
Abstract
Purpose
In patients who undergo implantable cardiac defibrillator (ICD) implantation for primary prevention of sudden cardiac death (SCD), data is unclear whether their ICD generator needs to be replaced at end of life if their left ventricular ejection fraction (EF) improves. Despite improvement in EF, the underlying scar may represent a potential substrate for ventricular arrhythmias.
Methods
Data on 280 patients who underwent ICD implantation for primary prevention of SCD was obtained from two centers. Patients were followed for any improvement in EF to ≥35%. All arrhythmic events during follow-up, including appropriate and inappropriate shocks/ATP, were recorded.
Results
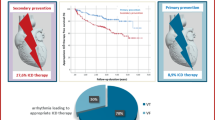
Thirty percent (n = 86/280) of patients improved their EF to >35% of which 41% (n = 37) underwent a generator change by the study ending period with the rest not yet at ERI. Mean baseline EF in patients with and without target EF improvement was 26 ± 7 and 23 ± 7% (p = 0.2). After excluding patients whose arrhythmic events data were unavailable, the final sample consisted of 62 patients in the EF improvement group and 156 patients in the group without EF improvement. In the group with EF improvement, appropriate events (shock + ATP) were noted in 19% of patients (n = 12/62) and inappropriate shocks and ATP in 6% of (n = 4/62) patients after their EF improved to >35%. Four patients received appropriate therapies when their EF was low prior to improvement. In contrast, in patients who had no improvement in EF, 27% (n = 43/156) received an appropriate therapy (p = 0.6) while 11% (n = 18/156) (p = 0.2) received inappropriate shocks and ATP. All-cause mortality was higher in patients without subsequent improvement in EF versus those with EF improvement (31 vs. 15% (p = .005).
Conclusions
There was no significant difference in the number of appropriate therapies received by each group. Patients continue to be at high risk for sudden cardiac death despite improvement in EF.

Similar content being viewed by others


Abbreviations
- SCD:
-
Sudden cardiac death
- ICD:
-
Implantable cardioverter defibrillator
- EF:
-
Ejection fraction
- CRTD:
-
Cardiac resynchronization therapy device
- ERI:
-
Elective replacement indicator
- EOL:
-
End of life
- ATP:
-
Anti-tachycardia pacing
References
Becker LB, Smith DW, Rhodes KV. Incidence of cardiac arrest: a neglected factor in evaluating survival rates. Ann Emerg Med. 1993;22:86–91.
Myerburg RJ, Castellanos A. Cardiac arrest and sudden death. In: Braunwald E, editor. Heart disease: a textbook of cardiovascular medicine. Philadelphia: WB Saunders; 1997. p. 742–79.
Antiarrhythmics versus Implantable Defibrillators (AVID) Investigators. A comparison of antiarrhythmic-drug therapy with implantable defibrillators in patients resuscitated from near-fatal ventricular arrhythmias. N Engl J Med. 1997;337:1576–83.
Wever EF, Hauer RN, van Capelle FL, Tijssen JG, Crijns HJ, Algra A, et al. Randomized study of implantable defibrillator as first-choice therapy versus conventional strategy in post-infarct sudden death survivors. Circulation. 1995;91:2195–203.
Moss AJ, Hall WJ, Cannom DS, Daubert JP, Higgins SL, Klein H, et al. Multicenter Automatic Defibrillator Implantation Trial Investigators. Improved survival with an implanted defibrillaton in patients with coronary disease at high risk for ventricular arrhythmia. N Engl J Med. 1996;335:1933–40.
Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346:877–83.
Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R, et al. Amiodarone or an implantable cardioverterdefibrillator for congestive heart failure. N Engl J Med. 2005;352:225–37.
Buxton AE, Lee KL, DiCarlo L, Gold MR, Greer GS, Prystowsky EN, et al. Electrophysiologic testing to identify patients with coronary artery disease who are at risk for sudden death. Multicenter Unsustained Tachycardia Trial Investigators. N Engl J Med. 2000;342(26):1937–45.
Epstein AE, Dimarco JP, Ellenbogen KA, Estes 3rd NA, Freedman RA, Gettes LS, et al. ACC/AHA/HRS 2008 Guidelines for device-based therapy of cardiac rhythm abnormalities. American College of Cardiology; American Heart Association Task Force on Practice Guidelines; American Association for Thoracic Surgery; Society of Thoracic Surgeons. Heart Rhythm. 2008;5(6):e1–62.
Metra M, Nodari S, Parrinello G, Giubbini R, Manca C, Dei CL. Marked improvement in left ventricular ejection fraction during long-term beta-blockade in patients with chronic heart failure: clinical correlates and prognostic significance. Am Heart J. 2003;145:292–9.
Cioffi G, Stefenelli C, Tarantini L, Opasich C. Prevalence, predictors, and prognostic implications of improvement in left ventricular systolic function and clinical status in patients >70 years of age with recently diagnosed systolic heart failure. Am J Cardiol. 2003;92:166–72.
