
Abstract
To elucidate the role of neighborhood walkability and crime on weight loss, we examined data from older adults residing in Chicago who participated in a randomized controlled trial lifestyle intervention. Controlling for individual demographic characteristics and the intervention assignment, the neighborhood homicide rate was significantly associated with weight change. Participants who resided in neighborhoods above the 50th percentile of homicide rate actually gained weight between pre- and post-intervention. On the other hand, there was no significant relationship between the level of walkability and weight loss. Our findings suggest that the social environment related to neighborhood crime may play a more important role in weight loss than the built environment, such as walkability. Urban characteristics related to walkability, such as sidewalks, may increase physical activity, however, interventions aiming to increase physical activity to promote weight loss will benefit by addressing the neighborhood social environment that determines how people navigate space.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The prevalence of adult obesity with Body Mass Index (BMI) greater than 30 is expected to reach nearly 50% of the United States (U.S.) population by 2030 (Centers for Disease Control and Prevention, 2022; Ward et al., 2019). While obesity is associated with multiple deleterious health outcomes, including cardiometabolic diseases and cancers (Afshin et al., 2017; Dixon, 2010; Lauby-Secretan et al., 2016; Wannamethee, Gerald Shaper, Whincup, Lennon, & Sattar, 2011), lifestyle weight-loss interventions have been shown to be beneficial in reducing a variety of these negative health conditions (Anderson et al., 2014; Appel et al., 2011; Elmer et al., 2006; Maruthur, Wang, & Appel, 2009) by improving glucose metabolism and reducing inflammation and oxidative stress, all of which contribute to cardiovascular and metabolic health risks (Esposito et al., 2003; Lofgren et al., 2005; Van Gaal, Wauters, & De Leeuw, 1997).
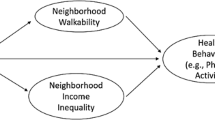
Studies have documented the effect of neighborhood social conditions, including social support and cohesion, a sense of community, crime and violence, and informal social control, on how people interact with others and with the environment (Bursik & Grasmick, 1993; Sampson, 2003; Shaw & McKay, 1942; Zorbaugh, 1929). Furthermore, neighborhood economic conditions that limit options for healthy good and opportunities for physical activity have been shown to be associated with obesity and weight gain (Black & Macinko, 2008; Coogan et al., 2012; Zhang, Bauer, Powell-Wiley, & Xiao, 2021). As such, neighborhood social and economic conditions determine the built environment (i.e., the physical aspects of where one lives). Research on the built environment has increased significantly over the past decades (Jackson et al., 2013), with an emphasis on how the built environment influences lifestyle behaviors that in turn affect weight management (Brownson et al., 2009; Laddu, Pauluch, & LaMonte, 2021; Scott, Dubowitz, & Cohen, 2009).
The built environment may influence individuals’ health by either facilitating or impeding healthy lifestyle behaviors, including adequate physical activity (Barnett et al., 2017). One important feature of the built environment is walkability. Walkability relates to aspects of physical structures that influence walking as a method of travel U.S. (Environmental Protection Agency, 2021). Studies have documented that people living in more walkable areas tend to be more physically active (Chen et al., 2019; Colley, Christidis, Michaud, Tjepkema, & Ross, 2019) and tend to have lower BMI (Casagrande et al., 2011; Cerin et al., 2018; Creatore et al., 2016; Hoehner, Handy, Yan, Blair, & Berrigan, 2011). Interestingly, however, Zenk and colleagues compared the effects of a weight management program between people living in neighborhoods with variations in the levels of walkability and access to recreational places and found no difference in the program’s effect by the level of neighborhood walkability (Zenk et al., 2019).
Prevalent crime as a component of the built environment, may be a barrier to walkability and physical activity (Gomez et al., 2004; Robinson, Carnes, & Oreskovic, 2016), and yet, research has produced conflicting findings regarding the association between physical activity and neighborhood crime rates (Foster et al., 2014a; Loukaitou-Sideris, 2006; Loukaitou-Sideris & Eck, 2007). While some studies show that higher crime rates and lower reported safety are associated with lower levels of physical activity (Boehmer et al., 2006; Gomez et al., 2004; Richardson, Troxel, Ghosh-Dastidar, et al., 2017; Schoeny, Fogg, Buchholz, Miller, & Wilbur, 2016), other studies have found no effect between these factors and physical activity (Prince et al., 2011; Ruijsbroek, Droomers, Groenewegen, Hardyns, & Stronks, 2015).
