
Abstract
Purpose
Systemic inflammation has been associated with corrected QT (QTc) interval prolongation. The role of inflammation on QTc prolongation in COVID-19 patients was investigated.
Methods
Patients with a laboratory-confirmed SARS-CoV-2 infection admitted to IRCCS San Raffaele Scientific Institute (Milan, Italy) between March 14, 2020, and March 30, 2020 were included. QTc-I was defined as the QTc interval by Bazett formula in the first ECG performed during the hospitalization, before any new drug treatment; QTc-II was the QTc in the ECG performed after the initiation of hydroxychloroquine drug treatment.
Results
QTc-I was long in 45 patients (45%) and normal in 55 patients (55%). Patients with long QTc-I were older and more frequently males. C-Reactive protein (CRP) and white blood cell (WBC) count at hospitalization were higher in patients with long QTc-I and long QTc-II. QTc-I was significantly correlated with CRP levels at hospitalization. After a median follow-up of 83 days, 14 patients (14%) died. There were no deaths attributed to ventricular arrhythmias. Patients with long QTc-I and long QTc-II had a shorter survival, compared with normal QTc-I and QTc-II patients, respectively. In Cox multivariate analysis, independent predictors of mortality were age (HR = 1.1, CI 95% 1.04–1.18, p = 0.002) and CRP at ECG II (HR 1.1, CI 95% 1.0–1.1, p = 0.02).
Conclusions
QTc at hospitalization is a simple risk marker of mortality risk in COVID-19 patients and reflects the myocardial inflammatory status.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
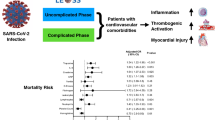
Since December 2019, the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was associated with coronavirus disease 2019 (COVID-19) [1,2,3,4]. The clinical spectrum of COVID-19 is wide, encompassing asymptomatic infection, mild upper respiratory tract illness, and acute respiratory distress syndrome, with a high mortality rate [5,6,7]. Despite multiple advanced critical care interventions, acute respiratory distress syndrome in COVID-19 patients is still associated with prolonged ventilation and high short-term mortality [8]. Small case series reported cardiac arrhythmias, cardiomyopathy, and cardiac arrest as terminal events in patients with COVID-19 [9,10,11,12,13].
Arrhythmias in COVID-19 patients are related to multiple factors including myocardial injury, systemic and local inflammation, QTc-prolonging drugs, and electrolytic imbalances [14]. QTc prolongation plays a major role in ventricular arrhythmias (VAs) in the setting of acute infection. According to the “multi-hit theory,” systemic inflammation itself significantly prolongs QTc interval, thus contributing to increase the risk of cardiac arrest [15]. The risk of QTc prolongation in COVID-19 has been reported to be higher in patients treated with the anti-malarian agent hydroxychloroquine, even if the correlation of this event with arrhythmias and in general cardiovascular adverse events is unclear [16]. The purpose of the present study was to evaluate the effects of inflammation and hydroxychloroquine on QTc interval in COVID-19 patients and to correlate these findings with the clinical outcome.
2 Methods
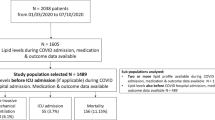
This is a single-center, retrospective study including 100 consecutive patients with a laboratory-confirmed COVID-19, admitted to the Emergency Rooms (ER) of the San Raffaele University Hospital (Milan, Italy) between March 14 and March 30, 2020.
2.1 Data collection
Upon presentation, a nasopharyngeal swab (COPAN Diagnostic, Inc., Murrieta, CA) was obtained in each patient to test for SARS-CoV-2 and processed in a local laboratory with RT-PCR assay. Hs-Troponin T (cTn-T) was obtained with Elecsys® Troponin T-high sensitive assay, at admission (cTn-T-adm) and peak (cTn-T-peak) in all patients, and a cutoff of 15 ng/mL was used based on the upper 99th percentile. Clinical and laboratory data were retrospectively collected on a shared electronic medical record. Deaths were collected on a daily basis, and causes of death were recorded. Clinical data were extracted from the electronic medical records and merged with the ECG data; data were carefully reviewed and confirmed by two independent researchers to guarantee the accuracy of the data extraction (EC and VDP). The primary endpoint of the study was death for any cause. Atrial and ventricular arrhythmia data were collected. The study complied with the Declaration of Helsinki; the Ethic Committee approved the study [17].
