
Abstract
Parental engagement in parenting programs is essential for good outcomes but can be challenging for many families. In low- and middle-income countries, where resources are limited and there are fewer support services, there is little research examining the factors that influence engagement. This mixed-methods study explored factors associated with parent engagement, as well as barriers and supports, in a pilot evaluation of a parenting program with 140 parents in North Macedonia, Republic of Moldova, and Romania. The relationship between various quantitative types of engagement (e.g., premature drop-out, participation) and a range of demographic, personal, and implementation factors were examined. Qualitative parent interviews explored barriers and supports to program engagement. Implementation variables (e.g., phone calls with parents, program fidelity and text messages sent to parents) were consistently positively associated with different types of engagement after controlling for other factors. Parents of boys, being a victim of intimate partner violence, more children in the household and better parental well-being were positively associated with premature drop-out whilst having a child enrolled in school was positively associated with participation. Barriers included logistical factors such as timing and lack of childcare facilities. Factors that increased engagement included facilitator skills/support, weekly text messages and phone calls and engagement strategies such as transport and childcare. The results emphasise the importance of implementation factors in increasing parent engagement in parenting programs and will help to inform the next phase of the project as well as other family-support initiatives in the three countries. The trial is registered on ClinicalTrials.gov (ID: NCT03552250).
Highlights
-
A mixed-methods approach was used to examine parent engagement in a parenting program in Southeastern Europe.
-
The most consistent associated factors across the types of engagement were implementation factors.
-
Results will inform later phases of the project and support implementation of parenting programs in Southeastern Europe.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Child behavior problems are of global concern with an estimated 6% prevalence for disruptive disorders (Polanczyk et al., 2015). Long-term outcomes for children with behavior problems are poor with increased risks of substance misuse, school drop-out, delinquency and serious criminal offending (e.g., Colman et al., 2009). Parenting behavior is the key factor in the development of childhood behavior problems (Harvey & Metcalfe, 2012) and behavioral parent training (BPT) programs that teach effective parenting strategies are recommended for reducing these problems (Tandon & Giedinghagen, 2017). BPT programs are effective in high-income countries as well as in low- and middle-income countries (LMIC), where 90% of the world’s children reside, resources are low, and child maltreatment and corporal punishment rates are high (Burkey et al., 2018).
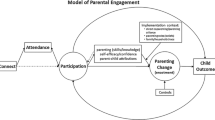
The effectiveness of parenting interventions is largely contingent on parent engagement (Reyno & McGrath, 2006), whereas their public health impact depends on the implementation success (see Glasgow et al., 1999). However, there is no agreed definition in the literature. Consequently, many different definitions of engagement used and little uniformity when reporting engagement outcomes highlighting the need for a universal definition (Chacko et al., 2016). This paper uses the definition provided by Piotrowska et al. (2017) who proposed a conceptual engagement model (CAPE - Connect, Attend, Participate, Enact - model) that specifically outlines individual-level indicators for successful engagement of parents into BPT. This conceptual model is particularly useful as it can be integrated within an implementation framework such as the RE-AIM framework (Glasgow et al., 1999). The RE-AIM framework defines implementation success on five dimensions: (1) Reach of the target population, (2) Efficacy of the BPT when delivered in a new context, (3) Adoption of the BPT by various institutions in the new setting, (4) Implementation fidelity (adherence of facilitators and participants), and (5) Maintenance of effects in participants as well as on the institution- and the community-level (sustainable integration of BPT into daily routines). Integrating both frameworks allows for a more comprehensive exploration of engagement. The CAPE model focuses on individual-level indicators of engagement whilst RE-AIM adds wider indicators such as program-level factors (e.g., fidelity). The integration between CAPE and RE-AIM encompasses: recruitment and enrolment (Connect; corresponds to RE-AIM Reach); attendance and retention (Attend; RE-AIM Reach and Implementation); adherence and active session participation (Participate; RE-AIM Implementation); implementing newly learned strategies (Enact; RE-AIM Implementation and Maintenance). Greater engagement predicts better outcomes (Morawska & Sanders, 2006), but is often challenging. As many as 25% of families eligible for BPT never enrol on a program and approximately 26% of attendees drop out before completion (Chacko et al., 2016). Identifying factors associated with increased or decreased parent engagement is a first step in establishing strategies to successfully engage families with BPT.
Numerous factors can make engagement in BPT more difficult for parents, and these can influence different stages of parent engagement, specifically the first three stages of the CAPE model. In the Connect stages, Eisner and Meidert (2011) found that larger household size and lower income were associated with lower likelihood to enrol in a BPT, whilst Dumas et al. (2007) found that time and scheduling demands were significant predictors of less intent to enrol (i.e., Connect). Parents who perceived little need for, or relevance of, treatment were more likely not to attend at all or to drop out of a parent program (Chacko et al., 2017). Gonzalez et al. (2021a) found that parents with higher levels of coercive and inconsistent parenting behaviours and parents with more symptoms of psychological distress had increased intention to participate in a parent program. For Attend stages, parents with stronger neighborhood support networks were more likely to complete a parent program, whilst parents whose native language was not the language of program delivery were less likely to attend or complete the program (Attend; Eisner & Meidert, 2011). Haggerty et al. (2002) found that higher levels of parental education predicted higher attendance rates, whilst Baker et al. (2011) reported that limited social support was associated with lower attendance. Koerting et al. (2013) highlighted the importance of program-related factors reporting that therapist skills/background, positive personal qualities of therapists and additional phone contact during program delivery all supported continued program engagement. In the Participation stages, Nix et al. (2009) found that low parent education and severity of child behaviour problems predicted parents’ quality of participation during sessions. Facilitator in-session skills have also been associated with increased quality of parents’ participation (Leitao et al., 2020). Also, Smith et al. (2013) found that higher levels of implementation fidelity (i.e., the degree to which a program is delivered as intended) led to better parental participation in sessions. The Participation stages are also the most important in influencing positive outcomes including improvements in parenting practices (Baydar et al., 2003; Piotrowska et al., 2017).
Eastern Europe has been identified as an area with high rates of child maltreatment (WHO, 2013) and low mental health resources (Kovess-Masfety et al., 2016). In a study exploring adverse childhood experiences (Bellis et al., 2014), physical abuse was the most common across eight Eastern European countries (18.6%) followed by violence towards mother (14.6%) and emotional neglect (11.8%), highlighting a demand for services to support parents. There is as yet limited research on parent engagement in Eastern Europe with evidence mainly coming from high-income countries. However, despite the three countries involved in the current research moving into the upper-middle-income category their needs and service provision for dealing with child protection issues are still under-resourced, as commonly observed in LMIC. BPT can be effectively delivered in LMIC (Burkey et al., 2018; Pedersen et al., 2019), however limited resources and high levels of deprivation may make parent engagement even more challenging. The present study examines factors associated with parent engagement in a BPT delivered in North Macedonia, Republic of Moldova, and Romania, three countries classified as upper-middle-income according to the latest World Bank statistics (The World Bank, 2021). It explores barriers and supports using a mixed-methods approach to identify procedures needing adaptation or change for later study phases to increase the reach, adoption, implementation and sustainability of the program in the three countries (for more details see Frantz et al., 2019). The factors of interest correspond to the Connect, Attend and Participate elements of the CAPE model (Piotrowska et al., 2017) and the Reach, Implementation and Maintenance elements of RE-AIM (Glasgow et al., 1999).
Method
Setting
This study was conducted from April to December 2018 in North Macedonia, Republic of Moldova, and Romania. Within each country, one institution under the guidance of a principal investigator undertook recruitment and implementation for a field test of the low-cost Parenting for Lifelong Health for Young Children (PLH-YC) program. The institutions included: a family psychotherapy institute that conducts research and education in systemic practice and family psychotherapy (North Macedonia), a non-governmental organisation that promotes access to services for adolescents and young people related to their general, mental, and sexual reproductive health (Republic of Moldova), and academics at a University (Romania). Jansen et al. (2021) report positive pre-post changes for various child behavior and parenting practice outcomes, as well as positive associations between post-intervention outcomes and program participation from the same trial.
