
Abstract
Callous-unemotional (CU) traits have been linked to more severe and sustained behavior problems among adolescents. The aims of this study were to examine the treatment impact and malleability of CU traits among adolescents and explore potential moderation effects of treatment condition and CU sub-typology. A sample of 159 adolescents (45.9% girls; M age = 14.7 years, SD = 1.47) and their parents participated in a randomized controlled trial of Functional Family Therapy with three assessments (baseline, 6-months and 18-months) of behavior problems, CU traits, prosocial skills and the parent-youth relationship. Latent growth curve model (LGCM) analyses revealed that children with higher CU traits had greater reductions in aggressive and rule-breaking behavior and greater improvements in social skills (|standardized coefficients| = 0.27–0.32). Similarly, higher CU traits were linked to larger increases in parent-ratings of family cohesion and youth-ratings of maternal support (standardized coefficients = 0.26–0.27). Reliable Change Index summaries showed that CU traits remained unchanged for the majority of participants (73.6% and 72.6% had no reliable short- and long-term change, respectively). Baseline anxiety linked to CU sub-typology moderated some of the study results. Findings show that adolescents with co-occurring behavior problems and elevated CU traits can obtain improvement in behavioral and relational outcomes in out-patient treatment. Strikingly, such improvements can occur notwithstanding a limited reduction in CU traits. Future work should investigate whether the treatment gains would be more substantial and stable if treatment adjuncts modifying the CU traits themselves were concurrently deployed.
Highlights
-
CU traits did not diminish the treatment outcomes for youth receiving quality psycho-social interventions in an outpatient setting.
-
CU traits did not predict sustained or reoccurring behavior problems, when youth were assessed at the 18 month follow up.
-
CU traits remained stable across treatment for most youth while showing some level of malleability among those with higher levels of CU traits.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Although several treatment programs have demonstrated an overall effectiveness for youth behavioral problems, there is considerable heterogeneity in this target population with respect to outcomes (Dopp et al., 2017; Sawyer et al., 2015; Weisz et al., 2017, 2019). One possible source of this heterogeneity are individual differences at the trait level, where key characteristics of the adolescent might influence treatment responsiveness and improvement. Knowledge about the associations between individual characteristics and therapy outcome is important to guide optimal or personalized treatments that increase the likelihood of positive gains for each patient (Ng and Weisz, 2015). Callous-unemotional (CU) traits have gained particular attention as a discriminating individual characteristic among children and adolescents with behavior problems as they relate to empathic and emotional limitations associated with higher risk of antisociality (Frick et al., 2014b, 2018). We aimed to assess whether CU traits predict the change in behavioral and relational outcomes and whether CU traits themselves change over time among adolescents in treatment for behavior problems.
Callous-Unemotional (CU) Traits
CU traits are defined by a lack of guilt and remorse, a lack of empathy, an uncaring attitude and shallow affect (Frick and White, 2008). They are akin to the affective dimension of psychopathy and have been proposed as the developmental precursors to adult antisocial personality disorder (Goulter et al., 2019; Viding and Kimonis, 2018). CU traits have been linked to more severe and persistent antisocial behavior and thereby designate a more high-risk subgroup of adolescents with behavior problems (Frick, 2012; Frick et al., 2018; Goulter et al., 2019; McMahon et al., 2010). These traits are associated with neurocognitive vulnerabilities that may help explain the pattern of diminished empathy and concern for others (Viding and McCrory, 2019). Children with high levels of CU traits show reduced amygdala activation when observing people in distress, lowered fear responses, lack of attending to fear and sadness in others and abnormal processing of punishment cues (Dadds et al., 2008; Fairchild et al., 2009; Frick et al., 2003; Hodsoll et al., 2014; Lozier et al., 2014; Viding et al., 2012). Twin studies show a stronger heritability of conduct problems when in combination with high versus low levels of CU traits (Viding et al., 2005, 2008). However, stronger heritability does not equal immutability and there is evidence of parenting factors moderating the biological risk for CU traits (Hyde et al., 2016; Henry et al., 2018), as well as childhood maltreatment leading to CU presentation in some cases (Viding and Kimonis, 2018).
A unique subgroup for conduct problems in children with CU traits has been proposed by Frick (e.g., Frick, 2012). Under the label “with limited prosocial emotions”, CU traits have been included as a specifier for the diagnosis of conduct disorder in DSM-V and for the diagnosis of conduct disorder and oppositional defiant disorder in ICD-11 (American Psychiatric Association, 2013; World Health Organization, 2018).
CU Traits and Treatment Outcomes
Three previous review articles provide somewhat mixed findings related to the associations between CU traits and treatment outcomes, especially with respect to adolescents in different treatment setting (Frick et al., 2014b; D. J. Hawes et al., 2014; Wilkinson et al., 2016). Across these reviews, 20 studies addressed this research question with adolescent samples. Six of these were in an out-patient clinic-based treatment setting, where two found CU traits to predict poorer response to treatment (Dadds et al., 2012; Masi et al., 2013), while the remaining four did not find support for elevated CU traits to predict treatment outcomes (Manders et al., 2013; Masi et al., 2011; Norlander, 2008; White et al., 2013). Comparatively, among the 14 studies conducted in forensic and in-patient settings, the majority found CU traits to predict negative outcomes such as program drop-out, reoffending, rearrests, infractions, and rates of seclusion and restraint (e.g., Falkenbach et al., 2003; Gretton et al., 2001; Hicks et al., 2000; Spain et al., 2004; Stellwagen and Kerig, 2010). Together, these results indicate that the association between CU traits and poorer treatment outcome might be less profound for adolescents receiving outpatient or home-based treatment compared to adolescents in forensic settings. Individualized and tailored high-quality services with a modular or adaptive approach could be able to appropriately assess and address the relevant risk factors and skill deficits needed to reduce both behavior problems and CU traits (Polaschek and Skeem, 2018; Wilkinson et al., 2016). Recommended treatment elements for youth behavior problems such as promoting the therapeutic alliance, treatment motivation and improvement of the parent-youth relationship (particularly parental warmth and positive involvement), appear to have a beneficial impact on the behavior of children and adolescents with conduct problems and CU traits (Mattos et al., 2017; O’Connor et al., 2016; Waller et al., 2013, 2018).
Two potentially influential factors need to be taken into account when studying the relationship between CU traits and treatment outcomes. The first relates to impulsivity, a risk factor for the development and maintenance of behavior problems (Kolko and Pardini, 2010). The second relates to different etiological paths associated with elevated CU trait subtypes. Although CU traits were intended to identify a relatively homogeneous subsample of adolescents with behavior problems, recent research suggests there to be two subtypes of CU traits that differ in their level of emotional reactivity (Craig and Moretti, 2018; Kimonis et al., 2012), with possibly distinct etiology (Viding and Kimonis, 2018). Primary CU traits are assumed to be caused by biological constraints or dysfunctions in the emotional systems, and one possible mechanism might be the increased DNA methylation of areas close to the oxytocin receptor gene (Cecil et al., 2014; Dadds et al., 2013). These dysfunctions manifest as a lack of emotional reactivity, diminished emotional attentiveness and low levels of anxiety (Craig and Moretti, 2018; Dadds et al., 2018; Kimonis et al., 2012). In contrast, secondary CU traits are thought to be acquired from environmental exposure to trauma, abuse and/or neglect where the resulting reactive and negative emotionality is thought to be protective and perceived as a lack of empathy and caring (Kahn et al., 2013). Despite this lack of behavioral expression of emotions, secondary CU traits are associated with hyperreactive emotional systems (Craig and Moretti, 2018; Kimonis et al., 2012), as indicated by signs of dysregulation of the hypothalamic–pituitary–adrenal (HPA) axis (Kimonis et al., 2016). To date we lack empirical evidence as to whether the influence of CU traits on treatment outcomes in adolescents differs between these subtypes.
Change in CU Traits Across Treatments
Equally important to testing how CU traits relate to the success of treatment in improving behavior, is whether psychosocial treatments can lead to reductions in CU traits. This is important when assessing the risk for relapse and recurrent treatment needs, as improvements in mere behavioral manifestations of antisocial tendencies might lead to overoptimistic clinical predictions. There is evidence to suggest that CU traits are malleable for younger children, in particular when the parents are involved in treatments that specifically target CU-specific risk factors (Dadds et al., 2019; Kimonis et al., 2019; Kjøbli et al., 2018; Waller et al., 2013). While some treatment studies in adolescent samples have also reported reductions in CU traits (e.g., Lui et al., 2019; Salekin et al., 2012; Thøgersen et al., 2021), others show more mixed results (Butler, 2011; Fonagy et al., 2018) or no change (Manders et al., 2013; Reddy et al., 2013). The fact that reductions in CU traits are mostly observed in studies without a control group or across treatment conditions, makes it difficult to ascertain that CU traits respond to treatment rather than being a result of time, maturation, or measurement effects. Additionally, previous research reports on group-based change statistics, but lack individual-based change statistics that can inform the rate at which participants experience reliable and clinically meaningful changes in CU (Estrada et al., 2018). It is also important to note that few treatment programs have been developed to specifically target unique CU trait factors (i.e., low parental/maternal warmth, relative punishment insensitivity/reward dominance, and emotional processing deficits). Further research is therefore needed to understand the degree to which CU traits among adolescents are malleable in the context of specific treatment programs, and if any observed changes are clinically meaningful.
Functional Family Therapy
Functional Family Therapy (FFT; Alexander et al., 2013) is a treatment program for adolescent behavior problems where the role of CU traits might be of particular relevance. First, FFT has been implemented in multiple countries based on its status as an evidence-based program (Robbins et al., 2016) and is likely to be offered to numerous adolescents with CU traits in multiple countries. Second, FFT therapists are intensely trained and supervised to work on treatment engagement and motivation, which might counter the lack of treatment motivation associated with CU traits (O’Neill et al., 2003). Third, FFT is specifically focused on ensuring a reduction in blame and negativity and improving family relationships and parent-youth interactions, which might be important protective factors for adolescents with CU traits (Roberts et al., 2017; Wilkinson et al., 2016). Fourth, the emphasis placed on relational and strength-based interventions over consequence-based parenting strategies, is in line with treatment suggestions for children with CU traits (D. J. Hawes and Dadds, 2005). Finally, the assessment-based individualization of treatment interventions and components in FFT should enable therapists to make relevant adjustments to match the needs, risk factors and relational dynamics of each adolescent and family (White et al., 2013).