Verma A, Wulffhart Z, Lakkireddy D, Khaykin Y, Kaplan A, Sarak B, et al. Natale A Incidence of left ventricular function improvement after primary prevention ICD implantation for non-ischaemic dilated cardiomyopathy: a multicenter experience. Heart. 2010;96(7):510–5.
Grimm W, Timmesfeld N, Efimova E. Left ventricular function improvement after prophylactic implantable cardioverter-defibrillator implantation in patients with non-ischaemic dilated cardiomyopathy. Europace. 2013;15(11):1594–600.
Poole JE, Gleva MJ, Mela T, Chung MK, Uslan DZ, Borge R, et al. Complication rates associated with pacemaker or implantable cardioverter-defibrillator generator replacements and upgrade procedures: results from the REPLACE registry. Circulation. 2010;122:1553–61.
Tarakji KG, Chan EJ, Cantillon DJ, Doonan AL, Hu T, Schmitt S, et al. Cardiac implantable electronic device infections: presentation, management, and patient outcomes. Heart Rhythm. 2010;7(8):1043–7.
Greenspon AJ, Patel JD, Lau E, Ochoa JA, Frisch DR, Ho RT, et al. 16-year trends in the infection burden for pacemakers and implantable cardioverter-defibrillators in the United States 1993 to 2008. JACC. 2011;58(10):1001–6.
Buxton AE, Lee KL, Hafley GE, Pires LA, Fisher JD, Gold MR, et al. Limitations of ejection fraction for prediction of sudden death risk in patients with coronary artery disease: lessons from the MUSTT study. J Am Coll Cardiol. 2007;50(12):1150–7.
Groh WJ. Lessons from a population. The limitations of left ventricular ejection fraction as the major determinant for primary prevention implantable cardioverter-defibrillators. J Am Coll Cardiol. 2006;47:1167–8. 16545647.
Stecker EC, Vickers C, Waltz J, Socoteanu C, John BT, Mariani R, et al. Population-based analysis of sudden cardiac death with and without left ventricular systolic dysfunction. Two-year findings from the Oregon Sudden Unexpected Death Study. J Am Coll Cardiol. 2006;47:1161–6.
de Vreede-Swagemakers JJ, Gorgels AP, Dubois-Arbouw WI, van Ree JW, Daemen MJ, Houben LG, et al. Out-of-hospital cardiac arrest in the 1990’s: a population-based study in the Maastricht area on incidence, characteristics and survival. J Am Coll Cardiol. 1997;30(6):1500–5.
Klem I, Weinsaft JW, Bahnson TD, Hegland D, Kim HW, Hayes B, et al. Assessment of myocardial scarring improves risk stratification in patients evaluated for cardiac defibrillator implantation. J Am Coll Cardiol. 2012;60(5):408–20.
Bello D, Fieno DS, Kim RJ, Pereles FS, Passman R, Song G, et al. Infarct morphology identifies patients with substrate for sustained ventricular tachycardia. J Am Coll Cardiol. 2005;45:1104–8.
Erkapic D, Sperzel J, Stiller S, Meltendorf U, Mermi J, Wegscheider K, et al. Long-term benefit of implantable cardioverter/defibrillator therapy after elective device replacement: results of the Incidence free Survival after ICD Replacement (INSURE) trial—a prospective multicenter study. Eur Heart J. 2013;34(2):130–7.
Naksuk N, Saab A, Li JM, Florea V, Akkaya M, Anand IS, et al. Incidence of appropriate shock in implantable cardioverter-defibrillator patients with improved ejection fraction. J Cardiac Fail. 2013;19:426–30.
Schliamser JE, Kadish AH, Subacius H, Shalaby A, Schaechter A, Levine J, et al. Significance of follow up left ventricular ejection fraction measurements in the defibrillators in non-ischemic cardiomyopathy treatment evaluation trial. Heart Rhythm. 2013;10:838–46.
Kini V, Soufi MK, Deo R, Epstein AE, Bala R, Riley M, et al. Appropriateness of primary prevention implantable cardioverter-defibrillators at the time of generator replacement: are indications still met? J Am Coll Cardiol. 2014;63(22):2388–94.
Acknowledgements
Part of the material in this manuscript is the result of work supported with resources and the use of facilities at the Robley Rex VA Medical Center in Louisville, KY
Author contributions
Jayasree Pillarisetti—idea, concept, design, data analysis, manuscript preparation
Rakesh Gopinathannair—design, critical revision of article
Matthew J. Haney—data collection
Bassem Abazid - Data collection
Wasiq Rawasia—data collection
Madhu Yeruva Reddy—critical revision of article
Niveditha Adabala—data collection
Sudharani Bommana—database administration
Martin Emert—critical review of article
Dhanunjaya Lakkireddy—critical review of article, approval of article
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Pillarisetti, J., Gopinathannair, R., Haney, M.J. et al. Risk of ventricular tachyarrhythmias following improvement of left ventricular ejection fraction in patients with implantable cardiac defibrillators implanted for primary prevention of sudden cardiac death. J Interv Card Electrophysiol 48, 283–289 (2017). https://doi.org/10.1007/s10840-017-0222-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-017-0222-1