Participants
Participants were primary caregivers (referred to as parents henceforth) of a child aged 2–9 years for whom they reported elevated levels of behavior problems using the Eyberg Child Behavior Inventory (Eyberg et al., 1980) cut-off of 131 on the Intensity scale or 15 on the Problem scale. Parents had to be aged 18+ years, live in the same household as the child for at least four nights a week and anticipate continuing to do so, agree to participate in the program, and provide informed consent to study participation. We recruited 140 parents using methods such as direct referrals from partner institutions (e.g., child mental health services, NGOs, GOs, kindergartens, schools), social media (Facebook), flyers, posters/billboards, TV, information stand in public events, parent recommendations, and personal communication (including door-to-door). In North Macedonia, families were mainly recruited via flyers in schools and kindergartens, and Facebook, Moldovan families via Facebook, and Romanian parents via personal distribution of materials and personal contacts with school and kindergarten staff, respectively. The majority of parents were female (n = 137, 97.9%) with a mean age of 35 years (see Table 1). Facilitators were staff from various social, educational or health organizations within each country.
Procedures
All parents and facilitators provided informed consent to full study participation. The study was approved by the Human Research Ethics Committee of the Anonymised University and local ethics committees in the three countries.
Intervention
A 12-session manualised group-based version of PLH-YC was tested with parents of children aged 2-9 years. PLH-YC is part of a broader initiative led by the World Health Organisation, UNICEF and partner universities to prevent or reduce violence against children by developing and testing evidence-informed low-cost parenting interventions. The program was originally developed and tested in South Africa (Lachman et al. 2016; Ward et al., 2020) and is currently being evaluated in several LMICs (e.g., Janowski et al., 2020; Lachman et al., 2021; McCoy et al., 2021; Murphy et al., 2021).
PLH-YC introduces social learning theory-based behavioral parenting techniques delivered using a collaborative process. Topics covered are: 1) Spending one-on-one time with your child; 2) Using words to describe actions; 3) Talking about feelings; 4) Using praise and rewards to reinforce positive behavior; 5) Giving positive, specific, and realistic instructions; 6) Establishing consistent household rules and routines; 7) Redirecting negative to positive behaviors; 8) Ignoring negative attention-seeking and demanding behaviors; 9) Using consequences to support compliance; 10) Using cool down as a consequence for aggressive behavior; 11) Avoiding and resolving family conflicts; 12) Reflection, celebration and moving on. Mindfulness-based stress reduction for parents is a consistent component throughout the sessions. The core techniques to teach new skills include group discussion, exploration of illustrated stories of parent-child interaction, role-play practice of skills, homework activity assignments, collective problem-solving, and feedback on homework experiences (Lachman et al., 2016). The program is delivered by a pair of facilitators. To encourage engagement, parents receive weekly text messages (SMS) and phone calls from facilitators. Additional strategies for encouraging parent engagement with the program included transportation and childcare. Childcare was not pre-specified, however experiences of some groups showed that childcare was necessary to enable some parents to participate in the program so childcare was provided for some groups (for details see below).
Implementation
The program was translated into Macedonian, Romanian for Moldova, and Romanian, the primary languages of the three countries. Only the Romanian version was used in Romania. Facilitators attended a five-day training workshop (30 h) provided by one of the program developers (Lachman). Facilitators received a program manual and coaching via online video conferences from a program developer to monitor implementation during delivery. Each country had process monitors to observe implementation of the program and evaluate delivery fidelity, use of engagement strategies, and frequency of phone calls and text messages.
Each country delivered four groups. Due to timing challenges with recruitment and program delivery, program implementation differed between countries. Facilitators in the Republic of Moldova delivered the 12-session program in weekly sessions (exception: sessions 10 and 11 were delivered within one week) and received weekly coaching sessions for facilitators (12 in total). Parents in three of the four groups used the transportation offer (one group was within walking distance for parents) whilst none of the groups utilised childcare. Facilitators in North Macedonia delivered the 12-session program in two sessions each week and had weekly coaching sessions (five in total). Parents in all four groups used the transportation offer and parents in three groups used childcare. Facilitators in Romania delivered the program in six sessions with one session per week and weekly coaching sessions (six in total). The six-session program utilised the same curriculum as the 12-session version with condensed content. The transport allowance was not used in Romania due to program delivery being within walking distance for parents, but all four groups used the childcare offer.
Measures
All measures were translated and back-translated into the three local languages. This process was completed by expert child psychiatrist and psychologist partners in each country, as well as with the developers of the questionnaires (e.g., CBCL).
Feasibility
Parent satisfaction scale
This was adapted from a satisfaction measure used by Webster-Stratton (1989). It consists of 42 items exploring parents’ perceptions of program acceptability including the program overall, program activities, program techniques, satisfaction with the facilitators and the group. Responses were recorded on a five-point Likert scale from 1 to 5. An example item is ‘How helpful were the group discussions regarding home activity assignments?’ with responses including 1 – very unhelpful, 2 – unhelpful, 3 – neutral, neither helpful or unhelpful, 4 – helpful, 5 – very helpful.
Potential factors associated with engagement
Family demographics
Key sociodemographic data were collected from each family. These included parent and child gender and age, parent education level, parent literacy skills, parent employment, marital status, parent relationship to child, parent religion, whether the child attended school, number of adults aged 18+ years in the household, and number of children aged 2-9 years cared for in the household.
Neighbourhood characteristics (Conduct problem prevention research group, 1991)
The Neighbourhood Questionnaire (11 items, α = 0.72) was used as a measure of neighbourhood characteristics. It includes three subscales: Safety (five items), Neighbourhood social involvement (four items) and Neighbourhood quality of public services (two items).
Parent relationship quality (Schumm et al., 1983)
The Kansas Marital Satisfaction Scale (KMSS, three items) was used to assess relationship satisfaction between intimate partners (α = 0.98).
Emotional social support (Sherbourne & Stewart, 1991)
The emotional support subscale of the Medical Outcome Study Social Support Survey (MOS) was used to assess perceived social support. The subscale consists of eight items about how often the parent receives social support (α = 0.96).
Parental mental health
Two measures were used to assess parental mental health: the brief version of the Depression, Anxiety, Stress Scale (DASS; Henry & Crawford, 2005) and WHO-5 Well-Being Scale (WHO, 1998). The DASS screens for symptoms of depression, anxiety and stress in 21 items (α = 0.91). The WHO-5 is a five-item screening tool assessing parental psychological well-being (α = 0.77).
Parenting behavior
Two measures assessed parenting behavior: the Parenting Scale (PS; Arnold et al., 1993) and the Parenting of Young Children Scale (PARYC; McEachern et al., 2012). The PS is a 30-item measure of dysfunctional practices incorporating three subscales (Laxness α = 0.66, Over-reactivity α = 0.72, and Verbosity α = 0.42) and an overall score (α = 0.61, without verbosity α = 0.68). Each item describes a situation on which parents choose between two responses using a seven-point Likert scale. Only the Total, Laxness and Over-reactivity scores were used due to low internal consistency for the Verbosity scale, consistent with other studies examining the measure’s psychometric properties (Pritchett et al., 2011; Rhoades & O’Leary, 2007). The PARYC is a 21-item measure of positive parenting and effective discipline. Items are summed to give an overall score (α = 0.85) and three subscales (Positive parenting α = 0.73, Setting limits α = 0.75, and Proactive parenting α = 0.76).
