
Abstract
Maternal prenatal distress (i.e., anxiety and depressive symptoms) increases the risk for childhood behavioral and emotional problems. So far, the potential role of maternal bonding in this association still needs further study. Maternal prenatal distress can affect the development of maternal bonding from pregnancy onwards. Maternal prenatal and postnatal bonding in turn have been shown to predict child behavioral functioning. We aimed to investigate whether maternal prenatal and postnatal bonding mediate the association between maternal prenatal distress and toddlers’ internalizing and externalizing problems. Data from a Dutch prospective longitudinal sample (N = 666) were used to conduct single and multiple mediation models. Mothers reported prenatal anxiety (State Anxiety Inventory) and prenatal depressive symptoms (Edinburgh Postnatal Depression Scale) at 24 weeks’ gestation and maternal prenatal bonding (Maternal Antenatal Attachment Scale) at 32 weeks’ gestation. At 6 weeks and 6 months postpartum mothers completed questionnaires to assess maternal postnatal bonding (Maternal Postnatal Attachment Scale). Mothers reported child internalizing and externalizing problems (Child Behavior Checklist) at 28 months postpartum. Maternal prenatal and postnatal bonding mediated the link between maternal prenatal anxiety and child externalizing problems but not internalizing problems. Only maternal bonding 6 months postpartum mediated the link between maternal prenatal depressive symptoms and child internalizing problems but not externalizing problems. Our study showed that maternal postnatal bonding more consistently mediated links between measures of maternal prenatal distress and child behavioral and emotional problems than maternal prenatal bonding. Interventions reducing maternal prenatal distress and promoting maternal bonding should be developed.
Highlights
-
We examined whether maternal pre- and postnatal bonding mediated links between maternal prenatal distress and child behavioral problems
-
Bonding 6 months postpartum mediated the link between prenatal distress and child behavioral and emotional problems
-
Only the link between prenatal anxiety and child externalizing problems was serially mediated by prenatal bonding and bonding 6 months postpartum
-
Postnatal bonding more consistently mediated links between prenatal distress and child behavioral problems than prenatal bonding
Similar content being viewed by others



Avoid common mistakes on your manuscript.
Several narrative and systematic reviews and meta-analyses have shown that maternal distress (i.e. anxiety and depressive symptoms) during pregnancy is an independent risk factor for offspring behavioral and emotional problems during childhood and adolescence as well as for mental health problems in adulthood (Beijers et al., 2014; Glover et al., 2018; Rees et al., 2019; Rogers et al., 2020; Stein et al., 2014; Talge et al., 2007; Van den Bergh et al., 2020). Talge et al., (2007) estimated that the attributable load of offspring emotional and behavioral problems as a result of maternal prenatal distress is roughly 15%. This demonstrates that maternal prenatal distress is a major public health issue (Glover et al., 2018).
Anxiety and depressive symptoms are comorbid forms of psychopathological problems that are also strongly correlated during pregnancy (Henrichs et al., 2009), and share a common clinical characteristic (i.e., general distress) (Clark & Watson., 1991). Yet, anxiety and depression have unique features such as, respectively, physiological hyperarousal and lack of positive mood (Clark & Watson, 1991). Therefore, pathways and mechanisms involved in the transmission of anxiety and depressive symptoms from mother to offspring may vary. Previous integrative models on the transmission of anxiety and depressive symptoms from mother to child have proposed several biological and environmental mechanisms (Stein et al., 2014; Goodman & Gottlib 1999; Beijers et al., 2014). First, shared genetic factors play an important role in this transmission (Eley et al., 2015; Goodman, 2020). For example, heritability estimates of anxiety and depression are ranging from 30% to 50% (Fernandez-Pujals et al., 2015; Hettema et al., 2001). Second, these figures indicate that environmental factors are also considerably involved in this transmission. That is, animal models and human studies have convincingly shown that maternal prenatal distress negatively influences the development of the offspring brain and subsequent child behavior through intrauterine mechanisms, such as altered maternal stress hormone levels (Beijers et al., 2014; Glover et al., 2018; Van den Bergh et al., 2020). A review based on human studies pointed out that increased levels of maternal stress hormones were associated with offspring behavioral and emotional problems, independent of neonatal outcomes and maternal postnatal distress (Sandman et al., 2011). Postnatal environmental factors have also been postulated to mediate the association between maternal prenatal distress and child behavioral and emotional problems (Stein et al., 2014; Van den Bergh et al., 2020). Based on their literature review on mechanisms underlying this link Beijers et al., (2014) suggested that maternal prenatal distress may foreshadow poor postnatal environmental conditions, such as maternal postnatal distress and compromised caregiving, that may negatively influence child behavioral development. The above illustrates that the association between maternal prenatal distress and child behavioral and emotional problems has frequently been studied. Evidence-based integrative theories suggest various potential mechanisms underlying this link. However, more work is needed to identify causal pathways or mediators, as this might reveal relevant modifiable factors to be addressed by clinical interventions targeting the reduction of maternal prenatal distress and its consequences.
Maternal Prenatal and Postnatal Bonding
Such a candidate mediator may concern a poor emotional tie of the mother with the (unborn) child (i.e., poor maternal bonding). Maternal bonding reflects the perceived affective tie from the mother towards her child stemming from the caregiving system and aiming at the protection of the child (Condon, 1993). Maternal bonding should not be confused with the already frequently studied concept of infant-mother attachment, i.e. an infant being “…strongly disposed to seek proximity to and contact with a specific figure… notably when he is frightened, tired or ill“ (Bowlby, 1969/1982). Maternal bonding originates in pregnancy (Cranley, 1993). Maternal prenatal bonding comprises the development of internal representations of and an emotional tie with the unborn child (Condon, 1993) and predicts maternal postnatal bonding (de Cock et al., 2016; Tichelman et al., 2019). The latter reflects (the level of) self-perceived pleasure in interacting with the child, the development of competence in understanding and meeting the child’s needs as well as being able to accept and adjust to the maternal role (Condon & Corkindale, 1998; Muller, 1994). From pregnancy onwards maternal distress can negatively affect the quality of maternal bonding (Tichelman et al., 2019). A recent systematic review indicated that maternal anxiety during pregnancy was associated with compromised perceptions of the emotional proximity to the unborn child (Göbel et al., 2018). Based on this Göbel et al., (2018) suggested that additional impairment of maternal bonding by anxiety symptoms might negatively affect the developing postnatal mother-infant relationship, which is, in turn, crucial for child development. Postnatally, mothers with depressive symptoms more negatively perceive their infant’s behavior and experience more hostility and a poorer emotional bond towards their infants (Cornish et al., 2006; Mason et al., 2011). The negative impact of maternal distress on maternal bonding may have important implications as maternal prenatal and postnatal bonding has been shown to be related to various child developmental, emotional and behavioral outcomes in infancy and toddlerhood (Fransson et al., 2020; Le Bas, Youssef, Macdonald, Teague, et al., 2021; Le Bas et al., 2020). To be more specific, a systematic review and meta-analysis based on 15 studies by Le Bas et al., (2020) on the association between antenatal and postnatal bonding with infant outcomes reported that stronger maternal bonding was associated with easier infant temperament and more positive infant mood. A large-scale multi-wave prospective pregnancy cohort study in Australia (n = 1347) found that measures of maternal bonding in the prenatal and postnatal period were consistently associated with infant social-emotional development at 12 months of age (Le Bas, Youssef, Macdonald, Teague, et al., 2021). Based on a prospective birth cohort in Sweden (n = 1093), Fransson et al., (2020) observed that maternal postnatal bonding difficulties were associated with more child behavioral problems at 18 months. As maternal prenatal distress can negatively affect maternal bonding (Göbel et al., 2018; Tichelman et al., 2019), suboptimal maternal prenatal and postnatal bonding may thus be an explanatory factor underlying the link between maternal prenatal distress and child behavioral problems.