Perceptions of neighborhood safety may influence these contradictory findings (Giles-Corti & Donovan, 2002). Perceived neighborhood safety seems to determine levels of physical activity, even after controlling for observed safety, such as neighborhood crime (Janssen, 2014). Other studies have documented the relationship between perceived neighborhood safety, physical activity, and obesity (Bacha et al., 2010; Chaparro, Bilfield, & Theall, 2019; Prins et al., 2013), with higher levels of perceived safety and access to recreational facilities associated with higher physical activity levels among low-income adults (Wilson-Frederick et al., 2014). A meta-analysis found that perceived fear of crime and actual crime rates were inversely correlated with physical inactivity (Rees-Punia et al., 2018). Overall, people who reported feeling safe from crime had 27% greater odds of achieving higher levels of physical activity, whereas those living in areas with high levels of actual crime had 28% lower odds of achieving higher levels of physical activity (Rees-Punia et al., 2018).
Interestingly, Foster and colleagues (Foster et al., 2014a) found that higher levels of certain types of crime, such as burglary and other personal crimes, were associated with increased walkability (Foster et al., 2014a). The authors speculated that walkable conditions may promote walking, while at the same time more people in the public sphere may increase opportunities for crime to take place. There is some evidence to suggest that the relationship between crime and physical activity may vary depending on the type of crime. Although high homicide rates (Kerr et al., 2015) and fear of crime (McGinn et al., 2008) seem to be associated with decreased walking, perceived drug-related crime has been associated with a higher level of walkability (Mason et al., 2013). Overall, the relationship between crime and walkability in current literature seems to be inconclusive.
This study aims to elucidate the role of walkability and neighborhood crime on weight loss using data from older Chicago residents participating in a randomized controlled trial (RCT) lifestyle intervention. This original RCT included predominantly Black older adults who lived on the South Side of Chicago, which is highly racially segregated and affected by increased crime. We hypothesized that neighborhood walkability and homicide would have differential effects on participants’ weight loss and physical activity. Specifically, pre- and post-intervention weight loss would be greater for participants living in neighborhoods with high walkability and lower for participants living in neighborhoods with high homicide rates.
Methods
Setting and data
This analysis utilized data from an RCT, Building Research in Diet and CoGnition (BRIDGE). Details on the trial have been published previously (Sanchez-Flack et al., 2020; Tussing-Humphreys et al., 2017). Briefly, the BRIDGE trial recruited 185 healthy, predominantly African American older adults over 55 years of age with a BMI greater than 30 kg/m2. Participants were randomized into three arms: MedDiet with a weight loss intervention (MedDiet-WL), MedDiet (MedDiet-A) without a weight loss intervention, and a Control group (TDC) with a typical diet without caloric restriction (Tussing-Humphreys et al., 2017). The two intervention groups met once weekly for 8 months, totaling 25 sessions. Baseline data were collected between 2017 and 2019. The study examined the effects of the intervention on cognitive functioning, as well as weight control, dietary intake, and cardiovascular, metabolic, and immune-related biomarkers. The BRIDGE trial was approved by the University of Illinois at Chicago (UIC) Institutional Review Board (IRB# 2016 − 0258) and has been registered at ClinicalTrials.gov (NCT03129048).
Variables and statistical analysis
Of the 185 original study participants, our analysis included 184 participants who resided within Cook County, Illinois. We geocoded participants’ residential addresses using ArcGIS and appended census tract numbers which were used to merge with the neighborhood variables.
The outcome variable was weight change between pre- and post-intervention (i.e., weight measurement taken eight months after the intervention). Individual-level measures included age (ranging between 55 and 81 years), sex (female vs. male), race (Black vs. all other groups), income (less than $40,000 vs. $40,000 or more), and education (high school or lower, some college, and college or higher). We also included the level of pre-intervention moderate to vigorous physical activity in minutes per day measured by the ActiGraph wGT3X triaxial accelerometer (Santos-Lozano et al., 2012).
Two neighborhood exposure variables were developed: walkability and crime. We used the National Walkability Index developed by the U.S. Environmental Protection Agency, which incorporates three indicators: intersection density (design), proximity to transit stops (distance), and mix of employment and household types (diversity) (Ewing & Cervero, 2010; Hajna et al., 2015; Kärmeniemi, Lankila, Ikäheimo, Koivumaa-Honkanen, & Korpelainen, 2018; Saelens, Sallis, Black, & Chen, 2003; Van Holle et al., 2012). The EPA National Walkability Index ranges between 1 and 20, with scores below 5.76 indicating the least walkable areas, scores above 15.26 indicating the most walkable areas, and a score of 10.50 reflecting average walkability (U.S. Environmental Protection Agency, 2021).