A planned part of the evaluation of Functional Family Therapy in Norway was therefore to test whether CU traits moderated any observed treatment effects (Ogden, 2013). The study applied a two-armed randomized controlled trial (RCT) design with timepoints for assessment fixed by time at baseline (0 months), post-treatment (6 months) and follow-up (18 months). Participants assigned to the control condition had alternative treatment options such as family counseling, child welfare services and public mental health care available, including other evidence-based treatments (Bjørnebekk et al., 2022; Ogden, 2013).
Current Study
Data from the Norwegian FFT evaluation was used to test the association between CU traits and treatment outcomes for adolescents with behavior problems within the context of out-patient treatment services. This is an important extension of previous research which has primarily studied the relationship between CU traits and treatment outcomes for younger children, samples including both younger children and adolescents or adolescents in forensic settings (Frick et al., 2014b; D. J. Hawes et al., 2014; Waller et al., 2013; Wilkinson et al., 2016). Our goal was to help address the gaps in our understanding by investigating two key questions: 1) Do baseline CU traits predict the success of treatment in improving behavior outcomes; and 2) Do CU traits change over the course of treatment?
Question 1: Do Baseline CU Traits Predict the Success of Treatment in Improving Behavior?
Previous research has provided mixed results with respect to the relationship between CU traits and treatment outcomes (Wilkinson et al., 2016). Findings vary among age groups, treatments provided, treatment settings and the outcome variables in question. In this study, we specifically looked at adolescents that are provided evidence-based treatments or high-quality psychosocial care, in a home- or clinic-based setting. Our primary outcome measures focused on adolescent antisocial and prosocial behavior and our secondary outcome measures focused on the quality of the parent-youth relationship. In addition, we wanted to assess the predictive value of baseline CU traits on treatment satisfaction, a client-centered measure of the quality of the treatment received. Given the inconclusiveness of previous research it is difficult to establish a testable hypothesis related to this research question. The current study therefore represents an exploratory investigation of the relationship between baseline CU traits and treatment outcomes (parental satisfaction with treatment and both short and long-term changes in antisocial behavior and parent-child relationship quality) in a sample of adolescents in treatment for behavior problems.
Question 2: Do CU Traits Change During Treatment?
It is important to study if a trait-level risk factor such as CU traits can be reduced among adolescents in treatment. This will help to better understand future risk of relapse and reoccurring antisocial behavior. As noted earlier, previous research findings are mixed with respect to whether adolescent CU traits change across treatment. Earlier studies have mostly reported on group average changes in CU traits, and it is therefore of interest in this study to assess the clinical significance of observed therapeutic changes in CU traits at an individual level as well. This would allow us to elucidate the number and percentage of study participants that have a clinically meaningful change in their level of CU traits in the context of high-quality treatment.
Do the results depend on treatment condition and CU subtype?
Two important aspects are worthy of further investigation to provide more detailed knowledge about CU traits. First, it is important to increase our empirical knowledge on whether specific treatment options are particularly useful for adolescents with CU traits. The randomized allocation to FFT and the active control condition allowed us to test for differential group effects relating to our research questions. These group comparisons can provide insights on differences between treatment conditions that might be masked by both significant and non-significant results observed in the full sample. Second, we wanted to conduct exploratory analysis as to whether the primary and secondary typology of CU traits moderated the results of the two primary research questions relating to a) the association between baseline CU traits and treatment gains and b) the susceptibility of CU traits to therapeutic change.
Method
Participants
The participants were recruited among families referred to Functional Family Therapy between 2013 and 2018 at three regional and one municipality child welfare organizations comprising both rural and urban settings in Norway. The clinical supervisor of each FFT-team determined eligibility for study inclusion based on referral information from the child welfare worker and an intake meeting with the family. Based on the referral and family information, the supervisor assessed whether the following inclusion criteria were met: a) the adolescent was between 11 and 19 years; and b) the adolescent displayed or were at risk for one or more of the following behavior problems: delinquency, aggressive or violent behavior, verbal aggression or threats, truancy, school-related problem behavior and/or drug use in relation to problem behaviors mentioned above. The inclusion of youth not displaying, but at risk for behavior problems, was based on the supervisor’s clinical assessment of individual, parental, familial and/or contextual risk factors. Standardized measures could be part of the referral information but were not used in the intake meeting. In addition, the supervisor made case-by-case decisions to exclude families from the study based on the presence of one or more of the following exclusion criteria: a) adolescents living by themselves; b) autism diagnosis; c) acute psychotic episode; d) imminent risk of suicide; e) home environments that pose a threat to the therapist’s life or safety; f) ongoing (incomplete) investigation by the local child welfare service; and/or g) concurrent services that were incompatible with commencing FFT-treatment, such as initiating individual psychotherapy for the referred adolescent.
Parents and adolescents were informed by the FFT team supervisor and a research assistant about the study and provided written consent prior to the first data collection. An initial sample of 161 adolescents and their parent(s) consented to the study and two families later revoked their consent. The sample of the current study thus included 159 adolescents (45.9% girls) with a mean age of 14.7 years (SD = 1.47) and their parent(s), 151 mothers (including eight step- and nine foster-mothers) and 90 fathers (including 15 step- and five foster-fathers). The majority of mothers (79.5%) and fathers (92.2%) were working full- or part-time, and 42.6% of the mothers and 34.4% of the fathers had a university or college degree. The mean self-reported annual parental income was approximately 460.000 Norwegian kroner, which is slightly lower than the average annual salary in Norway in 2016, 519.600 Norwegian kroner (Statistics Norway, 2017). There were 22 (13.8%) families who reported receiving some form of financial welfare support. Among the 130 (81.8%) families where either one or both parents were born in Norway, 11 of the youth were not born in Norway. Among the 28 (17.6%) families where the parent(s) were of minority/immigrant background, 15 of the youth were not born in Norway. Data on minority status was missing for 1 (0.6%) family.
Procedures
Data was obtained at three time points: prior to randomization to treatment condition (baseline) and then six (post-treatment) and 18 months (follow-up) after randomization. At each time point, the families met with a research assistant in their home or at a municipality office to complete the study questionnaire on portable computers provided by the research assistant. All questionnaires for parents and adolescents were programmed in the Ci3 software (Sawtooth Software). The research assistant instructed the family on how to use the Ci3 system and provided technical assistance if needed during questionnaire completion. The family received a light snack and a minor monetary compensation (approximately 50 US Dollars) for completing the questionnaires. When both parents completed questionnaires, we selected one main parent respondent per youth based on the highest level of data completeness. In cases where the mother and father data showed the same level of completeness, the maternal response was chosen as the main parent respondent. Only main parent respondent data was included in the analyses.
Measures
Callous-Unemotional Traits
CU traits were measured by the 12-item parent version of the Inventory of Callous-Unemotional traits (ICU; Frick, 2004; Kimonis et al., 2008). The ICU consists of both standard-scored items such as “Seems very cold and uncaring to others” and “Does not care who he/she hurts to get what he/she wants”, and reverse-scored items such as “Feels bad or guilty when he/she does something wrong” and “Tries not to hurt others’ feelings”. Each item is rated on a 4-point scale: 0 (not true at all), 1 (somewhat true), 2 (very true), and 3 (definitively true) and a total score is calculated as the sum of item scores after recoding reverse-scored items. Research on the current and other samples suggests that the unidimensional 12-item short version of the ICU (ICU12) is a reliable and valid measure of CU traits (Hawes et al., 2014; Thøgersen et al., 2020). The reliability of the ICU was acceptable in our sample, α = 0.864, similar to the test-retest reliability of the full scale observed in other samples (Moore et al., 2017). Normative cut-offs for the 24-item parent version of the ICU have been set to 34 for boys and 30 for girls (Kemp et al., 2021).
Antisocial Behaviors
The level of youth antisocial behavior was assessed by parents’ responses on the rule-breaking and aggressive behavior subscales of the Child Behavior Checklist (CBCL) which have considerable research support for their reliability and validity (Achenbach and Rescorla, 2001). The rule-breaking and aggressive subscales comprise of 17 and 18 items, respectively, that are rated on a 3-point scale: 0 (not true), 1 (somewhat or sometimes true), and 2 (very true or often true). In our sample these scales showed acceptable reliabilities, αs = 0.810–0.923.
Prosocial Behaviors
The level of youth prosocial behaviors was measured by parental responses to the Social Skills Rating Scale (SSRS; Gresham and Elliott, 1990). The scale comprises 40 items pertaining to various prosocial behaviors that are rated on a 4-point scale ranging from 1 (never) to 4 (very often). Item scores compile to four separate subscale scores related to Cooperation, Assertion, Self-Control, and Responsibility, as well as a total scale score. The SSRS has shown good psychometric properties in Norwegian adolescent samples and some predictive value for future behavior problems (Gamst-Klaussen et al., 2014; Sørlie et al., 2008). Only the total scale score was used, and it showed acceptable reliability in our sample, α = 0.869.
Parent–youth relationship quality
The quality of the parent-youth relationship was assessed by two measures. The first measure was the Family Environment Scale (FES), where parents and youth separately rate 90 items relating to nine different areas of the family environment as either 0 (not true) or 1 (true) (Moos and Moos, 2009). The cohesion and conflict subscales from both set of responders served as indicators for the quality of the youth-parent relationship. Example items from these subscales are “Family members really help and support one another” and “We fight a lot in our family”, respectively. These scales have typically been found to be the most reliable scales of the FES (Boyd et al., 1997; Taylor et al., 2014) and showed acceptable reliabilities in our sample, αs = 0.724–0.745.
