
Abstract
A considerable amount of research has illustrated that negative attitudes toward one’s own aging can directly hinder mental and physical well-being or lead to maladjustment in later stages of life (Swift et al. in Social Issues Policy Rev 11(1):195–231, https://doi.org/10.1111/sipr.12031, 2017). Research so far has focused on the analysis of individual factors related to attitudes toward aging, often related to personality traits. Our study proposes and tests a model of positive contact with aging (PCA). It analyses both individual and social antecedents of attitudes towards one’s own aging, hypothesizing that individual health self-efficacy directly affects attitudes towards one’s own aging and that the quality and quantity of contact with older adults indirectly impacts on attitudes towards one’s own aging through attitudes towards older adults. The model was tested in a wide sample of the Italian population (N = 753) with a varied age range. The PCA model tested showed excellent fit to the data, explaining a moderate amount of variance in attitudes toward one’s own aging (12%). This model promises to offer implications for active policies that can improve attitudes towards one’s own aging, promoting educational strategies to increase intergenerational exchanges and foster health-related self-efficacy.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
In one of his aphorisms, the famous Roman playwright Terenzio stated, “Senectus ipsa est Morbus” (Terenzio, Phormio, 160 B.C.) that is, “old age is in itself a disease”. Despite recent reports in the Global Health Estimates, by the World Health Organization (WHO), that indicate a significant increase in life expectancy globally—rising by 6 years over the past two decades—the aging process is still seen as a challenging phase of human existence.
It would seem that the worries associated with aging are not exclusive to older adults. Younger individuals are also said to associate aging with problems and complications. Studies have shown that a negative attitude toward one’s own aging modifies and influences behaviours throughout one’s life. It is believed to discourage individuals from staying healthy and diminish their commitment to prevention (e.g., Hummert, 1990), which ultimately hinders the process of ‘Active Aging’—the maintenance of positive physical, social and mental health throughout the aging process (e.g., Korkmaz Aslan et al., 2017). The WHO calls for a global pledge to promote active aging, which they define as “the process of optimizing health, participation and safety opportunities in order to improve the quality of life while people get older” (WHO, 2002, p. 12). Hence, the scientific community has accepted the challenge of designing strategies for active and positive aging by undertaking studies on the prevention of negative attitudes—and relevant individual behaviors—that affect the aging processes (Korkmaz Aslan et al., 2017). Despite evidence showing the role of mindset in aging, literature thus far has mainly focused on investigating the effects of negative attitudes, often limiting its scope of research to analyzing individual factors (e.g., Bryant et al., 2016; Kornadt et al., 2019).
The present study aims to supplement this literature by testing a model of positive contact with aging (PCA), which analyses both individual and social antecedents of attitudes towards one’s aging, hypothesizing that individual health self-efficacy directly affects attitudes towards one’s own aging and that the quality and quantity of contact with older adults indirectly impacts on attitudes towards one’s own aging through attitudes towards older adults. The role of sociodemographic variables (namely, gender and age) were also examined. Figures 1 and 2 depicts the model and the following paragraph will explain its theoretical basis. This model promises to offer implications for active policies that can improve attitudes towards aging, promoting educational strategies for a positive aging process.

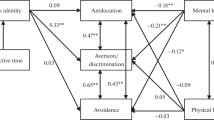
Path coefficients and R2 of the proposed model

Standardized coefficients and R2 of the proposed model. Only significant path are depicted
Attitudes Toward One’s Own Aging, Attitudes Toward Older Adults, and the Contact Hypothesis
Attitudes towards one’s own aging describe individuals’ expectations about the outcome and process of getting older (Wolff et al., 2018). Negative attitudes about one’s aging reflect undesirable losses associated with that process. They may include loss of independence, deteriorating health, and loneliness (Bousfield & Hutchison, 2010); all playing an important role in one’s own aging process (Levy, 2002). It has been speculated that this kind of perception influences outcomes through behavioural, physiological, and psychological processes which, in turn, may affect health outcomes too (Levy, 2009).
In recent years, a significant amount of literature has documented the association of negative attitudes toward one’s own aging with various health outcomes, such as a broad range of physical health, including cardiovascular diseases, circulatory problems, back or joint conditions, diabetes, gastrointestinal diseases and respiratory diseases (Gale & Cooper, 2018; Levy, 2009; Wurm et al., 2007). They also affect cognitive functioning (Schönstein et al., 2021), depression and anxiety (Lai, 2009; Wurm & Benyamini, 2014), and mortality rate (Kotter-Grühn et al., 2009; Sargent-Cox et al., 2014).
The ‘Risks of Ageism Model’ (RAM, Swift et al., 2017) suggested that a possible theoretical explanation of how negative attitudes toward aging affects the aging process is the result of stereotype processes. It is proposed that representations about aging are implicitly internalized throughout life (Levy, 2009; Swift et al., 2017). Thus, over time, stereotypically shared beliefs about old age can become detrimental to the individuals who embrace them and can ultimately lead to poorer physical and social health (Levy, 2003; Nussbaum et al., 2005; Robertson et al., 2015; Wurm et al., 2013).
Evidence suggested that people who expect worse outcomes from aging hold stereotypes about older adults (Levy, 2009). Thus, attitudes toward older adults can be one of the main predictors of negative attitudes toward one’s own aging. Negative attitudes toward older adults is a serious international concern. According to Swift et al. (2017), there can be economic and sociological explanations that have caused society to evolve in ageist ways. For example, capitalist societies may have contributed to the marginalization of older people by considering them as economically unproductive (Cowgill, 1974; Macnicol, 2006). Intergroup threat theory consistently suggests that older people are perceived as a burden on health care and welfare resources (Stephan & Stephan, 2000). Alternatively, the terror management theory suggests that age prejudices arise out of a fear of our own mortality (Chonody & Teater, 2016; Greenberg et al., 2002).
Notwithstanding the complexity of negative prejudices about older people, it has been shown that one successful strategy to reduce negative attitudes toward older adults is through intergenerational contact (Hagestad & Uhlenberg, 2005; Kotter-Grühn, 2015). This strategy is based on the ‘contact hypothesis’ which posits that contact between groups reduces prejudice by decreasing anxiety, while increasing empathy and knowledge about the other group (Allport, 1954). Contact between various age groups can be extended to everyday intergenerational contact within families, at the workplace, and in health and social service settings. A significant number of empirical studies highlight that ‘quality’ intergenerational interactions aid the formation of positive attitudes towards older adults (Gaggioli et al., 2014; Harwood et al., 2005; McKeown et al., 2006; Pinquart & Forstmeier, 2012; Roodin et al., 2013; Adorni et al., 2022).