2.2 12-Lead ECG
Standard resting 12-lead ECG was obtained in all patients using a MAC 5500 digital ECG recorder (GE Medical Systems, Milwaukee, Wisconsin). Two ECGs were obtained: ECG I performed at admission, before any new drug treatment; ECG II performed after initiation of hydroxychloroquine (HCQ) drug treatment during the hospitalization. All patients were treated with HCQ.
The following ECG parameters were calculated: RR interval (ms), QT interval, QTc interval with the Bazett formula in DII, and in V2 leads in ECG I and ECG II. All ECGs were analyzed using digital calipers by two groups of two independent physicians (LP and GF, SA, and LC), each group analyzing one-half of ECGs. The mean of the two independent measured values was used for analysis. If the difference between the two measured values was more than 20 ms, a third experienced electrophysiologist (PV) measured QTc. QTc-I was defined as the QTc interval in the ECG I; QTc-II was defined as the QTc in the ECG II. QTc intervals were classified as long when at least one among QTc in lead DII or in lead V2 was longer than 440 ms for men and 460 ms for women; when these criteria were not met, QTc intervals were considered normal. ∆QTc was defined as the difference between QTc-II and QTc-I in lead DII.
2.3 Statistical methods
Descriptive statistics were expressed in terms of median and interquartile range (IQR) for continuous variables, while frequency distribution and percentage were reported for categorical variables. All variables were tested for normality with Shapiro–Wilk test. Since normality distribution assumption in the whole population sample was not met, Mann–Whitney test or Fisher’s exact test was applied to compare patient groups, respectively in presence of continuous or categorical variables. QTc-I and QTc-II were compared with Wilcoxon signed-rank test. Correlation analysis was performed with Pearson correlation test and coefficient. Kaplan–Meier’s curves were drawn to describe the patients’ freedom from death during the follow-up period. The covariates entered in the multivariable Cox’s proportional hazard model were chosen according to their clinical significance and to whether the variable showed as statistically significant at univariate analysis. The following covariates were entered in the model: age, C-reactive protein (CRP) at ECG II, and dichotomized QTc-I. Significant variables were then selected through a stepwise backward approach. The alpha level was set at the conventional 0.05 level. Analyses were performed using the R statistical software version 3.6.3 (R Foundation for Statistical Computing, Vienna, Austria).
3 Results
3.1 Patients’ characteristics
One hundred consecutive patients with confirmed SARS-CoV-2 infection, admitted to the ER of San Raffaele Hospital, were included in the study. Median age at presentation was 65.0 years (IQR: 58.8–76.0); 74 (74.0%) were males. All patients were taking HCQ and 47 patients (47%) also azithromycin.
QTc-I was long in 45 patients (45%) and normal in 55 patients (55%). Patients with long QTc-I were older and more frequently males. C-Reactive protein (CRP) and white blood cell (WBC) count at hospitalization were higher in patients with long QTc-I (102.6 mg/L (66.9–172.1 mg/dL) and 7.9 × 109/L (5.3–11.5)), than in patients presenting with normal QTc-I (57.2 mg/L (33.4–139.2 mg/dL), p = 0.029; and 6.0 × 109/L (4.5–8.5), p = 0.05). QTc-II was recorded after a median of 5 days (IQR 3–7 days) of treatment. During hospitalization, QTc interval in lead DII increased from 435 ms (IQR 413–453) to 446 ms (IQR 417–469) (p = 0.007 for comparison QTc-I vs QTc-II); median ∆QTc was 17.5 ms (IQR 10–36). QTc also increased in lead V2 (QTc-I in lead V2: 435.5 ms (IQR 413–462), QTc-II in lead V2: 443 ms (IQR 422–470), p = 0.002). Complete patients’ characteristics based on dichotomized QTc-I are summarized in Table 1; patients’ characteristics based on dichotomized QTc-II are summarized in Table 2.
