
Abstract
This pilot study examined associations between transdiagnostic symptoms and parent-perceived parent-child relationship quality in treatment-seeking families of children with neurodevelopmental disabilities, and interactions among clinical symptoms and cognitive functioning. Sixty-three children between 8 to 13 years of age and their caregivers were assessed at baseline while seeking cognitive behaviour therapy for emotion regulation and mental health difficulties. Diagnoses included autism, ADHD, cerebral palsy, and learning disability, with 52% of children having multiple diagnoses. Parent-perceived parent-child relationship quality was assessed by the Positive Affect Index, autism symptoms (e.g., social communication, repetitive behaviours) by the Social Responsiveness Scale, Second Edition, mental health (i.e., internalizing problems, externalizing problems, behavioural symptoms) by the Behaviour Assessment Scale for Children, Third Edition, and IQ by the Weschler Abbreviated Scale of Intelligence, Second Edition. Results revealed that higher IQ scores and greater social communication challenges, externalizing problems, and behavioural symptoms, were associated with lower parent-child relationship quality. Interaction effects were found between IQ and social communication challenges, reflecting significantly stronger relationships between social communication challenges and lower parent-child relationship quality in the context of higher IQ. Understanding the interactions between cognitive functioning and social communication challenges can help to inform individualized supports, and advocate for a transdiagnostic approach to intervention.
Highlights
-
We examined associations between transdiagnostic symptoms and parent-perceived parent-child relationship quality in families of children with neurodevelopmental disabilities.
-
Social communication challenges, IQ, externalizing problems, and behavioural symptoms were negatively associated with parent-child relationship quality.
-
The strength of the relationship between social communication challenges and parent-child relationship quality was inversely related to IQ levels.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Children and youth with neurodevelopmental disabilities (NDDs) exhibit marked difficulties with cognition, communication, behaviour and/or motor abilities (Mullin et al., 2013). These conditions have an onset during infancy or childhood, and are hypothesized to result from abnormal brain development (Bishop & Rutter, 2008). The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-V-TR; American Psychiatric Association, 2022) includes conditions such as autism spectrum disorder (ASD), attention-deficit/hyperactivity disorder (ADHD), and learning disabilities as examples of NDDs. Additionally, although cerebral palsy is primarily presented as a motor disorder in the DSM-V-TR, it has also been conceptualized as a NDD (Granlund et al., 2021). Along with these heterogeneous challenges, children with NDDs frequently present with mental health challenges such as behaviour problems, anxiety disorders, and/or depression (Hansen et al., 2018), including those with ADHD (Biederman et al., 1996), autism (Rosen et al., 2018; White et al., 2009), cerebral palsy (Goodman & Graham 1996; Rosenbaum et al., 2007), and learning disabilities (Beitchman & Young, 1997). The most common treatment for such challenges is cognitive behaviour therapy (CBT; England-Mason, 2020), which has been shown to produce positive outcomes for families of youth with autism (Weiss et al., 2018), ADHD (Antshel et al., 2012), and learning disabilities (Shechtman & Pastor, 2005). Parental involvement in their children’s treatment is a common underlying component of these CBT interventions, and given its importance (Sofronoff et al., 2005), it is critical to consider the parent-child relationship within this context. The parent-child relationship is defined as the bond between a caregiver and their child (Troll and Fingerman, 1996). Past work has shown that a component of the parent-child relationship (relational frustration) mediates the relationship between parental stress and child behaviour problems in children with developmental delays (Dennis et al., 2018). Other aspects of the parent-child relationship, such as emotional support, cohesiveness, and warmth, have also been negatively related to autistic children’s internalizing and externalizing problems (Orsmond et al., 2006; Smith et al., 2008). In children with learning disabilities, avoidant and anxious mother-child attachment relationships are associated with greater child internalizing and externalizing problems (Al-Yagon, 2010).
In addition to mental health challenges, children with NDDs often have social communication and cognitive difficulties (Antshel et al., 2012; Beckung & Hagberg, 2002; Carpenter et al., 2002; van der Meer et al., 2012). For instance, authors have suggested that autistic youth diagnosed with comorbid ADHD also have transdiagnostic cognitive and social challenges (Mikami et al., 2019). Studies have examined how the parent-child relationship may be associated with these transdiagnostic symptoms, though most have done so within the context of specific diagnostic groups (e.g., Beurkens et al., 2013; Barfoot et al., 2017; Climie & Mitchell, 2017; Orsmond et al., 2006; Smith et al., 2008). One study found that aspects of parenting (e.g., psychological control) were associated with more externalizing problems across groups of children with autism, Down syndrome, and cerebral palsy (De Clercq et al., 2019). Other parental factors such as parent stress and wellbeing have been shown to be linked with child symptoms, including adaptive behaviour and emotional and behavioural problems, in children with developmental disabilities (Baker et al., 2003; Hastings, 2003; Lewis et al., 2006; Saloviita et al., 2003; Weiss et al., 2003). The quality of the parent-child relationship is also negatively associated with the severity of social communication problems in children with autism (Beurkens et al., 2013), and positively associated with cognitive functioning across children with different neurological conditions (e.g., epilepsy; Leiser et al., 2017). Complicating matters is the fact that there can be interactions between clinical symptoms and cognitive functioning. For example, internalizing problems appear to be more common in autistic children with higher IQ scores compared to those with lower IQ scores (Sukhodolsky et al., 2008). A study of children with epilepsy found that children with lower IQ scores had the most behavioural and mental health problems (Buelow et al., 2003). Given the high rates of comorbidity across NDDs (Christensen et al., 2014), significant overlap among symptoms (Mikami et al., 2019), and the fact that interventions have been shown to support child socioemotional functioning across diagnoses (Haft et al., 2019; Webster-Stratton & Reid, 2008), it might be helpful to better understand how transdiagnostic symptoms are associated with the parent-child relationship across NDD diagnoses.