Child behavior
Child behavior was assessed using the Child Behavior Checklist (CBCL; Achenbach & Rescorla, 2001) for children aged 1.5–5 years and 6–18 years. Scores for internalizing behavior (1.5–5 years α = 0.79, 6–18 years α = 0.78) and aggression (1.5–5 years α = 0.86, 6–18 years α = 0.87) were used in this study. We used the aggression subscale although not pre-specified in the study protocol (Frantz et al., 2019) because of the low internal consistency of the externalizing subscale (for details see also Jansen et al., 2021).
Child maltreatment
A measure based on the International Society for the Prevention of Child Abuse and Neglect (ISPCAN) Child Abuse Screening Tool for Trials (ICAST-Trial; Meinck et al., 2018) was used to assess incidence and prevalence of child abuse and neglect. Response options for individual items assessing frequency of behaviors in the past month were zero to more than eight times. Dichotomous variables assess the incidence of physical abuse (four items), emotional abuse (seven items) and neglect (three items). Overall abuse was calculated by summing all three subscales. Parent history of maltreatment in childhood was assessed using an adapted version of the ICAST Retrospective version (ICAST-R; Dunne et al., 2009). Three items were used: one on physical maltreatment taken from the ICAST-R; an additional two items were added to assess corporal punishment and psychological aggression in a more global way than specified in the ICAST-R. For an overall score of the three items, the three items were summed.
Intimate partner violence
Intimate partner violence (IPV) was assessed using 29 items from Heyman et al. (2013) adapted from the Conflict Tactics Scale (Straus & Douglas, 2004). The items used referred to abuse (physical and psychological) within the last month with an additional response for any previous incidents. An overall indication of IPV severity is calculated for self (perpetration) and partner (victimisation) and for physical and psychological aggression.
Obstacles to engagement scale (OES; Wilson et al., 2015)
This 14-item scale explores barriers to participation and engagement (subscales: personal obstacles, relevance of parenting programs, suitability of group-based programs, and time commitment barriers) (α = 0.88). Lower scores indicate more barriers.
Implementation variables
Information was collected by the process monitors. Data collected included the percentage of planned phone calls completed by facilitators, the percentage of planned text messages sent by facilitators, and the percentage of program content delivered (content fidelity).
Qualitative parent interviews
Semi-structured interviews explored four general themes: 1) acceptability and appropriateness of program materials, delivery, and key program components; 2) barriers to participation during sessions and engagement in home practice and other activities; 3) participant-reported observed change in parenting practices; and 4) child behavior at home. Parents with differing attendance rates were interviewed by data assessors as part of post-assessment. Parents were purposively selected based on attendance rates: high attendance (attend > 75% of sessions), low attendance (attend < 25% of sessions) and non-enrollers (attend no sessions). Thirty-three interviews were conducted: North Macedonia, 6; Republic of Moldova, 9; Romania, 18. Fifteen (45.5%) were high attenders (> 75% of sessions i.e., ten+ sessions in North Macedonia and Republic of Moldova or five+ sessions in Romania), 12 (36.4%) were moderate attenders (25–75% of sessions i.e., between three and nine in North Macedonia and Republic of Moldova or between two and four in Romania), three (9.1%) were low attenders (< 25% of sessions, i.e., less than three in North Macedonia and only one in Romania), and three (9.1%) were parents who did not enrol.
Engagement outcomes
Outcomes are reported based on elements of the integrated CAPE/RE-AIM model (Glasgow et al., 1999; Piotrowska et al., 2017). For Connect, premature drop-out – whether participants dropped out after pre-assessment but before enrolling in a group – was examined. Differences in program delivery across the three countries, meant that it was not possible to calculate the premature drop-out variable as specified in the study protocol (i.e., participants who did not attend three consecutive sessions and no sessions at a later stage). For Attend, program enrolment – whether participants attended at least one session of the program as pre-defined in the study protocol; participation rate – mean attendance rate for families enrolled in the program as pre-defined in the study protocol – and completion – whether participants had attended at least 67% of the program sessions as pre-defined in study protocol – were examined. For Participation, home activity completion (as a percentage) was examined. Home activity completion was based on participant self-report during group sessions and/or phone calls as noted by the facilitator or process monitor-report forms. Facilitators would ask parents whether they had managed to complete the home activity that week and then explore how it was implemented in terms of both positives and challenges.
Data Analysis
Quantitative
There was very little missing data. Two variables, religion and ICAST-R, had data missing from one participant (0.7%). All other variables had no missing data. Bivariate correlations were calculated between the outcome variables (premature dropout, enrolment, participation rate, completion rate, home activity completion) and potential factors. All variables with an association at significance level p < 0.05 were entered as factors in the regression models. Two multiple regression (participation rate and home activity completion) and three logistic regression models (completion rate, enrolment and premature dropout) were conducted. Factors were entered using a hierarchical method based on three blocks: country, parent/child characteristics (including sociodemographic factors), implementation measures and OES variables. Implementation variables were not entered in the premature dropout logistic regression model as they were not applicable. The country variable was entered as two dummy variables using North Macedonia as the reference category.
Qualitative
Parent interviews were transcribed and analysed using thematic analysis method (Braun & Clarke, 2006), to explore barriers to, and supports of, parent program engagement. An exploratory approach was used allowing for emergent themes to be coded. There were no pre-defined themes. Analyses were conducted in-country and combined to explore themes across the three countries. Only anonymised exemplary quotes for each theme were translated into English to reduce translation costs. Quote translations were completed by in-country teams.
Results
Supplemental Tables 1–3 show the associations between the variables and outcomes. Correlations and chi-square distributions with a p < 0.05 are highlighted in bold and were included in the regression models along with dummy variables to control for country.
Recruitment, Enrolment and Premature Dropout (CONNECT)
Recruitment was between April and June 2018. Two hundred and fifty-three families were screened of whom 162 (81%) met pre-screening criteria and were invited to provide informed consent. Informed consent was obtained from 100% of the 162 parents of whom 140 (86%) reported elevated levels of child behavior problems and were enrolled in the study. All 140 parents were allocated to one of four groups based on where they lived within each country, however 21 (15%) dropped out before allocation (for detailed participant flow see Jansen et al., 2021). Demographics are displayed in Table 1. There were no significant demographic differences between those allocated to a group and those who dropped out before allocation (for details see Jansen et al., 2021). A total of 110 parents attended at least one session, an overall enrolment rate of 79% (North Macedonia: 86%; Republic of Moldova: 83.7%; Romania: 70.2%).
Premature drop-out was significantly correlated with eight variables of which child gender, parents’ WHO well-being, physical IPV by partner and number of children aged 2-9 years in the household remained significant in the regression model. The odds of dropping out prematurely were 7.25 times higher for parents of boys. For every one-unit increase, parents reporting higher rates of physical IPV by their partner were 18.2% more likely to drop-out, parents with better mental well-being were 16.1% more likely to drop-out, and parents with more children aged 2-9 years in the household were 71% more likely to drop-out prematurely (see Table 2).
Program Participation (ATTEND)
Mean attendance ranged from M = 64%, SD = 29% (median = 75%) to M = 80%, SD = 23% (median = 88%) of the 12-session program for Republic of Moldova and North Macedonia respectively and M = 55%, SD = 37% (median = 67%) of the six-session program in Romania. Ninety-three (85%) enrolled parents attended at least 50% of the program, with 72 (66%) attending at least 75%. Eighty-two (75%) enrolled parents completed the program (i.e., attended at least 66% of sessions).
Of the ten significant correlations for program enrolment, none were significant associations in the regression model. Participation rate had ten significant correlations of which higher percentages of completed facilitator calls, text messages sent, and delivered session activities remained significantly associated with greater attendance rates (see Table 3). For completion, of the six significant correlations, only higher percentages of completed calls and higher levels of delivered session activities were associated with higher completion rates (see Table 4). For every one-unit increase, parents receiving higher percentages of facilitator calls were 5.7% more likely to complete the program and parents in groups where more session activities were delivered were 59.7% more likely to complete the program.