3.2 Inflammation and QTc in COVID-19
QTc-I in V2 lead showed a significant correlation with CRP determined at the first ECG (rho = 0.19, Pearson p = 0.05; Fig. 1, panel A). ∆QTc showed a significant correlation with CRP determined at the second ECG (rho = 0.22, Pearson p = 0.02; Fig. 1, panel B). There was no significant correlation between QTc-I and WBC, and between ∆QTc and WBC. The cTn-T-peak showed a significant correlation with CRP determined at the first ECG (rho = 0.26, Pearson p = 0.03) and CRP determined at the second ECG (rho = 0.24, Pearson p = 0.05); cTn-T-adm showed no correlation with CRP. QTc-I in V2 lead was long in 25 patients (50.0%) with elevated cTn-T-adm and in 21 patients (42.9%) with non-elevated cTn-T-adm (p = 0.79). Twenty-seven patients (52.9%) with elevated cTn-T-peak and 15 patients (32.3%) with non-elevated cTn-T-peak had long QTc-I in V2 lead (p = 0.13).

Panel A Correlation between QTc V2 in ECG I and CRP at ECG I. Panel B Correlation between ∆QTc and CRP at ECG II
3.3 Primary endpoint
During a median follow-up of 83.0 days (20.5–117.5), 14 patients (14%) died. Causes of death were end-stage respiratory failure in 11 patients (78%), septic shock in 2 patients (14%), and hemorrhagic shock in 1 patient (7%); all events occurred during hospitalization. There were no deaths due to ventricular arrhythmias. Twelve patients (12%) experienced de novo atrial fibrillation. Intensive care unit admission was necessary in 14 patients (14%), in 7 patients (15.6%) with long QTc-I, and in 7 patients (12.7%) with normal QTc-I.
Patients with long QTc-I had a shorter survival, compared with normal QTc-I patients (75.6% vs 94.5%, log-rank p = 0.01; Fig. 2, panel A). Long QTc-II patients had a shorter survival, compared with normal QTc-II patients (79.6% vs 93.5%, log-rank p = 0.047; Fig. 2, panel B).

Panel A Kaplan–Meier curve for dichotomized QTc-I. Panel B Kaplan–Meier curve for dichotomized QTc-II
In Cox univariate analysis, significant predictors of mortality were age (HR 1.10, CI 95% 1.04–1.17, p = 0.001), long QTc-I (HR 4.59, CI 95% 1.28–16.44, p = 0.019), CRP at ECG II (HR 1.01, CI 95% 1.00–1.01, p = 0.007), and cTn-T-peak (HR 1.02, CI 95% 1.01–1.03, p = 0.005). In Cox multivariate analysis, the independent predictors of mortality were age (HR = 1.1, CI 95% 1.04–1.18, p = 0.002) and CRP at ECG II (HR 1.1, CI 95% 1.0–1.1, p = 0.02).
4 Discussion
4.1 Main findings
Our study is the first to demonstrate a correlation between inflammation and QTc in COVID-19 patients. Inflammation, as expressed by CRP levels, appeared to be an independent risk factor for mortality; QTc can be used as a simple cardiac risk marker in patients with COVID-19.
4.2 Arrhythmogenesis in COVID-19 infection
SARS-CoV-2 replication causes direct cellular damage in target tissues, including lung epithelial cells, enterocytes of the small intestine, endothelial cells, and arterial smooth muscle cells; dying cells release inflammatory alarmins. Alveolar endothelial damage can progress into a microvascular lung vessels obstructive thrombo-inflammatory syndrome and hesitate in atypical ARDS [18].
Arrhythmias in COVID-19 patients are the result of the interplay between myocardial injury and prolonged QTc secondary to inflammation or drugs [19]. Cardiac injury, as demonstrated by troponin elevation, is associated with a higher incidence of ventricular arrhythmias [20]. The mechanisms of myocardial injury in patients with COVID-19 are not clearly understood, yet. Direct damage to the cardiomyocytes, systemic inflammation, myocardial interstitial fibrosis, interferon-mediated immune response, and exaggerated cytokine response, in addition to coronary plaque destabilization, myocarditis, and hypoxia might all be involved [21]. In a study by Chen et al. [22], levels of NT-proBNP, troponin-I, and CRP, i.e., markers of myocardial injury and inflammation, were significantly correlated with disease severity and critical illness. However, despite a high frequency of arrhythmias, mostly atrial fibrillation [23], only half of patients in intensive care units had acute cardiac injury; this evidence stimulated the search for other risk factors in COVID-19 patients’ arrhythmogenesis [20]. QTc prolongation secondary to inflammation and drug treatments is an attractive additional candidate.