Based on the literature mentioned above, the model of Positive Contact with Aging (PCA) that we propose in the current study suggests that negative attitudes toward one’s own aging are a direct consequence of negative attitudes toward older people, which in turn are derived from the (lack of) quality and quantity of contact with older adults (Fig. 1). Several studies have already reported that positive contact with older adults is associated with reduced negative attitudes toward older people (Drury et al., 2017; Hawkley et al., 2019). In addition, the ‘Positive Education on Aging and Contact Experience’ (PEACE; Levy, 2018) model presented the argument that the quality and quantity of positive contact with adults improve attitudes towards older people and attitudes toward one’s own aging (Levy, 2018). Nevertheless, to our knowledge, our proposed mediational hypothesis has never been tested. In analyzing this hypothesis, we will also take into consideration another individual factor: the perception of control people has over their own health, defined as health-related self-efficacy.
Health-Related Self-efficacy
Self-referential processes operate by enabling individuals to function as agents of self-regulation, allowing control over personal experiences. Among the most influential self-referential mechanisms of personal agency, the perception of self-efficacy is certainly the most influential motivational engine in enabling people to achieve desired outcomes by reinforcing the belief that they are producing positive effects with their actions (see Bandura, 1997, 2001; Caprara et al., 2006).
It turns out that perceived self-efficacy plays a key role not only in directly influencing actions and self-regulatory processes, but also (and especially) through its positive impact on cognitive, motivational, decision-making and affective determinants (e.g., Lunenburg, 2011; Opoku et al., 2022). It is therefore conceivable that, just as self-efficacy is known to have a positive impact in domains related to learning, work, well-being, and health (for a review, see Bandura, 1997, 2001), then it may also have a positive impact on the attitudes and evaluations people have toward aging.
Individual views on aging are closely connected with control beliefs (Heckhausen & Baltes, 1991). Health-related self-efficacy refers to beliefs about one’s ability to take appropriate action to produce positive health outcomes (Sheeran et al., 2016). Empirical evidence has often shown that self-efficacy is one of the most significant predictors of behavioural intentions and health behaviours (DiClemente et al., 1995). People of different health states, ages and ethnic groups decide whether to adopt healthy behaviours by exercising their self-efficacy evaluations (Mâsse & Anderson, 2003; Resnick et al., 2004; Sohng et al., 2002).
Indeed, as several studies have shown, the perception—positive or negative—of one’s own efficacy impacts variables related to health, success and relationships. For example, the lack of a positive perception of self-efficacy in the major domains of their lives, and thus a sense of ineffectiveness, leads young adults to be more vulnerable to stress (Flammer, 1995; Schneewind, 1995). Just as there is evidence that a sense of self-efficacy also positively impacts the quality of communication with parents and family members (Caprara et al., 2005).
However, self-efficacy theory does not specifically address the impact of self-efficacy on attitudes. Nonetheless, research findings show a positive impact of self-efficacy on attitudes in different areas (Laganà, 2008; Valencia-Vallejo et al, 2016).
Longitudinal data have, for example, shown that adolescents’ perceptions of self-efficacy across multiple domains of life exert a positive influence on positive thinking, particularly the positive view they have of themselves and their lives, as well as their positive expectations about their futures (Caprara et al., 2011). As far as the aging process is concerned, Brandtstädter (1992) suggested that self-efficacy beliefs are regarded as having vital importance in maintaining an optimistic perspective on personal development in middle and later adulthood (see also Rejeski et al., 2001). This leads us to hypothesize that perceived self-efficacy may also improve not only individual health self-efficacy by improving preventive behaviours and attention to one’s own physical health, but also by improving attitudes toward one’s own and others’ perceptions of aging. If an individual has a positive perception of his or her own health-related efficacy and positive contact with adults increases positive attitudes toward older adults, then these two variables together will greatly improve attitudes toward one’s own aging. That said, the direct impact of health-related self-efficacy and attitudes toward one’s own aging has never been empirically tested.
When analyzing individual factors that affect attitudes toward one’s own aging, the available literature has mainly focused on personality factors and emotions (Vize et al., 2022; Wahyuni & Krisnatuti, 2022). Through the PCA model, we analysed health-related self-efficacy beliefs for the first time, which might be regarded as a more effective tool for identifying the true barriers to positive aging and hence designing strategies to promote it.
The role of the sociodemographic variables (namely, gender and age) will be also examined. As for the association between these variables and attitudes toward one’s own aging, previous studies have reported that the attitudes toward one’s own aging become more negative with increasing age (Bryant et al.., 2016; Cummings et al., 2000; Schelling & Martin, 2008) and that women report greater anxiety related to their own aging process than men (Barrett & von Rohr, 2008; Cummings et al., 2000). In relation to attitudes toward older people, a systematic review on this topic (Marques et al., 2020) attests that the age and gender of respondents are the two individual-level determinants most commonly explored, though the majority of studies did not find a consistent age or gender effect. In testing our model, we controlled the age and gender of the participants to explore their effect on the variable of the model tested and to see if the effects on the hypothesized model could vary in function of these variables (see Fig. 2).
The Current Study
The purpose of this study is to test the PCA model, which specifically states that positive attitudes toward aging and a positive perception of health-related self-efficacy directly predicts a positive attitude toward one’s own aging. This, indirectly, is determined by the quality and quantity of contact one has with older adults, which, in turn, enhances attitudes toward one’s own aging.
In other words, attitudes toward one’s own aging are predicted directly by attitudes toward older adults and health-related self-efficacy and indirectly by the quality and quantity of contact with older people. Contact, through its quality and quantity, improves attitudes toward older people, and these positive attitudes, together with perceived health-related self-efficacy, improve attitudes toward one’s own aging (Fig. 1).
Socially shared beliefs that aging produces exclusively negative physical and psychosocial consequences can be changed by being in contact with older adults. It thus allows people to get in touch with the positive characteristics of older adults, generalizing it to attitudes toward older people in general and, in particular, improving attitudes toward their own aging. The same positive effect is produced by perceived self-efficacy, which is itself a predictor of good attitudes toward one’s own aging.
Materials and Methods
Participants
The data were collected via an anonymous online survey using a snowball sampling method between March and November 2020. The volunteers were recruited among the researchers’ pool of acquaintances, word of mouth, and online social networks. Eligible participants were between 18 and 65 years old and were all native Italian speakers. 753 participants took part in the online survey, 32% males and 68% females, with a mean age of 34.39 (SD = 13.33, range 18–64). The majority of respondents were educated to high school diploma level (45%) and lived in the north-west of Italy (52%). A detailed description of the sociodemographic characteristics of the sample is reported in Table 1.
