
Abstract
Developmental crisis is a construct that is central to many theories of psychosocial adult development, yet there is currently no validated psychometric measure of adult developmental crisis that can be used across adult age groups. To address this gap in the literature, we developed and validated an age-independent measure of adult developmental crisis for research and applied purposes, entitled the Developmental Crisis Questionnaire (DCQ-12). Exploratory and confirmatory factor analyses were conducted separately on different samples. A three-factor structure emerged as the best fit with the data: (1) Disconnection and Distress; (2) Lack of Clarity and Control and (3) Transition and Turning Point. The DCQ-12 showed predictive validity with measures of self-esteem, locus of control, authentic living, optimism, presence of and search for meaning, turning points and a related crisis measure. Four-week test–retest reliability ranged from 0.78 to 0.89 across subscales. As well as research uses, the DCQ-12 measure has potential application in practice, given that assessment of developmental crisis has relevance to professionals working in clinical and non-clinical roles to support and coach adults through periods of transition.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Research on developmental crisis episodes that occur during adulthood has been predominantly qualitative in methodology since the origins of such work in the 1960s (e.g., Denne & Thompson, 1991; Erikson, 1968; Jaques, 1965; Levinson et al., 1978; O’Connor & Wolfe, 1987; Robinson & Smith, 2010; Robinson & Stell, 2015). To move quantitative research on the topic forward, a validated psychometric measure of developmental crisis is needed. The current study presents a psychometric development and validation of a new measure of adult developmental crisis, the Developmental Crisis Questionnaire (DCQ-12). The measure taps the common features of crisis that are consistent across early adult, midlife and later life crisis; hence, it can be used across adult age groups.
Conceptualizing Developmental Crisis
The theory of lifespan development devised by Erikson (1968) views change as inherently discontinuous. Stable periods of structural stability are interspersed with periods of volatile instability that can degenerate into a crisis. Crisis episodes are, therefore, developmentally functional, as they represent a period in which a psychosocial integration is broken down so that a new and more complete integration can be achieved. The now popular idiom of “breakdown to breakthrough” captures this Eriksonian dynamic of disintegration followed by more holistic integration (Barton, 2017). During episodes of crisis, then, breakdowns comprise difficulties that might appear as symptoms of mental illness (e.g., strong and challenging negative emotions, difficulties with day-to-day functioning), but within the context of a crisis, these difficulties are expected to occur temporarily until a breakthrough phase commences. Indeed, research has shown that strong negative emotions are an important motive for reevaluating one’s lifestyle or worldview that may lead a person to change goals and explore directions that they would not have otherwise (Carver & Scheier, 1998; Robinson, 2020).
Levinson (1986, 1996) adopted Erikson's holistic paradigm in developing his theory of adult development. A central concept in Levinson’s theorizing is the life structure, which is the integration of a person’s internal world, such as values, goals and beliefs, as well as their external environment, which encompasses relationship commitments, social roles and responsibilities. The development of the life structure is a central feature of four adult life stages; pre-adulthood, early adulthood, middle adulthood and late adulthood (Levinson et al., 1978). Each era begins and ends with a transition period, which consists of the reappraisal of the existing life structure. Levinson conceived of developmental crisis in a similar way to Erikson; he portrays crisis as inherent to healthy development for most people, and therefore, while crises may be distressing, they are not pathological and avoiding them at all costs may be detrimental to growth. A crisis is, in Levinson’s framework, a call to reform a life structure in ways that allow for greater levels of life satisfaction, authenticity and balance between internal inclinations and external commitments (Levinson, 1996).
Since these theories were proposed by Erikson and Levinson, qualitative work has unearthed other models of age-specific developmental crises, including the holistic model of early adult crisis (Robinson et al., 2013), the phase model of midlife transition and crisis (O’Connor & Wolfe, 1987) and the model of later life crisis (Robinson & Stell, 2015).
The holistic model of early adult crisis proposes a series of phases through which young adults pass when they go through a developmental crisis (locked-in, separation and time-out, exploration and rebuilding) and four levels of analysis that contribute to understanding any particular crisis (person/environment, identity, motivation and affect–cognition) (Robinson et al., 2013). All early adult crises involve person–environment discontinuities, such as changing career or leaving a relationship/marriage, along with strong affective components and dramatic identity shifts.
The model of midlife transition and crisis devised by O’Connor and Wolfe (1987, 1991) argues that the midlife crisis starts from a stable person–environment life structure. Then through a combination of external life transitions, internal questioning and reassessment of beliefs and priorities, the person temporarily feels lost and disconnected. Towards the end of the midlife crisis episode, the individual seeks to re-establish a life structure, via a process of tentative experiments to adapt to changing circumstances and try out new commitments. This cautious experimental phase then cedes to a more permanent set of post-crisis commitments.
The model of later life crisis developed by Robinson and Stell (2015) describes the onset of a crisis in people aged 60–69 as triggered by multiple loss-inducing stressful life events, such as loss of health, loss of a person, loss of work via retirement, along with strong depressive emotions and cognitions. This then triggers a simultaneous exploration of acceptance versus the motive to change and fight against current circumstances, along with an endeavour to either re-engage with social roles or disengage from them. However, ageing brings multiple gains as well as losses, and previous research suggests less crisis in the over 60 s compared with early adulthood and midlife (Robinson & Wright, 2013). These models of early adult crisis, midlife crisis and later life crisis differ in a variety of ways but when looking at their theoretical origins, in the face of Erikson and Levinson, they all converge on some common features of a developmental crisis, five of which are described in turn.
Common Features of a Developmental Crisis
The first common feature of a developmental crisis is being in a time of transition or a turning point in a person’s life. This typically centres on transformative or discontinuous changes in external relationships and roles. Two large-scale studies on midlife found that the most commonly reported turning point themes are work/career shifts and changes in interpersonal relationships (Clausen, 1995; Wethington et al., 2004). These themes are also the most common retrospectively appraised features of crisis across different age groups (Robinson & Wright, 2013).