To our knowledge, no study has examined associations between transdiagnostic symptoms and parent-child relationship quality within the context of families seeking mental health treatment for children with various NDDs. Examining such associations is crucial because families of children with NDDs often struggle with negative parent-child dynamics (Climie & Mitchell, 2017; Plant & Sanders, 2007; Sealy & Glovinsky, 2016). The present study examined whether baseline clinical symptoms (i.e., mental health and social communication challenges) and cognitive functioning (i.e., IQ) are associated with parent-perceived parent-child relationship quality in children with varied NDDs, prior to their participation in a CBT intervention. As parent-child relationship quality has been linked to child outcomes generally (Beurkens et al., 2013; Leiser et al., 2017; Smith et al., 2008), exploring pre-intervention characteristics that may influence parent-child relationship quality in this diverse sample may aid in understanding the factors that promote successful interventions, and ultimately, the wellbeing of families of children with NDDs.
Method
Participants
The sample consisted of 63 children (79% boys) aged 8 to 13 years (M = 9.65, SD = 1.53), and their caregivers (86% mothers), aged 29 to 54 years (M = 43.60, SD = 5.66), who participated in a CBT intervention designed to improve children’s emotion regulation and mental health difficulties. Child diagnoses included autism (n = 52), ADHD (n = 37), learning disability (n = 14), and cerebral palsy (n = 2), with 52% of children having more than one diagnosis (Supplemental Fig. 1). Further parent and child characteristics are shown in Table 1. Children were required to have Full-Scale IQ-2 (FSIQ-2) scores of 79 or higher on the Vocabulary and Matrix Reasoning subscales of the Weschler Abbreviated Scale of Intelligence, Second Edition (WASI-II; Wechsler, 2011) to participate, which was administered by members of the research team. Additionally, children were required to have documented emotion regulation and mental health difficulties, as captured by the parent-report Anxiety Disorder Interview Schedule for DSM-IV: Parent Version (ADIS-P; Silverman & Albano, 1996) and/or the Behaviour Assessment System for Children, Third Edition (BASC-3; Reynolds & Kamphaus, 2015).
Measures
Parent-child relationship quality was assessed with the parent-report Positive Affect Index (PAI; Bengtson & Schrader, 1982), which assesses parents’ feelings towards their child and their perceptions of their child’s feelings towards them. Items are rated on a Likert scale, from 1 ‘not at all’ to 6 ‘extremely’, and higher scores indicate more positive parent-child relationship quality. Previous research has established the construct and discriminant validity and internal consistency of the PAI in the general population (Bengtson & Allen, 1993; Bengtson and Schrader, 1982) and in individuals with autism and Down syndrome (Greenberg et al., 2004; Orsmond et al., 2006). For the current sample, reliability ranged from acceptable (α = 0.78) to good (α = 0.85) for the individual subscales, and was good (α = 0.89) for the overall score.
Social communication challenges were assessed across the entire sample with the parent-report Social Responsiveness Scale, Second Edition (SRS-2; Constantino & Gruber, 2012). This measure has been used in samples of children with autism (Weiss et al., 2018), but also with children with other NDDs such as learning disability and cerebral palsy (Bölte et al., 2011; Campbell et al., 2021), to capture the range of possible social communication difficulties that occur across NDD diagnoses. Items are rated on a Likert scale from 1 ‘not true’ to 4 ‘almost always true’, and higher scores indicate higher levels of social communication challenges. In the present study, the Social Communication and Interaction (SCI) and Restricted Interests and Repetitive Behaviour (RRB) Index T-Scores were analyzed. The SRS-2 has demonstrated high internal consistency, interrater reliability, and validity in the general population and autism population (Barbosa et al., 2015; Bruni, 2014; Frazier et al., 2014). For the current sample, reliability was acceptable (α = 0.70) for the RRB subscale and excellent (α = 0.90) for the SCI subscale.
Mental health was assessed using the Internalizing Problems (i.e., anxiety, depression, somatization), Externalizing Problems (i.e., hyperactivity, aggression, conduct problems), and Behavioural Symptoms Index (i.e., attention problems, atypicality, withdrawal) Composite T-Scores from the parent-report Behaviour Assessment Scale for Children, Third Edition (BASC-3; Reynolds & Kamphaus, 2015). This measure assesses the behaviours and emotions of children and adolescents. Items are rated on a Likert scale from 1 ‘never’ to 4 ‘almost always’, with T-Scores above 70 reflecting clinically significant levels of mental health challenges. The BASC-3 contains strong psychometric properties, with acceptable reliability and moderate to high concurrent validity (Reynolds & Kamphaus, 2015; Zhou et al., 2020), and has been administered in a previous study with the same sample of children with NDDs (Tajik-Parvinchi et al., 2021).
Cognitive functioning was assessed using the Full-Scale IQ-2 (FSIQ-2) score on the Weschler Abbreviated Scale of Intelligence, Second Edition (WASI-II; Weschler, 2011), based on the two-subtest version using Vocabulary and Matrix Reasoning. The WASI-II has effectively measured the cognitive functioning of individuals with autism, intellectual disability, and ADHD (McCrimmon & Smith, 2013; Weiss et al., 2018). Children were categorized into low IQ (FSIQ-2 between 79 and 88; n = 10), average IQ (FSIQ-2 between 89 and 119; n = 42), and high IQ (FSIQ-2 > 119; n = 11) groups. The current sample’s mean and standard deviation (M = 104.14, SD = 15.28) were used to establish the low IQ (1 SD below mean), average IQ, and high IQ (1 SD above mean) groups.
Procedure
Participants were recruited from community advertisements, word of mouth, e-newsletters, and website postings in a large metropolitan center in Canada. Interested families completed a phone screening and online survey, which included the SRS-2, to assess eligibility for the study. Eligible participants attended an in-person appointment, where informed consent and assent were obtained, and researchers administered the WASI-II and collected demographic information (e.g., age, gender, family characteristics). Families then returned for a second visit within two weeks to complete other measures, including the PAI and BASC-3, prior to participating in the 10-week CBT intervention. The study was approved by the University Research Ethics Board.
