
Abstract
Background
Vascular complications are a known risk of catheter-based pulmonary vein antral isolation (PVAI). Procedure-related thromboembolic events necessitate full-dose anticoagulation, which worsens outcomes in the event of vascular access injury.
Objective
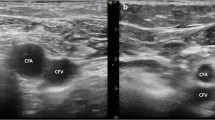
Real-time ultrasound allows direct visualization of vascular structures. We hypothesized that ultrasound use with venipuncture reduces vascular complications associated with PVAI.
Methods
Retrospective analysis of all adverse events occurring with PVAI was performed during two periods: 2005–2006 when ultrasound was not used and 2008–2010 when ultrasound was routinely employed. All patients received full-dose IV heparin during PVAI. In the no ultrasound cohort, only 14 % underwent PVAI without stopping warfarin, while 91 % of patients in the ultrasound cohort were on continued warfarin. Only patients deemed at high risk for thromboembolism with a periprocedural international normalized ratio (INR) less than 2 were bridged with subcutaneous low-molecular-weight heparin.
Results
Ultrasound reduced total vascular complications (1.7 vs. 0.5 %, p < 0.01) and decreased the incidence of major vascular complications by sevenfold. Warfarin with INR ≥ 1.2 on the day of PVAI was associated with more vascular complications (4.3 vs. 1.2 %, p < 0.01). Ultrasound guidance overcame the risk associated with warfarin therapy. Vascular complications in anticoagulated patients with INR ≥ 1.2 using ultrasound guidance were two- and ninefold lower than those in patients not using ultrasound with an INR < 1.2 (0.5 vs. 1.2 %, p < 0.05) and INR ≥ 1.2 (0.5 vs. 4.3 %, p < 0.01), respectively.
Conclusion
Ultrasound-guided venipuncture improves the safety profile of PVAI, reducing vascular complications in patients on warfarin to levels below those with no ultrasound and off warfarin.


Similar content being viewed by others

Abbreviations
- PVAI:
-
Pulmonary vein antral isolation
- AF:
-
Atrial fibrillation
- AV:
-
Arteriovenous
- F:
-
French
- mg/kg:
-
Milligram per kilogram
- mg:
-
Milligram
- s:
-
Seconds
- mm:
-
Millimeter
- INR:
-
International normalized ratio
- CT:
-
Computed tomography
- OR:
-
Odds ratio
- mg/dl:
-
Milligram per deciliter
- US:
-
Ultrasound
References
ACC/AHA/EHS. (2006). 2006 Guidelines for management of patients with atrial fibrillation. JACC Cardiovasc Interv, 48(4), e149–246.
Cappato, R., Calkins, H., Chen, S., et al. (2005). Worldwide survey on the methods, efficacy and safety of catheter ablation for human atrial fibrillation. Circulation, 111, 1100–1105.
Bertaglia, E., Zoppo, F., Tondo, C., et al. (2007). Early complications of pulmonary vein catheter ablation for atrial fibrillation: a multi-center prospective registry on procedural safety. Heart Rhythm, 4, 1265–1271.
Ortega, R., Song, M., Hansen, C., et al. (2010). Ultrasound-guided internal jugular vein cannulation. The New England Journal of Medicine, 362, e57.
Braner, D., Lai, S., Eman, S., et al. (2007). Central venous catheterization—subclavian vein. The New England Journal of Medicine, 357, e26.
Kanj, M., Wazni, O., & Natale, A. (2006). How to do circular mapping catheter-guided pulmonary vein antrum isolation: the Cleveland Clinic approach. Heart Rhythm, 3, 866–869.
Wazni, O., Beheiry, S., Fahmy, T., et al. (2007). Atrial fibrillation ablation in patients with therapeutic international normalized ratio. Circulation, 116, 2531–2534.
Ren, J., Marchlinski, F., Callans, D., et al. (2005). Increased intensity of anticoagulation may reduce risk of thrombus during atrial fibrillation ablation procedures in patients with spontaneous echo contrast. Journal of Cardiovascular Electrophysiology, 16, 474–477.
Hussein, A., Martin, D., Saliba, W., et al. (2009). Radiofrequency ablation of atrial fibrillation under therapeutic international normalized ratio: a safe and efficacious periprocedural anticoagulation strategy. Heart Rhythm, 6, 1425–1429.
Schmidt, M., Segerson, N., Marschang, H., et al. (2009). Atrial fibrillation ablation in patients with therapeutic international normalized ratios. Pacing Clin Electrophysiol, 32, 995–999.
Spragg, D., Dalal, D., Cheema, A., et al. (2008). Complications of catheter ablation for atrial fibrillation incidence and predictors. J Cardiovasc Electrophysiol, 19, 627–631.
Prudente, L., Moorman, R., Lake, D., et al. (2009). Femoral vascular complications following catheter ablation of atrial fibrillation. J Inter Card Electro, 26, 59–64.
Agency of Healthcare Research and Quality (2001). Making heath care safer: a critical analysis of patient safety practices. http://www.ahcpr.gov/clinic/ptsafety/chap21.htm
Hilty, W., Hudson, P., Levitt, M., et al. (1997). Real-time ultrasound-guided femoral vein catheterization during cardiopulmonary resuscitation. Annals of Emergency Medicine, 29, 331–336.
Seto, A., Abu-Fadel, M., Sparling, J., et al. (2010). Real-time ultrasound guidance facilitates femoral arterial access and reduces vascular complications: FAUST (Femoral Arterial Access with Ultrasound Trial). JACC Cardiovasc Interv, 7, 751–758.
Abhishek, F., Heist, E., Barrett, C., et al. (2011). Effectiveness of a strategy to reduce major vascular complications from catheter ablation of atrial fibrillation. Journal of Interventional Cardiac Electrophysiology, 30, 211–215.
Conflict of interest
Dr. Christine C. Tanaka-Esposito, Dr. Patrick J. Tchou, and Dr. Daniel J. Cantillon have received modest honorarium from Medtronic, Inc.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tanaka-Esposito, C.C., Chung, M.K., Abraham, J.M. et al. Real-time ultrasound guidance reduces total and major vascular complications in patients undergoing pulmonary vein antral isolation on therapeutic warfarin. J Interv Card Electrophysiol 37, 163–168 (2013). https://doi.org/10.1007/s10840-013-9796-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-013-9796-4