The second common feature of developmental crises is feeling overwhelmed with environmental demands and struggling to cope (Slaikeu, 1990). Caplan's (1964) theory of crisis emphasized the experience of overwhelming stress from the external world due to coping mechanisms that were previously found to be effective being no longer so (see also Halpern, 1973). In seeking and finding new and more effective coping mechanisms, the individual passing through a crisis episode makes changes to their habitual patterns of behaviour and changes their person–environment relationship, which in turn leads to alterations in life structure, if they become part of a stable person–environment balance that endures over time (Levinson, 1986).
The third common feature of a developmental crisis is the increased tendency to question and seek meaning. Individuals who self-define as being in a crisis read self-help books and books on spirituality and religion more than a matched comparison group who were defined as not being in a crisis (Robinson et al., 2017). Crises also frequently involve a heightened awareness of death and dying (Jaques, 1965; Robinson & Stell, 2015). Thus, a developmental crisis is frequently also an existential crisis, in which a whole range of assumptions and beliefs about life are questioned (Butėnaitė et al., 2016).
The fourth common feature of a developmental crisis is the change to identity and self. During a crisis episode, a person is drawn to reappraise their identity in light of new information or insights that occur during development (Levinson, 1996). A process of intensive self-reflection and intrapersonal curiosity is typical during a crisis, to facilitate the emergence of a new or altered identity (Robinson et al., 2017). People may become aware that they have ignored or suppressed aspects of their self and identity (Denne & Thompson, 1991). For example, the identity shifts within early adult crisis episodes have been characterized as a conflict between authentic dispositions and false selves constructed for social approval and concealment of supposedly inappropriate inclinations (Robinson & Smith, 2010). During the crisis, a person may experiment with expressing previously concealed aspects of the self. The self-reflective nature of a crisis prompts a person to challenge their identity and this is a key element in rebuilding the internal aspect of the life structure (Becker, 1997; Linley & Joseph, 2004; Robinson & Wright, 2013).
The fifth common theme is the experience of strong negative emotions. During a crisis episode, a person will experience a range of affects that are typically more intense, including anxiety about the uncertainty of the future and feelings of being out of control (Caplan, 1964), depressive feelings that come with a sense of loss (Robinson & Stell, 2015), as well as frustration or anger that stem from a perceived inability to cope with life and an appraisal that others may be the cause of this (Levinson, 1996).
Existing Related Measures of Crisis
The Halpern Crisis Scale was developed in 1973 as a general scale to assess the presence of a crisis episode. Although it attempted to formalize the construct of crisis, the scale suffers from key limitations. One limitation is that Halpern’s approach starts from a clinical perspective and fails to consider the developmental aspects of a crisis. Furthermore, the approach relies solely on identifying a set of behaviours associated with a crisis, but omits the emotional, cognitive and person–environment features of crisis. Third, the scale was developed ad hoc rather than via recognized psychometric protocols. The scale has not been used in developmental research since it was published, although it has been used to assess crisis in studies of cancer patients (e.g., Gottesman & Lewis, 1982; Lewis et al., 1979).
Two midlife crisis questionnaires have been developed: the 52-item Midlife Crisis Scale (MLC) (Hermans & Oles, 1999) and the 15-item Chinese Midlife Crisis Scale (C-MCS) (Shek, 1996). These scales are constructed to focus specifically on midlife, for example focusing on family/marriage, ageing, generativity and bereavement. Moreover, each scale has its problems. First, the MLC was developed in a male-only population which severely limits its generalizability. The C-MCS is a 15-item scale that was established without psychometric validation.
The Crisis Definition-Question (CD-Q) is a categorical yes-maybe-no assessment tool for assessing retrospective or concurrent appraisals of crisis (Robinson & Wright, 2013). Participants are provided with a definition of a developmental crisis and asked if they have experienced such a one in the past or whether they appraise that they are in a crisis now (see Table 1). The CD-Q is limited in its ability to meaningfully capture between-participant variance as it is a 3-alternative-forced-choice measure, and the single-item nature of the assessment leaves it prone to random error. The measure is used within the validation studies presented below to determine a meaningful cut-off point for the DCQ-12 in assessing the presence of crisis categorically.
The Current Study
The current research aims to develop a psychometrically valid, brief questionnaire to measure the perceived presence and extent of a developmental crisis. The questionnaire was predicted to have five latent dimensions, following the 5 common features of crisis presented above.
In order to develop the scale, exploratory and confirmatory factor analyses were conducted on separate samples. The resultant final scale was then subjected to further analyses to test its reliability (construct and test–retest) and validity (both convergent and discriminant) by looking at common criteria as well as correlations with theoretically related constructs.
Method
Initial Item Pool
Items for the new questionnaire were developed, based on the common themes described earlier elicited via a conceptual review of the literature on developmental crisis. A search of the literature was conducted for existing scales of a developmental crisis (Halpern, 1973; Hermans & Oles, 1999; Shek, 1996; Roozbehani & Dehkordi, 2018; Yusin et al., 1972). These were used as a starting point to develop the items for the initial item pool. The authors created 42 items across 5 predicted themes, as shown in Table 2. For the full list of items, see Table 3.
Participants were given the following instructions for responding to the item pool: “Please indicate whether the following statements describe your life in general over the past 6 months or so. In relation to appraising whether you have been experiencing something more than ‘normal’, make a judgement about the past 6 months relative to your adult life generally”. Then they rated each statement on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). The rationale for using a timeframe of 6 months was that this was judged from previous research to exclude stressors and events that do not amount to a crisis while capturing phenomena that occur within the expected duration of a developmental crisis. Participants were instructed to judge whether the phenomena described by the items were present more than “normal”, to help ensure that that are experienced as discontinuous with their life more generally.
Other Measures
Stress
To measure the perceived stress of participants, the Perceived Stress Scale (PSS; Cohen, 1988) was used. Specifically, the 10-item PSS asks participants to reflect on their thoughts and feelings during the last month and how overwhelming or uncontrollable participants find their lives. Items include “In the last month, how often have you felt that you were unable to control the important things in your life?” or “In the last month, how often have you found that you could not cope with all the things that you had to do?”. The items are rated on a 5-point frequency scale ranging from 0 (Never) to 4 (Very Often) with higher scores indicating higher perceived stress. The Cronbach’s alpha for the current study was 0.91.