The sample size adequacy was established by using Power Analysis (Cohen, 1988) and G*Power Version 3.1.9.7 (Faul et al., 2007). We calculated the sample size requested to perform ANCOVA with the following parameters—Effect size f = 0.25, α = 0.05, Power = 0.95. The first parameter indicates a medium effect size (Cohen, 1988). The following two parameters reflect the most widely used significance criterion and the generally accepted power level, respectively (Cohen, 1988). The sample comprised 386 individuals. Based on these considerations, the sample size of the study was adequate to determine medium-size effects. The study received the approval of the Ethical Committee of the Università Cattolica del Sacro Cuore of Milan, and all methods were performed following the relevant guidelines and regulations.
Procedure and Measures
The online survey was created and administered using the Qualtrics Platform. The first page of the online survey detailed the objective of the study and asked participants to provide their informed consent digitally, declaring to have read and accepted the confidentiality regulation. Participation was anonymous and participants could stop the research at any time without any consequences. The first part of the questionnaire collected information about socio-demographic indicators. After that, the participants responded to a series of scales described below.
Quantity of contact with older adults was measured through two items adapted from the Italian scale of Voci and Hewstone (2003), which focused on the frequency of contact with older adults in general and during a single day (“How many opportunities for contact do you have with people over 70? On a typical day, how often do you deal with people over 70?”). The scale ranged from 1 (rarely) to 5 (very often). A mean score between the two items was calculated (Pearson r = 0.63; p < 0.001), with a higher score reflecting higher frequency of contact.
Quality of contact with older adults was assessed using a semantic differential scale based on a validated Italian scale (Maggino & Mola, 2007). Participants were asked to rate their relationship with people over 70 they were in contact with using four pairs of opposite adjectives. The scale ranged from 1 (e.g., Cold) to 7 (e.g., Warm). The items were ‘Cold-Warm’, ‘Indifferent-Engaging’, and ‘Unfriendly-Friendly’, ‘Formal-Informal’. A mean score between the four items was calculated, with a higher score reflecting the depth of contact. In line with Cronbach’s recommendations (Cronbach, 1951), the scale showed an adequate internal consistency (Cronbach’s alpha = 0.86).
Health-related self-efficacy was assessed using a 9-item scale adapted from a validated Italian scale created by one of the authors of the present study (Steca et al., 2015). The items of the original scale were about self-efficacy referring to a specific medical condition. The reference to that disease was removed from the items used for the present study. Participants were asked to indicate how inclined they were to engage in a range of health-related behaviours. An example item is, “I feel capable of understanding when it is appropriate to seek medical attention for a physical condition.” The scale ranged from 1 (not at all capable) to 5 (completely capable). The final score was the mean score across the 9 items. A higher score reflected greater health-related self-efficacy. Because we used an adapted version of this scale, we performed Confirmatory Factor Analysis (CFA) to test the validity of the scale. The results indicated that the one-factor solution fit the data adequately (Chi-squared = 131.61, df = 24, p < 0.001; CFI = 0.956; SRMR = 0.038; RMSEA = 0.077, 90% CI [0.07, 0.09]). The scale showed an adequate internal consistency (Cronbach’s alpha = 0.85).
Attitudes towards older people and attitudes towards one’s own aging were measured using a brief version of the Anxiety about Aging Scale (AAS, Lasher & Faulkender, 1993). Participants were asked to indicate their agreement through a set of statements. The scale of attitudes toward older people was made up of three items (e.g., “I feel very comfortable when I am close to an older adult”); the scale of attitudes toward one’s own aging was made up of seven items (e.g., “It does not bother me at all to imagine myself as an older adult”). The scale ranged from 1 (strongly disagree) to 5 (strongly agree). The final score of each scale was represented by the mean score between items. A higher score reflected a more positive attitude towards older people and attitudes toward one’s own aging, respectively. The original items were translated from English to Italian. First, one of the authors carried out an independent forward translation. Secondly, the authors of the study organized a focus group to discuss the results of the translation and produce the final version of the scale. As we used a brief Italian version of this scale, not previously validated in the Italian context, we performed Confirmatory Factor Analysis (CFA) to test its validity. The results indicated that the two-factor solution fit the data adequately (Chi-squared = 117.79, df = 32, p < 0.001; CFI = 0.968; SRMR = 0.037; RMSEA = 0.060, 90% CI [0.05, 0.07]). The two scales (attitudes towards older adults and attitudes toward one’s own aging) showed good internal consistency (Cronbach’s α = 0.89 and 0.78 respectively).
Data analysis
The items of the scales created ad hoc for the present study underwent a preliminary analysis to check the normal distribution by calculating mean, standard deviation (SD), and indices of skewness and kurtosis through SPSS. Following Barbaranelli (2007), we considered skewness >|1| and kurtosis >|1| as indicative of asymmetrical distribution. Confirmatory Factor Analysis (CFA) was performed through SPSS (AMOS module) to test the validity of the scales created ad hoc or adapted for the present study. Hu and Bentler’s guidelines (1999) were used to determine if the expected model was plausible based on the data. Parameter estimates were computed using a maximum likelihood estimation method, while an optimal model fit was evaluated using the following criteria: a comparative fit index (CFI) of 0.95 or more, a standardized root mean squared residual (SRMR) of 0.05 or less, and a root mean square error of approximation (RMSEA) of 0.05 or less. Cronbach’s α was calculated through SPSS to examine internal consistency. Cronbach’s α higher than 0.60 was considered acceptable (Nunnally & Bernstein, 1994). Before running the analyses, data were screened through SPSS for the presence of multivariate outliers and tested for univariate normality, examining box plots, skewness and kurtosis values, and the Mahalanobis distance (Tabachnick & Fidell, 2007).
We tested our hypothesis on the predictive effect of the sociodemographic (gender, age) and psychological variables (quantity and quality of contact with older adults, health-related self-efficacy, and attitude toward older people) on attitudes towards one’s own aging, through a path model, by means of Jamovi (Version 2.2.5, The Jamovi project, 2021, retrieved from https://www.jamovi.org). Parameter estimates were computed using the method mentioned above. The non-parametric bootstrapping method (based on 5000 replications) was used to calculate standard error and confidence intervals of indirect effects (Cheung & Lau, 2008). The size of the standardized regression weights was evaluated according to guidelines (≥ .10, small; ≥ .30 medium; ≥ .50 large; Cohen, 1988). All statistical tests were two-tailed, and a p ≤ .05 was considered statistically significant.