Maternal Prenatal and Postnatal Bonding as Potential Mediators
A few recent studies investigated the mediating role of maternal postnatal bonding in the link between maternal prenatal distress and infant social-emotional development and child behavioral functioning (Fransson et al., 2020; Le Bas, Youssef, Macdonald, Mattick, et al., 2021). A large-scale prospective cohort study (n = 1579) in Australia examined the interrelationships between measures of maternal negative affect (i.e., anxiety, depressive symptoms, and stress) and maternal bonding in the pre- and postnatal period, as assessed in each pregnancy trimester and at 8 weeks and 12 months postpartum, and infant social-emotional development at 12 months of age (Le Bas, Youssef, Macdonald, Mattick, et al., 2021). Maternal bonding 8 weeks postpartum mediated the association between maternal prenatal negative affect and infant social-emotional development at 12 months (Le Bas, Youssef, Macdonald, Mattick, et al., 2021). A recent Swedish birth cohort study (n = 1093) investigated the influence of symptom duration of maternal depressive symptoms during the perinatal period on toddler behavior and the role of maternal postnatal bonding difficulties in this link (Fransson et al., 2020). Based on self-reported increased maternal depressive symptoms (or a research diagnosis of depression using a neuropsychiatric interview in a subset) in the prenatal and/or postnatal period, three trajectories of maternal depression were categorized: prenatal depression only, postnatal depression only or persistent depression. Maternal bonding at 6 months postpartum mediated the impact of maternal postnatal depression and persistent maternal pre- and postnatal depression on child behavioral and emotional problems at 18 months but not the impact of maternal prenatal depression only (Fransson et al., 2020). These findings indicate the significance of maternal postnatal bonding in transmitting the effects of maternal distress on the child. Although maternal prenatal bonding has been shown to be negatively associated with maternal distress in pregnancy and to be predictive of child development (Göbel et al., 2018; Le Bas et al., 2020; Tichelman et al., 2019), it is so far unknown whether it also plays a mediating role in the link between maternal prenatal distress and child behavioral and emotional problems. Research is needed examining the role of maternal pre- and postnatal bonding in this link. This can reveal crucial insights for the development, improvement, and adequate timing of targeted prevention and intervention programs to promote maternal perinatal mental health, maternal bonding and child outcome (Le Bas et al., 2020; Tichelman et al., 2019).
Child Sex
Studying whether the links between maternal prenatal distress and child behavioral outcomes and the mediating effects of these links via maternal pre- and postnatal bonding differ for boys and girls can additionally support the development of targeted interventions. Already in early childhood sex differences in child behavioral and emotional problems (i.e., externalizing and internalizing problems) have been observed (Achenbach & Rescorla, 2000). In comparison to boys, girls had more internalizing problems at age 36 months, whereas boys had higher levels of externalizing problems than girls (Henrichs et al., 2013). Biological theories suggest sex-specific responses of male and female fetuses to exposure to maternal distress signals (DiPietro et al., 2011), while social theories suggest gendered caregiving and parenting practices during early childhood and propose that socially constructed gender biases may create ways behavioral and emotional problems are seen and tolerated (Dean et al., 2017; Mesman & Groeneveld, 2018). Some previous studies indeed suggest that girls exposed to maternal prenatal distress are at a higher risk of developing internalizing problems than boys, while boys have a higher risk of developing externalizing problems (Van den Bergh et al., 2020). However, other studies found no evidence showing that child sex moderates this link (MacKinnon et al., 2018; Robinson et al., 2011). More research is needed into this matter. Also, a few studies reported that having a boy was related to higher levels of maternal bonding (Tichelman et al., 2019). Yet, to the best of our knowledge, it has not been studied so far whether the indirect link between maternal prenatal distress and toddlers’ behavioral problems via maternal pre-and/or postnatal bonding differs for boys and girls. This evokes investigating whether pathways differ for boys and girls.
The Present Study
Using data from a Dutch prospective longitudinal sample the present study addressed two major research questions:
-
1.
Do maternal pre- and postnatal bonding independently and/or serially mediate the potential association between maternal prenatal distress and child behavioral and emotional problems in toddlerhood?
-
2.
Does child sex moderate (a) the association between maternal prenatal distress and child behavioral and emotional problems; and (b) the mediation effects of maternal prenatal and postnatal bonding on this association (see Fig. 1 for a conceptual model)?
Fig. 1 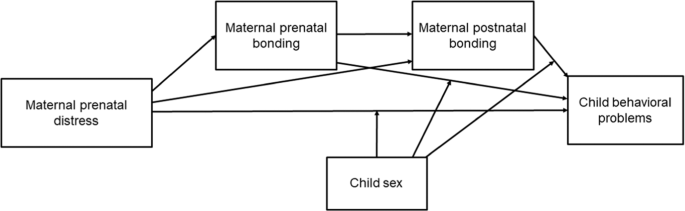
Conceptual model. Moderated-mediation model testing the mediating effect of maternal pre- and postnatal bonding on the link between maternal prenatal distress (anxiety or depressive symptoms) and child behavioral and emotional problems in toddlerhood by child sex

Methods
Participants and Procedures
The current study is based on a prospective longitudinal survey embedded in the IRIS study (Henrichs et al., 2019; Henrichs et al., 2016). The IRIS study is a stepped-wedge cluster-randomized trial (n = 13520) examining the (cost-)effectiveness of third trimester universal ultrasonography to reduce severe adverse perinatal outcomes as compared to usual care (i.e., third trimester clinically indicated ultrasonography) (trial registration number: NTR4367; date of registration: 21 March 2014) (Henrichs et al., 2019). Women with a low risk singleton pregnancy were enrolled in mid-pregnancy (22.8 weeks’ gestation (SD = 2.4)) via 60 midwifery practices between February 2015 and February 2016 (Henrichs et al., 2019).
To explore maternal psychosocial functioning and child neurodevelopmental outcomes, a longitudinal survey has been conducted among a non-selective subsample (n = 1475). This subsample had a baseline measurement (T0) at 24.0 weeks’ gestation on average (SD = 2.0). Follow-ups were conducted around 32 weeks’ gestation (T1, M = 32.0 weeks (SD = 0.6)) and 6 weeks (T2, M = 6.1 weeks (SD = 2.0)), 6 months (T3, M = 6.1 months (SD = 0.5)), and 26–29 months after birth (T4, M = 28.0 (SD = 1.0)). Data of T0-T4 were used for the current study. Mothers completed online questionnaires with Survalyzer (https://www.survalyzer.com/nl). This online tool was used for the development and administration of the questionnaires. Questionnaires were made available in Dutch or English. The design of the IRIS study has previously been depicted in more detail (Henrichs et al., 2016).
All women included in this study gave written informed consent for participation in both the IRIS study trial and the embedded survey. The IRIS study and the survey study have been approved by the IRB of VU Medical University Center Amsterdam, the Netherlands (reference numbers: 2013.409 and 2015.033, respectively).