Results
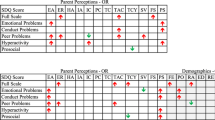
Analyses were conducted on baseline data. Bivariate correlations were computed among study variables to examine associations between total PAI scores and child characteristics. As shown in Table 2, there were significant negative associations between total PAI scores and IQ groups (rs = −0.38, p = 0.003), SCI challenges (rs = −0.41, p < 0.001), externalizing problems (rs = −0.37, p = 0.003), and behavioural symptoms (rs = −0.29, p = 0.02). Total PAI scores were not significantly associated with RRB (rs = −0.21, p = 0.10) or internalizing problems (rs = −0.15, p = 0.25).
Regressions were calculated to determine which child characteristics uniquely predicted total PAI scores, and potential interaction effects between clinical symptoms (i.e., SCI, RRB, internalizing problems, externalizing problems, behavioural symptoms) and cognitive functioning (i.e., IQ groups) were examined. As shown in Table 3, Model 1 with SCI challenges accounted for 35% adjusted variance in total PAI scores. SCI challenges did not account for a significant amount of unique variance (β = −0.009, p = 0.97), while IQ groups accounted for 15% unique variance (β = −0.43, p < 0.001). The interaction effect between SCI challenges and IQ groups accounted for 5.5% of additional unique variance in total PAI scores (β = −0.48, p = 0.03). As shown in Fig. 1, simple slopes analyses revealed that the low IQ group did not show a significant association between SCI challenges and total PAI scores (β = −0.18, p = 0.63). The average IQ group had SCI scores that accounted for 14% unique variance in total PAI scores (β = −0.40, p = 0.009). In the high IQ group, SCI challenges accounted for 62% unique variance in total PAI scores (β = −0.81, p = 0.002). All other regression models indicated only main effects of IQ, with no main effects for the clinical characteristics or the interaction terms.

Scatterplot of relations among parent-child relationship quality and social communication and interaction challenges within different IQ groups. Low IQ = FSIQ-2 between 79 and 88; Average IQ = FSIQ-2 between 89 and 119; High IQ = FSIQ-2 > 119
To investigate the influence of the autism-only group on the present study’s results, a sensitivity analysis was conducted with this subsample (n = 23). As shown in Supplemental Table 1, there were significant negative associations between SCI challenges and total PAI scores (rs = −0.48, p = 0.02). Total PAI scores were not significantly associated with IQ groups (rs = −0.10, p = 0.64), RRB (rs = −0.10, p = 0.65), internalizing problems (rs = −0.29, p = 0.17), externalizing problems (rs = −0.27, p = 0.21), and behavioural symptoms (rs = −0.32, p = 0.14). As shown in Supplemental Table 2, regression analyses revealed that IQ, clinical symptoms (i.e., SCI challenges, RRB, internalizing problems, externalizing problems, behavioural symptoms), or the interaction effects did not significantly predict total PAI scores across all the regressions.
Discussion
We examined associations between transdiagnostic child symptoms and parent-perceived parent-child relationship quality in families of children with various NDDs prior to participating in a CBT intervention for emotion regulation and mental health difficulties.
Parent-Child Relationship Quality and Mental Health Challenges
Children’s externalizing problems and behavioural symptoms were negatively associated with parent-child relationship quality, an association that was previously reported in other studies supporting transdiagnostic symptoms in children with autism, Down syndrome, and cerebral palsy (De Clercq et al., 2019). Externalizing problems reflect distress that is directed towards the environment, whereas internalizing problems reflect problems directed at oneself (Achenbach et al., 2016). Outward facing symptoms (e.g., aggression) may pose challenges to parenting and behaviour management (Woodman et al., 2015), which may in turn strain the parent-child relationship (Dennis et al., 2018). Though some studies have shown that internalizing problems are associated with the parent-child relationship (Smith et al., 2008), the present study did not find such links. It may be that inward facing symptoms of mental health problems (e.g., anxiety) may affect individuals themselves more than they impact others (Romero-Gonzalez et al., 2018). It is important to note the bidirectional nature of the relationship between children’s externalizing behaviours and behavioural problems in relation to parent-child relationship quality. It is possible that parent-child relationship difficulties may result in poorer child mental health outcomes, as supported by a study of children with NDDs (i.e., epilepsy), which found that lower mother-child interactional quality predicted greater child externalizing behaviour problems (Pianta & Lothman, 1994). Within the context of a negative parent-child relationship, parents may be unable to respond effectively to the needs of their children, eliciting children to exhibit more externalizing behaviours (e.g., aggression) and/or behavioural problems (e.g., hyperactivity) to engage the attention of their caregivers. Nonetheless, this link between children’s externalizing problems and behavioural symptoms and the parent-child relationship is unsurprising, considering literature which has demonstrated that participation in Parent-Child Interaction Therapy (PCIT; Eyberg et al., 1995) is associated with improvements in child behavioural problems (Al Sehli et al., 2021; Solomon et al., 2008). Related to mental health challenges, links have also been found between child temperament, which is a stable individual difference characteristic, rooted in a child’s biology and is influenced by the environment (Bates, 1989; Rothbart et al., 2000), and the parent-child relationship. For instance, relationships have been observed between child temperament and the parent-child relationship within the autism population (Kasari & Sigman, 1997), and between child impulsivity and maternal stress in the learning disability population (Barahmand et al., 2015).