Results
Descriptive statistics for all variables of interest are reported in Table 2. Zero-order correlations among all variables of the path analysis are reported in Table 3. All variables were normally distributed. We found 2 multivariate outliers, which were subsequently removed from the dataset.
We then tested our proposed model (see Fig. 1) through path analysis. In the tested model we also modelled covariance between quantity and quality of contact with older adults (r = 0.37, p < 0.001). No other covariances were estimated. The model showed an optimal fit to the data (Χ2 = 10.199, df = 5, p = 0.070; RMSEA = 0.037, 90% CI [0.00, 0.07]; CFI = 0.983; SRMR = 0.035).
Regarding the direct effects, we found that the quality and quantity of contact with older adults were significantly associated with attitude toward older people. Moreover, attitude toward older adults and attitude toward one’s own aging were significantly associated. Finally, health-related self-efficacy was significantly associated with attitudes toward one’s own aging—greater self-efficacy corresponded to a more positive attitude towards one’s own aging. Regarding the indirect effects, we found that quality and quantity of contact with older people were associated with attitudes toward one’s own aging through a mediating effect of attitude toward older people.
To assess for the effects of age and gender, we tested a further model where age and gender were related to all the variables in the model. The results found in the basic model did not change when adding age and gender to it. Table 4 report unstandardized regression weight, standard errors and standardized regression weights for the direct and indirect paths, respectively. Figure 2 shows the path coefficients and R2 of the model.
Regarding the role of age, we found that the older the age of the respondents, the greater the quantity of contact (β = 0.205; p < 0.001). We also found a significant path (β = − 0.091; p = 0.007) between age and a negative attitude towards older adults.
Regarding the role of gender (1 = male and 2 = women), we found that women had a greater quantity and quality of contact with older adults than men (β = − 0.128; p < 0.001 and β = − 0.150; p < 0.001, respectively); they also showed a more positive attitude towards older adults than men (β = − 0.113; p < 0.001), and a more negative attitude (β = − 0.113; p < 0.001) towards their own aging than men (β = − 0.087; p = 0.014).
Discussion
A considerable amount of research has illustrated that negative attitudes toward one’s aging can directly hinder mental and physical well-being or lead to maladjustment in later stages of life (Swift et al., 2017). With the aim of analyzing how to help people to grow old positively, we focus our attention on attitudes toward one’s own aging. Research so far has focused on the analysis of individual factors, often related to personality traits. Our study has analysed aspects both at the individual level (such as health-related self-efficacy and attitude toward older adults) and at the social level (the quantity and quality of contact with older people) that could be changed and therefore promoted by socio-political interventions. The model was tested in a wide sample of the Italian population with a varied age range.
The PCA model tested showed an excellent fit to the data, explaining a moderate amount of attitudes toward one’s own aging (12%). Hence, based on the results obtained to prevent the formation of negative attitudes toward one’s own aging, it is necessary, first and foremost, to foster contact with the people who are going through that change: older people. Exposure and contact with older adults may contribute to diluting some prejudices which are seen as obstructing one’s own positive aging process.
Typically, the most common stereotypes about older people refer to a decrease in both physical and cognitive competence (Fiske et al., 2002; Lamont et al., 2015). Other commonly shared perceptions are that older people are fragile, overly dependent on their family, asexual, and socially isolated as well as lacking creativity and unable to learn new skills (Hummert et al., 1994; Swift et al., 2013). Furthermore, it appears that people tend to overestimate the effects of aging on memory, the likelihood and incidence of Alzheimer’s disease, and the rates of poverty and depression among older adults (Cherry et al., 2014; Palmore, 1990). Through positive contact with older people, some of these stereotypes are challenged and may result in a deeper level of understanding of the complexity of the aging process which, in turn, can equip individuals with the psychological tools to anticipate a healthier older age, and thus develop less negative attitudes towards their own aging. In dealing with older adults, younger people can foster the notion that aging is a process that can cross people’s lives unevenly and lead to different outcomes; developing a better awareness of one’s ability to cope with old age and its relevant challenges. In other words, achieving a higher degree of health-efficacy would become particularly important at that point. It is necessary to specify that the model presented can be conceived as circular, rather than directional, because a better attitude toward one’s own aging may improve the attitude toward older people and vice versa.
Finally, consistent with the findings in other studies (e.g., Faudzi et al., 2020), negative attitudes toward one’s own aging are significantly related to gender in that women report more negative attitudes toward their ageing. We also found significant gender and age differences about attitudes toward older people—women and older participants show more positive attitudes toward older people (Hawkins, 1996; Rupp et al., 2005). Moreover, age and gender were also significantly associated with the quantity of contact with older people. It appears that young people and men seem to have lower chances of being in contact with older adults and are at particular risk of holding negative attitudes toward them.
Therefore, the issue requires a twofold approach. Firstly, increasing intergenerational exchanges is vital especially for young people, as it has been shown in a systematic review (Burnes et al., 2019). In particular the family context seems to play a pivotal role. To that end, studies have shown that close and intimate contact with grandparents results in a greater ability to take on his or her point of view, developing feelings of empathy for that person and, consequently, a greater understanding and more positive affection toward older people (Harwood et al., 2005). This is consistent with research showing that an out-group member (and, in turn, his or her out-group) can be included in an extended notion of the self (Aron et al., 2001). In addition, other studies have shown that individuals that have nurtured strong relationships with their grandparents hold more conspicuous political support for policies that are geared toward the enhancement of life of older adults (Silverstein & Parrott, 1997). As far as gender, it is well known that it is women who take care of the older adults in the family and thus have more contact with the older generation (Pinquart & Sorensen, 2003). This may explain why women are less victims of ageism than men. A more equal distribution of care burdens in the family in relation to the needs of the older adults could therefore also lead to a better attitude towards the older adults on the part of men.
Outside the family context, programmes designed around longer-term, more sustained contact with older people at work and other social contexts have resulted in more positive perceptions of older adults (Hernandez & Gonzalez, 2008). Thus, the research suggests that policymakers should investigate the potential for developing close intergenerational relationships over time. By facilitating an information-sharing process that aims at developing empathy and a shared desire to live in a mixed society in which ‘old age’ is seen as a resource, we can generate positive interactions and successfully challenge the stereotypes brought about by negative attitudes toward older adults (Harwood et al., 2005; Soliz & Harwood, 2006; Tam et al., 2006).