Depression
To measure depression, the 10-item version of the Center for Epidemiological Studies-Depression scale (CES-D; Andresen et al., 1994) was used. Items tap into the feelings of participants over the past week. Example items include “I felt that everything I did was an effort” and “I felt depressed”. The items were rated on a 4-point frequency scale from 1 (Rarely or none of the time) to 4 (All of the time) with higher scores indicating higher levels of depression. Cronbach’s alpha for the current study was 0.86.
Self-esteem
To measure self-esteem, the 10-item Rosenberg’s self-esteem scale (Rosenberg, 1965) was used. Example items include “On the whole, I am satisfied with myself” and “At times I think I am no good at all”. The items are scored on a 4-point Likert scale ranging from 1 (Strongly Agree) to 4 (Strongly Disagree) with higher scores indicating higher self-esteem. Cronbach’s alpha for the current study was 0.93.
Locus of Control
To measure locus of control, Rotter’s Locus of Control (LoC) scale (Rotter, 1966) was used. In this scale, participants are presented with 29 questions (4 filler items) each containing two statements, from which they choose the statement that they agree with most. Each question’s statements are designed to be reflective of either internal or external locus of control. Scores across the items are summed with higher scores indicating a more external locus of control. Cronbach’s alpha for the current study was 0.77.
Authenticity
To measure participants’ authenticity, the Authenticity Scale (Wood et al., 2008) was used. The 12-item scale is equally divided into 3 dimensions which are scored separately. The three dimensions are: authentic living (e.g., “I always stand by what I believe in”.), accepting external influence (e.g., “I usually do what other people tell me to do”.) and self-alienation (e.g., “I feel out of touch with the real me”.). Items are rated on a 7-point Likert scale ranging from 1 (does not describe me at all) to 7 (describes me very well) with higher scores indicating more of the respective dimension. Cronbach’s alphas for authentic living, accepting external influence and self-alienation were 0.82, 0.93 and 0.83, respectively.
Optimism
To measure optimism, the 12-item Life Orientation Test (LOT; Scheier & Carver, 1985) was used. The LOT is designed to tap into participants’ expectations about the future and their general dispositional optimism. The scale contains 12 items, 4 of which are filler ones (e.g., “I enjoy my friends a lot”.), 4 are positively keyed (e.g., “In uncertain times, I usually expect the best”.) and 4 are negatively keyed (e.g., “I hardly ever expect things to go my way”.). The items are rated on a 5-point Likert scale ranging from 4 (strongly agree) to 0 (strongly disagree) with higher scores indicating higher optimism. Cronbach’s alpha for the current study was 0.89.
Meaning in Life
To measure participants meaning in life, the 10-item Meaning in Life Questionnaire (MLQ; Steger et al., 2006) was used. The MLQ is divided in two dimensions, namely presence of meaning (e.g., “I understand my life’s meaning”.) and search for meaning (e.g., “I am always looking to find my life’s purpose”.), with 5 items tapping into each dimension. Items are rated on a 7-point Likert scale ranging from 1 (Absolutely Untrue) to 7 (Absolutely True). Both the presence and the search dimensions were of high reliability with Cronbach’s alphas of 0.92 and 0.92, respectively.
Crisis Definition Questionnaire
For another measure of whether participants are in a crisis, a crisis definition question (Robinson & Wright, 2013) was used. Participants were presented with the following definition of a crisis “A crisis episode is a period in adult life that is noticeably more difficult, stressful and unstable than normal and is an important turning point in your life due to changes that occur during it. Crisis episodes typically last for several years, but may be shorter or longer. Have you experienced any times of crisis in your adult life?” Then they had to respond with either “Yes”, “Maybe” or “No”.
Turning Points
To tap into participants’ self-reported experience of a transition or a turning point, questions from the Midlife in the United States (MIDUS) survey (Wethington et al., 2004) were used. Specifically, after participants are provided with a definition of a psychological turning point, they are then asked whether they have experienced one within the past 12 months in seven different domains: work, finding upsetting/encouraging news about a friend/oneself, fulfilling/giving up a dream. The respondents answer with either “Yes” or “No”.
Procedure
After developing the initial item pool, a survey was created and hosted on Qualtrics,Footnote 1 which is a software platform that supports creating and disseminating online questionnaires and experiments. Once participants read an information sheet and consented to take part in the research, they were first asked if they have had a mental health diagnosis within the past year. If the answer was positive, they were not allowed to continue and were debriefed instead as the reporting of a non-pathological experience of a developmental crisis is potentially confounded by the presence of a clinical mental illness. If they have not had a diagnosis, they completed the DCQ initial item pool. After that, each participant was randomly allocated to one of two groups which determined which questionnaires they completed. This was done to reduce the workload of filling in too many questionnaires per participant as per ethical guidelines. Group 1 (N = 192) completed the questionnaires, relating to stress, depression, self-esteem and locus of control, while Group 2 (N = 196) completed the questionnaires relating to authenticity, optimism and meaning in life. Then, all participants completed the Crisis Definition Questionnaire and the Turning Points questions. Finally, before being debriefed, they were asked to provide their email if they would be willing to be contacted later for a short follow-up. If the participant agreed, they were emailed four weeks later, asking them to complete the DCQ initial item pool only in order to establish test–retest reliability.
Participants
Four hundred and nineteen participants met the criteria for participation and completed the survey. Thirty one participants were removed for completing in under 5 min, on the basis that they would not have been able to provide meaningful responses in that timeframe. This meant a final sample size of 388. Of those who have completed the initial survey, 146 completed the 4-week follow-up.
The 388 participants were split into two samples for the purpose of running separate exploratory and confirmatory factor analyses. Sample 1 included participants from an existing participant pool of individuals aged 18–85 as well as those recruited from social media, while Sample 2 included participants who received user credits for the platform (SONA or SurveyCircle), which benefit them when distributing their own questionnaires. Table 2 summarizes the demographics of the two samples.
