
Abstract
Purpose
To evaluate how the integration of intracardiac echocardiography (ICE) and ultrasound-guided femoral venipuncture (USGVC) may affect the safety of catheter ablation (CA) of atrial fibrillation (AF).
Methods
From a single center 374 patients with AF underwent 3D electroanatomic mapping–guided CA with or without the integration of ICE and USGVC. The primary endpoints were periprocedural complications, fluoroscopy time, and procedure time between the two groups.
Results
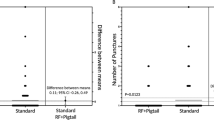
The median age of patients was 60 years. Sixteen patients had major complications (4.3%); 10 of these (2.7%) had major vascular complications. Thirty-seven patients had minor complications (9.9%) that did not require intervention. There were fewer major complications in the CA with the aid of ICE and USGVC than in the conventional approach (1% vs 7%, p = 0.004). The combined approach required less fluoroscopy time than the conventional procedure (median with ICE + USGVC 14 min (interquartile range (IQR) 8–21) vs median without ICE + USGVC 22 min (IQR 17–32)), p < 0.001, and less radiofrequency time (median with ICE + USGVC 1686 s (IQR 1367–1998) vs median time without ICE + USGVC: 1792 s (IQR 1390–2400)), p = 0.012. After adjustment for confounding factors, only the use of ICE + USGVC (hazard ratio: 0.139; p = 0.05) was a significantly protective factor against major complications.
Conclusion
The use of ICE and USGVC in CA of AF is associated with significantly fewer major complications and lower fluoroscopy and radiofrequency time, so these aids increased the safety of the procedure.


Similar content being viewed by others
References
Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, et al. 2016 ESC guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur J Cardiothorac Surg. 2016;50(5):e1–e88.
Mark DB, Anstrom KJ, Sheng S, Piccini JP, Baloch KN, Monahan KH, et al. Effect of catheter ablation vs medical therapy on quality of life among patients with atrial fibrillation: the CABANA randomized clinical trial. JAMA. 2019;321(13):1275–85.
Marrouche NF, Brachmann J, Andresen D, Siebels J, Boersma L, Jordaens L, et al. Catheter ablation for atrial fibrillation with heart failure. N Engl J Med. 2018;378(5):417–27.
Aldhoon B, Wichterle D, Peichl P, Čihák R, Kautzner J. Complications of catheter ablation for atrial fibrillation in a high-volume centre with the use of intracardiac echocardiography. Europace. 2013;15(1):24–32.
Arbelo E, Brugada J, Blomström-Lundqvist C, Laroche C, Kautzner J, Pokushalov E, et al. Contemporary management of patients undergoing atrial fibrillation ablation: in-hospital and 1-year follow-up findings from the ESC-EHRA atrial fibrillation ablation long-term registry. Eur Heart J. 2017;38(17):1303–16.
Sobolev M, Shiloh AL, Di Biase L, Slovut DP. Ultrasound-guided cannulation of the femoral vein in electrophysiological procedures: a systematic review and meta-analysis. Europace. 2017;19(5):850–5.
Yamagata K, Wichterle D, Roubícek T, Jarkovský P, Sato Y, Kogure T, et al. Ultrasound-guided versus conventional femoral venipuncture for catheter ablation of atrial fibrillation: a multicentre randomized efficacy and safety trial (ULTRA-FAST trial). Europace. 2018;20(7):1107–14.
Goya M, Frame D, Gache L, Ichishima Y, Tayar DO, Goldstein L, et al. The use of intracardiac echocardiography catheters in endocardial ablation of cardiac arrhythmia: meta-analysis of efficiency, effectiveness, and safety outcomes. J Cardiovasc Electrophysiol. 2020;31:664–73. https://doi.org/10.1111/jce.14367.