At the same time, it is necessary to foster a perception of health-related self-efficacy. Bandura (1977) presented four sources of self-efficacy: performance accomplishments, vicarious experience, verbal persuasion and physiological states. The former two have been used successfully in trial intervention as a way of fostering self-efficacy related to health behaviours (e.g., Bouwman et al., 2020; Parent & Fortin, 2000). Performance accomplishments, or mastery, refer to instances in which individuals have successfully applied positive behaviour which, consequently, boosted self-efficacy. Vicarious experiences, or modeling, are those in which an individual witnesses others successfully perform the desired behaviour. Seeing people perform the behaviour and succeed confirms to others that they all have the potential to perform that desired behaviour and provides vital information about how success can be achieved. According to meta-analyses studies, the types of intervention related to performance accomplishments and vicarious experience, particularly effective in health-related contexts, are those that use self-monitoring techniques: reinforcement and positive feedback, modeling and/or informing an individual how to act (Prestwich et al., 2014; Williams & French 2011).
Finally, we have to acknowledge that some meso-level aspects must be kept in mind when developing health self-efficacy and positive contact between generations. Institutional support for intergenerational exchange in all areas of social life should be fostered and promoted at institutional level. Conversely, there are many economic and care-related factors that can weigh on the formation of health-related self-efficacy. Being able to rely on an efficient local health care system that can respond to citizens' health problems in a timely manner is certainly a necessary and indispensable factor.
Lastly, some limitations of the present study must be mentioned. As we explored psychological indicators and attitudes in a sample of adults aged 19 to 65 enrolled through a snowball sampling method, our convenience sample was not representative of the general Italian population. Also, our results are specific to the Italian cultural context. Considering that cultural differences play an important role in attitude formation, it would be desirable to replicate this study to test the validity of our model in other cultural settings. Indeed, some recent research has indicated that population aging and socioeconomic development may play an important role in aging attitudes and that the effects may differ among individual cultures based on specific beliefs about aging (Lockenhoff et al., 2015). In particular, historical and ecological determinants in many Eastern cultures result in a higher likelihood of building stable relationships with people outside one’s “group” (Voronov & Singer, 2002) and that values such as filial piety and respect for older people are more commonly practiced in Eastern cultures (Lin & Bryant, 2009). One last consideration is the cross-sectional design, which makes it difficult to establish accurately the causal relationship between variables. Similar studies adopting a longitudinal and experimental approach may address this limitation.
However, notwithstanding its weaknesses, the PCA model provides a highly applicable method for reducing negative attitudes toward one’s own aging which would not only improve the life of older adults, but also promote an active aging process among all adults.
Data Availability
Data is available upon request to the first author.
References
Adorni, R., Manzi, C., Crapolicchio, E., & Steca, P. (2022). The role of the family doctor’s language in modulating people’s attitudes towards hearing loss and hearing aids. Health & Social Care in the Community, 30(5), e1775–e1784. https://doi.org/10.1111/hsc.13606
Allport, G. W. (1954). The nature of prejudice. Perseus Books.
Aron, A., Aron, E. N., & Norman, C. (2001). The self expansion model of motivation and cognition in close relationships and beyond. Interpersonal processesIn M. Clark & G. Fletcher (Eds.), Blackwell handbook in social psychology (Vol. 2, pp. 478–501). Basil Blackwell.
Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84, 191–215. https://doi.org/10.1037/0033-295X.84.2.191
Bandura, A. (1997). Self-efficacy: The exercise of Control. Freeman.
Bandura, A. (2001). Social cognitive theory: An agentic perspective. Annual Review of Psychology, 52, 1–26. https://doi.org/10.1146/annurev.psych.52.1.1
Barbaranelli, C. (2007). Analisi dei dati: tecniche multivariate per la ricerca psicologica e sociale. Edizioni universitarie di lettere economia diritto.
Barrett, A. E., & Von Rohr, C. (2008). Gendered perceptions of aging: An examination of college students. The International Journal of Aging and Human Development, 67(4), 359–386. https://doi.org/10.2190/AG.67.4.d
Bousfield, C., & Hutchison, P. (2010). Contact, anxiety, and young people’s attitudes and behavioral intentions towards the elderly. Educational Gerontology, 36(6), 451–466.
Bouwman, E. P., Onwezen, M. C., Taufik, D., de Buisonjé, D., & Ronteltap, A. (2020). Brief self-efficacy interventions to increase healthy dietary behaviours: Evidence from two randomized controlled trials. British Food Journal, 122(11), 3297–3311. https://doi.org/10.1108/BFJ-07-2019-0529
Brandtstädter, J. (1992). Personal control over development: Some developmental implications of self-efficacy. Self-efficacy: Thought control of action, 127–145.
Bryant, C., Bei, B., Gilson, K. M., Komiti, A., Jackson, H., & Judd, F. (2016). Antecedents of attitudes to aging: A study of the roles of personality and well-being. The Gerontologist, 56(2), 256–265. https://doi.org/10.1093/geront/gnu041
Burnes, D., Sheppard, C., Henderson, C. R., Jr., Wassel, M., Cope, R., Barber, C., & Pillemer, K. (2019). Interventions to reduce ageism against older adults: A systematic review and meta-analysis. American Journal of Public Health, 109(8), e1–e9.
Caprara, G. V., Capanna, C., Steca, P., & Paciello, M. (2005). Misura e determinanti personali della prosocialita. Un approccio sociale cognitivo (Measurement and personal determinants of prosocialness. A social-cognitive approach). Giornale Italiano di Psicologia, 32, 287–307. https://doi.org/10.1421/20313
Caprara, G. V., Steca, P., Gerbino, M., Paciello, M., & Vecchio, G. M. (2006). Looking for adolescents’ well-being: Self-efficacy beliefs as determinants of positive thinking and happiness. Epidemiology and Psychiatric Sciences, 15(1), 30–43. https://doi.org/10.1017/S1121189X00002013
Caprara, G. V., Vecchione, M., Alessandri, G., Gerbino, M., & Barbaranelli, C. (2011). The contribution of personality traits and self-efficacy beliefs to academic achievement: A longitudinal study. British Journal of Educational Psychology, 81(1), 78–96. https://doi.org/10.1348/2044-8279.002004
Cherry, K. E., Blanchard, B., Walker, E. J., Smitherman, E. A., & Lyon, B. A. (2014). Knowledge of memory aging across the lifespan. The Journal of Genetic Psychology: Research and Theory on Human Development, 175(6), 547–553. https://doi.org/10.1080/00221325.2014.982069
Cheung, G. W., & Lau, R. S. (2008). Testing mediation and suppression effects of latent variables: Bootstrapping with structural equation models. Organizational Research Methods, 11(2), 296–325. https://doi.org/10.1177/1094428107300343
Chonody, J. M., & Teater, B. (2016). Why do I dread looking old? A test of social identity theory, terror management theory, and the double standard of aging. Journal of Women & Aging, 28, 112–126. https://doi.org/10.1080/08952841.2014.950533
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. Laurence Erlbaum.
