusion of 535.1 (121.25) mg/kg. Among adults, the mean (SD) durations of infusion were 111.4 (24.98) min for Gammaplex 10% and 168.7 (47.02) min for Gammaplex 5% (Fig. 4); among pediatric subjects, the mean (SD) duration of infusion was 139.3 (42.89) min for Gammaplex 10%. Similar proportions of adults on each product received pre-infusion medications (Gammaplex 5%: n = 3, 9.1%; Gammaplex 10%: n = 3, 9.4%), including cetirizine, diphenhydramine, and paracetamol; six pediatric subjects (40%) received pre-infusion medications, including diphenhydramine, ibuprofen, loratadine, methylprednisolone, paracetamol, and saline. Although hydration was not required prior to infusion of Gammaplex 5% or Gammaplex 10%, three pediatric patients received IV saline during the study; no adults received saline prior to any infusion.

Mean infusion duration and mean dose per infusion for Gammaplex 5% in adults and Gammaplex 10% in adult and pediatric subjects. SD standard deviation
AEs were reported more frequently by subjects receiving Gammaplex 10% (44 of 47 subjects [93.6%]) than those receiving Gammaplex 5% (23 of 33 subjects [69.7%]). In contrast, product-related AEs occurred in similar proportions of subjects receiving Gammaplex 10% (16 of 47 subjects [34.0%]) and Gammaplex 5% (12 of 33 subjects [36.4%]) (Supplemental Table S4). Among adults, product-related AEs that occurred in more than one subject were headache (12.5% [Gammaplex 10%] and 18.2% [Gammaplex 5%]), migraine (6.3% and 6.1%, respectively), pyrexia (6.3% and 0%, respectively), fatigue (3.1% and 6.1%, respectively), and nausea (3.1% and 6.1%, respectively). Among pediatric subjects, the only AE that occurred in more than one subject was headache (20.0%). ARs (i.e., AEs that occurred during the infusion or within 72 h after completion of the infusion were product-related or had unknown causality) are summarized in Table 3.
No serious product-related AEs occurred with either formulation, no subject withdrew due to an AE, and no thromboembolic events occurred during the study. No notable differences in adult subjects were observed between the two formulations of Gammaplex in the results of clinical laboratory, vital signs, physical examination, or body weight assessments. The Gammaplex 10% formulation was also well tolerated in pediatric subjects with PID.
Discussion
This study is the first direct comparison of 5% IVIG and 10% IVIG products in subjects with PID. In this study, the results of the PK analysis met the primary objective of demonstrating the bioequivalence of Gammaplex 10% IVIG and Gammaplex 5% IVIG at the 28-day dosing interval. The secondary objectives of demonstrating the bioequivalence of Gammaplex 10% and Gammaplex 5% were also met, with the exception of adjusted AUC0–τ over the 21-day dosing interval, which had an upper confidence limit (1.26) that was just outside the upper prescribed bound of 1.25. In both primary and secondary PK analyses, the 90% CIs for baseline-adjusted values were wider than those for the respective analyses of the absolute IgG measurements. Subtracting baseline values from subsequent values magnifies experimental error and may explain the observed upper confidence limit of 1.26 for the secondary endpoint.
Trough levels of IgG, IgG subclasses 1 to 3, and antibodies to specific antigens were well maintained with Gammaplex 5% and Gammaplex 10% throughout the study. The reduction in trough levels of IgG subclass 4 observed across all treatments and age groups was expected, since IgG4 is reduced in proportion to other IgG subclasses during the Gammaplex manufacturing process. The role of IgG4 has not been fully elucidated, and the reductions in levels seen during this study were not clinically significant. In one pediatric subject, consistently low trough IgG levels were observed despite a dose increase; the cause of this was unclear but may have been related to a change in metabolism of IVIG prior to initiating Gammaplex 10% treatment. Since terminating this study, this subject has continued to exhibit inconsistent but increasing IgG catabolism despite product changes and a dosing increase (Bio Products Laboratory, data on file). Among the adult subjects, the mean infusion duration was 34% shorter for Gammaplex 10% than for Gammaplex 5%. Infusion durations were not reduced by half, as might be expected with equivalent doses administered via a 10% versus a 5% product, because the starting infusion rate per study protocol for Gammaplex 10% was half that of Gammaplex 5% (Table 1), to allow for an equivalent initial protein dose.
To minimize infusion-related side effects [15,16,17], previous studies of IVIG products have increased infusion rates incrementally at intervals of 30 or 60 min [18, 19]. As infusion time is an important factor for patients, this study was prospectively designed to increase infusion rates incrementally at 15-min intervals, if tolerated, to shorten overall infusion times; as reported above, this approach resulted in mean infusion times of 1.9 h for Gammaplex 10% in adults, 2.8 h for Gammaplex 5% in adults, and 2.3 h for Gammaplex 10% in children. Using the dosing schedules and infusion rates employed in this study (including the use of a 15-min titration schedule), Gammaplex 10% and Gammaplex 5% were both safe and well tolerated in adult subjects with PID. No notable differences were observed between the safety profiles of the two formulations.