Neighborhood crime was measured using homicide incident cases from the Cook County Medical Examiner’s archive, which includes all homicide deaths along with the address of each incident (Cook County Medical Examiner’s Office, 2021). We geocoded the incident address using ArcGIS and calculated the homicide rates at the census tract level. Walkability and neighborhood crime measures were examined as dichotomous variables, with greater than the 50th percentile treated as high walkability and high crime areas. We appended neighborhood walkability and crime data to participant records, using the participant’s address at the time of enrollment. We conducted descriptive statistics to characterize the sample. To assess differences in weight loss between pre- and post-intervention by walkability and crime, we performed regression analysis. We used Stata version 16 (StataCorp, LLC) for all statistical analyses.
Results
Table 1 describes characteristics of the study population and summarizes the distribution of participant characteristics by walkability score. The mean age of participants was 66 years, and the majority of participants were female and African American. More than 50% of participants had annual incomes over $40,000 and college or more education. Walkability scores in our sample ranged from 5.7 to 19.0, with a mean of 13.4. Over 91% of study participants lived in neighborhoods with a walkability score greater than the national average of 10.51. Neighborhoods with high walkability scores (above the 50th percentile) had a significantly lower average homicide rate, compared with areas with low walkability scores (below the 50th percentile). Sociodemographic and neighborhood characteristics did not differ by walkability score.
Table 2 presents the results of linear regression, with correlation coefficients for walkability score and homicide rate on weight change between pre- and post-intervention. Intervention assignment, age, gender, T1 weight, education, T1 physical activity, and household income were controlled for. Overall, study participants lost an average of 2.93 kg. Walkability score was not significantly associated with a weight change (p < .10). However, the homicide rate was significantly associated with a weight change (p < .05). Participants who resided in neighborhoods with a homicide rate above the 50th percentile lost 1.73 kg less than participants who lived in low homicide areas, controlling for all other confounders. Figure 1 illustrates the marginal effects of walkability and homicide rate on weight loss from the linear regression. Overall participants who lived in low homicide areas lost more weight than those in high homicide areas regardless of walkability. However, among those who lived in low homicide areas, high walkability was associated with greater weight loss than low walkability. For those who lived in high homicide areas, interestingly, high walkability actually was associated with less weight loss than low walkability.

Average weight loss between pre and post-intervention by walkability and homicide rate
Discussion
Our findings showed that neighborhood crime measured by the homicide rate was significantly associated with less weight loss, controlling for all other variables including the intervention assignment. Participants who resided in neighborhoods at or above the 50th percentile of homicide rate actually gained weight between pre-and post-intervention, regardless of randomization to one of the three intervention arms. On the other hand, the relationship between neighborhood walkability and weight loss was not statistically significant.
Current literature suggests that individuals living in high walkability areas tend to be more physically active. High walkability seems to decrease the risk of excessive weight gain (Lovasi et al., 2009; Rundle et al., 2008). Urban characteristics of walkable areas, such as sidewalks, increase physical activity (Hirsch et al., 2016; Rundle et al., 2016). Thus, policies to improve neighborhood walkability have been promoted for their potential positive impact on residents’ health (Centers for Disease Control & Prevention, 2020). High crime may negate the benefits of a walkable neighborhood environment for physical activity and weight management. Our findings, however, seem to suggest that the social environment, compared with the built environment, may play a more important role in residents’ weight loss. One of the reasons for this might be that the overall walkability score was higher in all Chicago neighborhoods than the national average. Chicago is a large urban city with high density, a mix of real estate types, and well-developed public transportation options (Leinberger & Rodriguez, 2016). In fact, Chicago is consistently ranked among the top-ten most walkable cities in the U.S. (Metromile, 2022; Walk Score, 2023). Indeed, study participants lived in Chicago neighborhoods with higher-than average walkability, and the lack of variability in the walkability score among study participants may have limited our ability to fully examine the contribution of walkability on physical activity and weight loss.
Conversely, high-crime neighborhoods are associated with a variety of poor health outcomes (Sampson, 2003; Won, Lee, Forjuoh, & Ory, 2016), and crime is shown to be a deterrent to residents’ physical activity (Gomez et al., 2004; Mason et al., 2013; Rees-Punia et al., 2018; Richardson, Troxel, Ghosh-Dastidar, et al., 2017; Robinson et al., 2016). Although some studies have found contradicting results (Pratt et al., 2015; Richardson, Troxel, Bhosh-Dastidar, et al., 2017). When aspects of the social environment, such as crime, are considered, the benefits of walkability may be diminished. Neighborhood crime is associated with residents’ fear of crime, which in turn influences engagement in outdoor physical activity. This argument is bolstered by the fact that the majority of neighborhoods within our study had similarly high levels of walkability, but different homicide rates. Among residents living in communities with high rates of homicide, walking may be perceived as dangerous (Jack & McCormack, 2014; Singh, 2016; Van Dyck, Veitch, De Bourdeaudhuij, Thornton, & Ball, 2013). The decision to choose outdoor physical activity may be influenced by homicide rates in the community independent of walkability score.