For the embedded longitudinal survey, 1475 women were enrolled for the non-selective subsample at 24 weeks’ gestation. Of those, 1422 women (96.4% of the initially enrolled 1475 subjects) provided data on maternal prenatal distress at T0 and were eligible for this study. Mothers of 748 children reported child behavioral and emotional problems in toddlerhood (53% of the 1422 eligible subjects). Data on maternal pre- and postnatal bonding, and covariates included in our main analyses were not available for 82 subjects because of drop-out, loss to follow-up or not filling in questionnaires. Thus, up to 666 mothers and children (47% of 1422 eligible subjects) were included in one or more of our main analyses. Due to varying numbers of missing data on the mediators (i.e., maternal prenatal and postnatal bonding) the number of mother-child pairs included in our main analyses ranged from 561 to 631 observations.
Compared to those excluded from the analyses due to missing data or loss-to-follow-up, included children (n = 666) had higher birth weights, M = 3524 grams (SD = 509) versus M = 3465 grams (SD = 533), t = 2.16, p = 0.031, and but did not differ in gestational ages at birth, M = 39.7 weeks (SD = 1.6) versus M = 39.6 (SD = 1.6), t = 1.29, p = 0.20. Responding mothers were more likely to be highly educated, 65.9% versus 50.1%, χ2 = 37.18, df = 1, p < 0.001 and Dutch, 87.2% versus 74.9%, χ2 = 36.15, df = 1, p < 0.001 and to have lower levels of prenatal anxiety, M = 32.4 (SD = 9.5) versus M = 34.1 (SD = 9.7), t = 3.25, p = 0.001 and prenatal depressive symptoms, M = 5.4 (SD = 4.0) versus M = 6.1 (SD = 4.3), t = 2.94 p = 0.003 than non-responders.
Measures
Maternal Prenatal Anxiety
At 24 weeks’ gestation mothers reported state anxiety using the Dutch validated short-form of the state anxiety subscale of the Spielberger State Trait Anxiety Inventory (STAI) (Spielberger, 1975; van der Bij et al., 2003). The 6-item version of the short-form of the STAI state anxiety subscale (STAI-S) assesses levels of anxiety symptoms in response to momentary stressors (Spielberger, 1975; van der Bij et al., 2003). Respondents were asked to indicate how well each item, e.g. “I am upset”, of the STAI-S represented their momentary emotional state (1 = not at all, 4 = very much so). When one item was missing, a weighted total STAI-S sum score was calculated. Higher total STAI-S sum scores, ranging from 20 to 80, indicate higher levels of state anxiety. Good psychometric properties have been reported for the Dutch version of the STAI-S (van der Bij et al., 2003). In our study, the internal consistency of the STAI-S was α = 0.83. This measurement was repeated six weeks after birth.
Maternal Depressive Symptoms
At 24 weeks’ gestation, maternal depressive symptoms in the last seven days were assessed using the 10-item Dutch version of the Edinburgh Postnatal Depression Scale (EPDS) (Bergink et al., 2011; Pop et al., 1992). The Dutch version of the EPDS has been validated in both the pre- and postnatal period (Bergink et al., 2011; Pop et al., 1992). Women were asked to answer items using a 4-point scale (0–3), e.g. “Things have been getting on top of me”, to indicate how well the items indicate women’s level of depressive feelings. When one or two EPDS items were missing, a weighted total sum score was calculated. Total sum scores range from 0 to 30 with higher scores indicating more depressive symptoms. The Dutch version of the EPDS has good psychometric properties (Pop et al., 1992). In our study, the internal consistency was α = 0.83. This measurement was repeated six weeks after birth.
Maternal Pre- and Postnatal Bonding
At 32 weeks’ gestation, and 6 weeks and 6 months postpartum, mothers reported experiences of maternal pre- and postnatal bonding using the Maternal Antenatal Attachment Scale (MAAS) and Maternal Postnatal Attachment Scale (MPAS), respectively (Condon, 1993; Condon & Corkindale, 1998). The MAAS comprises 19 items, e.g. “Over the past 2 weeks I have thought about, or have been preoccupied with the baby inside me/the developing baby”. Items are scored on a Likert scale ranging from 1 to 5. In case of missing items, a weighted total MAAS sum score allowing for ≤25% missing items was calculated. Higher total MAAS sum scores reflect increased levels of prenatal bonding. In our study, Cronbach’s alpha of the MAAS was 0.76.
To measure maternal postnatal bonding, the Maternal Postnatal Attachment Scale was used (MPAS) (Condon & Corkindale, 1998), comprising 19 items, e.g. “When I am not with the baby/child, I find myself thinking about the baby/child”. Items are scored using a Likert Scale ranging from 1 to 5. In case of missing items, a weighted total MPAS sum score allowing for ≤25% missing items was calculated. Higher scores reflect higher levels of maternal postnatal bonding. In our sample, Cronbach’s alpha of the MPAS was 0.79 at both 6 weeks and 6 months postpartum. A previous systematic review reported good psychometric properties for the MAAS and MPAS according to supportive evidence for structural validity as well as alphas larger than 0.70 for the various MPAS and MAAS (sub)scales (Wittkowski et al., 2020).
Child Behavioral and Emotional Problems
Using the preschool form of the Child Behavior Checklist (CBCL/1.5–5), mothers reported behavioral and emotional problems of toddlers aged 28 months (Achenbach & Rescorla, 2000). Mothers were asked to fill in each of the 99 items concerning behavioral and emotional problems in the preceding two months, e.g. “worries”, on a 3-point Likert scale (0 = not true, 2 = very true or often true). For the current study, we used two-broad-band scales that were established via second-order-factor-analyses based on the CBCL factor-analytically derived syndromes. That is, (1) the internalizing problems scale based on the sum score of the emotionally reactive, anxious/depressed, somatic complaints and withdrawn syndromes, and (2) the externalizing problems scale based on the sum score of the attention problems and aggressive behavior syndromes. In case of missing items, weighted internalizing and externalizing sum scores allowing for ≤25% missing items were calculated. Higher scores indicate more internalizing and externalizing problems, respectively. Adequate construct validity and test–retest reliability have been reported for the CBCL/1.5–5 (Achenbach & Rescorla, 2000). In our study, Cronbach’s alpha for the internalizing problems scale was 0.79 and 0.90 for the externalizing scale.
Covariates
Based on earlier research studying the associations of maternal prenatal distress and maternal pre- and postnatal bonding with child behavioral and developmental outcomes (de Cock et al., 2017; Le Bas, Youssef, Macdonald, Mattick, et al., 2021; Van Batenburg-Eddes et al., 2013), we considered the following potential covariates: maternal age, educational level, ethnic background, marital status, parity, gestational age at birth, birth weight, infant sex, smoking during pregnancy, and maternal postnatal distress. Due to the overarching trial design we considered to control for study condition (i.e., universal versus clinically indicated third trimester ultrasonography).
At enrollment women and/or midwifes reported maternal age, educational level coded as high (at least higher vocational training or a bachelor’s degree) versus low/medium (lower vocational training or less), maternal ethnicity (Dutch versus Non-Dutch), marital status (single/not living together versus married/living together), smoking during pregnancy (yes versus no or stopped) and parity (nulliparous versus multiparous). Information on birth weight, gestational age at birth, and child sex was derived from perinatal registries or medical hospital files filled in by trained research assistants (Henrichs et al., 2016). Postnatal distress was assessed using data from the 6 weeks follow-up assessment, when women reported anxiety and depressive symptoms again using the EPDS and STAI-S (Pop et al., 1992; Spielberger, 1975; van der Bij et al., 2003). At this follow-up, Cronbach’s alpha of the EPDS was 0.83 and 0.80 for the STAI-S.