Cowgill, D. O. (1974). Aging and modernization: a revision of the theory. In J. F. Gubrium (Ed.), Late life: Communities and environmental policy (pp. 123–146). Charles C. Thomas.
Cummings, S. M., Kropf, N. P., & Weaver, K. L. D. (2000). Knowledge of and attitudes toward aging among non-elders: Gender and race differences. Journal of Women & Aging, 12(1–2), 77–91. https://doi.org/10.1300/J074v12n01_06
Cronbach, L. J. (1951). Coefficient alpha and the internal structure of tests. Psychometrika, 16(3), 297–334.
DiClemente, C. C., Fairhurst, S. K., & Piotrowski, N. A. (1995). Self-efficacy and addictive behaviors. In Self-efficacy, adaptation, and adjustment (pp. 109–141). Springer.
Drury, L., Abrams, D., & Swift, H. J. (2017). Evidence review: Making intergenerational connections: What are they, why do they matter and how to make more of them. Age UK.
Faudzi, F. N. M., Armitage, C. J., Bryant, C., & Brown, L. J. (2020). Moderating effects of age on relationships between attitudes to aging and well-being outcomes. Aging & Mental Health, 24(10), 1620–1626. https://doi.org/10.1080/13607863.2019.1619167
Faul, F., Erdfelder, E., Lang, A. G., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39(2), 175–191. https://doi.org/10.3758/bf03193146
Fiske, S. T., Cuddy, A. J., Glick, P., & Xu, J. (2002). A model of (often mixed) stereotype content: Competence and warmth respectively follow from perceived status and competition. Journal of Personality and Social Psychology, 82(6), 878–902.
Flammer, A. (1995). Developmental analysis of control beliefs. In A. Bandura (Ed.), Self-efficacy in changing societies (pp. 69–113). Cambridge University Press.
Gaggioli, A., Morganti, L., Bonfiglio, S., Scaratti, C., Cipresso, P., Serino, S., & Riva, G. (2014). Intergenerational group reminiscence: A potentially effective intervention to enhance elderly psychosocial wellbeing and to improve children’s perception of aging. Educational Gerontology, 40(7), 486–498. https://doi.org/10.1080/03601277.2013.844042
Gale, C. R., & Cooper, C. (2018). Attitudes to aging and change in frailty status: The English Longitudinal Study of Aging. Gerontology, 64(1), 58–66. https://doi.org/10.1159/000477169
Greenberg, J., Schimel, J., & Martens, A. (2002). Ageism: denying the face of the future. In T. D. Nelson (Ed.), Ageism: Stereotyping and prejudice against older persons (pp. 3–26). MIT Press.
Hagestad, G. O., & Uhlenberg, P. (2005). The social separation of old and young: A root of ageism. Journal of Social Issues, 61, 343–360. https://doi.org/10.1111/j.1540-4560.2005.00409.x
Harwood, J., Hewstone, M., Paolini, S., & Voci, A. (2005). Grandparent-grandchild contact and attitudes toward older adults: Moderator and mediator effects. Personality and Social Psychology Bulletin, 31(3), 393–406. https://doi.org/10.1177/0146167204271577
Hawkins, M. J. (1996). College students’attitudes toward elderly persons. Educational Gerontology: An International Quarterly, 22(3), 271–279. https://doi.org/10.1080/0360127960220305
Hawkley, L. C., Norman, G. J., & Agha, Z. (2019). Aging expectations and attitudes: Associations with types of older adult contact. Research on Aging, 41(6), 523–548. https://doi.org/10.1177/0164027518824291
Heckhausen, J., & Baltes, P. B. (1991). Perceived controllability of expected psychological change across adulthood and old age. Journal of Gerontology, 46(4), P165–P173. https://doi.org/10.1093/geronj/46.4.P165
Hernandez, C. R., & Gonzalez, M. Z. (2008). Effects of intergenerational interaction on aging. Educational Gerontology, 34(4), 292–305. https://doi.org/10.1080/03601270701883908
Hu, L. T., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 1–55. https://doi.org/10.1080/10705519909540118
Hummert, M. L. (1990). Multiple stereotypes of elderly and young adults: A comparison of structure and evaluations. Psychology and Aging, 5(2), 182–93. https://doi.org/10.1037/0882-7974.5.2.182
Hummert, M. L., Garstka, T. A., Shaner, J. L., & Strahm, S. (1994). Stereotypes of the elderly held by young, middle-aged, and elderly adults. Journal of Gerontology, 49(5), P240–P249. https://doi.org/10.1093/geronj/49.5.P240
Korkmaz Aslan, G., Kartal, A., Özen Çınar, İ, & Koştu, N. (2017). The relationship between attitudes toward aging and health-promoting behaviours in older adults. International Journal of Nursing Practice, 23(6), e12594. https://doi.org/10.1111/ijn.12594
Kornadt, A. E., Siebert, J. S., & Wahl, H. W. (2019). The interplay of personality and attitudes toward own aging across two decades of later life. PLoS ONE, 14(10), e0223622. https://doi.org/10.1371/journal.pone.0223622
Kotter-Grühn, D. (2015). Changing negative views of aging: Implications for intervention and translational research. Annual Review of Gerontology and Geriatrics, 35(1), 167–186. https://doi.org/10.1891/0198-8794.35.167
Kotter-Grühn, D., Kleinspehn-Ammerlahn, A., Gerstorf, D., & Smith, J. (2009). Self-perceptions of aging predict mortality and change with approaching death: 16-year longitudinal results from the Berlin Aging Study. Psychology and Aging, 24(3), 654. https://doi.org/10.1037/a0016510
Laganà, L. (2008). Enhancing the attitudes and self-efficacy of older adults toward computers and the internet: Results of a pilot study. Educational Gerontology, 34(9), 831–843. https://doi.org/10.1080/03601270802243713
Lai, D. W. (2009). From burden to depressive symptoms: The case of Chinese-Canadian family caregivers for the elderly. Social Work in Health Care, 48(4), 432–449. https://doi.org/10.1080/00981380802591759
Lamont, R. A., Swift, H. J., & Abrams, D. (2015). A review and meta-analysis of age-based stereotype threat: Negative stereotypes, not facts, do the damage. Psychology and Aging, 30(1), 180. https://doi.org/10.1037/a0038586
Lasher, K. P., & Faulkender, P. J. (1993). Measurement of aging anxiety: Development of the Anxiety About Aging Scale. The International Journal of Aging & Human Development, 37(4), 247–259. https://doi.org/10.2190/1U69-9AU2-V6LH-9Y1L
Levy, B. R. (2003). Mind matters: Cognitive and physical effects of aging self-stereotypes. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 58(4), P203–P211. https://doi.org/10.1093/geronb/58.4.P203
Levy, B. R. (2009). Stereotype embodiment: A psychosocial approach to aging. Current Directions in Psychological Science, 18(6), 332–336. https://doi.org/10.1111/j.1467-8721.2009.01662.x
Levy, S. R. (2018). Toward Reducing Ageism: PEACE (Positive Education about Aging and Contact Experiences) Model. The Gerontologist, 58(2), 226–232. https://doi.org/10.1093/geront/gnw116
Levy, B. R., Slade, M. D., & Kasl, S. V. (2002). Longitudinal benefit of positive self-perceptions of aging on functional health. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 57, 409–417. https://doi.org/10.1093/geronb/57.5.P409
Lin, X., & Bryant, C. (2009). Students’ attitudes toward older people: A cross-cultural comparison. Journal of Intergenerational Relationships, 7, 411–424. https://doi.org/10.1080/15350770903285320
Lockenhoff, C. E., Lee, D. S., Buckner, K. M. L., Moreira, R. O., Mertinez, S. J., & Sun, M. Q. (2015). Cross-cultural differences in attitudes about aging: moving beyond the east-west dichotomy. In S.-T. Cheng, I. Chi, H. H. Fung, L. W. Li, & J. Woo (Eds.), Successful aging: Asian perspectives (pp. 321–333). Springer.