Although much of the scientific literature finds that urban communities with high walkability may also have high levels of crime (Foster et al., 2014b, 2021; Lee & Contreras, 2021), our findings indicate a more complex relationship between walkability and crime rates. We saw that areas with the highest walkability had lower homicide rates, reflecting current literature. At the same time, to a certain level, higher walkability was correlated with higher homicide rates. Urban communities with high walkability may also have high levels of crime rates (Foster et al., 2014b, 2021; Lee & Contreras, 2021). When walkability is high, residents living in disadvantaged neighborhoods may experience higher levels of violence compared to those in advantaged neighborhoods (Foster et al., 2014b, 2021; Lee & Contreras, 2021). Our findings warrant further investigation into the relationship between social conditions and the built environment, which perhaps interact to influence residents’ health behavior and consequently health outcomes.
Conclusion
Regular physical activity can positively influence weight management, but not all communities benefit equally from this component of the built environment because walkability is subject to the effects of the social environment, such as high crime. While the built environment represents the physical aspects of where one lives, the social environment creates space for residents to engage with their neighborhood. Interventions aiming to increase physical activity and promote healthy weight management will benefit by incorporating factors of the neighborhood social environment that determine how people navigate space. The social environment related to neighborhood crime may play a more important role in weight loss than aspects of the built environment such as walkability. The social environment and built environment may affect different aspects of urban neighborhood characteristics. Accordingly, urban policy and planning must take into account the interaction between the built and the social environments to facilitate residents’ health and well-being.
Change history
13 June 2023
A Correction to this paper has been published: https://doi.org/10.1007/s10865-023-00430-w
References
Afshin, A., Forouzanfar, M. H., Reitsma, M. B., Sur, P., Estep, K., Lee, A., & Tegegne, B. S. (2017). Health Effects of overweight and obesity in 195 countries over 25 years. The New England journal of medicine, 377(1), 13–27. https://doi.org/10.1056/NEJMoa1614362.
Anderson, A. S., Craigie, A. M., Caswell, S., Treweek, S., Stead, M., Macleod, M., & Steele, R. J. C. (2014). The impact of a bodyweight and physical activity intervention (BeWEL) initiated through a national colorectal cancer screening programme: Randomised controlled trial. BMJ: British Medical Journal, 348, https://doi.org/10.1136/bmj.g1823.
Appel, L. J., Clark, J. M., Yeh, H. C., Wang, N. Y., Coughlin, J. W., Daumit, G., & Brancati, F. L. (2011). Comparative effectiveness of weight-loss interventions in clinical practice. The New England journal of medicine, 365(21), 1959–1968. https://doi.org/10.1056/NEJMoa1108660.
Bacha, J., Appugliese, D., Coleman, S., Kaciroti, N., Bradley, R., Corwyn, R., & Lumeng, J. (2010). Maternal perception of neighborhood safety as a predictor of child weight status. The moderating effect of gender and assessment of potential mediators. Int J Ped Obes, 5, 72–79.
Barnett, D., Barnett, A., Nathan, A., Van Cauwenberg, J., & Cerin, E. (2017). Built environmental correlates of older adults’ total physical activity and walking: A systematic review and meta-analysis. Int J Behav Nutr Phys Act, 14(1), https://doi.org/10.1186/s12966-12017-10558-z.
Black, J., & Macinko, J. (2008). Neighborhoods and obesity. Nutrition Reviews, 66(1), 2–20. https://doi.org/10.1111/j.1753-4887.2007.00001.x.
Boehmer, T., Lovegreen, S., Haire-Joshu, D., & Brownson, R. (2006). What constitutes an obesogenic environment in rural communities? Am J Health Prom, 20(6), 411–421. https://doi.org/10.4278/0890-1171-20.6.411.
Brownson, R., Hoehner, C., Day, K., Forsyth, A., & Sallis, J. (2009). Measuring the built environment for physical activity. American Journal Of Preventive Medicine, 36(4 suppl), 99–123e112. https://doi.org/10.1016/j.amepre.2009.01.005.
Bursik, J., & Grasmick, H. (1993). Neighborhoods and crime: The dimensions of effective community control. New York: NY Lexington Books.
Casagrande, S. S., Gittelsohn, J., Zonderman, A. B., Evans, M. K., & Gary-Webb, T. L. (2011). Association of Walkability with obesity in Baltimore City, Maryland. American journal of public health (1971), 101(S1), S318–S324. https://doi.org/10.2105/AJPH.2009.187492.