Parent-Child Relationship Quality, IQ, and Social Communication Challenges
Social communication challenges were inversely linked with parent-child relationship quality, which echoes findings from previous studies of children with NDDs (Al-Yagon et al., 2020; Barfoot et al., 2017; Haven et al., 2013). Our measure of parent-child relationship quality was the PAI, which asks parents to rate the degree to which they express positive affect towards their children, and to which their children express positive affect towards them. Within the context of the present study, it may have been that communication difficulties were bidirectionally related to the expression and experience of positive emotions within the parent-child dyad. It would be misleading to focus solely on the bivariate relationship between social communication challenges and parent-child relationship quality, as interaction effects were found with IQ groups. In children with an estimated IQ over 119, social communication challenges had a greater negative impact on parent-child relationship quality. In children with IQ scores between 89 and 119, a weaker negative association was found, and in children with an IQ score of less than 89, social communication challenges did not have an impact on the parent-child relationship. Although previous studies have investigated interactions between social and cognitive functioning in the context of child anxiety symptoms (Sukhodolsky et al., 2008), the present study is the first to examine these interactions in relation to the parent-child relationship. It may be that parents have greater expectations for communication in children who have higher intellectual functioning (Clare et al., 1998) as they may have stronger verbal abilities. Moreover, the presence of social communication problems may impact children’s expression of positive affect towards their parents, which is how we operationalized the parent-child relationship in this study. Parents’ expectations of commensurate levels of social competence, coupled with the fact that social communication difficulties may impact children’s expression of positive affect, serves as a possible explanation for the stronger relationship between parent-child relationship quality and social communication difficulties in children with higher intellectual functioning. Alternatively, in children with a higher IQ, they may be more aware of their difficulties, particularly when social complexity and social demands rise during adolescence (Tantam, 2003). This may in turn contribute to the development of mental health challenges (Myles et al., 2003). As such, within children with higher intellectual functioning, increased social demands, an awareness of one’s disability, and resulting mental health challenges may bidirectionally impact parent-child dynamics.
Limitations
It is important to acknowledge limitations of these research findings. The sample size was small, consisted primarily of males with female caregivers, no children had intellectual disabilities, and most children had diagnoses of autism and ADHD. In particular, many participants had a diagnosis of autism (n = 52) in addition to other comorbidities, and as social communication difficulties are a core impairment within this population, this subsample of participants may have contributed to the variability observed in social difficulties in relation to parent-child relationship quality. Future research is needed including participants with diagnoses outside of autism. Given the distribution of IQ, we have a relatively small sample of individuals in the low and high IQ groups. Future work is needed to explore the interactions between social and cognitive functioning, particularly in children and youth with lower levels of cognitive functioning. Consistent with the social model of disability (Oliver, 1990; Barnes & Mercer, 2004), these individuals may face barriers to communication because environmental constraints may pose limits to their functional needs and abilities. As such, research is needed to explore these interactions when utilizing alternative communication strategies such as augmentative and alternative communication (Sigafoos et al., 2014), gestural communication (Mishra et al., 2021), and/or facial expressions (Dimitrovsky et al., 2000). Additionally, IQ assessments may not be a reliable indication of the cognitive functioning of children with NDDs, so future research should employ alternative methodologies to the WASI-II (e.g., non-verbal cognitive testing). Due to sample size limitations, potential unique associations within diagnostic groups could not be explored. For instance, DeClercq et al. (2022) found that parents of autistic children reported the most challenges concerning their relatedness with their child, while parents of children with cerebral palsy expressed the most worries about their child’s future. Additional work is needed to examine potential diagnostic differences in parent-child relationship quality in relation to transdiagnostic symptoms. Lastly, parent-child relationship quality was assessed using a brief, subjective parent-report scale, and measurement variance has not been established with an NDD sample for the measures utilized in the present study.
Clinical Implications
Within the context of therapy, it is critical to understand the clinical implications of adopting a transdiagnostic approach to treatment. Various studies have examined the benefits of supporting transdiagnostic symptoms, including programs such as the SCERTS Model (Prizant et al., 2006), which supports children’s social communication and emotional regulation, the Developmental, Individual Difference, Relationship-Based Model (DIRFloortime; Wieder 2013), which supports children’s social, emotional, and intellectual functioning, and Parent-Child Interaction Therapy (PCIT; Eyberg, 1988), which supports children’s behavioural and social functioning. These programs acknowledge the interdependencies between domains of development, rather than focusing on isolated skills and behaviours. Similarly, the present study’s findings suggest that practitioners may benefit from adopting a transdiagnostic approach to treatment for children with NDDs (Fusar-Poli et al., 2019), specifically targeting the interactions between social and cognitive functioning. Understanding transdiagnostic symptoms may inform the development of transdiagnostic evidence-based treatment approaches, such as the Modular Approach to Therapy for Children with Anxiety, Depression, Trauma, or Conduct Problems (MATCH-ADTC; Chorpita & Weisz, 2009). Nonetheless, it is also vital to continually acknowledge the importance of an individualized approach to treatment, as evidenced by the presence of a greater negative impact of social communication challenges on parent-child relationship quality in children with higher IQ. As parent-mediated interventions have been shown to be associated with increased generalization of skills across multiple contexts and the maintenance of treatment gains (Shalev et al., 2020), these nuanced differences are important to support to promote child and family wellbeing in this population.
References
Achenbach, T. M., Ivanova, M. Y., Rescorla, L. A., Turner, L. V., & Althoff, R. R. (2016). Internalizing/externalizing problems: Review and recommendations for clinical and research applications. Journal of the American Academy of Child & Adolescent Psychiatry, 55(8), 647–656. https://doi.org/10.1016/j.jaac.2016.05.012.
Al Sehli, S. A., Helou, M., & Sultan, M. A. (2021). The efficacy of parent-child interaction therapy (PCIT) in children with attention problems, hyperactivity, and impulsivity in Dubai. Case Reports in Psychiatry, 2021, 1–4. https://doi.org/10.1155/2021/5588612.
Al-Yagon, M.(2010). Maternal emotional resources and socio-emotional well-being of children with and without learning disabilities. Family Relations, 59(2), 152–169. https://doi.org/10.1111/j.1741-3729.2010.00592.x.
Al-Yagon, M., Forte, D., & Avrahami, L. (2020). Executive functions and attachment relationships in children with ADHD: Links to externalizing/internalizing problems, social skills, and negative mood regulation. Journal of Attention Disorders, 24(13), 1876–1890. https://doi.org/10.1177/1087054717730608.
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). https://doi.org/10.1176/appi.books.9780890425787.
Antshel, K. M., Faraone, S. V., & Gordon, M. (2012). Cognitive behavioral treatment outcomes in adolescent ADHD. FOCUS, 10(3), 334–345. https://doi.org/10.1176/appi.focus.10.3.334.
Barahmand, U., Piri, F., & Khazaee, A. (2015). A study of the relationship of academic achievement and impulsivity in children with specific learning disabilities to parenting strain and sense of competence in their mothers. Malaysian Journal of Health Sciences, 13, 7–14. https://doi.org/10.17576/jskm-2015-1301-02.