The second measure of the parent-youth relationship was the Inventory of Parent and Peer Attachment-Revised (IPPA; Armsden and Greenberg, 1987; Gullone and Robinson, 2005). IPPA is a self-report measure and comprises 25 items that assess three areas of perceived maternal, paternal and peer security: trust, communication, and alienation (Andretta et al., 2017). Example items from the three subscales with wording related to the maternal relationship are “My mother respects my feelings”, “If my mother knows something is bothering me, she asks me about it” and “Talking over my problems with my mother makes me feel ashamed or foolish”. Each item is rated on a 5-point scale ranging from 1 (Almost never or never true) to 5 (Almost always or always true). Given the high intercorrelation between the factors, they were compiled to three overall indices of youth perceived security in relationship to their mother, father, and peers, respectively. These scales had an acceptable reliability in our sample, αs = 0.931–0.941. One item on the peer scale (‘I get upset a lot more than my friends know about’) had a corrected item-total correlation of −0.047 and was not included in the analyses.
Treatment satisfaction
Treatment satisfaction was rated by parents at the 6 months (post-treatment) time point using a 12-item scale related to the quality of the treatment, information received, family involvement, change and effectiveness (Lubrecht, 1992). Example items are “How do you assess the quality of the treatment you received” and “How effective was this treatment for your family?”. Each item was rated on a 4-point scale ranging from 1 (Excellent) to 4 (Poor), and the total scale reliability in our sample was α = 0.854.
Impulsivity
The level of youth impulsivity was assessed by parent responses to the hyperactivity/impulsivity scale on the Swanson, Nolan, and Pelham—IV questionnaire (SNAP-IV; Swanson et al., 2001). The hyperactivity/impulsivity scale comprises 9 items, that are rated on a 4-point scale from (0) not at all to (3) very much. The reliability of the scale in our sample was good, α = 0.908.
Treatment conditions: Functional family therapy vs. other services
Participants randomized to the FFT condition received an intensive, short-term (3–6 months) family-focused treatment where both the adolescent and his/her parent(s) participated in the therapy sessions. The FFT treatment consists of an assessment-based tailoring of specific interventions spanning across five treatment phases with distinct goals: 1) Engagement to ensure family members participation in sessions; 2) Motivation to decrease the level of blame and negativity in the family and increase hope and motivation for change; 3) Relational Assessment to assess how risk and protective factors and family relational dynamics relate to the behavior problems; 4) Behavior Change to improve family skills such as communication, conflict management and problem solving to reduce problem behavior; and 5) Generalization to maintain and extend skill use inside and outside the family, prevent relapse and refer the family to additional support and services, if needed.
Participants randomized to the control condition were as a minimum referred to the local family counseling service and could access any other treatment or service available to them, including other evidence-based treatments. By parent-report at the six months post-treatment data collection, families in the control condition had utilized the following services: 40.3% (29) Multisystemic Therapy (MST; Henggeler et al., 2009), 40.3% (29) Parent Training/Guidance, 2.8% (2) Child Mental Health Services, 2.8% (2) No Services, with 13.8% (10) missing responses.
Primary and secondary sub-types of CU traits
Parent ratings on the anxious-depressed subscale of the CBCL served as a measure of the emotional hypo- or hyperreactivity linked to the primary and secondary CU trait subtypes, respectively. The 13 items on this subscale relate to whether the child seems fearful, worried, nervous, guilty, and depressed and are rated on a 3-point scale: 0 (not true), 1 (somewhat or sometimes true), and 2 (very true or often true). There is considerable research supporting this scale as a measure of anxiety (Achenbach and Rescorla, 2001) and it has been used in several previous studies on the subtypes of CU traits (Craig et al., 2021; Fanti et al., 2013; Kahn et al., 2013; Kimonis et al., 2011, 2012). In our sample, we observed an acceptable reliability for this scale, α = 0.869.
Analytic Plan
In answer to the first research question of whether CU traits predict treatment outcomes we applied two analytic strategies. Firstly, the degree to which baseline CU-traits predict parental treatment satisfaction was assessed by regression. Secondly, the degree to which baseline CU traits predict changes in the outcome measures was assessed using a latent growth curve model (LGCM) approach applicable to RCTs with three time-points (Mun et al., 2009). LGCMs are suited for studies with repeated measures due to their ability to explicitly model individual change over time, provide more statistical power and make estimates of both the rate and variability of change (Bollen and Curran, 2006; Curran and Muthén, 1999). With the intercept set at baseline in a model conditional on baseline CU traits, we obtained three standardized estimates of how baseline CU traits relate to the selected outcome variable: 1) the association at baseline between CU traits and the outcome measure, 2) the predictive value of baseline CU traits on a short-term slope (rate of change) of the outcome measures from baseline to post-treatment, and 3) the predictive value of baseline CU traits on a long-term slope (rate of change) from baseline to follow-up. A separate model analysis was run for each of the primary and secondary outcome variables (aggressive behavior, rule-breaking behavior, prosocial skills, family cohesion, family conflict and perceived maternal, paternal and peer security). Impulsivity was included as a covariate in each of these LGCM analyses.
To answer the second research question of whether CU traits change over the course of treatment, three analytic strategies were used. Firstly, we used an unconditional LGCM with CU traits as the outcome variable to estimate the level of CU traits at baseline and the short- and long-term change in CU traits. Secondly, we conducted repeated-measures t-tests comparing the mean of CU traits at baseline against the mean at either post-treatment or follow-up. Thirdly, to address the clinical significance of any observed changes we computed individual-based change statistics using the Reliable Change Index (RCI; Jacobson and Truax, 1991). The standard deviation of baseline CU traits and a test-retest reliability value of 0.85 were used in computing the SEdiff (Hawes et al., 2014). The RCI for both short-term and long-term changes in CU traits was calculated, providing information about the proportion of youth that were reliably improving, reliably deteriorating, or showing no reliable change. All analyses relating to this question were run for both the full sample and the subsample of adolescents with baseline CU traits above the normative cut-off levels for the 24-item parent-version of the ICU (Kemp et al., 2021), adapted for use with the 12-item version by dividing each gender-specific cut-off score by two.
To test whether our results differed between the treatment conditions, we added a dummy coded treatment condition variable to each of the initial analytic models. With respect to treatment outcomes, we tested for interaction effects of CU traits and treatment condition. With respect to change in CU traits, the LGCM of CU traits was made conditional on treatment condition, and the individual-based change statistics were calculated separately for each condition and their distribution compared using chi-square statistics with Fisher’s exact test. The same approach was used to explore whether the study results were dependent on CU traits subtypes. Baseline scores on the CBCL anxious-depressed scale were added to each of the initial analytic models as either an interaction term with CU traits or as a covariate. The individual-based change statistics were computed separately for a high (clinical) and a low (borderline or normal) anxiety group based on the multi-cultural, gender and age normed clinical cut-off score of the CBCL anxious-depressed scale (Achenbach and Rescorla, 2007). The distributions of reliable change between these two groups were compared using chi-square statistics with Fisher’s exact test.
Despite sustained efforts to contact and meet with the families, there was some attrition in data collection at both baseline (2 youth reports missing), post-treatment (59 youth and 49 parent-reports missing) and follow-up (61 youth and 52 parent-reports missing). Most cases had data at three time points, 84 (52.8%) and 97 (61.0%) by youth- and parent-report, respectively. Data was missing at one-time point for 29 (18.2%) youth and 21 (13.2%) parents, at two-time points for 44 (27.6%) youth and 41 (25.8%) parents, and completely missing for 2 (1.3%) youth. Cases missing data at a) both post-test and follow-up or b) follow-up were representative of attrition. This was observed for 52 (32.7%) cases using parent data, and 59 (27.3%) cases using youth data. In addition, the two cases missing youth data at baseline and one case missing youth post-test data were regarded as attrition. To assess for the effects of attrition we conducted t-tests on all variables at baseline comparing the means of attrition cases against non-attrition cases.
Given the amount of missing data in our sample, the PCaux-package for R was used to construct principal component auxiliary variables (Lang, et al., 2018), setting the limit of variance to be explained to 50%. The extraction of auxiliaries was done separately for each model tested, where variables that were included in each model were excluded from the calculations extracting the auxiliaries. The regression analyses and LCGM analyses were conducted in Mplus version 8 (Muthén and Muthén, 2017). Maximum likelihood estimation with robust standard errors (MLR) was used for increased robustness with respect to non-normality and non-independence of observations. A multiple imputation (MI) dataset was created using the PCaux-package in R and imported to SPSS version 26 for calculating group-based change statistics. The individual-based change statistics and Fisher’s exact test comparing the distributions of reliable change between treatment condition and CU typology groups, were computed in R version 3.63 using the observed data only.
Results
Descriptive Statistics and Model Fit
The means and standard deviations of the study variables across the three measurement timepoints and any statistically significant differences in the group means across time are presented in Table 1. The fit statistics for the unconditional LGCMs can be seen in the supplementary materials.
Attrition
Statistically significant differences between cases with and without attrition in youth data was observed for two of the 15 tests. Scores on the Social Skills Rating system, t(105) = 2.46, p = 0.008, were lower and parental responses to the Family Cohesion t(150) = −2.32, p = 0.011, were higher at baseline for cases showing attrition for youth data compared to non-attrition cases. Attrition in parent data showed statistically significant differences for two of the 15 tests. A significantly higher percentage of girls (60%) were found in the cases with parental attrition compared to cases without parental attrition (39%), t(157) = −2.45, p = 0.015. Additionally, youth responses to the Family Cohesion scale t(150) = 2.00, p = 0.047, were lower at baseline in families where there was parental attrition.
Question 1: Do Baseline CU Traits Predict the Success of Treatment in Improving Behavior?