Implementation and Home Activity Completion (PARTICIPATE)
Based on process monitor and/or facilitator completed fidelity checklists, implementation fidelity (the level of program content delivered as pre-specified in the protocol; see Frantz et al., 2019) ranged between 82% and 100%. The mean percentage for home activity completion across the three countries was 45% (SD = 40%, median 55%). The mean percentage of calls from facilitators to parents across the three countries was 34% (SD = 36%, median = 18%) whilst for text messages sent by facilitators to parents it was 53% (SD = 33%, median = 33%). Implementation fidelity was significantly positively correlated with number of completed text messages, calls, home activity completion, attendance and program completion.
Home activity completion was significantly correlated with 14 variables of which only facilitator calls and text messages remained significant with higher levels of completed calls and messages being associated with greater levels of engagement with home activities (see Table 5).
Barriers to and Supports for Program Engagement
Four main themes were identified in the qualitative analyses: motivation for attendance, valued program components, barriers/challenges to engagement, and supports to engagement.
Motivation for attendance
Parents in the Republic of Moldova and Romania identified several reasons for enrolling on the program. Some wanted to improve their own skills and “just wanted to be a better parent” (Romania). Another Romanian parent wanted to improve family life: “I joined because I wanted the best for my family … the most important thing is for things to be good in the family.” Parents also reported wanting to learn some general parenting skills with one parent in Republic of Moldova wanting to “learn some methods of education, or … how best to understand my child and how to react when I have a problem with him.” A few parents mentioned attending the program in order to change their child’s behavior. One parent in Republic of Moldova said: “I wanted to change his behavior so that he would behave in a good mood with someone and listen to me and stop when I ask him.” Other parents reported struggling with their child’s behavior, not knowing how to deal with their child and turning to the program for help: “Because I had serious problems with the child and we could not get along with each other. I was helpless” (Republic of Moldova).
Valued program components
Parents from all three countries identified a number of valued program components, the most frequently reported being sharing problems with other parents. Parents appreciated the opportunity to share experiences with other parents and help each other to solve problems:
We have so much to learn from each other. Maybe I have one problem, another parent deals with another problem … Maybe I will be having the problem you have now and I would know what to do, because being there and hearing someone talking about the same problem that I have … maybe I would get advice and we would solve it together (Romania).
Despite broadly overall positive feedback there were some initial reservations about sharing personal experiences at the beginning of the program: “We were sceptical in the beginning, but we later got closer and shared a lot of personal experiences” (North Macedonia).
Practising skills was perceived as another valued program component, particularly in helping parents to see how the child feels in particular situations. One parent in Republic of Moldova said: “[practising skills] was very useful because it was important for me to see things from his perspective and how to behave and what he feels when he is a child and you understand why he behaved like this.” However, some also reported that role-plays were somewhat uncomfortable: “There was a lot of laughing when we practiced roles and it was a bit embarrassing” (North Macedonia).
Respondents in Romania identified home activity feedback as useful, particularly the focus on individuals. One parent said: “They asked each one of us. Separately. Asking us how we have done at home with our children, each one of us. And each one of us answered … I enjoyed it.” Parents in Romania also appreciated the illustrated stories with one parent highlighting their usefulness for parents who were illiterate: “Some of the parents did not know how to read, but they understood the [illustrated stories]. Because you understand the question if there is an image attached to it. You think differently by seeing the image.”
Lastly, respondents in North Macedonia and Romania reported the value of ongoing support from group members outside of the group setting. A few parents mentioned the usefulness of contacting others when they had a problem with the children. One parent in North Macedonia said: “We still contact on social media when we face some problems and we socialize from time to time.”
Barriers/Challenges to parent engagement
Parents identified a number of barriers to engagement, many of which related to the different delivery program schedules across the three countries. For example, the number and frequency of sessions was identified as a barrier in North Macedonia and Romania. Parents in Romania, who received the six-session version, reported that the program was too short since they needed more time to apply the strategies: “I was glad at first, finding out there were 6 sessions. Afterwards, I would have been content with 12, to have more time to apply everything” (Romania). Parents in North Macedonia, who received the 12-session version delivered in six weeks, also reported needing more time between sessions to practice skills: “It would have been good to have the sessions more separate. We didn’t have time to practice what we learned” (North Macedonia).
Program timing was also seen as a barrier in the Republic of Moldova and Romania. The program was delivered during summer months when families typically go on holiday or children stayed with other family members: “Children were on vacation, they were gone for days, so I could not apply all the things we were learning during the sessions” (Romania). Work commitments were a barrier affecting attendance. One parent in Romania said: “I managed to join two sessions only because I needed to go work … I needed the money.” Parents in Romania who attended the six-session program described lack of time for group discussion as a barrier with too much content in each session meaning less time for other activities.
I would have liked to get more into some situations, and get, besides facilitators feedback, our own feedback … to get the opportunity to reflect on my errors, to practice more and be confident about how to use the things I have learned (Romania).
Another barrier was the lack of childcare during program delivery, particularly for Republic of Moldova that did not offer this. Where childcare was unavailable, parents reported that they “just can’t [attend] because I have no one to leave [the children] with” (Romania).
Supports for parent engagement
Parents in all countries identified facilitator support and skills as important, commenting on the facilitators’ warm and attentive natures: “I really liked the group leaders. They were attentive and shared advice. They cared about our daily schedules” (North Macedonia), valuing their expertise: “It was important to me what true psychologists would say that with experience, their opinions were interesting” (Republic of Moldova), and professionalism: “I appreciate the level of preparation of the leaders, their seriousness and punctuality, and all they have done for all of us as a group” (Romania).
Parents in the Republic of Moldova and Romania described feeling supported by the weekly phone calls and text messages sent by the facilitators and appreciated the reminder for the home activities that parents did in between sessions. One parent in Romania said
The text messages and phone calls were like a reminder from the leaders. It was particularly good because I remembered what I had to do, and they validated my home experience each time, by telling me: you are doing fine, stop thinking that you are wrong, keep going, you are a good parent. All the conversations had this positive feedback, which I must say, made me feel good. (Romania)
Lastly, parents in North Macedonia and Romania commented on the importance of the additional strategies for engagement with the program, particularly the availability of childcare. A parent in North Macedonia said that she was “grateful that I was able to leave my children with the carer so I could attend” whilst a parent in Romania reported that having “someone to look after her … it was important.” Parents in North Macedonia also commented on the usefulness of transportation to group sessions.
Discussion
This study is one of the few to examine factors associated with parent engagement in a BPT in Eastern Europe (in this case in three Southeastern European countries) as well as associated barriers and supports. Program implementation varied across countries, as did rates of parent engagement, though all rates were within the ranges found in other studies (Chacko et al., 2016; Haine-Schlagel & Walsh, 2015). Rates of fidelity of program implementation were good. The most consistent factors associated with increased parent engagement were the implementation variables, namely phone calls and text messages from facilitators and better implementation fidelity. These were the only significant factors for the Attend and Participate elements of parent engagement. Factors related to parent mental health, intimate partner violence, child gender and family size were significantly related to the Connect element of parent engagement. Parents identified several barriers to engagement including factors related to program logistics (session frequency, timing, childcare) as well as supports to engagement (facilitator characteristics, between session contact, childcare). These findings have enhanced our understanding of factors associated with parent engagement in BPT in three Southeastern European countries and provide insights which could aid in future implementation of BPT in these countries.