Baker, B. L., McIntyre, L. L., Blacher, J., Crnic, K., Edelbrock, C., & Low, C. (2003). Pre-school children with and without developmental delay: Behaviour problems and parenting stress over time. Journal of Intellectual Disability Research, 47(Pt 4-5), 217–230. https://doi.org/10.1046/j.1365-2788.2003.00484.x.
Barbosa, I. G., Rodrigues, D. H., Rocha, N. P., Simões-e-Silva, A. C., Teixeira, A. L., & Kummer, A. (2015). Psychometric properties of the Social Responsiveness Scale-2 (SRS-2) for autism spectrum disorder. Journal of Brasilian Psychiatry, 64(3), 230–237. https://doi.org/10.1590/0047-2085000000083.
Barfoot, J., Meredith, P., Ziviani, J., & Whittingham, K. (2017). Parent-child interactions and children with cerebral palsy: An exploratory study investigating emotional availability, functional ability, and parent distress. Child: Care, Health and Development, 43(6), 812–822. https://doi.org/10.1111/cch.12493.
Barnes, C. & Mercer, G. (2004). Theorising and researching disability from a social model perspective. In C. Barnes & G. Mercer (Eds.), Implementing the social model of disability: Theory and research (pp. 1–17). The Disability Press.
Bates, J. E. (1989). Concepts and measures of temperament. In G. A. Kohnstamm, J. E. Bates, & M. K. Rothbart (Eds.), Temperament in childhood (pp. 3–26). John Wiley & Sons.
Beckung, E., & Hagberg, G. (2002). Neuroimpairments, activity limitations, and participation restrictions in children with cerebral palsy. Developmental Medicine and Child Neurology, 44(5), 309–316. https://doi.org/10.1017/s0012162201002134.
Beitchman, J. H., & Young, A. R. (1997). Learning disorders with a special emphasis on reading disorders: A review of the past 10 years. Journal of the American Academy of Child & Adolescent Psychiatry, 36(8), 1020–1032. https://doi.org/10.1097/00004583-199708000-00009.
Bengtson, V. L., & Allen, K. R. (1993). The life course perspective applied to families over time. In P. Boss, W. Doherty, R. LaRossa, W. Schumm & S. Steinmetz (Eds.), Sourcebook of family theories and methods: A contextual approach (pp. 469–498). Plenum Press.
Bengtson, V. L., & Schrader, S. S. (1982). Parent-child relations. In D. J. Mangen & W. A. Peterson (Eds.), Research instruments in social gerontology: Social roles and social participation (Vol. 2, pp. 115–185). University of Minnesota Press.
Beurkens, N. M., Hobson, J. A., & Hobson, R. P. (2013). Autism severity and qualities of parent-child relations. Journal of Autism and Developmental Disorders, 43(1), 168–178. https://doi.org/10.1007/s10803-012-1562-4.
Biederman, J., Faraone, S., Milberger, S., Guite, J., Mick, E., Chen, L., Mennin, D., Marrs, A., Ouellette, C., Moore, P., Spencer, T., Norman, D., Wilens, T., Kraus, I., & Perrin, J. (1996). A prospective 4-year follow-up study of attention-deficit hyperactivity and related disorders. Archives of General Psychiatry, 53(5), 437–446. https://doi.org/10.1001/archpsyc.1996.01830050073012.
Bishop, D., & Rutter, M. (2008). Neurodevelopmental disorders: Conceptual issues. In M. Rutter, D. V. M. Bishop, D. S. Pine, S. Scott, J. Stevenson, E. Taylor, & A. Thappar (Eds.), Rutter’s child and adolescent psychiatry (pp. 32–41). https://doi.org/10.1002/9781444300895.ch3.
Bölte, S., Westerwald, E., Holtmann, M., Freitag, C., & Poustka, F. (2011). Autistic traits and autism spectrum disorders: The clinical validity of two measures presuming a continuum of social communication skills. Journal of Autism and Developmental Disorders, 41(1), 66–72. https://doi.org/10.1007/s10803-010-1024-9.
Bruni, T. P.(2014). Test review: Social Responsiveness Scale–Second Edition (SRS-2). Journal of Psychoeducational Assessment, 32(4), 365–369. https://doi.org/10.1177/0734282913517525.
Buelow, J. M., Austin, J. K., Perkins, S. M., Shen, J., Dunn, D. W., & Fastenau, P. S. (2003). Behavior and mental health problems in children with epilepsy and low IQ. Developmental Medicine & Child Neurology, 45(10), 683–692. https://doi.org/10.1017/S0012162203001270.
Campbell, H., Check, J., Kuban, K. C. K., Leviton, A., Joseph, R. M., Frazier, J. A., Douglass, L. M., Roell, K., Allred, E. N., Fordham, L. A., Hooper, S. R., Jara, H., Paneth, N., Mokrova, I., Ru, H., Santos, H. P., Fry, R. C., & O’Shea, T. M. (2021). Neonatal cranial ultrasound findings among infants born extremely preterm: Associations with neurodevelopmental outcomes at 10 years of age. The Journal of Pediatrics, 237, 197–205.e4. https://doi.org/10.1016/j.jpeds.2021.05.059.
Carpenter, M., Pennington, B. F., & Rogers, S. J. (2002). Interrelations among social-cognitive skills in young children with autism. Journal of Autism and Developmental Disorders, 32(2), 91–106. https://doi.org/10.1023/a:1014836521114.
Chorpita, B. F., & Weisz, J. R. (2009). MATCH-ADTC: Modular approach to therapy for children with anxiety, depression, trauma, or conduct problems. PracticeWise.
Christensen, D., Van Naarden Braun, K., Doernberg, N. S., Maenner, M. J., Arneson, C. L., Durkin, M. S., Benedict, R. E., Kirby, R. S., Wingate, M. S., Fitzgerald, R. & Yeargin-Allsopp, M. (2014). Prevalence of cerebral palsy, co-occurring autism spectrum disorders, and motor functioning–Autism and Developmental Disabilities Monitoring Network, USA, 2008. Developmental Medicine & Child Neurology, 56(1), 59–65. https://doi.org/10.1111/dmcn.12268.