The Gammaplex 10% formulation was also safe and well tolerated in pediatric subjects with PID. Based on the bioequivalence and PK analysis from this bridging study in PID subjects, Gammaplex 10% can be expected to have a therapeutic effect similar to the licensed Gammaplex 5%, which has demonstrated tolerability and efficacy in adult and pediatric patients with PID and ITP [11,12,13].
References
Wood P, Stanworth S, Burton J, Jones A, Peckham DG, Green T, et al. Recognition, clinical diagnosis and management of patients with primary antibody deficiencies: a systematic review. Clin Exp Immunol. 2007;149:410–23.
Jolles S. Subcutaneous and intramuscular immune globulin therapy [updated 22 December 2015]. http://www.uptodate.com/contents/subcutaneous-and-intramuscular-immune-globulin-therapy. Accessed 9 September 2016.
Stiehm ER. Adverse effects of human immunoglobulin therapy. Transfus Med Rev. 2013;27:171–8.
Cunningham-Rundles C, Siegal FP, Smithwick EM, Lion-Boule A, Cunningham-Rundles S, O'Malley J, et al. Efficacy of intravenous immunoglobulin in primary humoral immunodeficiency disease. Ann Intern Med. 1984;101:435–9.
Liese JG, Wintergerst U, Tympner KD, Belohradsky BH. High- vs low-dose immunoglobulin therapy in the long-term treatment of X-linked agammaglobulinemia. Am J Dis Child. 1992;146:335–9.
Roifman CM, Lederman HM, Lavi S, Stein LD, Levison H, Gelfand EW. Benefit of intravenous IgG replacement in hypogammaglobulinemic patients with chronic sinopulmonary disease. Am J Med. 1985;79:171–4.
Orange JS. Clinical focus on primary immunodeficiencies: clinical update in immunoglobulin therapy for primary immunodeficiency diseases. https://primaryimmune.org/wp-content/uploads/2011/04/Clinical-Update-in-Immunoglobulin-Therapy-for-Primary-Immunodeficiency-Diseases.pdf. Accessed 9 September 2016.
Saeedian M, Randhawa I. Immunoglobulin replacement therapy: a twenty-year review and current update. Int Arch Allergy Immunol. 2014;164:151–66.
GAMMAPLEX. Immune globulin intravenous [human], 5% liquid, for intravenous use [package insert]. Elstree, UK: Bio Products Laboratory; 2015.
Gammaplex. A sterile liquid of 5% w/v normal immunoglobulin [summary of product characteristics]. Elstree, UK: Bio Products Laboratory; 2015.
Melamed IR, Gupta S, Stratford Bobbitt M, Hyland N, Moy JN. Efficacy and safety of Gammaplex® 5% in children and adolescents with primary immunodeficiency diseases. Clin Exp Immunol. 2016;184:228–36.
Moy JN, Scharenberg AM, Stein MR, Suez D, Roberts RL, Levy RJ, et al. Efficacy and safety of a new immunoglobulin G product, Gammaplex((R)), in primary immunodeficiency diseases. Clin Exp Immunol. 2010;162:510–5.
Dash CH, Gillanders KR, Stratford Bobbitt ME, Gascoigne EW, Leach SJ. Safety and efficacy of Gammaplex(R) in idiopathic thrombocytopenic purpura (ClinicalTrials.gov--NCT00504075). PLoS One. 2014;9:e96600.
ICH Steering Committtee. ICH harmonised tripartite guideline: guideline for good clinical practice e6(r1). http://www.ich.org/fileadmin/Public_Web_Site/ICH_Products/Guidelines/Efficacy/E6/E6_R1_Guideline.pdf. Accessed February 29, 2016.
Berger M. Adverse effects of IgG therapy. J Allergy Clin Immunol Pract. 2013;1:558–66.
Gelfand EW, Hanna K, Group I-CIMIRS. Safety and tolerability of increased rate of infusion of intravenous immunoglobulin G, 10% in antibody-deficient patients. J Clin Immunol. 2006;26:284–90.
Sleasman JW, Duff CM, Dunaway T, Rojavin MA, Stein MR. Tolerability of a new 10% liquid immunoglobulin for intravenous use, Privigen, at different infusion rates. J Clin Immunol. 2010;30:442–8.