Centers for Disease Control & Prevention (2020). Designing Activity-Friendly Communities. Retrieved November 11, 2022, from https://www.cdc.gov/nccdphp/dnpao/features/walk-friendly-communities/index.html
Centers for Disease Control and Prevention (2022). Defining Adult Overweight & Obesity. from https://www.cdc.gov/obesity/adult/defining.html
Cerin, E., Conway, T., Adams, M., Barnett, A., Cain, K., Owen, N., & Sallis, J. (2018). Objectively-assessed neighbourhood destination accessibility and physical activity in adults from 10 countries: An analysis of moderators and perceptions as mediators. Social Science And Medicine, 211, 282–293.
Chaparro, M. P., Bilfield, A., & Theall, K. (2019). Exposure to Neighborhood Crime is Associated with lower levels of physical activity and higher obesity risk among adolescent girls, but not Boys. Childhood Obesity, 15(2), 87–92.
Chen, B. I., Hsueh, M. C., Rutherford, R., Park, J. H., & Liao, Y. (2019). The associations between neighborhood walkability attributes and objectively measured physical activity in older adults. PloS one, 14(9), e0222268–e0222268. https://doi.org/10.1371/journal.pone.0222268.
Colley, R. C., Christidis, T., Michaud, I., Tjepkema, M., & Ross, N. A. (2019). The association between walkable neighbourhoods and physical activity across the lifespan. Health reports, 30(9), 3–13. https://doi.org/10.25318/82-003-x201900900001-eng.
Coogan, P., Cozier, Y., Krishnan, S., Wise, L., Adams-Campbell, L., Rosenbreg, L., & Palmer, J. (2012). Neighborhood Socioeconomic Status in Relation to 10-Year Weight Gain in the Black Women’s Health Study. Obesity (Silver Spring, Md.), 18(10), 2064–2065. https://doi.org/10.1038/oby.2010.69.
Cook County Medical Examiner’s Office (2021). Medical Examiner Case Archive. Retrieved June 15, 2022, from https://datacatalog.cookcountyil.gov/Public-Safety/Medical-Examiner-Case-Archive/cjeq-bs86
Creatore, M. I., Glazier, R. H., Moineddin, R., Fazli, G. S., Johns, A., Gozdyra, P., & Booth, G. L. (2016). Association of Neighborhood Walkability with Change in overweight, obesity, and diabetes. JAMA: the journal of the American Medical Association, 315(20), 2211–2220. https://doi.org/10.1001/jama.2016.5898.
Dixon, J. B. (2010). The effect of obesity on health outcomes. Molecular and cellular endocrinology, 316(2), 104–108. https://doi.org/10.1016/j.mce.2009.07.008.
Elmer, P. J., Obarzanek, E., Ard, J., Brantley, P. J., Proschan, M. A., Erlinger, T. P., & Svetkey, L. P. (2006). Effects of Comprehensive Lifestyle modification on Diet, Weight, Physical Fitness, and blood pressure control: 18-Month results of a Randomized Trial. Annals of internal medicine, 144(7), 485–495. https://doi.org/10.7326/0003-4819-144-7-200604040-00007.
Esposito, K., Pontillo, A., Di Palo, C., Giugliano, G., Masella, M., Marfella, R., & Giugliano, D. (2003). Effect of weight loss and lifestyle changes on vascular inflammatory markers in obese women: A randomized trial. Journal Of The American Medical Association, 289(14), 1799–1804.
Ewing, R., & Cervero, R. (2010). Travel and the built environment. Journal of the American Planning Association, 76(3), 265–294. https://doi.org/10.1080/01944361003766766.
Foster, S., Hooper, P., Burton, N. W., Brown, W. J., Giles-Corti, B., Rachele, J. N., & Turrell, G. (2021). Safe habitats: Does the Association between Neighborhood Crime and walking Differ by Neighborhood Disadvantage? Environment and Behavior, 53(1), 3–39. https://doi.org/10.1177/0013916519853300.
Foster, S., Knuiman, M., Villanueva, K., Wood, L., Christian, H., & Giles-Corti, B. (2014a). Does walkable neighbourhood design influence the association between objective crime and walking? Int J Behav Nutr Phys Act, 26(11), https://doi.org/10.1186/s12966-12014-10100-12965.
Foster, S., Knuiman, M., Villanueva, K., Wood, L., Christian, H., & Giles-Corti, B. (2014b). Does walkable neighbourhood design influence the association between objective crime and walking? Int J Behav Nutr Phys Act, 26(11), https://doi.org/10.1186/s12966-12014-10100-12965.
Giles-Corti, B., & Donovan, R. (2002). The relative influence of individual, social and physical environment determinants of physical activity. Social Science And Medicine, 54(12), 1793–1812.
Gomez, J., Johnson, B. A., Selva, M., & Sallis, J. (2004). Violent crime and outdoor physical activity among inner-city youth. Preventive Medicine, 39, 876–881.