Results
All analyses were conducted using the R programming language (R Core Team, 2020). The core packages used were tidyverse (Wickham et al., 2019), psych (Revelle, 2021) and lavaan (Rosseel, 2012). Both the anonymized data and R scripts are available via the Open Science Framework.
Exploratory Factor Analysis
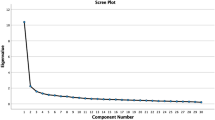
The first step of the psychometric validation process was to identify the underlying factor structure of the items (Clark & Watson, 1995). Using data from Sample 1 (n = 219), all items from the initial item pool but one (item 15 was excluded due to technical error) were subjected to an Exploratory Factor Analysis (EFA) using the correlation matrix. The data were suitable for an EFA based on Bartlett’s test (p < 0.001) and the Keyser–Meyer–Olkin measure (0.94). Principal axis factoring was used over principal component analysis (PCA) because PCA assumes that all variance is common variance, i.e. all variance is captured within the data, which was not a feasible assumption; this was reflected in the data as all initial communalities were significantly lower than 1, hence, supporting the use of principal axis factoring (Field, 2013; Tinsley & Tinsley, 1987). The eigenvalues of the first 10 factors were 17.26, 2.97, 1.82, 1.33, 1.30, 1.24, 1.07, 1.04, 0.92 and 0.82, respectively, and respectively accounted for 42.10%, 7.24%, 4.43%, 3.24%, 3.17%, 3.04%, 2.61%, 2.53%, 2.25% and 1.99% of the variance.
To decide how many factors to retain, three criteria were used: a visual inspection of the scree plot, Velicer's minimum average partial (MAP) test (Velicer, 1976; Velicer et al., 2000) and parallel analysis (O’Connor, 2000). An initial inspection of the scree plot (see Fig. 1) suggested that either 3 or 6 factors were suitable. Parallel analysis suggested 6 factors. The original formulation of the MAP test, which raises the smallest average partial correlation coefficient to the second power, suggested 6 factors, while the revised MAP test—which raises the same coefficient to the fourth power—suggested 3 factors. Given the oscillation between 6- and 3-factor solutions, both were examined.Footnote 2

Scree plot of the initial factor analysis (principal axis factoring)
First, the EFA was run with a 6-factor forced solution. An oblique rotation was used as the factors were bound to be correlated; the subsequent factor correlation matrix confirmed this (Fabrigar et al., 1999). An examination of the 6-factor solution showed that there are at least three spurious factors with many cross-loadings as well as low factor loadings (≤ 0.50). Therefore, this solution was rejected.
The EFA was then re-run with a forced 3-factor solution and an oblique rotation. Table 3 shows initial and extracted communalities as well as factor loadings for each item. A sufficient number of factors were retained given that discrepancies between initial and extracted communalities were few.
Four items were retained for each factor. This decision was driven by the aim of developing a brief scale and the rule of thumb that four items per scale is the recommended lowest threshold for item retention for good psychometric properties (Saucier & Goldberg, 2002). The subscales had very high reliability, as measured by Cronbach’s alpha. The lowest alpha value was α = 0.85. For factors 1 and 2, retaining more than four items did not improve alpha significantly (any increase < 0.02); hence, it was decided that it is not worth burdening the participant. The three retained factors were correlated. Disconnection and distress correlated with lack of clarity and control at 0.61 and with transition and turning point at 0.42; lack of clarity and control correlated with transition and turning point at 0.19.
Confirmatory Factor Analysis
To better establish the structural invariance of the DCQ, a confirmatory factor analysis (CFA) was done on a separate sample. For reporting the results of the CFA, we followed the guidelines of Brown (2015) and Jackson et al. (2009). To run the analysis, a model was built based on the 12-item 3-factor structure that emerged during the EFA—see Fig. 2.

Visual representation of the 12-item 3-factor model with standardized factor loadings
We first checked whether the data meet parametric assumptions. First, there were no missing values on any of the 12 variables for all 169 participants. Second, it was checked whether variables were normally distributed by inspecting the skewness and kurtosis for each variable. Kim (2013) has suggested that univariate non-normality arises only when absolute z values are greater than 3.29. No z value for kurtosis met the 3.29 threshold, while only 3 variables met the 3.29 threshold for skew. This suggests that univariate normality of the data can be assumed.
Given the assumed normality of the data, a CFA was run on the covariance matrix using a maximum-likelihood estimation with robust standard errors, which is the most popular and reliable method (Byrne, 2010). Overall, the indices (χ2(51) = 109.46, p < 0.001, although see Byrne (2010) and Newsom (2018) for weakness of the chi-square test in low sample sizes; GFI = 0.910, threshold > 0.95 and > 0.90 is acceptable; CFI = 0.911, threshold > 0.90; RMSEA = 0.082, 95% CI [0.061–0.104], threshold < 0.05 and < 0.08 is acceptable; SRMR = 0.085; threshold < 0.08; see Byrne (2010), Hair et al. (2019) and Newsom (2018) for threshold recommendations) suggest an adequate model (CFI is perfect) but not ideal (GFI and RMSEA could be better). One reason for the suboptimal performance of two of the indices could be attributed to two relatively weakly performing items, namely 25 and 9. Not only do these item have relatively low loadings on their factor in both the EFA and the CFA, but their error terms in the CFA are correlated at r > 0.1 with most other error terms that do not belong to the same factor.
Scale Reliability
The reliabilities of each factor and the total scale, as measured by Cronbach's alpha, Composite Reliability (CR) and test–retest reliability (measured by type A intraclass correlation coefficient with random effects for subjects and fixed effects for measures (Koo & Li, 2016)), were shown to be high. Specifically, Cronbach’s alpha for each factor ranged from 0.72 to 0.78 and 0.79 for the entire scale. The CR for each factor ranged from 0.74 to 0.78 and 0.91 for the entire scale. The four-week test–retest stabilityFootnote 3 for each factor ranged from 0.78 to 0.83 and 0.89 for the entire scale.