There were several factors associated with the Connect stage of parental engagement (premature drop-out in this study). Parents of boys were more likely to drop out of the study (not the program) before group allocation. Many other studies have shown no relationship between study recruitment and child gender (e.g., Dumas et al., 2007; Heinrichs et al., 2005), however this may be due to differences in the type of study i.e., whether it was a universal/selective prevention study or an indicated prevention/treatment study. Both Dumas et al. (2007) and Heinrichs et al. (2005) were universal prevention studies whilst the current study is an indicated prevention study. It may also be related to parents’ perception of behavior problems in boys being more accepted than girls and therefore parents feel less of a need to attend a parenting program. Godoy et al. (2014) found that parental appraisal of their child’s behavior problems (i.e., perception as problematic and awareness of it) was directly related to help-seeking behavior although no gender difference was found. They also found that parental mental health (stress and depression) was positively associated with parental appraisal and help-seeking behaviors. Similarly, Gonzalez et al. (2021a) found that parents with higher levels of psychological distress had higher intentions to participate in parenting programs. This may explain the current findings in relation to parent well-being whereby parents with better mental well-being were more likely to drop out of the study prematurely, suggesting that they may not have perceived the need for support.
Parents who had been victims of physical IPV were also more likely to drop out before group allocation. IPV is highly prevalent in Eastern European countries with a recent survey showing that 70% of women report some form of IPV since the age of 15 years (Organization for Security and Co-operation in Europe, 2019). What little research there is has shown no association between experience of IPV and parent engagement (Shenderovich et al., 2018). In more general terms, victims of IPV tend to be less likely to access services, although estimates vary due to inconsistencies in reporting and cultural differences (Satyen et al., 2019).
For the Attend stage of engagement, only implementation factors, namely number of completed calls with parents, text messages sent to parents and program fidelity defined as content fidelity, showed significant associations; increased levels of implementation factors were associated with greater parent engagement. This is particularly important given that high levels of implementation fidelity are associated with improvements in parenting practices and child externalizing behavior (Leitao et al., 2020). The results of the qualitative analyses further strengthen these findings with parents identifying facilitator skills and weekly phone calls and/or text messages as supportive of parent engagement. Smith et al. (2015) found that both practitioners and parents identified additional contact between the facilitator and parent as important in terms of reminders of upcoming sessions or when parents missed a session. In a review of the engagement literature, Koerting et al. (2013) also identified additional contact as supporting continued engagement in a parenting program. Given the importance of implementation factors, and additional contact with parents specifically, future studies should ensure that this provision is available during program delivery. This has implications for the time allocation for facilitators.
The qualitative analyses identified four main themes on parent engagement: motivation to attend, valued program components, barriers and supports. Parents wanted to attend the program to learn new skills, improve child behavior/family life, and/or to understand their child’s behavior. These are similar to reasons identified in other BPT research (for a review see Butler et al., 2020). The valued program components were also supportive of other research (e.g., Butler et al., 2020), including the sharing of experiences between parents. It is interesting that practising skills and home activity feedback were identified as valued components as these are key components of effective parenting programs (Kaminski et al., 2008; Leijten et al., 2019) and have been identified as important in other PLH-YC evaluations (e.g., Lachman et al., 2018). These and other delivery strategies are based on social learning theory principles and so social learning theory principles should be considered core components of both the program content and the implementation strategies.
Barriers identified were mostly related to the different delivery schedules of the program in the three countries. Parents in Romania, who received the six-session version, reported that the program was too short and there was not enough time for group discussions within sessions. In a review of the qualitative literature, Butler et al. (2020) also found that parents were wanting longer programs or additional sessions to discuss content in detail. Parents reported the group as being valuable in terms of sharing experiences with others (Butler et al., 2020), emphasising the need for enough time for group discussions. This was also highlighted in Mytton et al. (2014) where the group experience was identified as important for supporting parent participation. In North Macedonia, where parents received the 12-session version in bi-weekly sessions, parents reported wanting more time between sessions to implement the strategies learned. Time constraints is a consistent barrier across much of the literature on parent engagement. Butler et al. (2020) identified contextual barriers for parents attending a program including difficulties in finding time for implementing strategies each week. This would have been further exacerbated in the current study given that parents in North Macedonia were attending two sessions per week and therefore had more strategies to implement in a shorter amount of time. The bi-weekly delivery was not planned in North Macedonia but was a consequence of timing challenges on recruitment and program delivery. Timing was also an issue with the intervention being delivered in the summer. This was particularly challenging for parents in the Republic of Moldova and Romania since many of their children stay with grandparents over the summer and parents therefore had limited opportunities to practice the new skills. Mytton et al. (2014) reported that parents found the timing and frequency of sessions to be a barrier for attending a parenting program given the competing demands such as working patterns. This is supported by Koerting et al. (2013) who found that parents, but not practitioners, identified the timing of sessions to be a significant barrier to accessing services. Lack of childcare was identified as the other barrier, especially in the Republic of Moldova where childcare was not provided. Lack of childcare is often cited as a barrier to parent engagement (Koerting et al., 2013) and when childcare is offered, it is seen as supporting parent engagement in BPT programs (Butler et al., 2020). Addressing logistical barriers such as timing and childcare is of utmost importance in order to ensure parents are able to access parenting programs (Gonzalez et al., 2021b).
Limitations
The study has some limitations. Although it would have been useful to explore the effect of variations in program delivery, it was not possible to examine the country effects separately due to low power. This made the interpretation of results challenging, especially the quantitative results. Also, every effort was made to collect interviews from parents who attended few or no sessions, but very few of these were completed. These parents may have encountered additional or different barriers to those of parents with moderate or high attendance. For example, Lewis et al. (2016) found that parents who were non-completers were more likely to report the presence of obstacles leading to cancelling or rescheduling of sessions. Furthermore, causality cannot be determined. Although numerous other factors were controlled for, it is possible that the relationship between implementation factors (text messages, calls, and fidelity of the intervention) and engagement were due to other reasons not assessed. For example, facilitator skills/experience and facilitator personal qualities has been associated with parent engagement (Koerting et al., 2013; Leitao et al., 2020). Despite the limitations, this study is strong in its use of a mixed-methods design and in contributing to the scarce literature on barriers and supports to parent engagement in Eastern European settings.
Implications
These results have important implications for BPT implementation and policy in these countries. Given the high rates of child maltreatment and low mental health resources in Eastern Europe (WHO, 2013), the identification of factors that support and hinder parent engagement with parenting services could help increase access to services. Very few child and family support services are available (Koves-Masfety et al., 2016) and the high levels of social disadvantage exacerbate the need for such services (Eurostat, 2016). There are problems achieving universal access to services and mental health services are significantly underfinanced (Dlouhy, 2014; Winkler et al., 2017). The study results set the foundation for the successful implementation of the PLH-YC program in the three countries. They help to optimise a family support program that is 1) feasible, 2) scalable, and 3) that make most efficient use of local resources. Relevant supports for program implementation and participation (e.g., text messages, phone calls) as well as barriers (e.g., lack of childcare) were identified. Also, key constrains within the local contexts were reported (e.g., summer holidays). These implementation factors along with others will be addressed during the next phase of the study which examines differential effects of implementation components in a factorial experiment (Lachman et al., 2019). In addition to the promising pre-post effects of the intervention (see Jansen et al., 2021), addressing these implementation factors enhances the probability that the optimised parenting intervention will be implemented successfully, at large scale, and sustainable in the three countries. Future implementation and research would benefit from exploring the role of additional engagement boosters (e.g., regular calls or text messages) as well as peer-support (e.g., facilitators could suggest parents to exchange phone numbers or emphasise that informal meetings of participants have been helpful for other groups). Also, individuals with experiences of IPV could be especially encouraged to attend. In addition, it is important to address barriers for program participation in low-resource settings (e.g., provide childcare and transport vouchers). As needs from families might be different across countries/regions we suggest conducting local formative assessments of facilitators and barriers of engagement prior to implementation (e.g., in a small pilot study), and to ongoing adaptation of the implementation strategies to maximise implementation, reach and sustainability of support services.
References
Achenbach, T. M., & Rescorla, L. (2001). Manual for the ASEBA school-age forms & profiles. Burlington, VT: University of Vermont Research Center for Children, Youth and Families.
Arnold, D. S., O’leary, S. G., Wolff, L. S., & Acker, M. M. (1993). The Parenting Scale: A measure of dysfunctional parenting in discipline situations. Psychological Assessment, 5, 137–144. https://doi.org/10.1037/1040-3590.5.2.137.