Statistical Analyses
To answer our main research question we conducted three analytical steps. In a first step, we tested whether measures of maternal prenatal anxiety and depressive symptoms, and maternal pre- and postnatal bonding were correlated with each other and with child internalizing and externalizing problems using Pearson correlations. Pearson correlations of (r) < 0.3 represent small effects, 0.3 < r < 0.5 moderate effects, and r > 0.5 large effects (Cohen, 1988).
In a second step, taking into account the significant correlations observed, we then investigated whether measures of maternal pre- and postnatal bonding were single mediators of the potential association of maternal prenatal anxiety or depressive symptoms with child internalizing and externalizing problems. We used single mediation models applying Model 4 of the PROCESS macro included in the Statistical Package for Social Sciences (SPSS version 25.0) (Hayes, 2013). This SPSS macro applies the bootstrap method to examine (moderated) mediation models estimating the indirect effect of one or more potential mediator(s) based on 10,000 resamples and computing bias-corrected bootstrap 95% confidence intervals (CIs) (Hayes, 2013). This method can take into the account the potential non-normality and/or asymmetry of indirect effects (Hayes, 2013). To present effect sizes of the examined mediation models, completely standardized indirect effects (β) have been reported. Estimates of indirect effects are interpreted as statistically significant when CIs do not comprise zero.
In a third step, factors that were revealed to be significant single mediators were then analyzed jointly using multiple serial mediation models based on Model 6 of PROCESS. Using the bootstrap method, these models examined the joint mediating effect (i.e., total indirect effect) of all measures of maternal prenatal and postnatal bonding under investigation. Using these multiple serial mediation models, the possible independent (and serial) indirect effects of the individual mediators were also examined, while adjusting for all other mediators included these models (Preacher & Hayes, 2008). To rule out possible collinearity effects, mediation models were performed separately for maternal prenatal anxiety and depressive symptoms. Maternal prenatal anxiety and depressive symptoms were strongly associated, r = 0.65, p < 0.001.
Finally, Model 15 of PROCESS was used to test whether child sex moderated the (a) associations of maternal prenatal anxiety or depressive symptoms with child behavioral and emotional problems, and (b) whether it moderated the possible mediation effects of maternal pre- and postnatal bonding on these associations.
Potential covariates were examined for inclusion in the mediation models by running exploratory Pearson correlations with the mediators and child outcomes. Covariates were retained if they were significantly correlated with one of the mediators or outcomes. Covariates retained comprised child sex, maternal age, educational level, smoking during pregnancy, marital status, parity, and maternal anxiety (or maternal depressive symptoms) 6 weeks after birth. All results presented in this paper were based on complete case analysis.
Results
Sample Characteristics and Descriptives
Table 1 presents characteristics of mothers and children. Mothers were almost 32 years old on average, M = 31.7 (SD = 4.0), and the large majority of them were indigenous Dutch (87.2%) and highly educated (65.9%). Of the children 52.7% were boys. Correlations between maternal prenatal distress, maternal pre- and postnatal bonding and child internalizing and externalizing problems in toddlerhood are shown in Table 2. Maternal prenatal anxiety was negatively correlated with all measures of maternal prenatal and postnatal bonding and positively with maternal prenatal depressive symptoms and child internalizing and externalizing problems. Maternal prenatal depressive symptoms were also positively associated with both child outcomes and negatively associated with maternal bonding at age 6 weeks and 6 months postpartum but not with maternal prenatal bonding. All measures of bonding were negatively correlated with child internalizing and externalizing problems and positively with each other. The correlation between maternal bonding 6 weeks postpartum and maternal bonding 6 months postpartum was strong (r = 0.66, p < 0.001).
Maternal Prenatal Anxiety and Child Outcome: Single and Multiple Mediator Models
Taking into account the significant correlations observed, we then conducted six single mediator models testing whether measures of maternal pre- and postnatal bonding mediated the link between maternal prenatal anxiety and the child behavioral outcomes. These models were adjusted for the earlier described demographic and perinatal covariates and maternal postnatal anxiety six weeks after birth. Table 3a shows that maternal prenatal bonding mediated the link between maternal prenatal anxiety and child externalizing problems, β = 0.015, 95%CI [0.002, 0.032]. Maternal postnatal bonding at age six months also mediated this link, β = 0.020, 95%CI [0.005, 0.042]. Maternal postnatal bonding 6 weeks after birth was not a significant mediator of this link. Moreover, none of the measures of maternal pre- and postnatal bonding mediated the association between maternal prenatal anxiety and child internalizing problems.
As maternal prenatal bonding and postnatal bonding 6 months after birth were identified as single mediators of the link between maternal prenatal anxiety and child externalizing problems, a fully adjusted multiple serial mediation model was conducted to examine which of these factors were independent (or serial) mediators of this link. The results of this multiple serial mediation model are summarized in Fig. 2. In this fully adjusted model, maternal prenatal anxiety was directly associated with more child externalizing problems, B = 0.08, 95% confidence interval (CI) [0.01, 0.15], t(543) = 2.26, p = 0.025. The total indirect effect based on the sum of the tested mediating paths was significant, β = 0.023, 95% CI [0.005, 0.046]. Moreover, maternal prenatal bonding and maternal postnatal bonding 6 months after birth independently and serially mediated the association between maternal prenatal anxiety and child externalizing problems (see Fig. 2).

Multiple serial mediation model showing the links between maternal prenatal anxiety and child externalizing problems at age 28 months via maternal prenatal bonding and maternal postnatal bonding at age 6 months controlled for child sex, maternal age, educational level, and smoking during pregnancy, parity, marital status, and maternal anxiety 6 weeks after birth. Effect estimates reflect standardized coefficients (β). *p < 0.05, **p < 0.01; ***p < 0.001
Maternal Prenatal Depressive Symptoms and Child Outcome: Single and Multiple Mediation Models
Single mediation models revealed little evidence showing that measures of maternal bonding mediated the associations between maternal prenatal depressive symptoms and child internalizing and externalizing problems as shown in Table 3b. Only maternal bonding 6 months postpartum was found to significantly mediate the association between maternal prenatal depressive symptoms and child internalizing problems but not externalizing problems after adjustment for perinatal and demographic covariates and maternal depressive symptoms 6 weeks after birth. In this fully adjusted model, maternal prenatal depressive symptoms were directly associated with more child externalizing problems, B = 0.13, 95% CI [0.04; 0.23], t(584) = 2.78, p = 0.006 (see also Fig. 3). Moreover, as maternal prenatal depressive symptoms were not significantly correlated with maternal prenatal bonding, we were not able to include the latter variable in the single mediation models (see Table 3b). Due to these results further multiple mediation models concerning the link between maternal prenatal depressive symptoms and child behavioral and emotional problems were not performed.

Single mediator model showing the association between maternal depressive symptoms during pregnancy and child internalizing problems at age 28 months via maternal postnatal bonding at age 6 months controlled for child sex, maternal age, educational level, and smoking during pregnancy, parity, marital status, and maternal depressive symptoms 6 weeks after birth. Effect estimates reflect standardized coefficients (β). *p < 0.05
Child Sex
In a final step, we examined whether child sex moderated links between measures of prenatal distress and child outcomes or mediating effects of maternal prenatal and postnatal bonding on these links using multiple moderated mediation models. Child sex did not moderate the links between measures of maternal prenatal distress and child behavioral and emotional problems. Moreover, none of the tested moderated mediation effects by child sex were significant.