Convergent and Discriminant Validity
Convergent validity was first examined using the Fornell–Lacker criterion, which suggests that the average variance extracted for each component should exceed 0.50 (Fornell & Larcker, 1981). The average variance extracted (AVE) for each factor and total score was 0.47, except the Lack of Clarity and Control factor, where it was 0.46. Some have suggested that AVE is a conservative measure of the convergent validity of a scale and values of CR > 0.70 suffice to deem the measure adequate (Malhotra & Dash, 2011)—see Table 4. Hence, given that the DCQ's AVE values were close to 0.50 and the conservative nature of AVE, convergent validity was considered to be acceptable.
The discriminant validity of the DCQ was first examined by looking at the AVE of each factor—discriminant validity is achieved if the squared root of the AVE of each factor is greater than the inter-factor correlations. The square root of the AVE for each factor was 0.68–0.69. The highest inter-factor correlation was between factors 1 and 2 (Disconnection & Distress and Lack of Clarity & Control) of 0.72, suggesting some tentative discriminant validity concerns. Additionally, the heterotrait–monotrait (HTMT) criterion (Henseler et al., 2015) was also computed to assess the discriminant validity of the scale; values of < 0.85 (conservative) indicate sufficient discriminant validity between constructs (Kline, 2011). The highest value for the DCQ was 0.71, which supports the discriminant validity of the scale.
To further examine the convergent and discriminant validity of the DCQ-12, a correlational analysis was performed between the total score on the DCQ-12 and measures of stress, depression, self-esteem, locus of control, authenticity, optimism and meaning in life—see Table 5. Furthermore, pairwise comparisons of total scores on the DCQ-12 between people who said “Yes” vs “No” on the seven Psychological Turning Points questions as well as the Crisis Definition Questionnaire are presented in Table 6. Most correlations and pairwise comparisons show a meaningful pattern of relationship with the DCQ-12; however, most notably problems with discriminant validity were highlighted by the unexpectedly high correlations with the PSS and the CESD-10.
Categorical Scoring and Prevalence of Developmental Crisis in the Sample by Age and Gender
To facilitate the categorical assessment of developmental crisis for research or applied purposes, a categorical cut-off point of 42/60 was established for the total scale (or 3.5 if calculating the subscales and total scale as the mean of items). This cut-off is 1 standard deviation above the mean when rounded down to zero decimal places (mean = 33.4 and SD = 8.9). It is also a cut-off score that makes sense from a scoring point of view. It entails an average score of 14 across all three subscales. A subscale score of 14 is, on average, above the midpoint.
Using this cut-off criterion, the percentage of the total sample assessed who qualified as being in crisis was 19%. Broken down by gender and age group, using the same age categories as Robinson and Wright (2013), the proportion within age group and gender who qualified as being in crisis was as follows: Young adults (18–39); 25% of females in crisis and 16% of males in crisis. Midlife (40–49); 9% of females in crisis and 25% of males in crisis. Later life (60+); 0% of females in crisis and 5% of males in crisis. These prevalence estimates are provisional and will be the focus of further large-sample survey research.
Discussion
The aim of the current study was to develop a brief, psychometrically valid questionnaire to measure the presence and extent of developmental crises. Following an exploratory factor analysis of our item pool, 12 items were retained across three dimensions: Disconnection and Distress, Lack of Clarity and Control and Transition and Turning Point, each explaining 42.10%, 7.24% and 4.43% of the variance, respectively. A confirmatory factor analysis on a different sample using the same structure demonstrated adequate model fit (GFI = 0.910, CFI = 0.911, RMSEA = 0.082). Four-week test–retest reliability was high, ranging from 0.78 to 0.89.
The correlational relations between the DCQ subscales/total score and other variables show a clear theoretical fit with previous work on developmental crisis. All subscales and total scale are correlated with the absence of perceived meaning of life, while the subscales Transition and Turning Point and Disconnection and Distress were related to actively searching for meaning in life. This fits with qualitative research on crisis episodes that have also found them to be intensive periods of searching for meaning (Denne & Thompson, 1991). The Authentic Living subscale of the Authenticity scale is negatively related to the total score, Disconnection and Distress and Lack of Clarity and Control. This is congruent with previous research findings that periods of crisis are times in which individuals feel a disjunction between inner self and outer self that in turn manifests as feeling inauthentic (Hollis, 1993; Robinson et al., 2017). Both self-esteem and optimism were negatively correlated with all subscales, while stress and depression were positively correlated with all three subscales. In light of the high correlations with stress and with depression, a key issue going forward for research will be ensuring that developmental crisis is meaningfully distinguished from these variables. While a developmental crisis may be hard to distinguish from mental health disorders such as depression through a screening instrument such as the DCQ-12, the reverse is also likely to be true; it may be that the distress associated with developmental crisis and other developmentally normative phenomena are being incorrectly diagnosed or indicated as depression (Horwitz & Wakefield, 2012).
Relationships between DCQ-12 total score crisis and turning point events were broadly as predicted; those in crisis reported higher levels of giving up a dream, changes at work, upsetting news about self and other, and lower levels of fulfilling a dream. Curiously, though, good news about self and other was also related to being in crisis. This reflects the evidence that crisis episodes are transitional times of change and transformation in life that may come with more intense experiences of all kinds, including ones that bring insights and positive change (Bridges, 2004).
In terms of the provisional prevalence of crisis found, the prevalence is generally lower than that which has been found by way of the CD-Q single-item assessment (e.g., Robinson & Wright, 2013). The pattern of prevalence between genders and age groups does, however, show notable similarities with the Robinson and Wright study, such as females reporting crisis more than males. This reverses at midlife in the current sample: more males than females reported being in crisis, which once again fits with Robinson and Wright's (2013) finding that post-crisis growth was notably low in midlife males. Very few over-60 s qualified as being in crisis, which fits with a lower prevalence shown in other studies comparing age groups (Robinson & Wright, 2013) and also with theories of ageing that find generally higher levels of wellbeing in older adults compared with younger adults (Reed et al., 2014).