Baker, C. N., Arnold, D. H., & Meagher, S. (2011). Enrollment and attendance in a parent training prevention program for conduct problems. Prevention Science, 12, 126–138. https://doi.org/10.1037/1040-3590.5.2.137.
Baydar, N., Reid, J. M., & Webster-Stratton, C. (2003). The role of mental health factors and program engagement in the effectiveness of a preventive parenting program for Head Start mothers. Child Development, 74, 1433–1453. https://doi.org/10.1111/1467-8624.00616.
Bellis, M. A., Hughes, K., Leckenby, N., Jones, L., Baban, A., Kachaeva, M., Povilaitis, R., Pudule, I., Qirjako, G., Ulukol, B., Raleva, M., & Terzic, N. (2014). Adverse childhood experiences and associations with health-harming behaviours in young adults: surveys in eight eastern European countries. Bulletin of the World Health Organization, 92, 641–655. https://doi.org/10.2471/BLT.13.129247.
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3, 77–101. https://doi.org/10.1191/1478088706qp063oa.
Burkey, M. D., Hosein, M., Morton, I., Purgato, M., Adi, A., Kurzrok, M., Kohrt, B. A., & Tol, W. A. (2018). Psychosocial interventions for disruptive behavior problems in children in low‐and middle‐income countries: a systematic review and meta‐analysis. Journal of Child Psychology and Psychiatry, 59, 982–993. https://doi.org/10.1111/jcpp.12894.
Butler, J., Gregg, L., Calam, R., & Wittowski, A. (2020). Parents’ perceptions and experiences of parenting programs: A systematic review and metasynthesis of the qualitative literature. Clinical Child and Family Psychology Review, 23, 176–204. https://doi.org/10.1007/s10567-019-00307-y.
Chacko, A., Jensen, S. A., Lowry, L. S., Cornwell, M., Chimklis, A., Chan, E., Lee, D., & Pulgarin, B. (2016). Engagement in behavioral parent training: Review of the literature and implications for practice. Clinical Child and Family Psychology Review, 19, 204–215. https://doi.org/10.1007/s10567-016-0205-2.
Chacko, A., Wymbs, B. T., Rajwan, E., Wymbs, F., & Feirsen, N. (2017). Characteristics of parents of children with ADHD who never attend, drop out, and complete behavioral parent training. Journal of Child and Family Studies, 26, 950–960. https://doi.org/10.1007/s10826-016-0618-z.
Colman, I., Murray, J., Abbott, R. A., Maughan, B., Kuh, D., Croudace, T. J., & Jones, P. B. (2009). Outcomes of conduct problems in adolescence: 40-year follow-up of national cohort. British Medical Journal, 338, a2981–a2989. https://doi.org/10.1136/bmj.a2981.
Conduct Problem Prevention Research Group (1991). Neighbourhood questionnaire. Retrieved from: http://fasttrackproject.org/techrept/n/nhq/index.php. Accessed 06 July 2020.
Dlouhy, M. (2014). Mental health policy in Eastern Europe: a comparative analysis of seven mental health systems. BMC Health Services Research, 14, 1–8. https://doi.org/10.1186/1472-6963-14-42.
Dumas, J. E., Nissley-Tsiopinis, J., & Moreland, A. D. (2007). From intent to enrolment, attendance, and participation in preventive parenting groups. Journal of Child and Family Studies, 16, 1–26. https://doi.org/10.1007/s10826-006-9042-0.
Dunne, M. P., Zolotor, A. J., Runyan, D. K., Andreva-Miller, I., Choo, W. Y., Dunne, S. K., Gerbaka, B., Isaeva, O., Jain, D., Kasim, M. S., Macfarlane, B., Mamyrova, N., Ramirez, C., Volkova, E., & Youssef, R. (2009). ISPCAN Child Abuse Screening Tools Retrospective version (ICAST-R): Delphi study and field testing in seven countries. Child Abuse & Neglect, 33, 815–825. https://doi.org/10.1016/j.chiabu.2009.09.005.
Eisner, M., & Meidert, U. (2011). Stages of parental engagement in a universal parent training program. Journal of Primary Prevention, 32, 83–93. https://doi.org/10.1007/s10935-011-0238-8.
Eurostat (2016). File: People at risk of poverty or social exclusion by country, 2008 and 2014. Retrieved from: https://ec.europa.eu/eurostat/statistics-explained/index.php/File:People_at_risk_of_poverty_or_ social_exclusion,_by_country,_2008_and_2014.JPG. Accessed 24 Feb 2021.
Eyberg, S. M., Boggs, S. R., & Reynolds, L. A. (1980). Eyberg Child Behavior Inventory. Oregon: University of Oregon Health Sciences Centre.
Frantz, I., Foran, H. M., Lachman, J. M., Jansen, E., Hutchings, J., Băban, A., Fang, X., Gardner, F., Lesco, G., Raleva, M., Ward, C. L., Williams, M. E., & Heinrichs, N. (2019). Prevention of child mental health problems in Southeastern Europe: a multicentre sequential study to adapt, optimise and test the parenting programme ‘Parenting for Lifelong Health for Young Children’, protocol for stage 1, the feasibility study. BMJ Open, 9(1), e026684 https://doi.org/10.1136/bmjopen-2018-026684.
Glasgow, R. E., Vogt, T. M., & Boles, S. M. (1999). Evaluating the public health impact of health promotion interventions: the RE-AIM framework. American Journal of Public Health, 89, 1322–1327. https://doi.org/10.2105/AJPH.89.9.1322.
Godoy, L., Mian, N. D., Eisenhower, A. S., & Carter, A. S. (2014). Pathways to service receipt: Modeling parent help-seeking for childhood mental health problems. Administration and Policy in Mental Health and Mental Health Services Research, 41, 469–479. https://doi.org/10.1007/s10488-013-0484-6.
Gonzalez, C., Morawska, A., & Haslam, D. M. (2021a). A model of intention to participate in parenting interventions: The role of parent cognitions and behaviors. Behavior Therapy, 52, 761–773. https://doi.org/10.1016/j.beth.2020.09.006.
Gonzalez, C., Morawska, A., & Haslam, D. M. (2021b). Profiles of Parents’ Preferences for Delivery Formats and Program Features of Parenting Interventions. Child Psychiatry & Human Development, 1–16. https://doi.org/10.1007/s10578-021-01284-6.
Harvey, E. A., & Metcalfe, L. A. (2012). The interplay among preschool child and family factors and the development of ODD symptoms. Journal of Clinical Child & Adolescent Psychology, 41, 458–470. https://doi.org/10.1080/15374416.2012.673161.
Haggerty, K.P., Fleming, C.B., Lonczak, H.S., Oxford, M. L., Harachi, T. W., & Catalano, R. F. (2002). Predictors of Participation in Parenting Workshops. Journal of Primary Prevention, 22, 375–387. https://doi.org/10.1023/A:1015227623145.
Haine-Schlagel, R., & Walsh, N. E. (2015). A review of parent participation engagement in child and family mental health treatment. Clinical child and family psychology review, 18, 133–150. https://doi.org/10.1007/s10567-015-0182-x.
Heinrichs, N., Bertram, H., Kuschel, A., & Hahlweg, K. (2005). Parent recruitment and retention in a universal prevention program for child behavior and emotional problems: Barriers to research and program participation. Prevention Science, 6, 275–286. https://doi.org/10.1007/s11121-005-0006-1.
Henry, J. D., & Crawford, J. R. (2005). The short-form version of the Depression Anxiety Stress Scales (DASS-21): construct validity and normative data in a large non-clinical sample. British Journal of Clinical Psychology, 44, 227–239. https://doi.org/10.1348/014466505X29657.