Discussion
This longitudinal study showed that primarily maternal postnatal bonding 6 months after birth mediated the association between measures of maternal prenatal distress and child behavioral and emotional problems at age 28 months. Furthermore, we observed that only the association between maternal prenatal anxiety and child externalizing problems at age 28 months was mediated by maternal prenatal bonding and, in turn, by maternal postnatal bonding at age 6 months. We found no evidence for moderated mediation effects by child sex.
Our findings demonstrate the relevance of maternal prenatal bonding as well as maternal postnatal bonding in the link between maternal prenatal distress and child behavioral and emotional problems. It has been suggested that the promotion of maternal bonding early in life can improve child developmental patterns (Le Bas et al., 2020; Tichelman et al., 2019). Moreover, maternal bonding in the perinatal period is associated with child developmental and behavioral outcomes in infancy and toddlerhood (Fransson et al., 2020; Le Bas, Youssef, Macdonald, Teague, et al., 2021; Le Bas et al., 2020). In analogy to a previous cohort study using infant social-emotional development as an outcome (Le Bas, Youssef, Macdonald, Mattick, et al., 2021), we observed that maternal postnatal bonding in early infancy mediates the link between maternal prenatal distress and child behavioral and emotional problems. Yet, our study extends previous work by showing that maternal prenatal bonding mediates the link of maternal prenatal anxiety with toddlers’ externalizing problems.
Interestingly, maternal prenatal bonding mediated the association of maternal prenatal anxiety (but not of maternal prenatal depressive symptoms) with child externalizing problems. This finding may partly be explained by our observation of a non-significant correlation between maternal prenatal depressive symptoms and maternal prenatal bonding while prenatal anxiety was significantly correlated with prenatal bonding. Intuitively one might have expected significant negative correlations with maternal prenatal bonding for both maternal prenatal anxiety and maternal depressive symptoms as observed in earlier research (Condon & Corkindale, 1997; Le Bas, Youssef, Macdonald, Mattick, et al., 2021). Göbel et al., (2018) suggested that maternal prenatal anxiety can affect the quality of maternal prenatal bonding, i.e. experiences of emotional proximity to the unborn child in particular, including positive feelings towards the unborn child and the formation of representations of the future baby as a person. Similarly, feelings of worthlessness, guilt and lacking confidence as expectant mother due to prenatal depressive symptoms can inhibit the development of a positive bond with the fetus and increase maternal tendencies of having negative thoughts and feelings towards the unborn child (Rolle et al., 2020). As maternal distress regularly continues into the postnatal period (Fransson et al., 2020; Henrichs et al., 2009), it may also exert long-term effects on maternal postnatal bonding. This reasoning is supported by our findings and previous research showing links between maternal prenatal distress and poorer maternal postnatal bonding (Fransson et al., 2020; Le Bas, Youssef, Macdonald, Mattick, et al., 2021). Yet, the systematic review by Tichelman et al., (2019) reported that maternal prenatal depressive symptoms were not consistently related to maternal prenatal bonding across various previous studies, while the impact of anxiety on bonding has less often been studied so far. More research is needed to better understand the nature and (bi-)directionality of the links between maternal prenatal distress and maternal bonding in the perinatal period.
While maternal prenatal bonding was correlated with all maternal prenatal anxiety and child internalizing and externalizing problems, it only mediated the association of maternal prenatal anxiety with child externalizing but not internalizing problems. This latter finding might be a result of the adjustment for covariates. Whether maternal prenatal bonding indeed only mediates the link between maternal prenatal anxiety and child externalizing but not internalizing problems should be re-examined in longitudinal replication studies.
In contrast to maternal prenatal bonding, maternal postnatal bonding at age 6 months more consistently mediated the associations of maternal prenatal distress with child behavioral and emotional problems. This might be explained by the closer temporal proximity of the assessment time points of postnatal bonding and the child outcomes. Interestingly, we also observed that maternal prenatal and postnatal bonding serially mediated the link between maternal prenatal anxiety and child externalizing problems. The link between maternal prenatal and postnatal bonding is moderately stable in the pre- and postnatal period (de Cock et al., 2016; Tichelman et al., 2019). The negative influence of maternal prenatal anxiety on maternal prenatal bonding (Göbel et al., 2018), may therefore continue into the postnatal period leading to poorer maternal postnatal bonding, which, in turn, can affect child behavioral development (Fransson et al., 2020). Our results thus suggest that maternal prenatal anxiety negatively influences the development of maternal prenatal bonding, which subsequently affects toddlers’ externalizing behavior via poor maternal postnatal bonding. The current study and previous research suggest that maternal distress and bonding are interrelated in the prenatal and postnatal period but may also constitute unique predictors of child outcome (Fransson et al., 2020; Göbel et al., 2018; Henrichs et al., 2009; Le Bas, Youssef, Macdonald, Mattick, et al., 2021; Le Bas et al., 2020; Tichelman et al., 2019). To better understand this complexity larger studies are needed addressing possible pathways and temporal and bi-directional links between maternal distress and bonding across the prenatal and postnatal period and testing the direct and indirect effects of these constructs on child behavioral outcomes using, for example, crossed-lagged models (e.g., Le Bas, Youssef, Macdonald, Mattick et al., 2021).
Finally, child sex did not moderate the link between maternal prenatal distress and child behavioral and emotional problems in contrast to two previous studies (de Bruijn et al., 2009; Glasheen et al., 2013), but in line with other research (MacKinnon et al., 2018; Robinson et al., 2011). Also, child sex did not moderate mediation effects of maternal pre- and postnatal bonding on the link between maternal prenatal distress and child behavioral and emotional problems. The current study may have been insufficiently powered to detect moderated mediation effects, or our findings may suggest that child sex simply does not moderate mediation effects of maternal prenatal and postnatal bonding on this link.