Hajna, S., Ross, N. A., Brazeau, A. S., Bélisle, P., Joseph, L., & Dasgupta, K. (2015). Associations between neighbourhood walkability and daily steps in adults: A systematic review and meta-analysis. Bmc Public Health, 15(1), https://doi.org/10.1186/s12889-015-2082-x.
Hirsch, J. A., Winters, M., Ashe, M. C., Clarke, P. J., & McKay, H. A. (2016). Destinations that older adults experience within their GPS activity spaces. Environment and Behavior, 48(1), 55–77. https://doi.org/10.1177/0013916515607312.
Hoehner, C. M., Handy, S. L., Yan, Y., Blair, S. N., & Berrigan, D. (2011). Association between Neighborhood Walkability, Cardiorespiratory Fitness, and Body-Mass Index: 2169 Board #46 June 2 3:30 PM – 5:00 PM. Medicine and science in sports and exercise, 43(5), 569–570. https://doi.org/10.1249/01.MSS.0000401569.04304.b9.
Jack, E., & McCormack, G. R. (2014). The associations between objectively-determined and self-reported urban form characteristics and neighborhood-based walking in adults. International Journal of Behavioral Nutrition and Physical Activity, 11(1), 71. https://doi.org/10.1186/1479-5868-11-71.
Jackson, R., Dannenberg, A., & Frumkin, H. (2013). Health and the built environment: 10 years after. American Journal of Public Health, 103(9), 1542–1544. https://doi.org/10.2105/AJPH.2013.301482.
Janssen, I. (2014). Crime and perceptions of safety in the home neighborhood are independently associated with physical activity among 11–15 year olds. Preventive Medicine, 66, 113–117.
Kärmeniemi, M., Lankila, T., Ikäheimo, T., Koivumaa-Honkanen, H., & Korpelainen, R. (2018). The built environment as a determinant of physical activity: A systematic review of Longitudinal Studies and Natural experiments. Annals of Behavioral Medicine, 52(3), 239–251. https://doi.org/10.1093/abm/kax043.
Kerr, Z., Evenson, K., Moore, K., Block, R., & Diez Roux, A. V. (2015). Changes in walking associated with perceived neighbourhood safety and police-recorded crime: The multi-ethnic study of atherosclerosis. Preventive Medicine, 73, 88–93.
Laddu, D., Pauluch, A., & LaMonte, M. (2021). The role of the built environment in promoting movement and physical activity across the lifespan: Implications for public health. Progress in Cardiovascular Diseases, 64, 33–40.
Lauby-Secretan, B., Scoccianti, C., Loomis, D., Grosse, Y., Bianchini, F., & Straif, K. (2016). Body fatness and Cancer — viewpoint of the IARC Working Group. The New England journal of medicine, 375(8), 794–798. https://doi.org/10.1056/NEJMsr1606602.
Lee, N., & Contreras, C. (2021). Neighborhood Walkability and Crime: Does the Relationship Vary by Crime Type? Environment and Behavior, 53(7), 753–786. https://doi.org/10.1177/0013916520921843.
Leinberger, C., & Rodriguez, M. (2016). Foot traffic ahead: Ranking walkable urbanism in America’s largest metros, 2016. Retrieved from Washington, DC: https://smartgrowthamerica.org/wp-content/uploads/2016/06/foot-traffic-ahead-2016.pdf
Lofgren, I., Herron, K., West, K., Zern, T., Patalay, M., Koo, S., & Fernandez, M. (2005). Carbohydrate intake is correlated with biomarkers for coronary heart disease in a population of overweight premenopausal women. Journal of Nutritional Biochemistry, 16(4), 245–250.
Loukaitou-Sideris, A. (2006). Is it safe to walk?1 Neighborhood Safety and Security Considerations and their Effects on walking. Journal of Planning Literature, 20(3), 219–232.
Loukaitou-Sideris, A., & Eck, J. (2007). Crime prevention and active living. American Journal of Health Promotion, 21(4s), 380–389.
Lovasi, G. S., Neckerman, K. M., Quinn, J. W., Weiss, C. C., & Rundle, A. (2009). Effect of individual or Neighborhood Disadvantage on the Association between Neighborhood Walkability and Body Mass Index. American Journal of Public Health, 99(2), 279–284. https://doi.org/10.2105/ajph.2008.138230.
Maruthur, N. M., Wang, N. Y., & Appel, L. J. (2009). Lifestyle Interventions Reduce Coronary Heart Disease Risk: Results From the PREMIER Trial. Circulation (New York, N.Y.), 119(15), 2026–2031. doi:https://doi.org/10.1161/CIRCULATIONAHA.108.809491
Mason, P., Kearns, A., & Livingston, M. (2013). Safe Going”: The influence of crime rates and perceived crime and safety on walking in deprived neighbourhoods. Social Science & Medicine, 91, 15–24.