Limitations and Future Directions
This study represents an important step forward in the psychometric assessment of a developmental crisis in adults, but there are inherent limitations that call for further research to resolve. Firstly, crisis episodes proceed through discernable phases, but the current measure assesses crisis without considering the phase of a crisis that a person is in. While we are confident that the DCQ-12 provides an important general assessment of developmental crisis that can be used for research and applied purposes, future assessment approaches could take into account a more phase-specific approach to assessment. The challenge with a phase-sensitive approach is that the phases of crisis differ by age group (Robinson, 2020); thus, any phase-specific crisis assessment would need to be bespoke to an adult age group. Furthermore, as with other self-report tools, the questionnaires assess the first-person perception of being in a crisis episode, rather than the objective presence of particular life events.
The research could have also been affected by practical limitations in data collection. One such example is the use of multiple sources of data collection which can influence the quality of the repsponses. For instance, among the participants who received virtual credits, those coming from the SONA platform are psychology students who might be particularly interested in the topic and they might systematically differ compared to participants from SurveyCircle, who might be more incentivized to complete the study quicker. Hence, future studies could benefit from sticking to a single source of participants and standardizing the incentives. Also, despite rigorous post-hoc checks of the data on a case-by-case basis, further procedures could have been put in place during the data collection to verify the quality of the responses. Such procedures include adding trap items, instructional manipulation checks, collecting more metadata (browser information in addition to IPs and geolocation data), collecting paradata (timing, mouse clicks), implementing URL control (creating individual links, utilizing cookies) and using response pattern detection algorithms (Leiner, 2013; Oppenheimer et al., 2009; Teitcher et al., 2015).
A further important issue is that the nature of data collection means that the sample of older adults is both relatively small and is unlikely to be representative. The frequencies of crisis across age groups are, therefore, highly provisional and presented as a stimulus for post-validation large-sample cross-sectional research with samples that are rigorously stratified by demographic criteria such as education, income, social class and acculturation, homogenized across key age ranges. One priority area for future research on developmental crisis involves studies across age groups, cultures and ethnicities in order to establish whether the factorial structure, predictive validity and crisis prevalence are consistent across demographic groups or if there is meaningful cross-cultural variation. With a large enough sample, crisis prevalence can be explored down by narrower age groups than those used in this study to ensure more meaningfully defined stages, such as the following: emerging adulthood (18–29), established adulthood (30–39), early midlife (40–49), late midlife (50–59), older adults, aged 60–79 and older adults, aged 80+.
A final suggestion for future researchers in this area, in light of the strong correlations between stress and the measure of developmental crisis, is to look at the relationship between the DCQ-12, stressful life events and chronic stressors.
In summary, prior research on developmental crisis in adulthood has proceeded based mainly on qualitative methods, and those studies that have used quantitative methods have been constrained by serious limitations. The current study attempts to address these limitations by developing a brief, psychometrically valid questionnaire that measures the presence and extent of a developmental crisis. This brief measure can also be used in clinical and coaching settings, in conjunction with other tools, to provide a holistic psychological profile of the client and help give an informed view on whether a person is going through a developmental crisis or is experiencing distress or difficulty that relates to non-developmental dynamics. While the psychometric properties of the DCQ-12 show satisfactory model fit and convergent/divergent validity, there is room for improvement in both. Further studies conducted with the DCQ-12 will provide further information about the factorial structure, reliability and validity of the measure across multiple samples as well as its structural invariance across age groups. Based on that information, we are open to the prospect of developing a revised scale in the future via an expanded item set or a revised scoring system.
Data Availability
The raw and processed datasets, data processing pipeline and data analysis scripts are available on the Open Science Framework https://osf.io/t8hbw/.
Change history
09 September 2022
A Correction to this paper has been published: https://doi.org/10.1007/s10804-022-09428-1
Notes
During the peer-review process, we were also asked to examine a 2-factor solution. We explored but rejected this solution as no loadings for the second factor were > 0.70. The results of this model can be viewed in the codebook on the Open Science Framework.
Four-week test-retest sample size = 146 as everyone who responded to the follow-up was included, regardless of which group or sample they were allocated for the other analyses. This was done to maximize the sample size for this analysis.
References
Andresen, E. M., Malmgren, J. A., Carter, W. B., & Patrick, D. L. (1994). Screening for depression in well older adults: Evaluation of a short form of the CES-D. American Journal of Preventive Medicine, 10(2), 77–84.
Barton, J. (2017, March 24). Midlife crisis? Congratulations: This is not a breakdown. This is a breakthrough. Retrieved from https://lifelabs.psychologies.co.uk/posts/15744-midlife-crisis-congratulationd
Becker, G. (1997). Disrupted lives: How people create meaning in a chaotic world. University of California Press.
Bridges, W. (2004). Transitions: Making sense of life’s changes (2nd ed.). Da Capo Press.
Brown, T. A. (2015). Confirmatory factor analysis for applied research (Second edition). The Guilford Press.
Butėnaitė, J., Sondaitė, J., & Mockus, A. (2016). Components of existential crisis: A theoretical analysis. International Journal of Psychology: A Biopsychosocial Approach, 18, 9–27.
Byrne, B. M. (2010). Structural equation modeling with AMOS: Basic concepts, applications, and programming (2nd ed.). Routledge.
Caplan, G. (1964). Principles of preventive psychiatry. Basic Books Inc.
Carver, C. S., & Scheier, M. (1998). On the self-regulation of behavior. Cambridge University Press.
Clark, L. A., & Watson, D. (1995). Constructing validity: Basic issues in objective scale development. Psychological Assessment, 7(3), 309.
Clausen, J. A. (1995). Gender, contexts, and turning points in adults’ lives. In P. Moen, G. Elder, & K. Luscher (Eds.), Examining lives in context: Perspectives on the ecology of human development (pp. 365–389). American Psychological Association.
Cohen, S. (1988). Perceived stress in a probability sample of the United States. The social psychology of health (pp. 31–67). Sage Publications Inc.