Strengths and Limitations
Strengths of our study include the availability of data on a broad set of potential covariates and the prospective longitudinal design, with repeated measurements of maternal bonding in particular, allowing to test the directionality of effects of the proposed mediation model. However, our study also has a number of potential limitations. First, data on determinants, mediators and child outcomes were based on maternal reports possibly introducing self-report bias. Distressed mothers might be more prone to overreport toddlers’ behavioral and emotional problems (Gartstein et al., 2009), while mothers with positive bonding patterns might see their toddler’s behavior in a positive way or vice versa. However, the used self-report instruments to assess distress, bonding and child behavior, respectively, are considered gold-standard with confirmed validity (Achenbach & Rescorla, 2000; Condon, 1993; Condon & Corkindale, 1998; Pop et al., 1992; Spielberger, 1975; van der Bij et al., 2003). These instruments are extensively used in clinical and public health care for screening purposes and to guide diagnostic and treatment processes. Next to this, behavioral and emotional problems of young children at age 2-3 years and of children or adolescents at the ages of 4–18 years as assessed with parent report based on the CBCL, predicted DSM-IV diagnosed equivalents of psychopathology even 24 years later (Reef et al., 2011). Nevertheless, using father reports and/or observers’ assessments of child outcomes would have been a valuable addition to our study. Future research should also consider using observational measures to assess severity of maternal anxiety or depressive symptomatology by the use of clinical interviews and/or observations of maternal sensitivity for additional validation of maternal bonding. Second, we cannot rule out that genetic influences are involved in the interrelationships between maternal distress, maternal bonding and child outcome. Future studies investigating these interrelationships should therefore apply family-based behavioral genetic designs such as a sibling design making it possible to adjust for genetic and environmental influences shared by the siblings (Bekkhus et al., 2018). Such an approach would also allow to deduce whether exposure to maternal prenatal distress can be explained by intrauterine effects (Bekkhus et al., 2018). Third, compared to non-responders data of mother-child pairs included in our analyses were more complete in mothers with high levels of education and Dutch ethnicity and less prenatal distress as well as in children with higher birth weights. Thus, selection bias may have led to an underestimation of the associations under investigation. Moreover, the current sample was mainly based on highly educated and predominantly Dutch women with a low-risk pregnancy status possibly limiting the generalizability of our findings to clinical, ethnically diverse and low educated sub-populations. Large-scale population-based studies including these sub-populations are needed. Fourth, our study lacked data on paternal distress and bonding. Future studies should examine the joint impact and interplay of maternal and paternal distress and bonding in the pre- and postnatal period on child behavioral development. Fifth, the applied analytical approach did not allow to simultaneously analyze whether the effects of both maternal anxiety and depressive symptoms during pregnancy on the child outcomes were mediated by maternal prenatal and postnatal bonding due to the collinearity of these two forms of distress in the current sample. Future studies, that are based on adequately powered longitudinal samples (even larger than the current sample) and that allow the detection of small effect sizes, are needed to take such collinearity issues into account using structural equation modelling.
Clinical Implications
In our study, both maternal prenatal and maternal postnatal bonding mediated the associations between maternal prenatal distress and child behavioral and emotional problems. This has important implications for prevention and intervention strategies in the perinatal period. Since maternal prenatal distress represents a serious public health problem (Talge et al., 2007), universal screening for maternal prenatal distress as part of antenatal care should be combined with multimodal psychological interventions for distressed pregnant women designed to reduce maternal distress and improve maternal bonding. Such interventions are scarce so far. A randomized pilot study among 60 pregnant women with moderate to severe depressive symptomatology suggested that group-based cognitive-behavioral therapy emphasizing the mother-baby relationship may exert beneficial effects on reducing postpartum depressive symptoms and improving maternal bonding (Alhusen et al., 2021). More research is needed to develop and evaluate similar multimodal preventive (online) interventions targeting both the reduction of maternal prenatal distress and promotion of maternal bonding.
Conclusions
This longitudinal study revealed that mainly maternal postnatal bonding 6 months after birth mediated the link between maternal prenatal distress and child behavioral and emotional problems in toddlerhood. Our findings suggest that maternal prenatal anxiety negatively influences the development of maternal bonding during pregnancy, which subsequently affects toddlers’ externalizing behavior via poor maternal bonding in early infancy. We observed no evidence that child sex may modulate the mediating effects of maternal pre- and postnatal bonding on the link between maternal prenatal distress and child behavioral and emotional problems. Future work should examine the interplay of effects of maternal and paternal perinatal distress and bonding on children’s mental health and invest in developing multimodal preventive interventions supporting distressed women with bonding difficulties during pregnancy and early motherhood.
Data Availability
The provided ethical approval for the IRIS study does not allow publication of individual participant level data. Requests for a de-identified dataset require a Data Transfer Agreement that is in accordance with the European Union´s General Data Protection Regulation (GDPR).
References
Achenbach, T. M., & Rescorla, L. A. (2000). Manual for ASEBA preschool forms & profiles. University of Vermont, Research Center for Children, Youth and Families.
Alhusen, J. L., Hayat, M. J., & Borg, L. (2021). A pilot study of a group-based perinatal depression intervention on reducing depressive symptoms and improving maternal-fetal attachment and maternal sensitivity. Archives of Women’s Mental Health, 24(1), 145–154. https://doi.org/10.1007/s00737-020-01032-0.
Le Bas, G. A., Youssef, G. J., Macdonald, J. A., Rossen, L., Teague, S. J., Kothe, E. J., McIntosh, J. E., Olsson, C. A., & Hutchinson, D. M. (2020). The role of antenatal and postnatal maternal bonding in infant development: A systematic review and meta-analysis. Social Development, 29(1), 3–20. <Go to ISI>://WOS:000481540500001.
Le Bas, G. A., Youssef, G. J., Macdonald, J. A., Mattick, R., Teague, S. J., Honan, I., McIntosh, J. E., Khor, S., Rossen, L., Elliott, E. J., Allsop, S., Burns, L., Olsson, C. A., & Hutchinson, D. M. (2021). Maternal bonding, negative affect, and infant social-emotional development: A prospective cohort study. Journal of Affective Disorders, 281, 926–934. https://doi.org/10.1016/j.jad.2020.11.031.
Le Bas, G. A., Youssef, G., Macdonald, J. A., Teague, S., Mattick, R., Honan, I., McIntosh, J. E., Khor, S., Rossen, L., Elliott, E. J., Allsop, S., Burns, L., Olsson, C. A., & Hutchinson, D. (2021). The role of antenatal and P\postnatal maternal bonding in infant development. Journal of the American Acadamy of Child and Adolescent Psychiatry. https://doi.org/10.1016/j.jaac.2021.08.024.
Van Batenburg-Eddes, T., Brion, M. J., Henrichs, J., Jaddoe, V. W., Hofman, A., Verhulst, F. C., Lawlor, D. A., Davey Smith, G., & Tiemeier, H. (2013). Parental depressive and anxiety symptoms during pregnancy and attention problems in children: a cross-cohort consistency study. Journal of Child Psychology and Psychiatry, 54(5), 591–600. https://doi.org/10.1111/jcpp.12023.
Beijers, R., Buitelaar, J. K., & de Weerth, C. (2014). Mechanisms underlying the effects of prenatal psychosocial stress on child outcomes: beyond the HPA axis. European Child & Adolescent Psychiatry, 23(10), 943–956. https://doi.org/10.1007/s00787-014-0566-3.
Bekkhus, M., Lee, Y., Nordhagen, R., Magnus, P., Samuelsen, S. O., & Borge, A. I. H. (2018). Re-examining the link between prenatal maternal anxiety and child emotional difficulties, using a sibling design. International Journal of Epidemiology, 47(1), 156–165. https://doi.org/10.1093/ije/dyx186.
Van den Bergh, B. R. H., van den Heuvel, M. I., Lahti, M., Braeken, M., de Rooij, S. R., Entringer, S., Hoyer, D., Roseboom, T., Raikkonen, K., King, S., & Schwab, M. (2020). Prenatal developmental origins of behavior and mental health: The influence of maternal stress in pregnancy. Neuroscience and Biobehavioral Reviews, 26–64. https://doi.org/10.1016/j.neubiorev.2017.07.003.
Bergink, V., Kooistra, L., Lambregtse-van den Berg, M. P., Wijnen, H., Bunevicius, R., van Baar, A., & Pop, V. (2011). Validation of the Edinburgh Depression Scale during pregnancy. Journal of Psychosomatic Research, 70(4), 385–389. https://doi.org/10.1016/j.jpsychores.2010.07.008.
van der Bij, A. K., de Weerd, S., Cikot, R. J., Steegers, E. A., & Braspenning, J. C. (2003). Validation of the dutch short form of the state scale of the Spielberger State-Trait Anxiety Inventory: considerations for usage in screening outcomes. Community Genetics, 6(2), 84–87. https://doi.org/10.1159/000073003.