Heyman, R. E., Slep, A. M. S., Snarr, J. D., & Foran, H. M. (2013). Practical tools for assessing partner maltreatment in clinical practice and public health settings. In H. M. Foran, S. R. H. Beach, A. M. S. Slep, R. E. Heyman, & M. Z. Wamboldt (Eds.), Family Problems and Family Violence: Reliable Assessment and the ICD-11 (pp. 43–70). New York: Springer.
Janowski, R. K., Wessels, I., Bojo, S., Monday, F., Maloney, K., Achut, V., Oliver, D., Lachman, J. M., Cluver, L., & Ward, C. L. (2020). Transferability of evidence-based parenting programs to routine implementation in postconflict South Sudan. Research on Social Work Practice, 30, 858–869. https://doi.org/10.1177/1049731520932986.
Jansen, E., Frantz, I., Hutchings, J., Lachman, J., Williams, M., Taut, D., Baban, A., Raleva, M., Lesco, G., Ward, C. L., Gardner, F. Fang, X., Heinrichs, N., & Foran, H. M. (2021). Preventing child mental health problems in southeastern Europe: Feasibility study (phase 1 of MOST framework). Family Process. Online First. https://doi.org/10.1111/famp.12720.
Kaminski, J. W., Valle, L. A., Filene, J. H., & Boyle, C. L. (2008). A meta-analytic review of components associated with parent training program effectiveness. Journal of Abnormal Child Psychology, 36, 567–589. https://doi.org/10.1007/s10802-007-9201-9.
Koerting, J., Smith, E., Knowles, M. M., Latter, S., Elsey, H., McCann, D. C., Thompson, M., & Sonuga-Barke, E. J. (2013). Barriers to, and facilitators of, parenting programs for childhood behavior problems: a qualitative synthesis of studies of parents’ and professionals’ perceptions. European Child & Adolescent Psychiatry, 22, 653–670. https://doi.org/10.1007/s00787-013-0401-2.
Kovess-Masfety, V., Keyes, K., Hamilton, A., Hanson, G., Bitfoi, A., Golitz, D., Koc, C., Kuijpers, R., Lesinskiene, S., Mihova, Z., Otten, R., Fermanian, C., & Pez, O. (2016). Is time spent playing video games associated with mental health, cognitive and social skills in young children. Social Psychiatry and Psychiatric Epidemiology, 51, 349–357. https://doi.org/10.1007/s00127-016-1179-6.
Lachman, J. M., Sherr, L., Cluver, L., Ward, C. L., Hutchings, J., & Gardner, F. (2016). Integrating evidence and context to develop a parenting program for low-income families in South Africa. Journal of Child and Family Studies, 25, 2337–2352. https://doi.org/10.1007/s10826-016-0389-6.
Lachman, J. M., Kelly, J., Cluver, L., Ward, C. L., Hutchings, J., & Gardner, F. (2018). Process evaluation of a parenting program for low-income families in South Africa. Research on Social Work Practice, 28, 188–202. https://doi.org/10.1177/1049731516645665.
Lachman, J. M., Heinrichs, N., Jansen, E., Brühl, A., Taut, D., Fang, X., Gardner, F., Hutchings, J., Ward, C. L., Williams, M. E., Raleva, M., Baban, A., Lesco, G., & Foran, H. M. (2019). Preventing child mental health problems through parenting interventions in Southeastern Europe (RISE): Protocol for a multi-country cluster randomized factorial study. Contemporary Clinical Trials, 86, 105855 https://doi.org/10.1016/j.cct.2019.105855.
Lachman, J. M., Alampay, L. P., Jocson, R. M., Alinea, C., Madrid, B., Ward, C., Hutchings, J., Mamauag, B. L., Garilao, M. A. V. F. V., & Gardner, F. (2021). Effectiveness of a parenting programme to reduce violence in a cash transfer system in the Philippines: RCT with follow-up. The Lancet Regional Health-Western Pacific, 17, 100279 https://doi.org/10.1016/j.lanwpc.2021.100279.
Leijten, P., Gardner, F., Mendelez-Torres, G. J., van Aar, J., Hutchings, J., Schulz, S., Knerr, W., & Overbeek, G. (2019). Meta-analyses: Key parenting program components for disruptive child behavior. Journal for the American Academy of Child & Adolescent Psychiatry, 58, 180–190. https://doi.org/10.1016/j.jaac.2018.07.900.
Leitao, S. M., Seabra-Santos, M. J., & Gaspar, M. F. (2020). Therapist factors matter: A systematic review of parent interventions directed at children’s behavior problems. Family Process. Online First, https://doi.org/10.1111/famp.12550
Lewis, E. M., Feely, M., Seay, K. D., Fedoravicis, N., & Kohl, P. L. (2016). Child welfare involved parents and Pathways Triple P: perceptions of program acceptability and appropriateness. Journal of Child and Family Studies, 25, 3760–3770. https://doi.org/10.1007/s10826-016-0526-2.
McCoy, A., Lachman, J. M., Ward, C. L., Tapanya, S., Poomchaichote, T., Kelly, J., Mukaka, M., Cheah, P. Y., & Gardner, F. (2021). Feasibility pilot of an adapted parenting program embedded within the Thai public health system. BMC Public Health, 21, 1–19. https://doi.org/10.1186/s12889-021-11081-4.
McEachern, A. D., Dishion, T. J., Weaver, C. M., Shaw, D. S., Wilson, M. N., & Gardner, F. (2012). Parenting Young Children (PARYC): Validation of a Self-Report Parenting Measure. Journal of Child and Family Studies, 21, 498–511. https://doi.org/10.1007/s10826-011-9503-y.
Meinck, F., Boyes, M. E., Cluver, L., Ward, C. L., Schmidt, P., DeStone, S., & Dunne, M. P. (2018). Adaptation and psychometric properties of the ISPCAN Child Abuse Screening Tool for use in trials (ICAST-Trial) among South African adolescents and their primary caregivers. Child Abuse & Neglect, 82, 45–58. https://doi.org/10.1016/j.chiabu.2018.05.022.
Morawska, A., & Sanders, M. R. (2006). A review of parental engagement in parenting interventions and strategies to promote it. Journal of Children’s Services, 1, 29–40. https://doi.org/10.1108/17466660200600004.
Murphy, K., Embleton, L., Lachman, J. M., Owino, E., Kirwa, S., Makori, D., & Braitstein, P. (2021). “From analog to digital”: The feasibility, acceptability, and preliminary outcomes of a positive parenting program for street-connected mothers in Kenya. Children and Youth Services Review, 127, 106077 https://doi.org/10.1016/j.childyouth.2021.106077.
Mytton, J., Ingram, J., Manns, S., & Thomas, J. (2014). Facilitators and barriers to engagement in parenting programs: A qualitative systematic review. Health Education & Behavior, 41, 127–137. https://doi.org/10.1177/1090198113485755.
Nix, R. L., Bierman, K. L., & McMahon, R. J. (2009). How attendance and quality of participation affect treatment response to parent management training. Journal of Consulting and Clinical Psychology, 77, 429–438. https://doi.org/10.1037/a0015028.
Organization for Security and Co-operation in Europe (2019). Well-being and Safety of Women: OSCE-led survey on violence against women. Vienna, Austria: OSCE. Available at: https://www.osce.org/secretariat/413237?download=true
Pedersen, G. A., Smallegange, E., Coetzee, A., Hartog, K., Turner, J., Jordans, M. J., & Brown, F. L. (2019). A systematic review of the evidence for family and parenting interventions in low-and middle-income countries: child and youth mental health outcomes. Journal of Child and Family Studies, 28, 2036–2055. https://doi.org/10.1007/s10826-019-01399-4.
Piotrowska, P. J., Tully, L. A., Lenroot, R., Kimonis, E., Hawes, D., Moul, C., Frick, P. J., Anderson, V., & Dadds, M. R. (2017). Mothers, fathers, and parental systems: A conceptual model of parental engagement in programs for child mental health – Connect, Attend, Participate, Enact (CAPE). Clinical Child and Family Psychology Review, 20, 146–161. https://doi.org/10.1007/s10567-016-0219-9.