Lunenburg, F. C. (2011). Self-efficacy in the workplace: Implications for motivation and performance. International Journal of Management, Business, and Administration, 14(1), 1–6.
Macnicol, J. (2006). Age discrimination an historical and contemporary analysis. Cambridge University Press.
Maggino, F., & Mola, T. (2007). Il differenziale semantico per la misura degli atteggiamenti: Costruzione, applicazione e analisi. Firenze University Press.
Marques, S., Mariano, J., Mendonça, J., De Tavernier, W., Hess, M., Naegele, L., Peixeiro, F., & Martins, D. (2020). Determinants of ageism against older adults: A systematic review. International Journal of Environmental Research and Public Health, 17(7), 2560. https://doi.org/10.3390/ijerph17072560
Mâsse, L. C., & Anderson, C. B. (2003). Ethnic differences among correlates of physical activity in women. American Journal of Health Promotion, 17(6), 357–360. https://doi.org/10.4278/0890-1171-17.6.357
McKeown, J., Clarke, A., & Repper, J. (2006). Life story work in health and social care: Systematic literature review. Journal of Advanced Nursing, 55(2), 237–247. https://doi.org/10.1111/j.1365-2648.2006.03897.x
Nunnally, J., & Bernstein, I. (1994). Psychometric theory (3rd ed.). McGraw-Hill.
Nussbaum, J. F., Pitts, M. J., Huber, F. N., Krieger, J. L. R., & Ohs, J. E. (2005). Ageism and ageist language across the life span: Intimate relationships and Non-intimate interactions. Journal of Social Issues, 61(2), 287–305. https://doi.org/10.1111/j.1540-4560.2005.00406.x
Opoku, M. P., Agyei-Okyere, E., Nketsia, W., Torgbenu, E. L., & Kumi, E. O. (2022). Perceived self-efficacy of students and its influence on attitudes and knowledge about HIV/AIDS in Ghana. The International Journal of Health Planning and Management, 37(2), 755–769. https://doi.org/10.1002/hpm.3371
Palmore, E. B. (1990). Ageism, negative and positive. Springer.
Parent, N., & Fortin, F. (2000). A randomized, controlled trial of vicarious experience through peer support for male first-time cardiac surgery patients: Impact on anxiety, self-efficacy expectation, and self-reported activity. Heart & Lung, 29(6), 389–400. https://doi.org/10.1067/mhl.2000.110626
Pinquart, M., & Forstmeier, S. (2012). Effects of reminiscence interventions on psychosocial outcomes: A meta-analysis. Aging & Mental Health, 16(5), 541–558. https://doi.org/10.1080/13607863.2011.651434
Pinquart, M., & Sorensen, S. (2003). Associations of stressors and uplifts of caregiving with caregiver burden and depressive mood: A meta-analysis. Journals of Gerontology; Series B: Psychological Science and Social Science, 58(2), 112–128.
Prestwich, A., Kellar, I., Parker, R., MacRae, S., Learmonth, M., Sykes, B., & Castle, H. (2014). How can self-efficacy be increased? Meta-analysis of dietary interventions. Health Psychology Review, 8(3), 270–285. https://doi.org/10.1080/17437199.2013.813729
Rejeski, W. J., Miller, M. E., Foy, C., Messier, S., & Rapp, S. (2001). Self-efficacy and the progression of functional limitations and self-reported disability in older adults with knee pain. Journal of Gerontology: Social Sciences, 56B, S261–S265. https://doi.org/10.1093/geronb/56.5.S261
Resnick, B., Luisi, D., Vogel, A., & Junaleepa, P. (2004). Reliability and validity of the self-efficacy for exercise and outcome expectations for exercise scales with minority older adults. Journal of Nursing Measurement, 12(3), 235–248. https://doi.org/10.1891/jnum.12.3.235
Robertson, D. A., Savva, G. M., King-Kallimanis, B. L., & Kenny, R. A. (2015). Negative perceptions of aging and decline in walking speed: A self-fulfilling prophecy. PLoS ONE, 10(4), e0123260. https://doi.org/10.1371/journal.pone.0123260
Roodin, P., Brown, L. H., & Shedlock, D. (2013). Intergenerational service-learning: A review of recent literature and directions for the future. Gerontology & Geriatrics Education, 34, 3–25. https://doi.org/10.1080/02701960.2012.755624
Rupp, D. E., Vodanovich, S. J., & Credé, M. (2005). The multidimensional nature of ageism: Construct validity and group differences. The Journal of Social Psychology, 145(3), 335–362. https://doi.org/10.3200/SOCP.145.3.335-362
Sargent-Cox, K. A., Anstey, K. J., & Luszcz, M. A. (2014). Longitudinal change of self-perceptions of aging and mortality. Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 69(2), 168–173. https://doi.org/10.1093/geronb/gbt005
Schelling, H. R., & Martin, M. (2008). Attitudes toward one’s own aging: A question of age or a question of resources? Zeitschrift Fur Gerontologie Und Geriatrie, 41(1), 38–50. https://doi.org/10.1007/s00391-007-0451-5
Schneewind, K. A. (1995). Impact of family processes on control beliefs. In A. Bandura (Ed.), In self-efficacy in changing societies (pp. 114–148). University of Cambridge Press.