Our study is the first to demonstrate a correlation between inflammation and QTc in COVID-19 population. Inflammation, as reflected by CRP levels, is a predictor of mortality in COVID-19 patients: in a machine learning model, hs-CRP with a cutoff of 41.2 mg/L was a key node in the classification tree [24]. A significant relationship between systemic inflammation, QTc prolongation, and TdP occurrence during the active phase of infections was demonstrated in non-COVID-19 patients [15]. They showed that inflammation causes QTc prolongation secondary to increased expression of K + channel gene KCNJ2. In their study, the mean QTc interval was 461 ms, that is higher than our findings of 435 ms; the longer QTc interval was probably related to the older age [25] of their study population. The frequency of prolonged QTc interval was more than 3 times higher than the control group, and the QTc duration correlated with CRP levels and inflammatory marker levels. In our cohort, there was a significant correlation between CRP and QTc-I at ECG I, but not with QTc-II; CRP was reduced at ECG II, while QTc-II was prolonged. Therefore, QTc-II prolongation was related not only to the extent of systemic inflammation, but also to the drug treatment.
Some drugs used in COVID-19 infection are known to cause QTc prolongation; this is the case of HCQ and azithromycin [19]. In our cohort, in which all patients were taking HCQ and 47 patients (47%) azithromycin, no arrhythmic deaths were observed, suggesting a relatively safe arrhythmic profile of HCQ in COVID-19 patients. This is consistent with the results from a randomized controlled clinical trial that did not observe ventricular tachycardias in 438 HCQ recipients [26]. In a recent systematic review including 1515 patients with COVID-19, ventricular arrhythmias occurred in only 2 patients within a subgroup of 28 patients treated with high-dose chloroquine [27]. This could be explained by the fact that QTc prolongation is modest, as also reported in the prospective observational study by Priori et al. [16]; in their experience, median QTc prolongation was 18 ms, similar to our finding of 17.5 ms, and no life-threatening arrhythmic events were reported. Furthermore, malignant ventricular arrhythmias in these patients represent a minority of cardiovascular deaths, and they are frequently associated with severe metabolic derangement [28].
4.3 Clinical role of QTc in COVID-19 infection
In our study, patients with long QTc-I or QTc-II had a higher mortality than patients with normal QTc. At univariate analysis, long QTc-I was a significant predictor of death. At multivariate analysis, age and CRP at ECG II were significant predictors of death. Age and inflammation status thus appeared as the main determinants of mortality, while QTc is a marker of cardiac involvement in high-risk patients. Age has been already identified as a major risk factor for mortality in COVID-19 patients in several studies, with age ≥ 65 years associated with a twofold increased risk of death [29], and a 20-fold-increased risk of mortality in patients aged ≥ 80 years, compared with those aged 50–59 [30].
cTn-T is another known risk factor for mortality in COVID-19 patients [11, 12]. We did not find any significant correlation between cTn-T-adm, cTn-T-peak, and QTc-I in V2; also, 32.3% patients with non-elevated cTn-T-peak had long QTc-I; these observations might hint QT prolongation as the expression of a cardiac involvement that goes beyond overt necrosis. Only cTn-T-peak, but not cTn-T-adm, was a significant predictor of mortality, thus suggesting that QTc-I at clinical presentation might provide prognostic information earlier than cTn-T. Our results are in agreement with Farrè et al. who demonstrated that a prolonged QTc was independently associated with a higher mortality in COVID-19 patients [31].
Our data point towards QTc at clinical presentation as a simple and easily available marker of initial myocardial disease that identifies patients at higher risk of death.
4.4 Strengths and limitations
This study was a retrospective single-center study from a university hospital in Lombardy region, one of Italian areas hit harder by the COVID-19 outbreak. The main limitation of this study is the limited number of patients included. However, statistically significant differences from these preliminary data add robustness to our hypothesis-generating observations.
5 Conclusions
QTc at clinical presentation (QTc-I) is a simple cardiac risk marker in COVID-19 patients. Its use in clinical practice needs a more extensive validation for triaging patients at higher risk of death.
Data availability
Data is available on request to the corresponding author.
Abbreviations
- COVID-19:
-
Coronavirus disease 2019
- CRP:
-
C-Reactive protein
- SARS-CoV-2:
-
Severe acute respiratory syndrome coronavirus 2
- WBS:
-
White blood cells
References
WHO. Novel coronavirus – China. 2020. http://www.who.int/csr/don/12-january-2020-novel-coronavirus-china/en/. Accessed 1 June 2021.