McGinn, A., Evenson, K., Herring, A., Huston, S., & Rodriguez, D. (2008). The association of perceived and objectively measured crime with physical activity: A cross-sectional analysis. Journal of Physical Activity & Health, 5(1), 117–131.
Metromile. (2022). What are the most. Walkable Cities in the U.S.?.
Pratt, M., Yin, S., Soler, R., Njai, R., Siegel, P., & Liao, Y. (2015). Does Perceived Neighborhood Walkability and Safety Mediate the Association between Education and Meeting Physical Activity Guidelines? Preventing Chronic Disease, 12, 140570. https://doi.org/10.5888/pcd12.140570.
Prince, S., Kristjansson, E., Russell, K., Billette, J. M., Sawada, M., Ali, A., & Prud’homme, D. (2011). A multilevel analysis of neighbourhood built and social environments and adult self-reported physical activity and body mass index in Ottawa, Canada. International Journal Of Environmental Research And Public Health, 8, 3953–3978.
Prins, R., Kamphuis, C., van Empelen, P., Beenackers, M., Brug, J., Mackenbach, J., & Oenema, A. (2013). Explaining socio-demographic differences in disengagement from sports in adolescence. Eur J Public Health, 23, 811–816.
Rees-Punia, E., Hathaway, E., & Gay, J. (2018). Crime, perceived safety, and physical activity: A meta-analysis. Preventive Medicine, 111, 307–313.
Richardson, A., Troxel, W., Bhosh-Dastidar, M., Beckman, R., Hunter, G., DeSantis, A., & Dubowitz, T. (2017). One size doesn’t fit all: Cross-sectional associations between neighborhood walkability, crime and physical activity depends on age and sex of residents. Bmc Public Health. https://doi.org/10.1186/s12889-016-3959-z.
Richardson, A., Troxel, W., Ghosh-Dastidar, M., Hunter, G., Beckman, R., Colabianchi, N., & Dubowitz, T. (2017). Pathways through which higher neighborhood crime is longitudinally associated with greater body mass index. International Journal of Behavioral Nutrition and Physical Activity, 14(155), https://doi.org/10.1186/s12966-12017-10611-y.
Robinson, A., Carnes, F., & Oreskovic, N. (2016). Spatial analysis of crime incidence and adolescent physical activity. Preventive Medicine, 85, 74–77.
Ruijsbroek, A., Droomers, M., Groenewegen, P., Hardyns, W., & Stronks, K. (2015). Social safety, self-rated general health and physical activity: Changes in area crime, area safety feelings and the role of social cohesion. Health & Place, 31, 39–45.
Rundle, A., Field, S., Park, Y., Freeman, L., Weiss, C. C., & Neckerman, K. (2008). Personal and neighborhood socioeconomic status and indices of neighborhood walk-ability predict body mass index in New York City. Social Science & Medicine, 67(12), 1951–1958. https://doi.org/10.1016/j.socscimed.2008.09.036.
Rundle, A. G., Sheehan, D. M., Quinn, J. W., Bartley, K., Eisenhower, D., Bader, M. M. D., & Neckerman, K. M. (2016). Using GPS Data to Study Neighborhood Walkability and Physical Activity. American Journal of Preventive Medicine, 50(3), e65–e72. https://doi.org/10.1016/j.amepre.2015.07.033.
Saelens, B. E., Sallis, J. F., Black, J. B., & Chen, D. (2003). Neighborhood-Based differences in physical activity: An Environment Scale evaluation. American Journal of Public Health, 93(9), 1552–1558. https://doi.org/10.2105/ajph.93.9.1552.
Sampson, R. (2003). Neighborhood-level context and health: Lessons from sociology. In I. Kawachi, & L. Berkman (Eds.), Neighborhoods and health. New York, NY: Oxford University Press.
Sanchez-Flack, J., Tussing-Humphreys, L., Lamar, M., Fantuzzi, G., Schiffer, L., Blumstein, L., & Fitzgibbon, M. (2020). Building research in diet and cognition (BRIDGE): Baseline characteristics of older obese african american adults in a randomized controlled trial to examine the effect of the Mediterranean diet with and without weight loss on cognitive functioning. Pre Med Rep, 101302, https://doi.org/10.1016/j.pmedr.2020.101302.
Santos-Lozano, A., Marin, P., Torres-Luque, G., Ruiz, J., Lucia, A., & Garatachea, N. (2012). Technical variability of the GT3X accelerometer. Medical Engineering & Physics, 34(6), 787–790.
Schoeny, M., Fogg, L., Buchholz, S., Miller, A., & Wilbur, J. E. (2016). Barriers to physical activity as moderators of intervention effects. Preventive Medicine Reports, 5, 57–64. https://doi.org/10.1016/j.pmedr.2016.11.008.