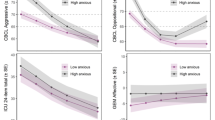
The results of the conditional LGCM analyses showing the relationship between baseline CU traits and a) baseline levels, b) short- and c) long-term change slopes of the treatment outcome variables, with impulsivity as a covariate, are seen in Table 2. For the primary outcomes, baseline CU traits predicted the short-term change on two of three measures and long-term change for all three measures. CU traits were predictive of greater reduction in antisocial behavior and greater increases in prosocial behavior. For the secondary outcomes related to the quality of the parent-youth relationship, baseline CU traits predicted more positive short-term change in two of seven outcome variables, and more positive long-term change in two of seven variables. The regression of treatment satisfaction on baseline CU traits was non-significant, with a pooled estimated regression coefficient of 0.02, SE = 0.17, p = 0.90. These findings suggest that baseline levels of CU traits predict greater behavioral improvements with respect to the primary outcomes in this sample. For the changes on the secondary outcome measures and treatment satisfaction, baseline CU traits were mostly not predictive.
Question 2: Do CU Traits Change During Treatment?
Full-sample analyses
First, the unconditional LGCM with CU traits as the outcome variable showed adequate model fit (X2 = 1.26, df = 2, p = 0.532; CFI = 1.00; RMSEA = 0.00, 90CI: [0.00, 0.14], SRMR = 0.05). The estimated mean of CU traits at baseline was 15.95, SE = 0.58. p < 0.001, the estimated short--term change was −1.19, SE = 0.82, p = 0.15, and the estimated long-term change was −0.72, SE = 1.04, p = 0.49. These results did not support the hypothesis that CU traits change during treatments. Second, repeated measures t-tests comparing the level of CU traits at baseline (M = 15.93, SD = 7.34) to post-treatment (M = 14.17, SD = 7.37) and follow-up (M = 12.64, SD = 6.72) values were statistically significant, t(379) = 2.54, p = 0.015 and t(465) = 2.09, p = 0.037, respectively. The mean score reductions on the ICU12 in the MI dataset were 3.06 and 2.51 scale points for the short- and long-term change, respectively, providing some support for CU change across treatment. Third, the individual-based change statistics was calculated using the observed data available (n = 106 for both short- and long-term change). From baseline to post-treatment assessment, 73.6% (78) had no reliable change, 17.0% (18) had a reliable decrease and 9.4% (10) had a reliable increase in their CU traits. For the long-term 18-month period, 72.6% (77) had no reliable change, 20.8% (22) had a reliable decrease and 6.6% (7) had a reliable increase. The net number of youth with a reliable decrease in CU traits were thus 8 for short-term change and 15 for long-term change. Collectively, these findings provide limited support for the hypothesis that CU traits change across treatment. A plot of the change from baseline to follow-up is illustrated in Fig. 1.

Clinical significance plot of CU traits comparing baseline to 18-month follow-up. Evolution of CU traits for each participant from baseline to 18-month follow-up. The middle diagonal line represents equal baseline and follow-up scores and the gray shaded area around it represents the area of no reliable change. Beyond the shaded area, the lower right triangle area represents reliable improvement, while upper left triangle area represents reliable deterioration
Subsample analyses
The previous analyses pertaining to change in CU traits were rerun in the subsample of 77 youth (36 boys and 41 girls) with CU traits above the 12-item adjusted normative cut-off score. First, the LGCM analysis provided estimates of baseline mean and short- and long-term change to be 21.71, SE = 0.55, p < 0.001, −3.45, SE = 1.31, p = 0.008 and −2.20, SE = 2.06, p = 0.29, respectively. These results show that among this subgroup, there is a significant short-term change in CU traits, but a non-significant long-term change. Second, the repeated measures t-tests showed that the short- and long-term changes in CU traits were more pronounced in this subsample with a mean short-term difference of −6.71 scale points, t(455) = 4.41, p < 0.001 and a mean long-term difference of −6.72 scale points, t(593) = 4.33, p < 0.001. These findings were in line with the hypothesis that CU traits change over treatment. Third, individual change statistics in this subgroup showed that the observed short-term change was not reliable for 41 youth, reliably decreasing for 15 youth and reliably increasing for one youth. The observed long-term change in this group was not reliable for 33 youth, reliably decreasing for 20 youth and reliably increasing for none. Collectively, these findings provided partial support for the hypothesis that CU traits change across treatment.
Treatment condition
When treatment condition was added as either a covariate or moderator into the previous analytic models, it consistently failed to reach statistical significance. For instance, the p-values of the standardized coefficients for the CUxCondition term on the change slopes ranged from p = 0.14 (coefficient = −0.21, SE = 0.14) for the long-term change slope for youth-reported family conflict, to p = 0.99 (coefficient = 0.00, SE = 0.16) for the long-term change slope for aggressive behavior. When included in the LGCM of CU traits, the estimated coefficients for the effects of treatment condition on short- and long-term change were 0.65, SE = 1.24, p = 0.602 and −1.24, SE = 1.55, p = 0.424, respectively. Fisher’s exact test comparing the distribution of reliable change categories between the two treatment conditions was non-significant both short-term, p = 0.693, and long-term, p = 0.755. For additional details related to treatment condition, see the supplementary materials.
Primary vs. secondary CU traits
The exploration of whether baseline levels of anxiety had a relation to the study results, yielded non-significant findings for the most part. Only two of the coefficients estimated for the interaction term of CU traits and anxiety on change slopes indicated possible moderation effects. For the long-term change slope for rule breaking behavior the estimated standardized coefficient of the interaction term was 0.26, SE = 0.11, p = 0.013, and for the long-term change slope for social skills, it was −0.20, SE = 0.09, p = 0.028. Probing of these interactions showed that for participants with baseline levels of anxiety in the normal or borderline range according to the multicultural norms (Achenbach and Rescorla, 2007), CU traits were significantly related to the long-term reductions in rule breaking behavior, −0.41, SE = 0.14, p = 0.004, and long-term increases in social skills, 0.36, SE = 0.12, p = 0.005. Among those with baseline anxiety scores in the clinical range, the standardized coefficients were non-significant, −0.05, SE = 0.14, p = 0.734 and 0.14, SE = 0.16, p = 0.384, for the long-term change on rule breaking and social skills respectively. For all other change slopes, the significance of the standardized coefficients of the interaction term ranged from p = 0.06 (0.16, SE = 0.09) for the short-term change in youth-reported family cohesion to p = 0.99 (0.00, SE = 0.09) for long-term change in maternal support. When included in the LGCM of CU traits, the estimated coefficients for the effect of baseline anxiety on short- and long-term change were 0.05, SE = 0.11, p = 0.665 and −0.09, SE = 0.14, p = 0.503, respectively. Fisher’s exact test comparing the distribution of reliable change categories between the low and high anxiety groups was non-significant both short-term, p = 0.447, and long-term, p = 0.543. These results point to the predictive value of CU traits and the malleability of CU traits not to differ by the primary and secondary sub-typology. For additional details and plots related to probing of the interactions, see the supplementary materials.
Discussion
Adolescents with behavior problems and elevated CU traits show more severe and persistent antisocial behavior (Frick et al., 2014b). The underlying risk factors and mechanisms associated with CU traits in adolescents might attenuate the responsiveness to treatments aimed at reducing behavior problems (Frick et al., 2014a, 2018; Wilkinson et al., 2016). In the current study, we examined the relationship between CU traits and treatment outcomes in a sample of 159 adolescents participating in a two-armed RCT of FFT treatment against an alternative treatments control condition. An LCGM-framework was used to address two research questions: 1) Do baseline CU traits predict the success of treatment in improving behavior?; and 2) Do CU traits change during treatment? Additionally, we tested the effect of treatment conditions by comparing FFT to the active treatments control condition. In exploratory analyses, we also tested whether baseline levels of anxiety, as an indicator of CU typology, distinctly influenced our findings.
Although we found CU traits to be associated with more aggression, rule-breaking behavior, and lower social skills at baseline, they did not negatively predict short- or long-term gains on these measures in either of the treatment groups. On the contrary, we observed that CU traits were related to larger reductions in aggressive and rule breaking behavior, and larger increases in prosocial behavior, parent-reported family cohesion and perceived maternal support across the two treatment groups. Previous research has also shown more positive change in measured outcomes in relation to CU traits (Fonagy et al., 2018; Manders et al., 2013; White et al., 2013). The increased gains related to maternal support found in our study are interesting, as reduced maternal support has been associated with CU traits in prior studies (Pardini et al., 2007). The active treatment types received by the youth in this study, might thus not only be less negatively impacted by CU traits, but also have the ability to change CU-specific risk factors. This is in line with research where highly specialized interventions for youth with CU traits show promising results and counter the notion that CU traits always attenuate treatment results (Kimonis et al., 2019; Salekin et al., 2012; Silva et al., 2020).
The observed increased positive changes for adolescents with elevated CU traits might in part be driven by regression to the mean effects or limitations in the possible range of improvement for those with less severe levels of CU traits and antisocial behavior. Nevertheless, the results indicate that youth with CU traits can benefit from established psycho-social interventions, provided that these are intensive and individualized high-quality treatments focused on treatment engagement, motivation, tailoring and improving parental warmth and family collaboration (Frick et al., 2014b; Polaschek and Skeem, 2018; Silva et al., 2020; Wilkinson et al., 2016). It is of note that much of the research reporting reduced treatment response in adolescents with elevated CU traits, has been conducted in forensic, institutional, or residential settings (e.g., Falkenbach et al., 2003; Gretton et al., 2001; Spain et al., 2004). In these contexts, several additional risk factors might account for poorer treatment outcomes among adolescents with elevated CU traits (e.g., negative peer influence, lack of family/parental support, challenges in adequately tailoring treatment to individual needs).