WHO. Director-General’s opening remarks at the media briefing on Covid-19: 11 March 2020. https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-COVID-19---11-march-2020. Accessed 1 June 2021.
Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, Zhao X, Huang B, Shi W, Lu R, Niu P, Zhan F, Ma X, Wang D, Xu W, Wu G, Gao GF, Tan W, Investigating China Novel Coronavirus, and Team Research. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;382(8):727–33.
Gramegna M, Baldetti L, Beneduce A, Pannone L, Falasconi G, Calvo F, Pazzanese V, Sacchi S, Pagnesi M, Moroni F, Ajello S, Melisurgo G, Agricola E, Camici PG, Scandroglio AM, Landoni G, Ciceri F, Zangrillo A, Cappelletti AM. St-segment-elevation myocardial infarction during Covid-19 pandemic: insights from a regional public service healthcare hub. Circ Cardiovasc Interv. 2020;13(8):e009413.
Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, Liu L, Shan H, Lei CL, Hui DSC, Du B, Li LJ, Zeng G, Yuen KY, Chen RC, Tang CL, Wang T, Chen PY, Xiang J, Li SY, Wang JL, Liang ZJ, Peng YX, Wei L, Liu Y, Hu YH, Peng P, Wang JM, Liu JY, Chen Z, Li G, Zheng ZJ, Qiu SQ, Luo J, Ye CJ, Zhu SY, Zhong NS, Covid China Medical Treatment Expert Group for. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382(18):1708–20.
Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, Wang B, Xiang H, Cheng Z, Xiong Y, Zhao Y, Li Y, Wang X, Peng Z. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323(11):1061–9.
Ciceri F, Castagna A, Rovere-Querini P, De Cobelli F, Ruggeri A, Galli L, Conte C, De Lorenzo R, Poli A, Ambrosio A, Signorelli C, Bossi E, Fazio M, Tresoldi C, Colombo S, Monti G, Fominskiy E, Franchini S, Spessot M, Martinenghi C, Carlucci M, Beretta L, Scandroglio AM, Clementi M, Locatelli M, Tresoldi M, Scarpellini P, Martino G, Bosi E, Dagna L, Lazzarin A, Landoni G, Zangrillo A. Early predictors of clinical outcomes of Covid-19 outbreak in Milan, Italy. Clin Immunol. 2020;217:108509.
Zangrillo A, Beretta L, Scandroglio AM, Monti G, Fominskiy E, Colombo S, Morselli F, Belletti A, Silvani P, Crivellari M, Monaco F, Azzolini ML, Reineke R, Nardelli P, Sartorelli M, Votta CD, Ruggeri A, Ciceri F, De Cobelli F, Tresoldi M, Dagna L, Rovere-Querini P, SerpaNeto A, Bellomo R, Landoni G, C. OVID-BioB Study Group. Characteristics, treatment, outcomes and cause of death of invasively ventilated patients with Covid-19 ARDS in Milan, Italy. Crit Care Resusc. 2020;22(3):200–11.
Ruan Q, Yang K, Wang W, Jiang L, Song J. Clinical predictors of mortality due to Covid-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020;46(5):846–8.
Baldi E, Sechi GM, Mare C, Canevari F, Brancaglione A, Primi R, Klersy C, Palo A, Contri E, Ronchi V, Beretta G, Reali F, Parogni P, Facchin F, Bua D, Rizzi U, Bussi D, Ruggeri S, OltronaVisconti L, Savastano S, CARe Researchers Lombardia. Out-of-hospital cardiac arrest during the Covid-19 outbreak in Italy. N Engl J Med. 2020;383(5):496–8.
Shi S, Qin M, Shen B, Cai Y, Liu T, Yang F, Gong W, Liu X, Liang J, Zhao Q, Huang H, Yang B, Huang C. Association of cardiac injury with mortality in hospitalized patients with Covid-19 in Wuhan, China. JAMA Cardiol. 2020;5(7):802–10.
Guo T, Fan Y, Chen M, Wu X, Zhang L, He T, Wang H, Wan J, Wang X, Lu Z. Cardiovascular implications of fatal outcomes of patients with Coronavirus disease 2019 (Covid-19). JAMA Cardiol. 2020;5(7):811–8.
Arentz M, Yim E, Klaff L, Lokhandwala S, Riedo FX, Chong M, Lee M. Characteristics and outcomes of 21 critically ill patients with Covid-19 in Washington State. JAMA. 2020;323(16):1612–4.