Schönstein, A., Dallmeier, D., Denkinger, M., Rothenbacher, D., Klenk, J., Bahrmann, A., & Wahl, H. W. (2021). Health and subjective views on aging: Longitudinal findings from the ActiFE Ulm Study. The Journals of Gerontology: Series B, 76(7), 1349–1359. https://doi.org/10.1093/geronb/gbab023
Sheeran, P., Maki, A., Montanaro, E., Avishai-Yitshak, A., Bryan, A., Klein, W. M., & Rothman, A. J. (2016). The impact of changing attitudes, norms, and self-efficacy on health-related intentions and behavior: A meta-analysis. Health Psychology, 35(11), 1178. https://doi.org/10.1037/hea0000387
Silverstein, M., & Parrott, T. M. (1997). Attitudes toward public support of the elderly: Does early involvement with grandparents moderate generational tensions? Research on Aging, 19(1), 108–132. https://doi.org/10.1177/0164027597191005
Sohng, K. Y., Sohng, S., & Yeom, H. A. (2002). Health-promoting behaviors of elderly Korean immigrants in the United States. Public Health Nursing, 19(4), 294–300. https://doi.org/10.1046/j.1525-1446.2002.19409.x
Soliz, J., & Harwood, J. (2006). Shared family identity, age salience, and intergroup contact: Investigation of the grandparent–grandchild relationship. Communication Monographs, 73(1), 87–107. https://doi.org/10.1080/03637750500534388
Steca, P., Greco, A., Cappelletti, E., D’addario, M., Monzani, D., Pancani, L., & Parati, G. (2015). Cardiovascular management self-efficacy: Psychometric properties of a new scale and its usefulness in a rehabilitation context. Annals of Behavioral Medicine, 49(5), 660–674. https://doi.org/10.1007/s12160-015-9698-z
Stephan, W. G., & Stephan, C. W. (2000). An integrated threat theory of prejudice. In S. Oskamp (Ed.), Reducing prejudice and discrimination. Lawrence Erlbaum Associates.
Swift, H., Abrams, D., Lamont, R. A., & Drury, L. (2017). The risks of ageism model: How ageism and negative attitudes towards age can be a barrier to active aging. Social Issues and Policy Review, 11(1), 195–231. https://doi.org/10.1111/sipr.12031
Swift, H. J., Abrams, D., & Marques, S. (2013). Threat or boost? Social comparison affects older people’s performance differently depending on task domain. Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 68(1), 23–30. https://doi.org/10.1093/geronb/gbs044
Tabachnick, B. G., & Fidell, L. S. (2007). Using multivariate statistics. Pearson Education Inc.
Valencia-Vallejo, N., López-Vargas, O., & Sanabria-Rodríguez, L. (2016). Self-efficacy in computer-based learning environments: A bibliometric analysis. Psychology, 7(14), 1839. https://doi.org/10.4236/psych.2016.714170
Vize, C. E., Sharpe, B. M., Miller, J. D., Lynam, D. R., & Soto, C. J. (2022). Do the Big Five personality traits interact to predict life outcomes? Systematically testing the prevalence, nature, and effect size of trait-by-trait moderation. European Journal of Personality, 08902070221111857.
Voci, A., & Hewstone, M. (2003). Intergroup contact and prejudice toward immigrants in Italy: The mediational role of anxiety and the moderational role of group salience. Group Processes & Intergroup Relations, 6(1), 37–54.
Voronov, M., & Singer, J. A. (2002). The myth of individualism-collectivism: A critical review. The Journal of Social Psychology, 142, 461–480. https://doi.org/10.1080/00224540209603912
Wahyuni, R., & Krisnatuti, D. (2022). Analysis stressors, coping strategies, and their effects on quality of life of the elderly during the Covid-19 pandemic. Journal of Family Sciences, 7(1), 14–28. https://doi.org/10.29244/jfs.v7i1.39108
WHO. (2002). Active aging: A policy framework. World Health Organization.
Williams, S. L., & French, D. P. (2011). What are the most effective intervention techniques for changing physical activity self-efficacy and physical activity behaviour—and are they the same? Health Education Research, 26(2), 308–322. https://doi.org/10.1093/her/cyr005
Wolff, J. L., Mulcahy, J., Huang, J., Roth, D. L., Covinsky, K., & Kasper, J. D. (2018). Family caregivers of older adults, 1999–2015: Trends in characteristics, circumstances, and role-related appraisal. The Gerontologist, 58(6), 1021–1032. https://doi.org/10.1093/geront/gnx093
Wurm, S., & Benyamini, Y. (2014). Optimism buffers the detrimental effect of negative self-perceptions of aging on physical and mental health. Psychology & Health, 29(7), 832–848. https://doi.org/10.1080/08870446.2014.891737
Wurm, S., Tesch-Romer, C., & Tomasik, M. J. (2007). Longitudinal findings on aging-related cognitions, control beliefs, and health in later life. Journals of Gerontology Series B: Psychological Sciences & Social Sciences, 62B, 156–164. https://doi.org/10.1093/geronb/62.3.P156
Wurm, S., Warner, L. M., Ziegelmann, J. P., Wolff, J. K., & Schüz, B. (2013). How do negative self-perceptions of aging become a self-fulfilling prophecy? Psychology and Aging, 28(4), 1088. https://doi.org/10.1037/a0032845
Funding
Open access funding provided by Università Cattolica del Sacro Cuore within the CRUI-CARE Agreement. This work was supported by private funding through an agreement between Amplifon S.p.A. and the Center for Studies and Research of the Catholic University of Milan (Grant number R1064400240).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The author(s) declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Informed Consent
All study participants provided informed consent prior to participation in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Manzi, C., Adorni, R., Giannella, V.A. et al. How to Age More Positively? Analyzing Determinants that Shape Attitudes Towards Aging. J Adult Dev 31, 53–64 (2024). https://doi.org/10.1007/s10804-023-09447-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10804-023-09447-6