Polanczyk, G. V., Salum, G. A., Sugaya, L. S., Caye, A., & Rohde, L. (2015). Annual research review: a meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. Journal of Child Psychology and Psychiatry, 56, 345–365. https://doi.org/10.1111/jcpp.12381.
Pritchett, R., Kemp, J., Wilson, P., Minnis, H., Bryce, G., & Gillberg, C. (2011). Quick, simple measures of family relationships for use in clinical practice and research. A systematic review. Family Practice, 28, 172–187. https://doi.org/10.1093/fampra/cmq080.
Reyno, S. M., & McGrath, P. J. (2006). Predictors of parent training efficacy for child externalizing behavior problems – a meta-analytic review. Journal of Child Psychology and Psychiatry, 47, 99–111. https://doi.org/10.1111/j.1469-7610.2005.01544.x.
Rhoades, K. A., & O’Leary, S. G. (2007). Factor structure and validity of the parenting scale. Journal of Clinical Child and Adolescent Psychology, 36, 137–146. https://doi.org/10.1080/15374410701274157.
Satyen, L., Rogic, A. C., & Supol, M. (2019). Intimate partner violence and help-seeking behavior: A systematic review of cross-cultural differences. Journal of Immigrant and Minority Health, 21, 879–892. https://doi.org/10.1007/s10903-018-0803-9.
Schumm, W. R., Scanlon, E. D., Crow, C. L., Green, D. M., & Buckler, D. L. (1983). Characteristics of the Kansas Marital Satisfaction Scale in a sample of 79 married couples. Psychological Reports, 53, 583–588. https://doi.org/10.2466/pr0.1983.53.2.583.
Shenderovich, Y., Eisner, M., Cluver, L., Doubt, J., Berezin, M., Majokweni, S., & Murray, A. L. (2018). What affects attendance and engagement in a parenting program in South Africa. Prevention Science, 19, 977–986. https://doi.org/10.1007/s11121-018-0941-2.
Sherbourne, C. D., & Stewart, A. L. (1991). The MOS social support survey. Social science & medicine, 32, 705–714. https://doi.org/10.1016/0277-9536(91)90150-B.
Smith, J. D., Dishion, T. J., Shaw, D. S., & Wilson, M. N. (2013). Indirect effects of fidelity to the Family Check-Up on changes in parenting and early childhood problem behaviors. Journal of Consulting and Clinical Psychology, 81, 962–974. https://doi.org/10.1037/a0033950.
Smith, E., Koerting, J., Latter, S., Knowles, M. M., McCann, D. C., Thompson, M., & Sonuga‐Barke, E. J. (2015). Overcoming barriers to effective early parenting interventions for attention‐deficit hyperactivity disorder (ADHD): Parent and practitioner views. Child: Care, Health and Development, 41, 93–102. https://doi.org/10.1111/cch.12146.
Straus, M. A., & Douglas, E. M. (2004). A short form of the Revised Conflict Tactics Scales, and typologies for severity and mutuality. Violence and Victims, 19, 507–520. https://doi.org/10.1891/vivi.19.5.507.63686.
Tandon, M., & Giedinghagen, A. (2017). Disruptive behavior disorders in children 0 to 6 years old. Child and Adolescent Psychiatric Clinics, 26, 491–502. https://doi.org/10.1016/j.chc.2017.02.005.
The World Bank (2021). New World Bank country classifications by income level: 2021-2022. World Bank Blogs, July 01, 2021. https://blogs.worldbank.org/opendata/new-world-bank-country-classifications-income-level-2021-2022
Ward, C. L., Wessels, I. M., Lachman, J. M., Hutchings, J., Cluver, L. D., Kassanjee, R., Nhapi, R., Little, F., & Gardner, F. (2020). Parenting for Lifelong Health for young children: a randomized controlled trial of a parenting program in South Africa to prevent harsh parenting and child conduct problems. Journal of Child Psychology and Psychiatry, 61, 503–512. https://doi.org/10.1111/jcpp.13129.
Webster-Stratton, C. (1989). Systematic comparison of consumer satisfaction of three cost-effective parent training programs for conduct problem children. Behavior Therapy, 20, 103–115. https://doi.org/10.1016/S0005-7894(89)80121-2.
Wilson, S. M., Wildman, B. G., Ciesla, J., Smith, A. W., & Dempster, R. (2015). Factor structure of the Obstacles to Engagement Scale: Problems, solutions, and hypotheses. Journal of Child and Family Studies, 24, 891–898. https://doi.org/10.1007/s10826-014-9899-2.
Winkler, P., Krupchanka, D., Roberts, T., Kondratova, L., Machů, V., Höschl, C., Sartorius, N., Van Voren, R., Aizberg, O., Bitter, I., Cerga-Pashoja, A., Deljkovic, A., Fanaj, N., Germanavicius, A., Honkov, H., Hovsepyan, A., Ismayilov, F. N., Strkalj, S., Jarema, M., & Thornicroft, G. (2017). A blind spot on the global mental health map: a scoping review of 25 years’ development of mental health care for people with severe mental illnesses in central and eastern Europe. The Lancet Psychiatry, 4, 634–642. https://doi.org/10.1016/S2215-0366(17)30135-9.
World Health Organization (1998). Well-Being Measures in Primary Health Care – the DepCare Project. Copenhagen: WHO Regional Office for Europe.
World Health Organisation (2013). European report on preventing child maltreatment. Copenhagen: WHO Regional Office for Europe.
Acknowledgements
We would like to thank the RISE research team including the data management and assessment team as well as all the facilitators, data assessors, process monitors, program coordinators and research coordinators in North Macedonia, Republic of Moldova and Romania. Also, we thank the partner organizations in each country that helped with the recruitment of parents. Finally, we are grateful for the support of the scientific consultant on the RISE project (Linda Collins), the Data Safety and Monitoring Board (DSMB, Robert McMahon and Terje Ogden), and the Data Protection Officer (DPO, Peter Schartner).
Author Contributions
All authors contributed to the study conception and design. Data analysis were performed by H.M.F. and M.E.W. The first draft of the manuscript was written by M.E.W. and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
This work was funded from the European Union’s Horizon 2020 research and innovation program under grant agreement No 779318.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
H.M.F., D.T., I.F., and M.E.W. declare that they have no competing interests. J.M.L., J.H., and C.L.W. are co-developers of PLH Children, which is licensed under a Creative Commons 4.0 Non-commercial No Derivatives license, and, with colleagues, co-founders of the Parenting for Lifelong Health initiative. J.H. is Co-director of the Children’s Early Intervention Trust, a non-profit institution responsible for the dissemination of the program in Europe. J.M.L. and J.H. receive occasional fees for providing training and supervision of PLH facilitators, coaches, and trainers. J.M.L., J.H., and C.L.W. have participated (and are participating) in a number of research studies involving the program, as investigators, and the University of Oxford, University of Cape Town, and Bangor University receive research funding for these. N.H. serves as an international advisory board member for the Triple P program. Conflict is avoided by declaring this potential conflict of interests; and by conducting and disseminating rigorous, transparent and impartial evaluation research on both this and other similar parenting programs.
Ethical Approval
Ethical approval was granted by the Human Research Ethics Committee of the University of Klagenfurt and local ethics committees in North Macedonia, Republic of Moldova and Romania. All procedures performed in the study were in accordance with the APA ethical standards in the treatment of the study sample.
Informed Consent
Informed written consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

{kind=link}
Cite this article
Williams, M.E., Foran, H.M., Hutchings, J. et al. Exploring Factors Associated with Parent Engagement in A Parenting Program in Southeastern Europe. J Child Fam Stud 31, 3097–3112 (2022). https://doi.org/10.1007/s10826-022-02411-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-022-02411-0