Clare, L., Garnier, H. & Gallimore, R. (1998). Parents' developmental expectations and child characteristics: Longitudinal study of children with developmental delays and their families. American Journal on Mental Retardation, 103(2), 117–129. https://doi.org/10.1352/0895-8017(1998)1032.0.CO;2.
Climie, E. A., & Mitchell, K. (2017). Parent-child relationship and behavior problems in children with ADHD. International Journal of Developmental Disabilities, 63(1), 27–35. https://doi.org/10.1080/20473869.2015.1112498.
Constantino, J. N., & Gruber, C. P. (2012). Social Responsiveness Scale – Second Edition (SRS-2). Western Psychological Services.
De Clercq, L. E., Prinzie, P., Warreyn, P., Soenens, B., Dieleman, L. M., & De Pauw, S. (2022). Expressed emotion in families of children with and without autism spectrum disorder, cerebral palsy and Down syndrome: Relations with parenting stress and parenting behaviors. Journal of Autism and Developmental Disorders, 52(4), 1789–1806. https://doi.org/10.1007/s10803-021-05075-9.
De Clercq, L., Van der Kaap-Deeder, J., Dieleman, L. M., Soenens, B., Prinzie, P., & De Pauw, S. S. W. (2019). Parenting and psychosocial development in youth with and without autism spectrum disorder, cerebral palsy, and Down syndrome: A cross-disability comparison. Advances in Neurodevelopmental Disorders, 3(2), 220–234. https://doi.org/10.1007/s41252-019-00112-2.
Dennis, M. L., Neece, C. L., & Fenning, R. M. (2018). Investigating the influence of parenting stress on child behavior problems in children with developmental delay: The role of parent-child relational factors. Advances in Neurodevelopmental Disorders, 2(2), 129–141. https://doi.org/10.1007/s41252-017-0044-2.
Dimitrovsky, L., Spector, H., & Levy-Shiff, R. (2000). Stimulus gender and emotional difficulty level: Their effect on recognition of facial expressions of affect in children with and without LD. Journal of Learning Disabilities, 33(5), 410–416. https://doi.org/10.1177/002221940003300501.
England-Mason, G. (2020). Emotion regulation as a transdiagnostic feature in children with neurodevelopmental disorders. Current Developmental Disorders Reports, 7(3), 130–138. https://doi.org/10.1007/s40474-020-00200-2.
Eyberg, S. (1988). Parent-child interaction therapy. Integration of Traditional and Behavioral Concerns, 10(1), 33–46. https://doi.org/10.1300/J019v10n01_04.
Eyberg, S. M., Boggs, S. R., & Algina, J. (1995). Parent-child interaction therapy: A psychosocial model for the treatment of young children with conduct problem behavior and their families. Psychopharmacology Bulletin, 31(1), 83–91.
Frazier, T. W., Ratliff, K. R., Gruber, C., Zhang, Y., Law, P. A., & Constantino, J. N. (2014). Confirmatory factor analytic structure and measurement invariance of quantitative autistic traits measured by the Social Responsiveness Scale-2. Autism, 18(1), 31–44. https://doi.org/10.1177/1362361313500382.
Fusar-Poli, P., Solmi, M., Brondino, N., Davies, C., Chae, C., Politi, P., Borgwardt, S., Lawrie, S. M., Parnas, J., & McGuire, P. (2019). Transdiagnostic psychiatry: A systematic review. World Psychiatry, 18(2), 192–207. https://doi.org/10.1002/wps.20631.
Haft, S. L., Chen, T., LeBlanc, C., Tencza, F., & Hoeft, F. (2019). Impact of mentoring on socio-emotional and mental health outcomes of youth with learning disabilities and attention-deficit hyperactivity disorder. Child and Adolescent Mental Health, 24(4), 318–328. https://doi.org/10.1111/camh.12331.
Hastings, R. P. (2003). Child behaviour problems and partner mental health as correlates of stress in mothers and fathers of children with autism. Journal of Intellectual Disability Research, 47(Pt 4-5), 231–237. https://doi.org/10.1046/j.1365-2788.2003.00485.x.
Goodman, R., & Graham, P. (1996). Psychiatric problems in children with hemiplegia: cross sectional epidemiological survey. BMJ, 312(7038), 1065–1069. https://doi.org/10.1136/bmj.312.7038.1065.
Granlund, M., Imms, C., King, G., Andersson, A. K., Augustine, L., Brooks, R., Danielsson, H., Gothilander, J., Ivarsson, M., Lundqvist, L. O., Lygneg†rd, F. & Almqvist, L. (2021). Definitions and operationalization of mental health problems, wellbeing and participation constructs in children with NDD: Distinctions and clarifications. International Journal of Environmental Research and Public Health, 18(4), 1656–1656. https://doi.org/10.3390/ijerph18041656.
Greenberg, J. S., Seltzer, M. M., Krauss, M. W., Chou, R. J., & Hong, J. (2004). The effect of quality of the relationship between mothers and adult children with schizophrenia, autism, or Down syndrome on maternal well-being: The mediating role of optimism. The American Journal of Orthopsychiatry, 74(1), 14–25. https://doi.org/10.1037/0002-9432.74.1.14.
Hansen, B. H., Oerbeck, B., Skirbekk, B., Petrovski, B. É., & Kristensen, H. (2018). Neurodevelopmental disorders: Prevalence and comorbidity in children referred to mental health services. Nordic Journal of Psychiatry, 72(4), 285–291. https://doi.org/10.1080/08039488.2018.1444087.
Haven, E. L., Manangan, C. N., Sparrow, J. K., & Wilson, B. J. (2013). The relation of parent-child interaction qualities to social skills in children with and without autism spectrum disorders. Autism, 18(3), 292–300. https://doi.org/10.1177/1362361312470036.
Kasari, C., & Sigman, M. (1997). Linking parental perceptions to interactions in young children with autism. Journal of Autism and Developmental Disorders, 27(1), 39–57. https://doi.org/10.1023/A:1025869105208.