Denne, J. M., & Thompson, N. L. (1991). The experience of transition to meaning and purpose in life. Journal of Phenomenological Psychology, 22(2), 109.
Erikson, E. H. (1968). Identity: Youth and crisis. Norton.
Fabrigar, L. R., Wegener, D. T., MacCallum, R. C., & Strahan, E. J. (1999). Evaluating the use of exploratory factor analysis in psychological research. Psychological Methods, 4(3), 272.
Field, A. (2013). Discovering statistics using IBM SPSS statistics. Sage.
Fornell, C., & Larcker, D. F. (1981). Evaluating structural equation models with unobservable variables and measurement error. Journal of Marketing Research, 18(1), 39. https://doi.org/10.2307/3151312
Gottesman, D., & Lewis, M. S. (1982). Differences in crisis reactions among cancer and surgery patients. Journal of Consulting and Clinical Psychology, 50(3), 381–388. https://doi.org/10.1037/0022-006X.50.3.381
Hair, J. F., Black, W. C., Babin, B. J., & Anderson, R. E. (2019). Multivariate data analysis (8th ed.). Cengage.
Halpern, H. A. (1973). Crisis theory: A definitional study. Community Mental Health Journal, 9(4), 342–349.
Henseler, J., Ringle, C. M., & Sarstedt, M. (2015). A new criterion for assessing discriminant validity in variance-based structural equation modeling. Journal of the Academy of Marketing Science, 43(1), 115–135. https://doi.org/10.1007/s11747-014-0403-8
Hermans, H. J., & Oles, P. K. (1999). Midlife crisis in men: Affective organization of personal meanings. Human Relations, 52(11), 1403–1426.
Hollis, J. (1993). The middle passage: From misery to meaning in midlife. Inner City Books.
Horwitz, A. V., & Wakefield, J. C. (2012). All we have to fear: Psychiatry’s transformation of natural anxieties into mental disorders. Oxford University Press.
Jackson, D. L., Gillaspy, J. A., Jr., & Purc-Stephenson, R. (2009). Reporting practices in confirmatory factor analysis: An overview and some recommendations. Psychological Methods, 14(1), 6.
Jaques, E. (1965). Death and the mid-life crisis. International Journal of Psycho-Analysis, 46, 502–514.
Kim, H.-Y. (2013). Statistical notes for clinical researchers: Assessing normal distribution (2) using skewness and kurtosis. Restorative Dentistry & Endodontics, 38(1), 52–54.
Kline, R. B. (2011). Convergence of structural equation modeling and multilevel modeling. Sage.
Koo, T. K., & Li, M. Y. (2016). A guideline of selecting and reporting intraclass correlation coefficients for reliability research. Journal of Chiropractic Medicine, 15(2), 155–163. https://doi.org/10.1016/j.jcm.2016.02.012
Leiner, D. J. (2013). Too fast, too straight, too weird: Post hoc identification of meaningless data in internet surveys. SSRN Electronic Journal. https://doi.org/10.2139/ssrn.2361661
Levinson, D. J. (1986). A conception of adult development. American Psychologist, 41(1), 3.
Levinson, D. J. (1996). The seasons of a woman’s life. Ballantine Books.
Levinson, D. J., Darrow, C. N., Klein, E. B., Levinson, M. H., & McKee, B. (1978). The seasons of a man’s life. Random House Digital Inc.
Lewis, M. S., Gottesman, D., & Gutstein, S. (1979). The course and duration of crisis. Journal of Consulting and Clinical Psychology, 47(1), 128–134. https://doi.org/10.1037/0022-006X.47.1.128
Linley, P. A., & Joseph, S. (2004). Positive change following trauma and adversity: A review. Journal of Traumatic Stress: Official Publication of the International Society for Traumatic Stress Studies, 17(1), 11–21.
Malhotra, N., & Dash, S. (2011). Marketing research an applied orientation. Pearson Publishing.
Newsom, J. T. (2018). Some clarifications and recommendations on fit indices. Retrieved from http://web.pdx.edu/~newsomj/semclass/ho_fit.pdf
O’Connor, B. P. (2000). SPSS and SAS programs for determining the number of components using parallel analysis and Velicer’s MAP test. Behavior Research Methods, Instruments, & Computers, 32(3), 396–402.
O’Connor, D. J., & Wolfe, D. M. (1987). On managing midlife transitions in career and family. Human Relations, 40(12), 799–816.
O’Connor, D. J., & Wolfe, D. M. (1991). From crisis to growth at midlife: Changes in personal paradigm. Journal of Organizational Behavior, 12(4), 323–340. https://doi.org/10.1002/job.4030120407
Oppenheimer, D. M., Meyvis, T., & Davidenko, N. (2009). Instructional manipulation checks: Detecting satisficing to increase statistical power. Journal of Experimental Social Psychology, 45(4), 867–872.
R Core Team. (2020). R: A language and environment for statistical computing. R Foundation for Statistical Computing. Retrieved from https://www.R-project.org/
Reed, A. E., Chan, L., & Mikels, J. A. (2014). Meta-analysis of the age-related positivity effect: Age differences in preferences for positive over negative information. Psychology and Aging, 29(1), 1–15. https://doi.org/10.1037/a0035194
Revelle, W. (2021). psych: Procedures for psychological, psychometric, and personality research [Manual]. Retrieved from https://CRAN.R-project.org/package=psych
Robinson, O. C. (2020). Development through adulthood. Red Globe Press.
Robinson, O. C., Demetre, J. D., & Litman, J. A. (2017). Adult life stage and crisis as predictors of curiosity and authenticity: Testing inferences from Erikson’s lifespan theory. International Journal of Behavioral Development, 41(3), 426–431.
Robinson, O. C., & Smith, J. A. (2010). Investigating the form and dynamics of crisis episodes in early adulthood: The application of a composite qualitative method. Qualitative Research in Psychology, 7(2), 170–191.
Robinson, O. C., & Stell, A. J. (2015). Later-life crisis: Towards a holistic model. Journal of Adult Development, 22(1), 38–49.