Bowlby, J. (1969/1982). Attachment and loss: Vol. 1. Attachment. Basic Books.
de Bruijn, A. T., van Bakel, H. J., Wijnen, H., Pop, V. J., & van Baar, A. L. (2009). Prenatal maternal emotional complaints are associated with cortisol responses in toddler and preschool aged girls. Developmental Psychobiology, 51(7), 553–563. https://doi.org/10.1002/dev.20393.
Clark, L. A., & Watson, D. (1991). Tripartite model of anxiety and depression - psychometric evidence and taxonomic implications. Journal of Abnormal Psychology, 100(3), 316–336. https://doi.org/10.1037/0021-843x.100.3.316.
de Cock, E. S., Henrichs, J., Vreeswijk, C. M., Maas, A. J., Rijk, C. H., & van Bakel, H. J. (2016). Continuous feelings of love? The parental bond from pregnancy to toddlerhood. Journal of Family Psychology, 30(1), 125–134. https://doi.org/10.1037/fam0000138.
de Cock, E. S., Henrichs, J., Klimstra, T. A., Janneke, B. M. M. A., Vreeswijk, C., Meeus, W. H. J., & van Bakel, H. J. A. (2017). Longitudinal associations between parental bonding, parenting stress, and executive functioning in toddlerhood. Journal of Child and Family Studies, 26(6), 1723–1733. https://doi.org/10.1007/10826-017-0679-7.
Cohen, J. (1988). Statistical Power Analysis for the Behavioral Sciences (2nd ed.). Lawrence Erlbaum Associates, Publishers.
Condon, J. T. (1993). The assessment of antenatal emotional attachment - development of a questionnaire instrument. British Journal of Medical Psychology, 66, 167–183. https://doi.org/10.1111/j.2044-8341.1993.tb01739.x.
Condon, J. T., & Corkindale, C. (1997). The correlates of antenatal attachment in pregnant women. British Journal of Medical Psychology, 70(Pt 4), 359–372. https://doi.org/10.1111/j.2044-8341.1997.tb01912.x.
Condon, J. T., & Corkindale, C. J. (1998). The assessment of parent-to-infant attachment: Development of a self-report questionnaire instrument. Journal of Reproductive and Infant Psychology, 16, 57–76. https://doi.org/10.1080/02646839808404558.
Cornish, A. M., McMahon, C. A., Ungerer, J. A., Barnett, B., Kowalenko, N., & Tennant, C. (2006). Maternal depression and the experience of parenting in the second postnatal year. Journal of Reproductive and Infant Psychology, 24(2), 121–132. https://doi.org/10.1080/02646830600644021.
Cranley, M. S. (1993). The origins of the mother-child relationship—A review. Physical & Occupational Therapy in Pediatrics, 12, 39–51. https://doi.org/10.1080/J006v12n02_03.
Dean, M., Harwood, R., & Kasari, C. (2017). The art of camouflage: Gender differences in the social behaviors of girls and boys with autism spectrum disorder. Autism, 21(6), 678–689. https://doi.org/10.1177/1362361316671845.
DiPietro, J. A., Costigan, K. A., Kivlighan, K. T., Chen, P., & Laudenslager, M. L. (2011). Maternal salivary cortisol differs by fetal sex during the second half of pregnancy. Psychoneuroendocrinology, 36(4), 588–591. https://doi.org/10.1016/j.psyneuen.2010.09.005.
Eley, T. C., McAdams, T. A., Rijsdijk, F. V., Lichtenstein, P., Narusyte, J., Reiss, D., Spotts, E. L., Ganiban, J. M., & Neiderhiser, J. M. (2015). The intergenerational transmission of anxiety: A Children-of-Twins Study. American Journal of Psychiatry, 172(7), 630–637. https://doi.org/10.1176/appi.ajp.2015.14070818.
Fernandez-Pujals, A. M., Adams, M. J., Thomson, P., McKechanie, A. G., Blackwood, D. H., Smith, B. H., Dominiczak, A. F., Morris, A. D., Matthews, K., Campbell, A., Linksted, P., Haley, C. S., Deary, I. J., Porteous, D. J., MacIntyre, D. J. & & McIntosh, A. M. (2015). Epidemiology and Heritability of Major Depressive Disorder, Stratified by Age of Onset, Sex, and Illness Course in Generation Scotland: Scottish Family Health Study (GS:SFHS).PLoS One, 16, e0142197.
Fransson, E., Sorensen, F., Kallak, T. K., Ramklint, M., Eckerdal, P., Heimgartner, M., Krageloh-Mann, I., & Skalkidou, A. (2020). Maternal perinatal depressive symptoms trajectories and impact on toddler behavior? the importance of symptom duration and maternal bonding. Journal of Affective Disorders, 273, 542–551. https://doi.org/10.1016/j.jad.2020.04.003.
Gartstein, M. A., Bridgett, D. J., Dishion, T. J., & Kaufman, N. K. (2009). Depressed mood and maternal report of child behavior problems: Another look at the depression-distortion hypothesis. Journal of Applied Developmental Psychology, 30(2), 149–160. https://doi.org/10.1016/j.appdev.2008.12.001.
Glasheen, C., Richardson, G. A., Kim, K. H., Larkby, C. A., Swartz, H. A., & Day, N. L. (2013). Exposure to maternal pre- and postnatal depression and anxiety symptoms: risk for major depression, anxiety disorders, and conduct disorder in adolescent offspring. Development and Psychopathology, 25(4 Pt 1), 1045–1063. https://doi.org/10.1017/S0954579413000369.
Glover, V., O’Donnell, K. J., O’Connor, T. G., & Fisher, J. (2018). Prenatal maternal stress, fetal programming, and mechanisms underlying later psychopathology-A global perspective. Development and Psychopathology, 30(3), 843–854. https://doi.org/10.1017/S095457941800038X.
Göbel, A., Stuhrmann, L. Y., Harder, S., Schulte-Markwort, M., & Mudra, S. (2018). The association between maternal-fetal bonding and prenatal anxiety: An explanatory analysis and systematic review. Journal of Affective Disorders, 239, 313–327. https://doi.org/10.1016/j.jad.2018.07.024.
Goodman, S. H. (2020). Intergenerational transmission of depression. Annual Review of Clinical Psychology, 16, 213–238. https://doi.org/10.1146/annurev-clinpsy-071519-113915.
Hayes, A. F. (2013). Introduction to mediation, moderation, and conditional process analysis: a regression-based approach. Guilford Press.
Henrichs, J., Schenk, J. J., Schmidt, H. G., Velders, F. P., Hofman, A., Jaddoe, V. W. V., Verhulst, F. C., & Tiemeier, H. (2009). Maternal pre- and postnatal anxiety and infant temperament. The Generation R Study. Infant and Child Development, 18(6), 556–572. https://doi.org/10.1002/Icd.639.
Henrichs, J., Verfaille, V., Jellema, P., Viester, L., Pajkrt, E., Wilschut, J., van der Horst, H. E., Franx, A., & de Jonge, A., group, I. s. (2019). Effectiveness of routine third trimester ultrasonography to reduce adverse perinatal outcomes in low risk pregnancy (the IRIS study): nationwide, pragmatic, multicentre, stepped wedge cluster randomised trial. BMJ, 367, l5517 https://doi.org/10.1136/bmj.l5517.