Leiser, K., Heffelfinger, A., & Kaugars, A. (2017). Associations among parent-child relationships and cognitive and language outcomes in a clinical sample of preschool children. The Clinical Neuropsychologist, 31(2), 423–437. https://doi.org/10.1080/13854046.2016.1268649.
Lewis, P., Abbeduto, L., Murphy, M., Richmond, E., Giles, N., Bruno, L., Schroeder, S., Anderson, J., & Orsmond, G. (2006). Psychological well-being of mothers of youth with fragile X syndrome: Syndrome specificity and within-syndrome variability. Journal of Intellectual Disability Research, 50(Pt 12), 894–904. https://doi.org/10.1111/j.1365-2788.2006.00907.x.
McCrimmon, A. W., & Smith, A. D. (2013). Review of the Wechsler Abbreviated Scale of Intelligence, Second Edition (WASI-II). Journal of Psychoeducational Assessment, 31(3), 337–341. https://doi.org/10.1177/0734282912467756.
Mikami, A. Y., Miller, M., & Lerner, M. D. (2019). Social functioning in youth with attention-deficit/hyperactivity disorder and autism spectrum disorder: Transdiagnostic commonalities and differences. Clinical Psychology Review, 68, 54–70. https://doi.org/10.1016/j.cpr.2018.12.005.
Mishra, A., Ceballos, V., Himmelwright, K., McCabe, S., & Scott, L. (2021). Gesture production in toddlers with autism spectrum disorder. Journal of Autism and Developmental Disorders, 51(5), 1658–1667. https://doi.org/10.1007/s10803-020-04647-5.
Myles, B. S., Simpson, R. L., & Babkie, A. M. (2003). Autism spectrum disorders: A natural fit with DDD. Focus on Autism and Other Developmental Disabilities, 18(4), 268–269. https://doi.org/10.1177/10883576030180040801.
Mullin, A. P., Gokhale, A., Moreno-De-Luca, A., Sanyal, S., Waddington, J. L. & Faundez, V. (2013). Neurodevelopmental disorders: Mechanisms and boundary definitions from genomes, interactomes and proteomes. Translational Psychiatry, 3(12), e329. https://doi.org/10.1038/tp.2013.108.
Oliver, M. (1990). The politics of disablement. Macmillan Education.
Orsmond, G. I., Seltzer, M. M., Greenberg, J. S. & Krauss, M. W. (2006). Mother-child relationship quality among adolescents and adults with autism. American Journal of Mental Retardation, 111(2), 121–137. https://doi.org/10.1352/0895-8017(2006)111[121:MRQAAA]2.0.CO;2.
Pianta, R. C., & Lothman, D. J. (1994). Predicting behavior problems in children with epilepsy: Child factors, disease factors, family stress, and child-mother interaction. Child Development, 65(5), 1415–1428. https://doi.org/10.1111/j.1467-8624.1994.tb00826.x.
Plant, K. M., & Sanders, M. R. (2007). Predictors of care-giver stress in families of preschool-aged children with developmental disabilities. Journal of Intellectual Disability Research, 51(2), 109–124. https://doi.org/10.1111/j.1365-2788.2006.00829.x.
Prizant, B. M., Wetherby, A. M., Rubin, E., Laurent, A. C., & Rydell, P. J. (2006). The SCERTS Model: A comprehensive educational approach for children with autism spectrum disorders (Vol. 1). Brookes Publishing.
Reynolds, C. R., & Kamphaus, R. W. (2015). Behaviour Assessment System for Children - Third Edition. Pearson.
Romero-Gonzalez, M., Chandler, S., & Simonoff, E. (2018). The relationship of parental expressed emotion to co-occurring psychopathology in individuals with autism spectrum disorder: A systematic review. Research in Developmental Disabilities, 72, 152–165. https://doi.org/10.1016/j.ridd.2017.10.022.
Rosen, T. E., Mazefsky, C. A., Vasa, R. A., & Lerner, M. D. (2018). Co-occurring psychiatric conditions in autism spectrum disorder. International Review of Psychiatry, 30(1), 40–61. https://doi.org/10.1080/09540261.2018.1450229.
Rosenbaum, P., Paneth, N., Leviton, A., Goldstein, M., Bax, M., Damiano, D., Dan, B. & Jacobsson, B. (2007). A report: The definition and classification of cerebral palsy April 2006. Developmental Medicine and Child Neurology, Supplement, 109, 8–14. https://doi.org/10.1111/j.1469-8749.2007.tb12610.x.
Rothbart, M. K., Ahadi, S. A., & Evans, D. E. (2000). Temperament and personality: Origins and outcomes. Journal of Personality and Social Psychology, 78(1), 122–135. https://doi.org/10.1037//0022-3514.78.1.12.
Saloviita, T., Itälinna, M., & Leinonen, E. (2003). Explaining the parental stress of fathers and mothers caring for a child with intellectual disability: A Double ABCX Model. Journal of Intellectual Disability Research, 47(Pt 4-5), 300–312. https://doi.org/10.1046/j.1365-2788.2003.00492.x.
Sealy, J., & Glovinsky, I. P. (2016). Strengthening the reflective functioning capacities of parents who have a child with a neurodevelopmental disability through a brief, relationship-focused intervention. Infant Mental Health Journal, 37(2), 115–124. https://doi.org/10.1002/imhj.21557.
Shalev, R. A., Lavine, C., & Di Martino, A. (2020). A systematic review of the role of parent characteristics in parent-mediated interventions for children with autism spectrum disorder. Journal of Developmental and Physical Disabilities, 32, 1–21. https://doi.org/10.1007/s10882-018-9641-x.
Shechtman, Z., & Pastor, R. (2005). Cognitive-behavioral and humanistic group treatment for children with learning disabilities: A comparison of outcomes and process. Journal of Counseling Psychology, 52(3), 322–336. https://doi.org/10.1037/0022-0167.52.3.322.
Sigafoos, J., O’Reilly, M. F., Lancioni, G. E., & Sutherland, D. (2014). Augmentative and alternative communication for individuals with autism spectrum disorder and intellectual disability. Current Developmental Disorders Reports, 1(2), 51–57. https://doi.org/10.1007/s40474-013-0007-x.