Robinson, O. C., & Wright, G. R. (2013). The prevalence, types and perceived outcomes of crisis episodes in early adulthood and midlife: A structured retrospective-autobiographical study. International Journal of Behavioral Development, 37(5), 407–416.
Robinson, O. C., Wright, G. R., & Smith, J. A. (2013). The holistic phase model of early adult crisis. Journal of Adult Development, 20(1), 27–37.
Roozbehani, A., & Dehkordi, M. A. (2018). Construction and validation of Iranian midlife challenges scale. Journal of Psychology & Clinical Psychiatry, 9(6), 640–646. https://doi.org/10.15406/jpcpy.2018.09.00602
Rosenberg, M. (1965). Society and the adolescent self-image (Vol. 61). Princeton University Press.
Rosseel, Y. (2012). lavaan: An R package for structural equation modeling. Journal of Statistical Software, 48(2), 1–36.
Rotter, J. B. (1966). Generalized expectancies for internal versus external control of reinforcement. Psychological Monographs: General and Applied, 80(1), 1.
Saucier, G., & Goldberg, L. R. (2002). Assessing the big five: Applications of 10 psychometric criteria to the development of marker scales. In B. De Raad & M. Perugini (Eds.), Big five assessment (pp. 29–58). Hogrefe and Huber.
Scheier, M. F., & Carver, C. S. (1985). Optimism, coping, and health: Assessment and implications of generalized outcome expectancies. Health Psychology, 4(3), 219.
Shek, D. T. (1996). Midlife crisis in Chinese men and women. The Journal of Psychology, 130(1), 109–119.
Slaikeu, K. A. (1990). Crisis intervention: A handbook for practice and research (2nd ed.). Allyn and Bacon.
Steger, M. F., Frazier, P., Oishi, S., & Kaler, M. (2006). The meaning in life questionnaire: Assessing the presence of and search for meaning in life. Journal of Counseling Psychology, 53(1), 80.
Teitcher, J. E., Bockting, W. O., Bauermeister, J. A., Hoefer, C. J., Miner, M. H., & Klitzman, R. L. (2015). Detecting, preventing, and responding to “fraudsters” in internet research: Ethics and tradeoffs. The Journal of Law, Medicine & Ethics, 43(1), 116–133.
Tinsley, H. E., & Tinsley, D. J. (1987). Uses of factor analysis in counseling psychology research. Journal of Counseling Psychology, 34(4), 414.
Velicer, W. F. (1976). Determining the number of components from the matrix of partial correlations. Psychometrika, 41(3), 321–327.
Velicer, W. F., Eaton, C. A., & Fava, J. L. (2000). Construct explication through factor or component analysis: A review and evaluation of alternative procedures for determining the number of factors or components. Problems and solutions in human assessment (pp. 41–71). Springer.
Wethington, E., Kessler, R. C., & Pixley, J. E. (2004). Turning points in adulthood. In O. G. Brim, C. D. Ryff, & R. C. Kessler (Eds.), How healthy are we? A national study of well-being at midlife (pp. 586–613). University of Chicago Press.
Wickham, H., Averick, M., Bryan, J., Chang, W., McGowan, L., François, R., Grolemund, G., Hayes, A., Henry, L., Hester, J., Kuhn, M., Pedersen, T., Miller, E., Bache, S., Müller, K., Ooms, J., Robinson, D., Seidel, D., Spinu, V., & Yutani, H. (2019). Welcome to the tidyverse. Journal of Open Source Software, 4(43), 1686. https://doi.org/10.21105/joss.01686
Wood, A. M., Linley, P. A., Maltby, J., Baliousis, M., & Joseph, S. (2008). The authentic personality: A theoretical and empirical conceptualization and the development of the Authenticity Scale. Journal of Counseling Psychology, 55(3), 385.
Yusin, A., Sinay, R., & Nihira, K. (1972). Adolescents in crisis: Evaluation of a questionnaire. American Journal of Psychiatry, 129(5), 574–577.
Funding
No external funding received.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Te authors declare no competing or conflicting interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix: Develop Crisis Questionnaire (DCQ-12)
Appendix: Develop Crisis Questionnaire (DCQ-12)
Please indicate whether the following statements describe your life in general over the past 6 months or so. In relation to appraising whether you have been experiencing something more than “normal”, make a judgement of the past six months relative to your adult life generally.
-
1.
I feel like the “inner me” has been out of sync with the “outer me”.
-
2.
I feel like my life has lost direction.
-
3.
I have been experiencing stronger negative emotions than normal.
-
4.
I have been thinking that life is meaningless.
-
5.
I have been confident about what I need to do to make it in life. (R)
-
6.
I have been feeling in control of my life. (R)
-
7.
My life feels stable and predictable. (R)
-
8.
I have felt that I have had the resources to deal with any challenges that life throws at me.(R)
-
9.
I am experiencing a time of transition in my life.
-
10.
I am passing through a major turning point in my life.
-
11.
I feel like I may be in the process of leaving the “old me” behind and am developing a “new me”.
-
12.
I have noticed that the way I have thought about my life has changed.
Instructions for Participants
Please indicate whether the following statements describe your life in general over the past 6 months or so. In relation to appraising whether you have been experiencing something more than “normal”, make a judgement of the past 6 months relative to your adult life generally”.
Scoring Instructions
All items are presented on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Take the sum of items 1, 2, 3 and 4 for Disconnection and Distress; the sum of items 5, 6, 7 and 8 for Lack of Clarity and Control; and the sum of items 9, 10, 11 and 12 for Turning Point and Transition. (R) denotes reverse-worded items.
Categorical scoring: Where a 2-level categorical variable is required, a score of 42 or more is coded as crisis present, while a score of 41 or less is coded as crisis absent.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Petrov, N., Robinson, O.C. & Arnett, J.J. The Developmental Crisis Questionnaire (DCQ-12): Psychometric Development and Validation. J Adult Dev 29, 265–278 (2022). https://doi.org/10.1007/s10804-022-09403-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10804-022-09403-w