
Abstract
Parents of children with disabilities are an important part of their child’s special education team. However, parents often have limited involvement in school-based therapies that are provided as part of a child’s Individualized Education Program. The field lacks tools to assess the domain and extent of parent needs for optimal engagement in their child’s special education therapies. Study one assessed the Parent-Therapist Partnership Survey’s (PTPS) (formerly known as the Needs of Parents Questionnaire -School-Based Therapy Version) measure’s clarity, fit, and comprehensiveness. Study two assessed the factor structure and internal consistency. Two factors emerged – Need to Be an Informed, Engaged Member of Their Child’s Team, and Need for Support and Guidance. Internal consistency was 0.93 for the overall scale. The PTPS can serve as a powerful measure to better identify opportunities to engage parents in school therapeutic goals while improving parent-provider collaboration in school-based therapies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Rehabilitative and habilitative therapies, such as speech-language therapy, social work services, and occupational therapy, can help children with disabilities develop adaptive strategies and increase daily functioning (Houtrow et al., 2019; Novak & Honan, 2019). Many children ages 3–21 receive therapies in their school as part of their school-based Individualized Education Program (IEP; a federally mandated special education service plan covered under the Individuals with Disabilities Education Act [IDEA] of 2004). School-based therapies delivered through special education services are called “related services” (also referred to as “school-based therapies”). Outpatient and early intervention service delivery settings have largely shifted to family-centered care models that emphasize family involvement in therapy planning and implementation (Dempsey & Keen, 2008). However, little work has been done regarding how parents and families can be better engaged specifically in school-based therapies. Since special education services are publicly funded through IDEA (2004), special education related services are often the most equitable and accessible therapy service delivery system for many families – particularly those who do not have insurance or access to an array of local providers, as well as for those who face barriers (time, transportation, caps on the number of sessions covered by insurance) to accessing outpatient services.
Parent participation in special education services, including related services, is a central tenant of special education law (IDEA, 2004). Furthermore, parent participation in therapeutic services has been shown to have numerous positive outcomes, such as promoting skill maintenance and generalization, increasing parent-provider collaboration, improving health, behavioral and academic outcomes for children with disabilities, reducing parent stress, and increasing parent sense of efficacy (Dixon, 1996; Gunning et al., 2019; Hand et al., 2012; Hudson et al., 2003; McIntyre, 2008; Newmann & Wehlage, 1995; Pears et al., 2015; Roberts et al., 2006; Sofronoff & Farbotko, 2002; Stuttard et al., 2014, 2016). Furthermore, involving parents in therapy services increases the amount of time children can practice therapeutic skills during the week – instead of only having a limited amount of time per week with a school clinician, children can continue practicing skills throughout their week during their daily routines, exponentially increasing the dosage of the intervention children receive and the amount of time they get to practice therapeutic skills in different settings. To effectively involve parents in therapeutic implementation and decision-making, providers must first better understand what parents need to engage with these therapies. Previous studies have shown that parents, in particular parents from ethnically and linguistically diverse backgrounds, often face barriers to fully participating in special education services (Blue-Banning et al., 2004; Harry, 2008; Jung, 2011). Given both the legal mandate and the clear benefit to parent participation in a child’s school-based therapies, it is critical that we understand how to engage parents in school-based therapies.
Numerous studies have assessed the needs of parents of children with disabilities. However, many of these studies do not use formal, empirically validated measures (Pickard & Ingersoll, 2015; Spann et al., 2003) or use measures that are outside the scope of therapeutic care in the school setting. For example, a commonly used measure is the Family Needs Survey (Bailey & Simeonsson, 1988), which covers needs related to information, support, community services, financial needs, and family functioning for parents of children receiving early intervention services. While this survey has been used to assess the needs of parents with older children in Sweden (Granlund & Roll-Pettersson, 2001), the items and domains covered are too broad to assess the specific needs parents have when interacting with school-based providers. Furthermore, the Family Needs Survey only assesses the importance of needs and not the degree to which needs are met, a crucial component of meeting the needs of parents of children with disabilities (Brown et al., 2012).
The Family Needs Questionnaire was originally designed to assess the needs of parents with children with traumatic brain injury (Waaland et al., 1993) and was later adapted for children with developmental disabilities (Siklos & Kerns, 2006). This measure assesses the general needs faced by parents of children with developmental disabilities and the degree to which these needs are met. This measure has some items that relate specifically to interactions with therapy providers, such as “I need to be actively involved in my child’s treatments and therapies” and “I need to have information regarding [my] child’s therapeutic or educational progress.” However, it also contains numerous items that are outside of the scope of needs related specifically to interactions with school-based clinicians, such as “I need to take week-long vacations by myself each year” (Siklos & Kerns, 2006, p. 925). Thus, the Family Needs Questionnaire is too broad to effectively assess what parents need to effectively engage in school-based therapeutic care.