Rosu R, Cismaru G, Muresan L, Puiu M, Gusetu G, Istratoaie S, et al. Intracardiac echocardiography for transseptal puncture. A guide for cardiac electrophysiologists. Med Ultrason. 2019;21(2):183–90.
Lin D, Callans DJ. Use of intracardiac echocardiography during atrial fibrillation ablation to avoid complications. Futur Cardiol. 2015;11(6):683–7.
Cappato R, Calkins H, Chen SA, Davies W, Iesaka Y, Kalman J, et al. Updated worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circ Arrhythm Electrophysiol. 2010;3(1):32–8.
Andrade JG, Champagne J, Dubuc M, Deyell MW, Verma A, Macle L, Leong-Sit P, Novak P, Badra-Verdu M, Sapp J, Mangat I, Khoo C, Steinberg C, Bennett MT, Tang ASL, Khairy P and investigators, CIRCA-DOSE study. cryoballoon or radiofrequency ablation for atrial fibrillation assessed by continuous monitoring: a randomized clinical trial. Circulation, 2019; 140(22):1779–1788.
Manolis AS, Melita-Manolis H, Vassilikos V, Maounis T, Chiladakis J, Christopoulou-Cokkinou V, et al. Thrombogenicity of radiofrequency lesions: results with serial D-dimer determinations. J Am Coll Cardiol. 1996;28(5):1257–61.
Enriquez A, Saenz LC, Rosso R, Silvestry FE, Callans D, Marchlinski FE, et al. Use of intracardiac echocardiography in interventional cardiology: working with the anatomy rather than fighting it. Circulation. 2018;137(21):2278–94.
Cismaru G, Schiau S, Muresan L, Rosu R, Puiu M, Gusetu G, et al. Intravascular pulmonary venous ultrasound imaging for catheter ablation of atrial fibrillation. Expert Rev Med Devices. 2017;14(4):309–14.
Dello Russo A, Russo E, Fassini G, Casella M, Innocenti E, Zucchetti M, et al. Role of intracardiac echocardiography in atrial fibrillation ablation. J Atr Fibrillation. 2013;5(6):786.
Sharma PS, Padala SK, Gunda S, Koneru JN, Ellenbogen KA. Vascular complications during catheter ablation of cardiac arrhythmias: a comparison between vascular ultrasound guided access and conventional vascular access. J Cardiovasc Electrophysiol. 2016;27(10):1160–6.
Brooks AG, Wilson L, Chia NH, Lau DH, Alasady M, Leong DP, et al. Accuracy and clinical outcomes of CT image integration with Carto-sound compared to electro-anatomical mapping for atrial fibrillation ablation: a randomized controlled study. Int J Cardiol. 2013;168(3):2774–82.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The institutional review board approval was given under the condition that the patients’ data were collected in an aggregate and anonymized form.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
CONDENSED ABSTRACT
From a single center 374 patients with atrial fibrillation (AF) underwent radiofrequency catheter ablation (CA) with or without the integration of intracardiac echocardiography (ICE) and ultrasound-guided femoral venipuncture cannulation (USGVC). There were fewer major complications in the CA with the aid of ICE and USGVC than in the conventional approach (1% vs 7%, p = 0.004). The combined approach required less fluoroscopy (median with ICE + USGVC: 14 minutes vs median without ICE + USGVC: 22 minutes, p < 0.001), and radiofrequency (median with ICE + USGVC 1686 seconds vs median time without ICE + USGVC 1792 seconds, p = 0.012) time than the conventional procedure. The use of ICE and USGVC in CA of AF increased the safety of the procedure.
Rights and permissions
About this article

Cite this article
La Greca, C., Cirasa, A., Di Modica, D. et al. Advantages of the integration of ICE and 3D electroanatomical mapping and ultrasound-guided femoral venipuncture in catheter ablation of atrial fibrillation. J Interv Card Electrophysiol 61, 559–566 (2021). https://doi.org/10.1007/s10840-020-00835-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-020-00835-6