Silverman, W. K., & Albano, A. M. (1996). Anxiety disorders interview schedule for DSM-IV: Parent interview schedule (Vol. 1). Oxford University Press.
Smith, L. E., Greenberg, J. S., Seltzer, M. M., & Hong, J. (2008). Symptoms and behavior problems of adolescents and adults with autism: Effects of mother-child relationship quality, warmth, and praise. American Journal on Mental Retardation, 113(5), 387–402. https://doi.org/10.1352/2008.113:387-402.
Sofronoff, K., Attwood, T., & Hinton, S. (2005). A randomised controlled trial of a CBT intervention for anxiety in children with Asperger syndrome. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 46(11), 1152–1160. https://doi.org/10.1111/j.1469-7610.2005.00411.x.
Solomon, M., Ono, M., Timmer, S., & Goodlin-Jones, B. (2008). The effectiveness of parent-child interaction therapy for families of children on the autism spectrum. Journal of Autism and Developmental Disorders, 38(9), 1767–1776. https://doi.org/10.1007/s10803-008-0567-5.
Sukhodolsky, D. G., Scahill, L., Gadow, K. D., Arnold, L. E., Aman, M. G., McDougle, C. J., McCracken, J. T., Tierney, E., White, S. W., Lecavalier, L., & Vitiello, B. (2008). Parent-rated anxiety symptoms in children with pervasive developmental disorders: Frequency and association with core autism symptoms and cognitive functioning. Journal of Abnormal Child Psychology, 36(1), 117–128. https://doi.org/10.1007/s10802-007-9165-9.
Tajik-Parvinchi, D., Farmus, L., Tablon Modica, P., Cribbie, R. A., & Weiss, J. A. (2021). The role of cognitive control and emotion regulation in predicting mental health problems in children with neurodevelopmental disorders. Child: Care, Health and Development, 47(5), 608–617. https://doi.org/10.1111/cch.12868.
Tantam, D. (2003). The challenge of adolescents and adults with Asperger syndrome. Child and Adolescent Psychiatric Clinics of North America, 12(1), 143–viii. https://doi.org/10.1016/s1056-4993(02)00053-6.
Troll, L. E., & Fingerman, K. L. (1996). Connections between parents and their adult children. In C. Magai & S. H. McFadden (Eds.), Handbook of emotion, adult development, and aging (pp. 185–205). Academic Press. https://doi.org/10.1016/B978-012464995-8/50012-1.
van der Meer, J. M. J., Oerlemans, A. M., van Steijn, D. J., Lappenschaar, M. G. A., de Sonneville, L. M. J., Buitelaar, J. K., & Rommelse, N. N. J. (2012). Are autism spectrum disorder and attention-deficit/hyperactivity disorder different manifestations of one overarching disorder? Cognitive and symptom evidence from a clinical and population-based sample. Journal of the American Academy of Child & Adolescent Psychiatry, 51(11), 1160–1172.e3. https://doi.org/10.1016/j.jaac.2012.08.024.
Webster-Stratton, C., & Reid, M. (2008). Adapting the Incredible Years child dinosaur social, emotional, and problem-solving intervention to address comorbid diagnoses. Journal of Children’s Services, 3(3), 17–30. https://doi.org/10.1108/17466660200800016.
Wechsler, D. (2011). Wechsler Abbreviated Scale of Intelligence - Second Edition (WASI-II). Pearson.
Weiss, J. A., Sullivan, A., & Diamond, T. (2003). Parent stress and adaptive functioning of individuals with developmental disabilities. Journal on Developmental Disabilities, 10(1), 129–135.
Weiss, J. A., Thomson, K., Burnham Riosa, P., Albaum, C., Chan, V., Maughan, A., Tablon, P., & Black, K. (2018). A randomized waitlist-controlled trial of cognitive behavior therapy to improve emotion regulation in children with autism. Journal of Child Psychology and Psychiatry, 59(11), 1180–1191. https://doi.org/10.1111/jcpp.12915.
White, S. W., Oswald, D., Ollendick, T., & Scahill, L. (2009). Anxiety in children and adolescents with autism spectrum disorders. Clinical Psychology Review, 29(3), 216–229. https://doi.org/10.1016/j.cpr.2009.01.003.
Wieder S. (2013) Developmental, Individual Difference, Relationship-Based (DIR) Model. In F. R. Volkmar (Ed.) Encyclopedia of autism spectrum disorders. Springer. https://doi.org/10.1007/978-1-4419-1698-3_615.
Woodman, A. C., Mawdsley, H. P., & Hauser-Cram, P. (2015). Parenting stress and child behavior problems within families of children with developmental disabilities: Transactional relations across 15 years. Research in Developmental Disabilities, 36, 264–276. https://doi.org/10.1016/j.ridd.2014.10.011.
Zhou, X., Reynolds, C., Zhu, J., & Kamphaus, R. W. (2020). Differentiating autism from ADHD in children and adolescents using BASC-3. Journal of Pediatric Neuropsychology, 6(3), 61–65. https://doi.org/10.1007/s40817-020-00082-7.
Funding:
This study was supported by the Chair in Autism Spectrum Disorders Treatment and Care Research (#RN284208; Canadian Institutes of Health Research in partnership with the Kids Brain Health Network, the Sinneave Family Foundation, the Canadian Autism Spectrum Disorders Alliance, Autism Speaks Canada and Health Canada) and additional funding from an Operating Grant from CIHR and Kids Brain Health Network. The first author (NV) received additional funding from the LaMarsh Centre for Child & Youth Research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Ethical approval
All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Parents gave written consent for themselves and their children, and children gave verbal assent.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Vashi, N., Bohr, Y. & Weiss, J.A. Transdiagnostic Symptoms in Children with Neurodevelopmental Disabilities and Perceived Parent-Child Relationship Quality: A Pilot Study. J Child Fam Stud 32, 3472–3481 (2023). https://doi.org/10.1007/s10826-023-02570-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-023-02570-8