The scale that most closely assesses the needs of parents when engaging with clinicians is the Needs of Parents Questionnaire (NPQ; Kristjánsdóttir, 1995). This measure assesses parent perceptions of the relative importance of 43 parent-focused needs, and extent to which each need is met, to engage in their child’s hospital-based care. The NPQ covers 6 domains - the need: (1) to be able to trust doctors and nurses, (2) for information, (3) related to other family members, (4) to feel that [parents] are trusted, (5) related to human and physical resources, and (6) for support and guidance (Kristjánsdóttir, 1995, p. 100). For each item, parents answer 3 questions: (1) “How important do you feel the following statements are for you in relation to your child’s hospitalization;” (2) “The need, concern, or service presented in the statements: how well and to what extent do you feel it is being met;” and (3) “Would you need help from the hospital to fulfill these particular needs?” The original measure demonstrated high internal consistency across the three parts of the instrument (α > 0.91) and face validity was acceptable. No previous factor analyses were reported for the original measure.
Murphy & Risser (2022) adapted the items in the NPQ to create the (previously named) Needs of Parents Questionnaire – School-Based Therapy Version (NPQ-SBT) to assess the needs of parents specifically related to engaging in school-based therapies. They found that an average of 83% of needs were reported as important but an average of 51% of needs were unmet. Furthermore, disparities emerged regarding the needs reported as unmet between Parents of Color and White parents as well as between families with one child with a disability and two children with a disability. However, more research is needed to support these findings, as the sample sizes reported in Murphy & Risser’s (2022) paper are small (n = 41). Furthermore, to thoroughly investigate the needs that parents have in engaging with school-based services and to further explore the disparities reported by Murphy & Risser (2022) , the psychometric properties of their adapted measure must first be determined. Since the questions of the original NPQ have been changed, and items have been both added and deleted, the content validity and the factor structure of the adapted measure must also be examined to accurately identify the constructs the adapted inventory measures. In addition, since the measure is now significantly different in purpose and content from the original NPQ, the authors have subsequently titled the measure the Parent-Therapist Partnership Survey (PTPS), and it will be referred to as such throughout the current manuscript.
While item-level data will be useful in allowing clinicians to better support individual families, identifying the factors that emerge within the PTPS will allow providers to monitor groups of parent needs at more macroscopic levels (e.g., classroom level, grade level, school level, district level). Identifying findings for these higher levels requires creating composite categories of needs, as monitoring large numbers of parent needs at these higher levels will likely not be feasible for school personnel, given the demands on time and resources that the school setting presents. Thus, ensuring the PTPS has strong factors could support clinicians and schools in higher-level monitoring as well as developing higher-level interventions to support parent engagement more broadly.
This text describes two studies in the PTPS Development. In the first study, the authors adapted and sought parent feedback on the content of Murphy & Risser’s (2022) adapted measure NPQ-SBT to enhance its content validity. After undertaking a comparison of the original NPQ and the NPQ-SBT to ensure no relevant questions were excluded by Murphy & Risser (2022), relevant items were added back into the measure and were adapted to relate to needs associated with school-based therapies. The updated measure was then sent to a group of parents of children with disabilities who reviewed items clarity and relevance. This feedback was used to further revise the measure. In the second study, the finalized measure was sent out to parents of children receiving special education related services. These responses were used to conduct an exploratory factor analysis to identify the factors that emerged to form the finalized PTPS. Internal consistency was calculated for each sub-scales as well as for the overall measure.
This project had three goals. First, this study engaged community stakeholders to ensure the PTPS instructions and item-wording was clear and provided a comprehensive inventory of parent needs. Second, after stakeholder feedback was incorporated, factor analyses identified the factor structure of the measure. Third, analyses assessed the internal consistency of the full PTPS and of each factor. Ultimately, the goal of this work was to create a tool to identify opportunities to improve parents engagement and parent-therapist partnerships in school-based therapies for children with disabilities.
Study One: Questionnaire Refinement and Adaptation
Methods
Original NPQ-SBT
The NPQ-SBT (Murphy & Risser, 2022) is a 22-item measure adapted from the Needs of Parents Questionnaire (Kristjánsdóttir, 1995). The NPQ-SBT covered four of the six original NPQ sub scales: (1) Parents’ need to feel that they are trusted (5 Items); (2) Parents’ need for information (6 Items); (3) Parents’ need for support and guidance (6 Items); and (4) Parents’ need for their own human and physical resources (5 items). For each item, parents were asked to rate “How important is this need to you?” on a five-point Likert scale (0 = Does Not Concern Me, 1 = Not Important, 2 = Somewhat Important, 3 = Important, 4 = Very Important). For any item marked as some level of importance (Somewhat Important, Important, or Very Important), parents were asked to rate, “How well do you feel that the need is being met by your child’s service providers” on a five-point Likert scale (1 = Not at All, 2 = Seldom, 3 = To some extent, 4 = Most often, 5 = Fully). The authors recommend that future administrations of this adapted measure always ask about the level of needs being met, as opposed to only asking after a respondent indicates some level of importance for an item, in order to provide more comprehensive data. The third portion of the original NPQ, which asked parents to identify if they would need help from providers to fulfill each need, was not included in the study.