Although antisocial behavior, family cohesion and maternal support all improved following treatment in those with high levels of CU traits, the CU traits themselves showed only limited change. Both the growth model and reliable change index analyses indicated that for the majority of the study participants, the level of CU traits remained at the same level. These results suggest that for most individuals, CU traits are relatively stable in adolescence across an 18-month period, even in the context of active treatment. This supports previous longitudinal studies on the stability of CU traits in adolescents (van Baardewijk et al., 2011; López-Romero et al., 2014; Muñoz and Frick, 2007), and is in line with the results from treatment studies of the MST program (Butler, 2011; Fonagy et al., 2018). These findings are at odds with the statistically significant reductions observed when applying more traditional group-based change statistics (Lui et al., 2019; Manders et al., 2013; Salekin et al., 2012). The clinical meaningfulness of such statistically significant findings needs to be assessed, as the observed average reduction in our study of a couple of scale points can occur by a minimal 1-scale-point change on merely two or three questions on the ICU12. Furthermore, it seems that baseline levels of CU traits might be a moderator of CU change, as our results, and those of a previous study, observed more pronounced reductions in CU traits for adolescents with elevated baseline levels of CU traits (Thøgersen et al., 2021). Importantly, the growth curve analysis indicate that these reductions might be temporary, and the observed short-term effects could be driven by regression to the mean effects. This suggests that long-term reductions in CU traits might only be obtainable with more targeted or prolonged treatments. It could very well be that current treatment approaches for adolescent behavior problems do not assess and target CU traits appropriately, and new approaches need to be developed and tested to ensure effective interventions for sustained reductions in CU traits (e.g., Silva et al., 2019, 2020). More research is therefore needed to shed light on how treatment adjuncts might effectively target change in CU traits, and how these reductions might in turn be maintained over time to lower the future risk of antisocial behavior.
We observed no indication that our findings differed between the treatment conditions. This implies that FFT provided neither better nor worse outcomes for adolescents with CU traits when compared to the alternative treatments available in Norway. Although there might be plausible theoretical advantages of using the FFT approach to work with youth with CU traits (Thøgersen et al., 2021; White et al., 2013), these were not empirically observed in the current study when FFT was compared to other high-quality treatment options. This might be due to the fact that some of the treatments provided in the control condition (e.g., MST and parent management training) have treatment foci and interventions similar to that of FFT. Further research is needed to better understand how treatments for behavior problems can be even more optimized for adolescents with CU traits. It would be important to specifically identify the treatment interventions or adjuncts that are relevant and effective in relation to the distinct emotional and empathic limitations associated with CU traits. One could investigate whether there are elements in existing evidence-based programs that are particularly effective for those with CU traits, conduct detailed studies of the therapeutic change processes (e.g., Mattos et al., 2017) or develop and test novel intervention approaches that focus more specifically on CU specific risk factors (e.g., Kimonis et al., 2019; Silva et al., 2020).
Moreover, the relationship between CU traits and treatment outcomes did not seem to differ much between the two proposed sub-typologies of CU traits. Significant interaction terms were only observed in relation to the long-term change slopes for rule breaking behavior and social skills. Closer inspection of these interactions revealed that the effect of CU traits on the change slopes was significant only at low levels of anxiety, and not at high levels of anxiety. Change slopes plots for the low anxiety – low CU and low anxiety – high CU groups showed that the greater improvement of the latter could be due to more extreme baseline scores in the latter and restrictions in the range of potential improvement in the former group. The interactions did not suggest a differential effect of traditional treatments between groups representing primary and secondary CU types. To our knowledge no previous treatment study of adolescents with CU traits have tested whether results differed by CU typology. One study of adults found no difference in treatment outcomes when comparing primary and secondary psychopaths (Poythress et al., 2010). This suggests that the distinction between primary and secondary CU traits might have implications related to assessment and treatment goals but might not necessarily impact the treatment outcomes of adolescents receiving currently available treatments (Polaschek and Skeem, 2018).
Despite its strengths as a two-armed randomized controlled trial with three time-points, well-validated measures and multiple informants, this study had several limitations. First, we included questionnaire-based measures of CU traits, but no measure of other dimensions of psychopathy, such as narcissism and impulsivity, nor independent rating of CU traits. It might be that multidimensional and/or clinician-/observer-rated measures of psychopathy would have been related to reduced treatment outcomes. Second, our analysis relied on anxiety as indication of CU typology, but this may not be the best indicator for secondary type CU traits. These results cannot rule out potentially differential effects of CU trait typologies based on measures more specifically related to trauma history. However, subtyping on anxiety corresponds with the original primary versus secondary distinction of psychopathy and trauma history is not unequivocally associated with CU traits combined with high emotionality/anxiety (Cecil et al., 2017). Lastly, we cannot completely rule out the possibility that effects related to floor/ceiling of measures or regression to the mean might in part contribute to the increased improvements in outcomes observed in relation to elevated CU traits.
Further work is needed to advance our knowledge on the interaction between CU traits and treatment. Adolescents with elevated levels of CU traits are likely to remain a group with increased risk for future problems, and it is important to understand the impact of CU traits on more distal treatment outcomes such adult educational achievement, work status, criminality, and drug use. Furthermore, it is relevant to test whether prolonged treatment or additional treatment components could lower the risk for long-term negative outcomes and relapse. There is also a need to develop and test interventions specifically aimed at reducing CU traits. These might serve as stand-alone or adjunct treatments components to further enhance treatment benefits and support a prosocial developmental pathway. Recent advances in developing interventions specifically tailored to adolescents with CU traits are promising (Reddy et al., 2013; Salekin et al., 2012; Silva et al., 2019, 2020), and identifying the effective components and long-term outcomes of these approaches in larger randomized trials warrant investigation.
The identification of CU traits as a specific developmental etiology of behavioral expressions of conduct problems can help make advances in both research and clinical practice (Beauchaine and Hinshaw, 2020). The results of the current study support the notion that reductions in adolescent behavior problems are possible even in the context of elevated CU traits, when appropriate care is provided (Polaschek and Skeem, 2018; Silva et al., 2020; Wilkinson et al., 2016). Importantly, behavioral improvements were not reliant on changes in CU traits themselves. This suggests that interventions aimed at changing problematic outcomes in developmental processes in the behavioral and interpersonal domain might be effective, even if the associated risk factor related to emotional processing (here elevated CU traits) is in and of itself more resistant to change (Blair et al., 2014; Dadds et al., 2018; Frick, 2016). More specifically, adolescents with CU traits might be well capable of learning to improve their interpersonal skills, prioritize prosocial goal achievement, strengthen their inhibitory control, and perform logical perspective taking. Such skill developments could help reduce future antisocial and increase prosocial behaviors despite the limitations in recognizing and processing prosocial emotions. CU traits might therefore be neither a necessary nor sufficient criteria for sustained behavior problems in adolescents receiving appropriate treatment.
Data Availability
Due to the nature of this research, study participants did not agree for their data to be shared publicly, so supporting data is not available.
References
Achenbach, T. M., & Rescorla, L. (2007). Multicultural supplement to the manual for the ASEBA school-age forms & profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth & Families.
Achenbach, T. M., & Rescorla, L. A. (2001). Manual for ASEBA school-age forms & profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth & Families.
Alexander, J. F., Waldron, H. B., Robbins, M. S., & Neeb, A. A. (2013). Functional family therapy for adolescent behavior problems. Washington, DC: American Psychological Association.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (DSM-5®). Washington, DC: American Psychiatric Publications.
Andretta, J. R., McKay, M. T., Harvey, S. A., & Perry, J. L. (2017). Inventory of parent and peer attachment-revised scores in adolescents: A psychometric and person-oriented study. Family Relations, 66(3), 527–540. https://doi.org/10.1111/fare.12252.
Armsden, G. C., & Greenberg, M. T. (1987). The inventory of parent and peer attachment: Individual differences and their relationship to psychological well-being in adolescence. Journal of Youth and Adolescence, 16(5), 427–454. https://doi.org/10.1007/bf02202939.
van Baardewijk, Y., Vermeiren, R., Stegge, H., & Doreleijers, T. (2011). Self-reported psychopathic traits in children: Their stability and concurrent and prospective association with conduct problems and aggression. Journal of Psychopathology and Behavioral Assessment, 33(2), 236–245. https://doi.org/10.1007/s10862-010-9215-4.
Beauchaine, T. P., & Hinshaw, S. P. (2020). RDoC and psychopathology among youth: Misplaced assumptions and an agenda for future research. Journal of Clinical Child & Adolescent Psychology, 49(3). https://doi.org/10.1080/15374416.2020.1750022.
Bjørnebekk, G., Olseth, A. R. & Hagen, K. A. (2022). The effectiveness of Functional Family Therapy in Norwegian Child Welfare Services.
Blair, R. J. R., Leibenluft, E., & Pine, D. S. (2014). Conduct disorder and callous-unemotional traits in youth. The New England Journal of Medicine, 371(23), 2207–2216. https://doi.org/10.1056/nejmra1315612.
Bollen, K. A., & Curran, P. J. (2006). Latent curve models: A structural equation perspective. New York: Wiley.
Boyd, C. P., Gullone, E., Needleman, G. L., & Burt, T. (1997). The Family Environment Scale: reliability and normative data for an adolescent sample. Family Process, 36(4), 369–373. https://doi.org/10.1111/j.1545-5300.1997.00369.x.
Butler, S., Baruch, G., Hickey, N., & Fonagy, P. (2011). A randomized controlled trial of multisystemic therapy and a statutory therapeutic intervention for young offenders. Journal Of The American Academy Of Child & Adolescent Psychiatry, 50(12), 1220–1235.
Cecil, C. A. M., McCrory, E. J. P., Barker, E. D., Guiney, J., & Viding, E. (2017). Characterising youth with callous-unemotional traits and concurrent anxiety: evidence for a high-risk clinical group. European Child & Adolescent Psychiatry, 140(1), 1–14. https://doi.org/10.1007/s00787-017-1086-8.
Cecil, C. A. M., Lysenko, L. J., Jaffee, S. R., Pingault, J. B., Smith, R. G., Relton, C. L., Woodward, G., McArdle, W., Mill, J., & Barker, E. D. (2014). Environmental risk, Oxytocin Receptor Gene (OXTR) methylation and youth callous-unemotional traits: a 13-year longitudinal study. Molecular Psychiatry, 19(10), 1071–1077. https://doi.org/10.1038/mp.2014.95.