Merad M, Martin JC. Pathological inflammation in patients with Covid-19: a key role for monocytes and macrophages. Nat Rev Immunol. 2020;20(6):355–62.
Lazzerini PE, Acampa M, Laghi-Pasini F, Bertolozzi I, Finizola F, Vanni F, Natale M, Bisogno S, Cevenini G, Cartocci A, Giabbani B, Migliacci N, D’Errico A, Dokollari A, Maccherini M, Boutjdir M, Capecchi PL. Cardiac arrest risk during acute infections: systemic inflammation directly prolongs QTc interval via cytokine-mediated effects on potassium channel expression. Circ Arrhythm Electrophysiol. 2020;13(8):e008627.
Mazzanti A, Briani M, Kukavica D, Bulian F, Marelli S, Trancuccio A, Monteforte N, Manciulli T, Morini M, Carlucci A, Viggiani G, Cannata F, Negri S, Bloise R, Memmi M, Gambelli P, Carbone A, Molteni M, Bianchini R, Salgarello R, Sozzi S, De Cata P, Fanfulla F, Ceriana P, Locatelli C, Napolitano C, Chiovato L, Tomasi L, Stefanini GG, Condorelli G, Priori SG. Association of hydroxychloroquine with QTc interval in patients with COVID-19. Circulation. 2020;142(5):513–5. https://doi.org/10.1161/CIRCULATIONAHA.120.048476.
Rovere-Querini P, Tresoldi C, Conte C, Ruggeri A, Ghezzi S, De Lorenzo R, Di Filippo L, Farina N, Ramirez GA, Ripa M, Mancini N, Cantarelli E, Galli L, Poli A, De Cobelli F, Bonini C, Manfredi AA, Franchini S, Spessot M, Carlucci M, Dagna L, Scarpellini P, Ambrosio A, Di Napoli D, Bosi E, Tresoldi M, Lazzarin A, Landoni G, Martino G, Zangrillo A, Poli G, Castagna A, Vicenzi E, Clementi M, Ciceri F, COVID-BioB Study Group. Biobanking for COVID-19 research. Panminerva Med. 2020. https://doi.org/10.23736/s0031-0808.20.04168-3.
Ciceri F, Beretta L, Scandroglio AM, Colombo S, Landoni G, Ruggeri A, Peccatori J, D’Angelo A, De Cobelli F, Rovere-Querini P, Tresoldi M, Dagna L, Zangrillo A. Microvascular Covid-19 lung vessels obstructive thromboinflammatory syndrome (microclots): an atypical acute respiratory distress syndrome working hypothesis. Crit Care Resusc. 2020;22(2):95–7.
Lazzerini PE, Boutjdir M, Capecchi PL. Covid-19, arrhythmic risk, and inflammation: mind the gap! Circulation. 2020;142(1):7–9.
Driggin E, Madhavan MV, Bikdeli B, Chuich T, Laracy J, Biondi-Zoccai G, Brown TS, Der Nigoghossian C, Zidar DA, Haythe J, Brodie D, Beckman JA, Kirtane AJ, Stone GW, Krumholz HM, Parikh SA. Cardiovascular considerations for patients, health care workers, and health systems during the Covid-19 pandemic. J Am Coll Cardiol. 2020;75(18):2352–71.
Babapoor-Farrokhran S, Gill D, Walker J, Rasekhi RT, Bozorgnia B, Amanullah A. Myocardial injury and Covid-19: possible mechanisms. Life Sci. 2020;253:117723.
Chen C, Chen C, Yan JT, Zhou N, Zhao JP, Wang DW. Analysis of myocardial injury in patients with Covid-19 and association between concomitant cardiovascular diseases and severity of Covid-19. Zhonghua Xin Xue Guan Bing Za Zhi. 2020;48(7):567–71.
Iacopino S, Placentino F, Colella J, Pesce F, Pardeo A, Filannino P, Artale P, Desiro D, Sorrenti P, Campagna G, Fabiano G, Peluso G, Giacopelli D, Petretta A. New-onset cardiac arrhythmias during COVID-19 hospitalization. Circ Arrhythm Electrophysiol. 2020;13(11):e009040. https://doi.org/10.1161/CIRCEP.120.009040.