Henrichs, J., Verfaille, V., Viester, L., Westerneng, M., Molewijk, B., Franx, A., van der Horst, H., Bosmans, J. E., de Jonge, A., Jellema, P. & Group, I. S. (2016). Effectiveness and cost-effectiveness of routine third trimester ultrasound screening for intrauterine growth restriction: study protocol of a nationwide stepped wedge cluster-randomized trial in The Netherlands (The IRIS Study). BMC Pregnancy Childbirth, 16(1), 310.
Henrichs, J., Rescorla, L., Donkersloot, C., Schenk, J. J., Raat, H., Jaddoe, V. W., Hofman, A., Verhulst, F. C., & Tiemeier, H. (2013). Early vocabulary delay and behavioral/emotional problems in early childhood: the Generation R study. Journal of Speech, Language, and Hearing Research, 56(2), 553–566. https://doi.org/10.1044/1092-4388(2012/11-0169).
Hettema, J. M., Neale, M. C., & Kendler, K. S. (2001). A review and meta-analysis of the genetic epidemiology of anxiety disorders. American Journal of Psychiatry, 158(10), 1568–1578. https://doi.org/10.1176/appi.ajp.158.10.1568.
MacKinnon, N., Kingsbury, M., Mahedy, L., Evans, J., & Colman, I. (2018). The association between prenatal stress and externalizing symptoms in childhood: Evidence from the Avon Longitudinal Study of Parents and Children. Biological Psychiatry, 83(2), 100–108. https://doi.org/10.1016/j.biopsych.2017.07.010.
Mason, Z. S., Briggs, R. D., & Silver, E. J. (2011). Maternal attachment feelings mediate between maternal reports of depression, infant social-emotional development, and parenting stress. Journal of Reproductive and Infant Psychology, 29(4), 382–394. https://doi.org/10.1080/02646838.2011.629994.
Mesman, J., & Groeneveld, M. G. (2018). Gendered parenting in early childhood: Subtle but unmistakable if you know where to look. Child Development Perspectives, 12(1), 22–27. https://doi.org/10.1111/cdep.12250.
Muller, M. E. (1994). A questionnaire to measure mother-to-infant attachment. Journal of Nursing Measurement, 2(2), 129–141. https://www.ncbi.nlm.nih.gov/pubmed/7780768.
Pop, V. J., Komproe, I. H., & van Son, M. J. (1992). Characteristics of the Edinburgh Postnatal Depression Scale in The Netherlands. Journal of Affective Disorders, 26(2), 105–110. https://doi.org/10.1016/0165-0327(92)90041-4.
Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40(3), 879–891. https://doi.org/10.3758/brm.40.3.879.
Reef, J., Diamantopoulou, S., van Meurs, I., Verhulst, F. C., & van der Ende, J. (2011). Developmental trajectories of child to adolescent externalizing behavior and adult DSM-IV disorder: results of a 24-year longitudinal study. Social Psychiatry and Psychiatric Epidemiology, 46(12), 1233–1241. https://doi.org/10.1007/s00127-010-0297-9.
Rees, S., Channon, S., & Waters, C. S. (2019). The impact of maternal prenatal and postnatal anxiety on children’s emotional problems: a systematic review. European Child & Adolescent Psychiatry, 28(2), 257–280. https://doi.org/10.1007/s00787-018-1173-5.
Robinson, M., Mattes, E., Oddy, W. H., Pennell, C. E., van Eekelen, A., McLean, N. J., Jacoby, P., Li, J., De Klerk, N. H., Zubrick, S. R., Stanley, F. J., & Newnham, J. P. (2011). Prenatal stress and risk of behavioral morbidity from age 2 to 14 years: the influence of the number, type, and timing of stressful life events. Development and Psychopathology, 23(2), 507–520. https://doi.org/10.1017/S0954579411000241.
Rogers, A., Obst, S., Teague, S. J., Rossen, L., Spry, E. A., Macdonald, J. A., Sunderland, M., Olsson, C. A., Youssef, G., & Hutchinson, D. (2020). Association between maternal perinatal depression and anxiety and child and adolescent development: A Meta-analysis. JAMA Pediatrics, 174(11), 1082–1092. https://doi.org/10.1001/jamapediatrics.2020.2910.
Rolle, L., Giordano, M., Santoniccolo, F., & Trombetta, T. (2020). Prenatal attachment and perinatal depression: A systematic review. International Journal of Environmenatl Research and Public Health, 17(8). https://doi.org/10.3390/ijerph17082644.
Sandman, C. A., Davis, E. P., Buss, C., & Glynn, L. M. (2011). Prenatal programming of human neurological function. International Journal of Peptides, 2011, 837596 https://doi.org/10.1155/2011/837596.
Spielberger, C. D. (1975). The measurement of state and trait anxiety: conceptual and methodological issues. In L. Levi (Ed.), Emotions—their parameters and measurement. The Raven Press.
Stein, A., Pearson, R. M., Goodman, S. H., Rapa, E., Rahman, A., McCallum, M., Howard, L. M., & Pariante, C. M. (2014). Effects of perinatal mental disorders on the fetus and child. Lancet, 384(9956), 1800–1819. https://doi.org/10.1016/S0140-6736(14)61277-0.
Talge, N. M., Neal, C., Glover, V., Early Stress, Translational Research and Prevention Science Network: Fetal and Neonatal Experience on Child and Adolescent Mental Health (2007). Antenatal maternal stress and long-term effects on child neurodevelopment: how and why? Journal of Child Psychology and Psychiatry, 48(3–4), 245–261. https://doi.org/10.1111/j.1469-7610.2006.01714.x.
Tichelman, E., Westerneng, M., Witteveen, A. B., van Baar, A. L., van der Horst, H. E., de Jonge, A., Berger, M. Y., Schellevis, F. G., Burger, H., & Peters, L. L. (2019). Correlates of prenatal and postnatal mother-to-infant bonding quality: A systematic review. PLoS One, 14(9), e0222998. https://doi.org/10.1371/journal.pone.0222998.
Wittkowski, A., Vatter, S., Muhinyi, A., Garrett, C., & Henderson, M. (2020). Measuring bonding or attachment in the parent-infant-relationship: A systematic review of parent-report assessment measures, their psychometric properties and clinical utility. Clinical Psychology Review, 82, 101906. https://doi.org/10.1016/j.cpr.2020.101906.
Acknowledgements
We gratefully acknowledge the contribution of the participating women, midwives, obstetricians, sonographers, IRIS study data management and research assistants team, and staff at participating midwifery practices and hospitals in the Netherlands as well as of the Perinatal Registry of the Netherlands (Perined) for providing data based on their database. We also gratefully acknowledge the contribution and preparatory work by June Hirschmann.
Funding
This study was funded by the Netherlands Organization for Health Research and Development (ZonMw) as part of the research program Pregnancy and Childbirth, grant number: 209030001.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Consent to Participate
All women included in this study gave written informed consent for participation in both the IRIS study trial and the embedded longitudinal survey.
Ethical Approval
The Dutch Institutional Review Board of the VU Medical University Center Amsterdam has approved the IRIS study and the embedded longitudinal survey (reference numbers: 2013.409 and 2015.033).
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Henrichs, J., de Kroon, M., Walker, A. et al. Maternal Prenatal Distress, Maternal Pre- and Postnatal Bonding and Behavioral and Emotional Problems in Toddlers. A Secondary Analysis of the IRIS Study. J Child Fam Stud 32, 2113–2126 (2023). https://doi.org/10.1007/s10826-022-02529-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-022-02529-1