Craig, S. G., & Moretti, M. M. (2018). Profiles of primary and secondary callous-unemotional features in youth: The role of emotion regulation. Development and Psychopathology, 7, 1–12. https://doi.org/10.1017/s0954579418001062.
Craig, S. G., Goulter, N., & Moretti, M. M. (2021). A systematic review of primary and secondary callous-unemotional traits and psychopathy variants in youth. Clinical Child and Family Psychology Review, 24(1), 65–91. https://doi.org/10.1007/s10567-020-00329-x.
Curran, P. J., & Muthén, B. O. (1999). The application of latent curve analysis to testing developmental theories in intervention research. American Journal of Community Psychology 27(4), 567–595. https://doi.org/10.1023/A:1022137429115.
Dadds, M. R., Masry, Y. E., Wimalaweera, S., & Guastella, A. J. (2008). Reduced eye gaze explains “fear blindness” in childhood psychopathic traits. Journal Of The American Academy Of Child & Adolescent Psychiatry, 47(4), 455–463. https://doi.org/10.1097/chi.0b013e31816407f1.
Dadds, M. R., Cauchi, A. J., Wimalaweera, S., Hawes, D. J., & Brennan, J. (2012). Outcomes, moderators, and mediators of empathic-emotion recognition training for complex conduct problems in childhood. Psychiatry Research, 199(3), 201–207. https://doi.org/10.1016/j.psychres.2012.04.033.
Dadds, M. R., Kimonis, E. R., Schollar-Root, O., Moul, C., & Hawes, D. J. (2018). Are impairments in emotion recognition a core feature of callous–unemotional traits? Testing the primary versus secondary variants model in children. Development and Psychopathology, 30(1), 67–77. https://doi.org/10.1017/s0954579417000475.
Dadds, M. R., English, T., Wimalaweera, S., Schollar-Root, O., & Hawes, D. J. (2019). Can reciprocated parent-child eye gaze and emotional engagement enhance treatment for children with conduct problems and callous-unemotional traits: a proof-of-concept trial. Journal of Child Psychology and Psychiatry, 60(6), 676–685. https://doi.org/10.1111/jcpp.13023.
Dadds, M. R., Moul, C., Cauchi, A., Dobson-Stone, C., Hawes, D. J., Brennan, J., & Ebstein, R. E. (2013). Methylation of the oxytocin receptor gene and oxytocin blood levels in the development of psychopathy. Development and Psychopathology, 26(1), 33–40. https://doi.org/10.1017/s0954579413000497.
Dopp, A. R., Borduin, C. M., White, M. H., & Kuppens, S. (2017). Family-based treatments for serious juvenile offenders: A multilevel meta-analysis. Journal of Consulting and Clinical Psychology, 85(4), 335–354. https://doi.org/10.1037/ccp0000183.
Estrada, E., Ferrer, E., & Pardo, A. (2018). Statistics for evaluating pre-post change: relation between change in the distribution center and change in the individual scores. Frontiers in Psychology, 9, 2696 https://doi.org/10.3389/fpsyg.2018.02696.
Fairchild, G., Goozen, S. H. M. V., Calder, A. J., Stollery, S. J., & Goodyer, I. M. (2009). Deficits in facial expression recognition in male adolescents with early-onset or adolescence-onset conduct disorder. Journal of Child Psychology and Psychiatry, 50(5), 627–636. https://doi.org/10.1111/j.1469-7610.2008.02020.x.
Falkenbach, D. M., Poythress, N. G., & Heide, K. M. (2003). Psychopathic features in a juvenile diversion population: reliability and predictive validity of two self-report measures. Behavioral Sciences & the Law, 21(6), 787–805. https://doi.org/10.1002/bsl.562.
Fanti, K. A., Demetriou, C. A., & Kimonis, E. R. (2013). Variants of callous-unemotional conduct problems in a community sample of adolescents. Journal of Youth and Adolescence, 42(7), 964–979. https://doi.org/10.1007/s10964-013-9958-9.
Fonagy, P., Butler, S., Cottrell, D., Scott, S., Pilling, S., Eisler, I., Fuggle, P., Kraam, A., Byford, S., Wason, J., Ellison, R., Simes, E., Ganguli, P., Allison, E., & Goodyer, I. M. (2018). Multisystemic therapy versus management as usual in the treatment of adolescent antisocial behavior (START): a pragmatic, randomised controlled, superiority trial. The Lancet. Psychiatry,, 5(2), 119–133. https://doi.org/10.1016/s2215-0366(18)30001-4.
Frick, P. J. (2012). Developmental pathways to conduct disorder: implications for future directions in research, assessment, and treatment. Journal of Clinical Child & Adolescent Psychol, 41(3), 378–389.
Frick, P. J. (2016). Current research on conduct disorder in children and adolescents. South African Journal of Psychology, 46(2), 160–174. https://doi.org/10.1177/0081246316628455.
Frick, P. J., & White, S. F. (2008). Research review: the importance of callous-unemotional traits for developmental models of aggressive and antisocial behavior. Journal of Child Psychology and Psychiatry, 49(4), 359–375. https://doi.org/10.1111/j.1469-7610.2007.01862.x.
Frick, P. J., Ray, J. V., Thornton, L. C., & Kahn, R. E. (2014b). Annual Research Review: A developmental psychopathology approach to understanding callous‐unemotional traits in children and adolescents with serious conduct problems. Journal of Child Psychology and Psychiatry, 55(6), 532–548. https://doi.org/10.1111/jcpp.12152.
Frick, P. J., Ray, J. V., Thornton, L. C., & Kahn, R. E. (2014a). Can callous-unemotional traits enhance the understanding, diagnosis, and treatment of serious conduct problems in children and adolescents? A comprehensive review. Psychological Bulletin, 140(1), 1–57. https://doi.org/10.1037/a0033076.
Frick, P. J., Cornell, A. H., Bodin, S. D., Dane, H. E., Barry, C. T., & Loney, B. R. (2003). Callous-unemotional traits and developmental pathways to severe conduct problems. Journal of Abnormal Psychology, 39(2), 246–260.
Frick, P. J. (2004). Inventory of callous–unemotional traits. Unpublished rating scale.
Frick, P. J., Robertson, E. L., & Clark, J. E. (2018). Callous-unemotional traits. In. M. M. Martell (Ed.) Developmental pathways to disruptive, impulse-control and conduct disorders (pp. 139–160). London, UK: Academic Press. https://doi.org/10.1016/b978-0-12-811323-3.00006-7.
Gamst-Klaussen, T., Rasmussen, L.-M. P., Svartdal, F., & Strømgren, B. (2014). Comparability of the social skills improvement system to the social skills rating system: A Norwegian study. Scandinavian Journal of Educational Research, 60(1), 20–31. https://doi.org/10.1080/00313831.2014.971864.
Goulter, N., McMahon, R. J., Pasalich, D. S., & Dodge, K. A. (2019). Indirect effects of early parenting on adult antisocial outcomes via adolescent conduct disorder symptoms and callous-unemotional traits. Journal of Clinical Child and Adolescent Psychology, 1–13. https://doi.org/10.1080/15374416.2019.1613999.
Gresham, F. M., & Elliott, S. N. (1990). Social skills rating system. Manual. Circle Pines, MN: American Guidance Service.
Gretton, H. M., Mcbride, M., Hare, R. D., O’Shaughnessy, R., & Kumka, G. (2001). Psychopathy and recidivism in adolescent sex offenders. Criminal Justice and Behavior, 28(4), 427–449. https://doi.org/10.1177/009385480102800403.
Gullone, E., & Robinson, K. (2005). The Inventory of Parent and Peer Attachment-Revised (IPPA-R) for children: A psychometric investigation. Clinical Psychology & Psychotherapy, 12(1), 67–79. https://doi.org/10.1002/cpp.433.
Hawes, D. J., & Dadds, M. R. (2005). The treatment of conduct problems in children with callous-unemotional traits. Journal of Consulting and Clinical Psychology, 73(4), 737–741. https://doi.org/10.1037/0022-006x.73.4.737.
Hawes, D. J., Price, M. J., & Dadds, M. R. (2014). Callous-unemotional traits and the treatment of conduct problems in childhood and adolescence: A comprehensive review. Clinical Child and Family Psychology Review, 17(3), 248–267. https://doi.org/10.1007/s10567-014-0167-1.
Hawes, S. W., Byrd, A. L., Henderson, C. E., Gazda, R. L., Burke, J. D., Loeber, R., & Pardini, D. A. (2014). Refining the parent-reported Inventory of Callous–Unemotional Traits in boys with conduct problems. Psychological Assessment, 26(1), 256–266. https://doi.org/10.1037/a0034718.
Henggeler, S. W., Schoenwald, S. K., Borduin, C. M., Rowland, M. D. & Cunningham, P. B. (2009). Multisystemic therapy for antisocial behavior in children and adolescents, Second Edition. New York: Guilford Press.
Henry, J., Dionne, G., Viding, E., Vitaro, F., Brendgen, M., Tremblay, R. E., & Boivin, M. (2018). Early warm‐rewarding parenting moderates the genetic contributions to callous–unemotional traits in childhood. Journal of Child Psychology and Psychiatry, 59(12), 1282–1288. https://doi.org/10.1111/jcpp.12918.
Hicks, M. M., Rogers, R., & Cashel, M. (2000). Predictions of violent and total infractions among institutionalized male juvenile offenders. The Journal of the American Academy of Psychiatry and the Law, 28(2), 183–190.
Hodsoll, S., Lavie, N., & Viding, E. (2014). Emotional attentional capture in children with conduct problems: the role of callous-unemotional traits. Frontiers in Human Neuroscience, 8, 570 https://doi.org/10.3389/fnhum.2014.00570.
Hyde, L. W., Waller, R., Trentecosta, C. J., Shaw, D. D., Neiderhiser, J. M., & Ganiban, J. M., et al. (2016). Heritable and nonheritable pathways to early callous-unemotional behaviors. American Journal of Psychiatry, 173(9), 903–910. https://doi.org/10.1176/appi.ajp.2016.15111381.