Yan Li, Zhang H-T, Goncalves J, Xiao Y, Wang M, Guo Y, Sun C, Tang X, Jing L, Zhang M, Huang X, Xiao Y, Cao H, Chen Y, Ren T, Wang F, Xiao Y, Huang S, Tan Xi, Huang N, Jiao Bo, Cheng C, Zhang Y, Luo A, Mombaerts L, Jin J, Cao Z, Li S, Hui Xu, Yuan Ye. An interpretable mortality prediction model for Covid-19 patients. Nat Mach Intell. 2020;2(5):283–8.
Rabkin SW, Cheng XJ, Thompson DJ. Detailed analysis of the impact of age on the QT interval. J Geriatr Cardiol. 2016;13(9):740–8.
Cavalcanti AB, Zampieri FG, Rosa RG, Azevedo LCP, Veiga VC, Avezum A, Damiani LP, Marcadenti A, Kawano-Dourado L, Lisboa T, Junqueira DLM, de Barros E Silva PGM, Tramujas L, Abreu-Silva EO, Laranjeira LN, Soares AT, Echenique LS, Pereira AJ, Freitas FGR, Gebara OCE, Dantas VCS, Furtado RHM, Milan EP, Golin NA, Cardoso FF, Maia IS, Hoffmann Filho CR, Kormann APM, Amazonas RB, Bocchi de Oliveira MF, Serpa-Neto A, Falavigna M, Lopes RD, Machado FR, Berwanger O; Coalition Covid-19 Brazil I Investigators. Hydroxychloroquine with or without azithromycin in mild-to-moderate Covid-19. N Engl J Med. 2020;383(21):2041–52. https://doi.org/10.1056/NEJMoa2019014.
Jankelson L, Karam G, Becker ML, Chinitz LA, Tsai MC. QT prolongation, torsades de pointes, and sudden death with short courses of chloroquine or hydroxychloroquine as used in Covid-19: a systematic review. Heart Rhythm. 2020;17(9):1472–9.
Turagam MK, Musikantow D, Goldman ME, Bassily-Marcus A, Chu E, Shivamurthy P, Lampert J, Kawamura I, Bokhari M, Whang W, Bier BA, Malick W, Hashemi H, Miller MA, Choudry S, Pumill C, Ruiz-Maya T, Hadley M, Giustino G, Koruth JS, Langan N, Sofi A, Dukkipati SR, Halperin JL, Fuster V, Kohli-Seth R, Reddy VY. Malignant arrhythmias in patients with COVID-19: incidence, mechanisms, and outcomes. Circ Arrhythm Electrophysiol. 2020;13(11):e008920. https://doi.org/10.1161/CIRCEP.120.008920.
Mehra MR, Desai SS, Kuy S, Henry TD, Patel AN. Cardiovascular disease, drug therapy, and mortality in Covid-19. N Engl J Med. 2020;382(25):e102.
Williamson EJ, Walker AJ, Bhaskaran K, Bacon S, Bates C, Morton CE, Curtis HJ, Mehrkar A, Evans D, Inglesby P, Cockburn J, McDonald HI, MacKenna B, Tomlinson L, Douglas IJ, Rentsch CT, Mathur R, Wong AYS, Grieve R, Harrison D, Forbes H, Schultze A, Croker R, Parry J, Hester F, Harper S, Perera R, Evans SJW, Smeeth L, Goldacre B. Factors associated with Covid-19-related death using Opensafely. Nature. 2020;584(7821):430–6.
Farré N, Mojón D, Llagostera M, Belarte-Tornero LC, Calvo-Fernández A, Vallés E, Negrete A, García-Guimaraes M, Bartolomé Y, Fernández C, García-Duran AB, Marrugat J, Vaquerizo B. Prolonged QT interval in SARS-CoV-2 infection: prevalence and prognosis. J Clin Med. 2020;9(9):2712. https://doi.org/10.3390/jcm9092712.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
The study complied with the Declaration of Helsinki; the Ethic Committee approved the study.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Simone Gulletta and Paolo Della Bella equally contributed to the study and are shared first authors.
Rights and permissions
About this article

Cite this article
Gulletta, S., Della Bella, P., Pannone, L. et al. QTc interval prolongation, inflammation, and mortality in patients with COVID-19. J Interv Card Electrophysiol 63, 441–448 (2022). https://doi.org/10.1007/s10840-021-01033-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-021-01033-8