Ballow M, Pinciaro PJ, Craig T, Kleiner G, Moy J, Ochs HD, et al. Flebogamma® 5% DIF intravenous immunoglobulin for replacement therapy in children with primary immunodeficiency diseases. J Clin Immunol. 2016;36:583–9.
Lozano-Blasco J, Martin-Mateos MA, Alsina L, Dominguez O, Giner MT, Piquer M, et al. A 10% liquid immunoglobulin preparation for intravenous use (Privigen(R)) in paediatric patients with primary immunodeficiencies and hypersensitivity to IVIG. Allergol Immunopathol (Madr). 2014;42:136–41.
Acknowledgments
The GMX07 Study Group included the following investigators: Oral Alpan, MD (O and O Alpan LLC, Fairfax, VA, USA); Dr. Ronnie Chee (Royal Free London NHS Foundation Trust, London, UK); Karin Chen, MD (Primary Children’s Hospital, Salt Lake City, UT, USA); Terry Chin, MD (MemorialCare Health Systems/Miller Children’s Hospital, Long Beach, CA, USA); Joseph A. Church, MD (Children’s Hospital Los Angeles, Los Angeles, CA, USA); David Elkayam, MD (Bellingham Asthma Allergy and Immunology Clinic, Bellingham, WA, USA); Dr. Stephen Jolles (University Hospital of Wales, Cardiff, UK); Michael Kaliner, MD (Institute for Asthma & Allergy, Chevy Chase, MD, USA); Gary Kleiner, MD, PhD (Joe DiMaggio Children’s Hospital, Hollywood, FL, USA); Gergely Krivan, MD (Egyesitett Szent Istvan es Szent Laszlo Korhaz-Rendelointezet, Budapest, Hungary); Isaac R. Melamed, MD (IMMUNOe – International Research Centers, Centennial, CO, USA); James N. Moy, MD (Rush University Medical Center, Chicago, IL, USA); Syed M. Rehman, MD (Toledo Institute of Clinical Research, Toledo, OH, USA); Mark R. Stein, MD (Allergy Associates of the Palm Beaches, PA, North Palm Beach, FL, USA); Richard L. Wasserman, MD, PhD (Allergy Partners of North Texas Research, Dallas, TX, USA); and Duane W. Wong, MD (Arizona Allergy Associates, Chandler, AZ, USA). The authors thank the subjects and their caregivers for their participation in the study and all staff at the study centers for their contributions. Bio Products Laboratory Ltd. provided funding for medical writing and editorial support in the development of this manuscript. Edwin Thrower, PhD, and Morgan C. Hill, PhD, of Ashfield Healthcare Communications (Middletown, CT, USA) revised the manuscript based on input from authors, and Dena McWain of Ashfield Healthcare Communications copyedited and styled the manuscript per journal requirements.
Authorship Contributions
Acquisition, analysis, and interpretation of data: RLW, IRM, MRS, SJ, MN, JNM
Critical revision of the manuscript for important intellectual content: RLW, IRM, MRS, SJ, MN, JNM
Approval of the manuscript for submission/publication: RLW, IRM, MRS, SJ, MN, JNM
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflict of Interest
RLW has served as a consultant for ADMA Biologics, Bio Products Laboratories, Grifols, Kedrion, Korean Green Cross, ProMetic, Shire, and Therapure; as an investigator for ADMA Biologics, Bio Products Laboratories, CSL Behring, Kedrion, Shire, and ProMetic; and as a speaker for Baxter/Shire and CSL Behring.
IRM has served as a clinical trial investigator for Bio Products Laboratory.
MRS has served as a consultant and speaker for Baxter Healthcare, Green Cross, and CSL Behring; and as an investigator for ADMA Biologics, Green Cross, ProMetic, Bio Products Laboratories, and Kedrion.
SJ reports consulting, speaker, travel, advisory board, and research support from CSL Behring, Baxter, Bio Products Laboratory, Biotest, SOBI, Shire, Viropharma, and Octapharma.
MN is an employee of Bio Products Laboratory.
JNM has served as a clinical trial investigator for Bio Products Laboratory, a consultant for Baxter and ProMetic, and an iDMC member for MacroCure and Octapharma.
Funding
This study was supported by Bio Products Laboratory (Study GMX07).
Additional information
An erratum to this article is available at http://dx.doi.org/10.1007/s10875-017-0418-2.
Electronic Supplementary Material
ESM 1
(DOCX 45 kb)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made.
The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
To view a copy of this licence, visit https://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wasserman, R.L., Melamed, I.R., Stein, M.R. et al. Evaluation of the Safety, Tolerability, and Pharmacokinetics of Gammaplex® 10% Versus Gammaplex® 5% in Subjects with Primary Immunodeficiency. J Clin Immunol 37, 301–310 (2017). https://doi.org/10.1007/s10875-017-0383-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10875-017-0383-9