Jacobson, N. S., & Truax, P. (1991). Clinical significance: a statistical approach to defining meaningful change in psychotherapy research. Journal of Consulting and Clinical Psychology, 59(1), 12–19. https://doi.org/10.1037//0022-006x.59.1.12.
Kahn, R. E., Frick, P. J., Youngstrom, E. A., Youngstrom, J. K., Feeny, N. C., & Findling, R. L. (2013). Distinguishing primary and secondary variants of callous-unemotional traits among adolescents in a clinic-referred sample. Psychological Assessment, 25(3), 966–978. https://doi.org/10.1037/a0032880.
Kemp, E. C., Frick, P. J., Matlasz, T. M., Clark, J. E., Robertson, E. L., Ray, J. V., Thornton, L. C., Wall Myers, T. D., Steinberg, L., & Cauffman, E. (2021). Developing cutoff scores for the inventory of callous-unemotional traits (ICU) in justice-involved and community samples. Journal of Clinical Child and Adolescent Psychology. https://doi.org/10.1080/15374416.2021.1955371.
Kimonis, E. R., Skeem, J. L., Cauffman, E., & Dmitrieva, J. (2011). Are secondary variants of juvenile psychopathy more reactively violent and less psychosocially mature than primary variants? Law and Human Behavior, 35(5), 381–391. https://doi.org/10.2307/41489008?ref=search-gateway:4c9e1d8068250fcebd99519c38a504c0.
Kimonis, E. R., Frick, P. J., Cauffman, E., Goldweber, A., & Skeem, J. (2012). Primary and secondary variants of juvenile psychopathy differ in emotional processing. Development and Psychopathology, 24(3), 1091–1103. https://doi.org/10.1017/s0954579412000557.
Kimonis, E. R., Goulter, N., Hawes, D. J., Wilbur, R. R., & Groer, M. W. (2016). Neuroendocrine factors distinguish juvenile psychopathy variants. Developmental Psychobiology, 59(2), 161–173. https://doi.org/10.1002/dev.21473.
Kimonis, E. R., Frick, P. J., Skeem, J. L., Marsee, M. A., Cruise, K., Munoz, L. C., Aucoin, K. J., & Morris, A. S. (2008). Assessing callous-unemotional traits in adolescent offenders: Validation of the Inventory of Callous-Unemotional Traits. International Journal of Law and Psychiatry, 31(3), 241–252. https://doi.org/10.1016/j.ijlp.2008.04.002.
Kimonis, E. R., Fleming, G., Briggs, N., Brouwer-French, L., Frick, P. J., Hawes, D. J., Bagner, D. M., Thomas, R., & Dadds, M. (2019). Parent-child interaction therapy adapted for preschoolers with callous-unemotional traits: an open trial pilot study. Journal of Clinical Child & Adolescent Psychology, 48(sup1), S347–S361. https://doi.org/10.1080/15374416.2018.1479966.
Kjøbli, J., Zachrisson, H. D., & Bjørnebekk, G. (2018). Three randomized effectiveness trials — one question: can callous-unemotional traits in children be altered? Journal of Clinical Child & Adolescent Psychology, 47(3), 436–443. https://doi.org/10.1080/15374416.2016.1178123.
Kolko, D. J., & Pardini, D. A. (2010). ODD dimensions, ADHD, and Callous-Unemotional Traits as predictors of treatment response in children with disruptive behavior disorders. Journal of Abnormal Psychology, 119(4), 713–725. https://doi.org/10.1037/a0020910.
Lang, K. M., Little, T. D., Chesnut, S., Gupta, V., Jung, B. & Panko, P. (2018). PcAux: Automatically extract auxiliary features for simple, principled missing data analysis [R Package] Version: 0.0.0.9013. http://github.com/PcAux-Package/PcAux.
López-Romero, L., Romero, E., & Villar, P. (2014). Assessing the stability of psychopathic traits: adolescent outcomes in a six-year follow-up. Spanish Journal of Psychology, 17(e97), 1–11.
Lozier, L. M., Cardinale, E. M., VanMeter, J. W., & Marsh, A. A. (2014). Mediation of the relationship between callous-unemotional traits and proactive aggression by amygdala response to fear among children with conduct problems. JAMA Psychiatry, 71(6), 627–636. https://doi.org/10.1001/jamapsychiatry.2013.4540.
Lubrecht, J. (1992). Family satisfaction survey. In K. Kutash & T. R. Rivera (Eds), Measures of satisfaction with child mental health services (pp. 21–23). Florida Mental Health Institute.
Lui, J. H. L., Barry, C. T., & Marcus, D. K. (2019). A short-term intervention for adolescents with callous-unemotional traits and emotion-processing deficits. Journal of Social and Clinical Psychology, 38(6), 475–500.
Manders, W. A., Deković, M., Asscher, J. J., van der Laan, P. H., & Prins, P. J. M. (2013). Psychopathy as predictor and moderator of multisystemic therapy outcomes among adolescents treated for antisocial behavior. Journal of Abnormal Child Psychology, 41(7), 1121–1132. https://doi.org/10.1007/s10802-013-9749-5.
Masi, G., Manfredi, A., Milone, A., Muratori, P., Polidori, L., Ruglioni, L., & Muratori, F. (2011). Predictors of nonresponse to psychosocial treatment in children and adolescents with disruptive behavior disorders. Journal of Child and Adolescent Psychopharmacology, 21(1), 51–55. https://doi.org/10.1089/cap.2010.0039.
Masi, G., Muratori, P., Manfredi, A., Lenzi, F., Polidori, L., Ruglioni, L., Muratori, F., & Milone, A. (2013). Response to treatments in youth with disruptive behavior disorders. Comprehensive Psychiatry, 54(7), 1009–1015. https://doi.org/10.1016/j.comppsych.2013.04.007.
Mattos, L. A., Schmidt, A. T., Henderson, C. E., & Hogue, A. (2017). Therapeutic alliance and treatment outcome in the outpatient treatment of urban adolescents: The role of callous-unemotional traits. Psychotherapy, 54(2), 136–147. https://doi.org/10.1037/pst0000093.
McMahon, R. J., Witkiewitz, K., & Kotler, J. S. (2010). Predictive validity of callous–unemotional traits measured in early adolescence with respect to multiple antisocial outcomes. Journal of Abnormal Psychology, 119(4), 752–763. https://doi.org/10.1037/a0020796.
Moore, A. A., Carney, D., Moroney, E., Machlin, L., Towbin, K. E., Brotman, M. A., Pine, D. S., Leibenluft, E., Roberson-Nay, R., & Hettema, J. M. (2017). The Inventory of Callous-Unemotional Traits (ICU) in children: reliability and heritability. Behavior Genetics, 47(2), 141–151. https://doi.org/10.1007/s10519-016-9831-1.
Moos, R. H., & Moos, B. S. (2009). Family environment scale manual (4th ed.). Melno Park, CA: Mindgarden.
Mun, E. Y., Eye, Avon, & White, H. R. (2009). An SEM approach for the evaluation of intervention effects using pre-post-post designs. Structural Equation Modeling: A Multidisciplinary Journal, 16(2), 315–337. https://doi.org/10.1080/10705510902751358.
Muñoz, L. C., & Frick, P. J. (2007). The reliability, stability, and predictive utility of the self-report version of the Antisocial Process Screening Device. Scandinavian Journal of Psychology, 48(4), 299–312. https://doi.org/10.1111/j.1467-9450.2007.00560.x.
Muthén, L. K., & Muthén, B. O. (1998–2017). Mplus User’s Guide. Eighth Edition. Los Angeles, CA: Muthén & Muthén.
Ng, M. Y., & Weisz, J. R. (2015). Annual Research Review: Building a science of personalized intervention for youth mental health. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 57(3), 216–236. https://doi.org/10.1111/jcpp.12470.
Norlander, B. J. (2008). Targeting dimensions of psychopathy in at-risk youth: Assessment and utility of a focused cognitive behavioral therapy program (PhD thesis). https://digital.library.unt.edu/ark:/67531/metadc9055/m2/1/high_res_d/dissertation.pdf.
O’Connor, T. G., Humayun, S., Briskman, J. A., & Scott, S. (2016). Sensitivity to parenting in adolescents with callous/unemotional traits: Observational and experimental findings. Journal of Abnormal Psychology, 125(4), 502–513.
O’Neill, M. L., Lidz, V., & Heilbrun, K. (2003). Adolescents with psychopathic characteristics in a substance abusing cohort: treatment process and outcomes. Law and Human Behavior, 27(3), 299–313. https://doi.org/10.1023/a:1023435924569.
Ogden, T. (2013). Evaluation of Functional Family Therapy (FFT) in Norway. http://www.isrctn.com/ISRCTN58861782.
Pardini, D. A., Lochman, J. E., & Powell, N. (2007). The development of callous-unemotional traits and antisocial behavior in children: are there shared and/or unique predictors? Journal of Clinical Child & Adolescent Psychology 36(3) 319–333. https://doi.org/10.1080/15374410701444215.
Polaschek, D. L. L., & Skeem, J. L. (2018). Treatment of adults and juveniles with psychopathy. In C. J. Patrick (Ed.), Handbook of psychopathy 2nd ed. (pp. 710–731). New York, NY: The Guilford Press.
Poythress, N. G., Edens, J. F., Skeem, J. L., Lilienfeld, S. O., Douglas, K. S., Frick, P. J., Patrick, C. J., Epstein, M., & Wang, T. (2010). Identifying subtypes among offenders with antisocial personality disorder: A cluster-analytic study. Journal of Abnormal Psychology, 119(2), 389–400. https://doi.org/10.1037/a0018611.
Reddy, S. D., Negi, L. T., Dodson-Lavelle, B., Silva, B. O., Pace, T. W. W., Cole, S. P., Raison, C. L., & Craighead, L. W. (2013). Cognitive-based compassion training: A promising prevention strategy for at-risk adolescents. Journal of Child and Family Studies, 22(2), 219–230. https://doi.org/10.1007/s10826-012-9571-7.