Scott, M., Dubowitz, T., & Cohen, D. (2009). Regional differences in walking frequency and BMI: What role does the built environment play for Blacks and Whites? Health & Place, 15(3), 897–902.
Shaw, C., & McKay, H. (1942). Juvenile delinquency and urban areas. Juvenile delinquency and urban areas. Chicago, IL: University of Chicago Press.
Singh, R. (2016). Factors affecting walkability of neighborhoods. Procedia - Social and Behavioral Sciences, 216, 643–654. https://doi.org/10.1016/j.sbspro.2015.12.048.
Tussing-Humphreys, L., Lamar, M., Blumenthal, J. A., Babyak, M., Fantuzzi, G., Blumstein, L., & Fitzgibbon, M. L. (2017). Building research in diet and cognition: The BRIDGE randomized controlled trial. Contemporary Clinical Trials, 59, 87–97. https://doi.org/10.1016/j.cct.2017.06.003.
U.S. Environmental Protection Agency (2021). Walkability Index. Retrieved June 15, 2022, from https://edg.epa.gov/metadata/catalog/search/resource/details.page?uuid=%7B251AFDD9-23A7-4068-9B27-A3048A7E6012%7D
Van Dyck, D., Veitch, J., De Bourdeaudhuij, I., Thornton, L., & Ball, K. (2013). Environmental perceptions as mediators of the relationship between the objective built environment and walking among socio-economically disadvantaged women. International Journal of Behavioral Nutrition and Physical Activity, 10(1), 108. https://doi.org/10.1186/1479-5868-10-108.
Van Gaal, L., Wauters, M., & De Leeuw, I. (1997). The beneficial effects of modest weight loss on cardiovascular risk factors. International Journal of Obesity & Related Metabolic Disorders, 21(Suppl 1), S5–S9.
Van Holle, V., Deforche, B., Van Cauwenberg, J., Goubert, L., Maes, L., Van De Weghe, N., & De Bourdeaudhuij, I. (2012). Relationship between the physical environment and different domains of physical activity in european adults: A systematic review. Bmc Public Health, 12(1), 807. https://doi.org/10.1186/1471-2458-12-807.
Walk Score (2023). Cities & Neighborhoods. from ttps://www.walkscore.com/cities-and-neighborhoods/
Wannamethee, S. G., Gerald Shaper, A., Whincup, P. H., Lennon, L., & Sattar, N. (2011). Obesity and risk of Incident Heart failure in older men with and without pre-existing Coronary Heart Disease: Does Leptin have a role? Journal of the American College of Cardiology, 58(18), 1870–1877. https://doi.org/10.1016/j.jacc.2011.06.057.
Ward, Z., Bleich, S., Cradock, A., Barrett, J., Giles, C., Flax, C., & Gortmaker, S. (2019). Projected U.S. State-Level prevalence of adult obesity and severe obesity. New England Journal of Medicine, 381, 2440–2450. https://doi.org/10.1056/NEJMsa1909301.
Wilson-Frederick, S., Thorpe Jr, R., Bell, C., Bleich, S., Ford, J., & LaVeist, T. (2014). Examination of race disparities in physical inactivity among adults of similar social context. Ethnicity And Disease, 24(3), 363–369.
Won, J., Lee, C., Forjuoh, S., & Ory, M. (2016). Neighborhood safety factors associated with older adults’ health-related outcomes: A systematic literature review. Social Science & Medicine, 165, 177–186.
Zenk, S., Tarlov, E., Wing, C., Slater, S., Jones, K., Fitzgibbon, M., & Powell, L. (2019). Does the built environment influence the effectiveness of behavioral weight management interventions? Preventive Medicine, 126, https://doi.org/10.1016/j.ypmed.2019.105776.
Zhang, D., Bauer, C., Powell-Wiley, T., & Xiao, Q. (2021). Association of Long-Term Trajectories of Neighborhood Socioeconomic Status with Weight Change in older adults. JAMA Network Open, 4(2), e2036809. https://doi.org/10.1001/jamanetworkopen.2020.36809.
Zorbaugh, H. (1929). The Gold Coast and the Slum. Chicago, IL: The University of Chicago Press.
Funding
Sage Kim was supported by NIMHD (R01MD014839); Lisa Tussing-Humphrys was supported by NIMHD (U54MD012523; Marian Fitzgibbon was supported by NHLBI (R01HL129153); Caryn Peterson was supported by NCI (U54CA202995; U54CA202997).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest/Competing interests
None.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kim, S.J., Blesoff, J.R., Tussing-Humphrys, L. et al. The association between neighborhood conditions and weight loss among older adults living in a large urban city. J Behav Med 46, 882–889 (2023). https://doi.org/10.1007/s10865-023-00410-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10865-023-00410-0