Robbins, M. S., Alexander, J. F., Turner, C. W., & Hollimon, A. (2016). Evolution of functional family therapy as an evidence-based practice for adolescents with disruptive behavior problems. Family Process, 55(3), 543–557. https://doi.org/10.1111/famp.12230.
Roberts, R., McCrory, E. J. P., Joffe, H., Lima, N. D., & Viding, E. (2017). Living with conduct problem youth: Family functioning and parental perceptions of their child. European Child & Adolescent Psychiatry, 8, 1–10. https://doi.org/10.1007/s00787-017-1088-6.
Salekin, R. T., Tippey, J. G., & Allen, A. D. (2012). Treatment of conduct problem youth with interpersonal callous traits using mental models: Measurement of risk and change. Behavioral Sciences & the Law, 30(4), 470–486. https://doi.org/10.1002/bsl.2025.
Sawyer, A. M., Borduin, C. M., & Dopp, A. R. (2015). Long-term effects of prevention and treatment on youth antisocial behavior: A meta-analysis. Clinical Psychology Review, 42, 130–144. https://doi.org/10.1016/j.cpr.2015.06.009.
Silva, D. R., da, Rijo, D., Castilho, P., & Gilbert, P. (2019). The efficacy of a compassion-focused therapy–based intervention in reducing psychopathic traits and disruptive behavior: A clinical case study with a juvenile detainee. Clinical Case Studies, 18(5), 323–343. https://doi.org/10.1177/1534650119849491.
Silva, D. R. da, Rijo, D., Salekin, R. T., Paulo, M., Miguel, R., & Gilbert, P. (2020). Clinical change in psychopathic traits after the PSYCHOPATHY.COMP program: Preliminary findings of a controlled trial with male detained youth. Journal of Experimental Criminology, 1–25. https://doi.org/10.1007/s11292-020-09418-x.
Sørlie, M.-A., Hagen, K. A., & Ogden, T. (2008). Social competence and antisocial behavior: continuity and distinctiveness across early adolescence. Journal of Research on Adolescence, 18(1), 121–144. https://doi.org/10.1111/j.1532-7795.2008.00553.x.
Spain, S. E., Douglas, K. S., Poythress, N. G., & Epstein, M. (2004). The relationship between psychopathic features, violence and treatment outcome: the comparison of three youth measures of psychopathic features. Behavioral Sciences & the Law, 22(1), 85–102. https://doi.org/10.1002/bsl.576.
Statistics Norway (2017). Laveste lønnsvekst på 2000-tallet. https://www.ssb.no/arbeid-og-lonn/statistikker/lonnansatt/aar/2017-02-01#content.
Stellwagen, K. K., & Kerig, P. K. (2010). Relating callous-unemotional traits to physically restrictive treatment measures among child psychiatric inpatients. Journal of Child and Family Studies, 19(5), 588–595. https://doi.org/10.1007/s10826-009-9337-z.
Swanson, J. M., Kraemer, H. C., Hinshaw, S. P., Arnold, L. E., Conners, C. K., & Abikoff, H. B., et al. (2001). Clinical relevance of the primary findings of the MTA: Success rates based on severity of ADHD and ODD symptoms at the end of treatment. Journal of the American Academy of Child & Adolescent Psychiatry, 40, 168–179.
Taylor, L. K., Merrilees, C. E., Goeke-Morey, M. C., Shirlow, P., & Cummings, E. M. (2014). Trajectories of adolescent aggression and family cohesion: The potential to perpetuate or ameliorate political conflict. Journal of Clinical Child & Adolescent Psychology, 45(2), 369–373. https://doi.org/10.1080/15374416.2014.945213.
Thøgersen, D. M., Bjørnebekk, G., Scavenius, C., & Elmose, M. (2021). Callous-unemotional traits do not predict functional family therapy outcomes for adolescents with behavior problems. Frontiers in Psychology, 11, 537706 https://doi.org/10.3389/fpsyg.2020.537706.
Thøgersen, D. M., Andersen, M. E., & Bjørnebekk, G. (2020). A multi-informant study of the validity of the inventory of callous-unemotional traits in a sample of Norwegian adolescents with behavior problems. Journal of Psychopathology and Behavioral Assessment, 1–13. https://doi.org/10.1007/s10862-020-09788-6.
Vanwoerden, S., Reuter, T., & Sharp, C. (2016). Exploring the clinical utility of the DSM-5 conduct disorder specifier of ‘with limited prosocial emotions’ in an adolescent inpatient sample. Comprehensive Psychiatry, 69, 116–131. https://doi.org/10.1016/j.comppsych.2016.05.012.
Viding, E., & McCrory, E. J. P. (2019). Towards understanding atypical social affiliation in psychopathy. The Lancet. Psychiatry, 6(5), 437–444. https://doi.org/10.1016/s2215-0366(19)30049-5.
Viding, E., Blair, R. J. R., Moffitt, T. E., & Plomin, R. (2005). Evidence for substantial genetic risk for psychopathy in 7-year-olds. Journal of Child Psychology and Psychiatry, 46(6), 592–597. https://doi.org/10.1111/j.1469-7610.2004.00393.x.
Viding, E., Jones, A. P., Frick, P. J., Moffitt, T. E., & Plomin, R. (2008). Heritability of antisocial behavior at 9: do callous-unemotional traits matter? Developmental Science, 11(1), 17–22. https://doi.org/10.1111/j.1467-7687.2007.00648.x.
Viding, E., Sebastian, C. L., Dadds, M. R., Lockwood, P. L., Cecil, C. A. M., Brito, S. A. D., & McCrory, E. J. P. (2012). Amygdala response to preattentive masked fear in children with conduct problems: The role of callous-unemotional traits. The American Journal of Psychiatry, 169(10), 1109–1116. https://doi.org/10.1176/appi.ajp.2012.12020191.
Viding, E., & Kimonis, E. R. (2018). Callous-unemotional traits. In C. J. Patrick (Ed.) The handbook of psychopathy (2nd ed.) (pp. 144–164). New York, NY: The Guilford Press.
Waller, R., Gardner, F., & Hyde, L. W. (2013). What are the associations between parenting, callous-unemotional traits, and antisocial behavior in youth? A systematic review of evidence. Clinical Psychology Review, 33(4), 593–608.
Waller, R., Hyde, L. W., Klump, K. L., & Burt, S. A. (2018). Parenting is an environmental predictor of callous-unemotional traits and aggression: A monozygotic twin differences study. Journal of The American Academy of Child & Adolescent Psychiatry, 57(12), 955–963. https://doi.org/10.1016/j.jaac.2018.07.882.
Weisz, J. R., Kuppens, S., Ng, M. Y., Vaughn-Coaxum, R. A., Ugueto, A. M., Eckshtain, D., & Corteselli, K. A. (2019). Are psychotherapies for young people growing stronger? Tracking trends over time for youth anxiety, depression, attention-deficit/hyperactivity disorder, and conduct problems. Perspectives on Psychological Science, 14(2), 216–237. https://doi.org/10.1177/1745691618805436.
Weisz, J. R., Kuppens, S., Ng, M. Y., Eckshtain, D., Ugueto, A. M., Vaughn-Coaxum, R., Jensen-Doss, A., Hawley, K. M., Marchette, L. S. K., Chu, B. C., Weersing, V. R., & Fordwood, S. R. (2017). What five decades of research tells us about the effects of youth psychological therapy: A multilevel meta-analysis and implications for science and practice. American Psychologist, 72(2), 79–117. https://doi.org/10.1037/a0040360.
White, S. F., Frick, P. J., Lawing, K., & Bauer, D. (2013). Callous-unemotional traits and response to functional family therapy in adolescent offenders: Callous-unemotional traits and FFT. Behavioral Sciences & the Law, 31(2), 271–285.
Wilkinson, S., Waller, R., & Viding, E. (2016). Practitioner Review: Involving young people with callous unemotional traits in treatment-does it work? A systematic review. Journal of Child Psychology and Psychiatry, 57(5), 552–565. https://doi.org/10.1111/jcpp.12494.
World Health Organization, (2018). ICD-11 for mortality and morbidity statistics (ICD-11 MMS) 2018 version. Retrieved from: https://icd.who.int/browse11/l-m/en.
Acknowledgements
We want to acknowledge the adolescents and their parents who participated in this study and the therapists providing treatment to the families. A special acknowledgement also goes to Asgeir R. Olseth for assistance with data management and statistical analyses.
Funding
This study was supported by the TrygFonden under Grant 120499; and the Norwegian Center for Child Behavioral Development. Open access funding provided by NUBU - The Norwegian Center for Child Behavioral Development.
Author information
Authors and Affiliations
Contributions
All authors contributed to the conception and design of the study. Gunnar Bjørnebekk and Dagfinn Mørkrid Thøgersen prepared the materials and collected the data. Dagfinn Mørkrid Thøgersen performed the statistical analysis with guidance from Gunnar Bjørnebekk. Dagfinn Mørkrid Thøgersen wrote the first draft of the manuscript. All authors contributed to manuscript revision, and read and approved the submitted version.
Corresponding author
Ethics declarations
Conflict of interest
The first author of this article has been and is currently involved with the implementation of the FFT program in Norway and Denmark. None of the other authors have any disclosures regarding conflict of interest.
Ethics approval and Consent
Ethical approval for this study was obtained from The National Committee for Medical and Health Research Ethics (NEM) on October 2nd, 2012 (Reference number: 2010/497). All data was collected and stored in compliance with Norwegian laws and regulations by The Norwegian Center for Child Behavioral Development. Prior to the first data collection participants were informed about the study and provided a written informed consent.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Thøgersen, D.M., Elmose, M., Viding, E. et al. Behavioral Improvements but Limited Change in Callous-Unemotional Traits in Adolescents Treated for Conduct Problems. J Child Fam Stud 31, 3342–3358 (2022). https://doi.org/10.1007/s10826-022-02435-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-022-02435-6