In the NPQ-SBT scoring system, needs ratings are dichotomized into “Important” (needs endorsed as “Important” or “Very Important”) or “Not Important” (needs endorsed as “Does Not Concern Me,” “Not Important,” or “Somewhat Important.”). The proportions of needs deemed as important can be calculated for each sub scale and for the entire measure. Needs were dichotomized as unmet if they were endorsed as “Not at all,” “Seldom,” or “To Some Extent” met. Proportions of unmet needs are calculated for each sub scale and for the overall measures.
The initial reading level of the NPQ-SBT is at the 9th grade reading level, according to the Flesch-Kincaid Grade Level Test (Onwuegbuzie et al., 2013).
Procedure
After obtaining IRB approval, 11 parents of children with disabilities were asked to assess the clarity and relevance of the items in the NPQ-SBT and additional items added in from the original NPQ deemed relevant to parent engagement in school-based therapies. Responding parents were asked to rate how easy each item was to understand using a three-point Likert scale (“This statement is not clear to me” [Unclear], “This statement is a little clear to me but could be more clear” [Somewhat Clear], or “This statement is very clear to me” [Clear]).
Parents were also asked to answer the question, “Do you feel like the statements above [in the NPQ-SBT] adequately cover the concerns and experiences parents navigating related services might have?” on a 3-point Likert scale (Not at All, Somewhat, Yes). Parents then explained why they chose their rating in an open-response question. Next, parents were asked two open-ended questions to identify areas missed in the survey. These questions were (1) “What other needs do you, or other parents you know, have when working with related service providers that we did not talk about in our survey?” and (2) “What other needs are important for you, or other parents you know, when working with related service providers that we did not talk about in our survey?” Finally, parents provided basic demographics about themselves and their child with a disability.
Following the collection of parents’ responses, items marked as “Unclear” or “Sort of Clear” by any of the participants were reviewed by the research team and clarified. The relevance feedback provided by the participating parents was used to re-evaluate the questions in the NPQ-SBT as well as to add additional questions pertaining to issues parents find important that were not covered in the survey.
Results
Participants
Thirty-nine parents were contacted, 18 (46%) parents accessed the online REDCap survey, and 11 (28%) parents provided feedback on the survey. In addition, 9 (23%) parents provided basic demographic information. The average age of these 9 parents was 44.0 (SD = 9.1, range: 34–59). Their children with disabilities ranged in grade level, with three children in pre-kindergarten, one child in kindergarten, two children in middle school (grades 6–8), and three children in high school. Three parents reported having a bachelor’s degree as their highest level of education, and six reported having a master’s degree. The median number of related services each child received as part of their Individual Education Program was 4 (M = 3.4, SD = 1.3, Range: 1–5). Three children received physical therapy services, 8 children received occupational therapy, 7 received speech/language therapy, 7 received social work services, 3 received psychological services, and 3 received other related services not listed.
Parent Review
Thirty-eight items were presented to parents for review. Twenty-eight (74%) of these items had at least one rating of “Somewhat Clear” or “Unclear” and were thus reviewed by the research team for clarity. Parent readability ratings for each item in the NPQ-SBT, and additional items added in from the original NPQ, are provided in Table 1.
Nine parents responded to the question, “Do you feel like the statements above adequately cover the concerns and experiences parents navigating related services might have?” Three (33%) indicated “Somewhat” and six (67%) indicated “Yes.” Of the three parents who indicated “Somewhat,” one parent commented on the need for greater specificity regarding the survey items that addressed need for information (e.g., to how often, what type of feedback, detail of the feedback). In addition, another parent commented on the need to emphasize the survey items in the context of the general question being asked (e.g., “How important is this need to you?”), since the items on their own were confusing. The third parent commented on the need to discuss medication, but since most school providers do not prescribe medication, the research team felt this theme was outside the scope of this measure.
In response to the question, “What other needs do you, or other parents you know, have when working with related service providers that we did not address in our survey?” parents reported the following needs: (1) more information on how disabilities impact children in the classroom and the accommodations that can help them work around the challenges; (2) sibling assistance; (3) increased collaboration between service providers to improve the information and supports families receive; (4) support with helping the child understand, express their opinions about, and benefit from their related services; (5) help navigating the “big picture” of what services are available and why services are being received; and (6) communicating in a way parents understand.
In response to the question, “What other needs are important for you, or other parents you know, when working with related service providers that we did not talk about in our survey?” the following topics were suggested: (1) childcare during meetings where parent participation is required; (2) increased urgency when determining services; (3) less judgement from providers that parents are not “doing enough;” (4) respect for and acknowledgement of cultural differences; (5) taking the child into account when working with providers; and (6) information on the written goals service providers create for the child’s IEP.
After the NPQ-SBT was adapted based on parent feedback, the final measure had a 5.3 grade reading level as calculated by the Flesch-Kincaid Grade Level Test. Readability scores at the 5th grade reading level are considered an appropriate reading level for measures for adults (Calderón et al., 2006). As mentioned in the introduction, this newly adapted measure was renamed to the Parent-Therapist Partnership Survey (PTPS) due to the drastically different content and nature of this measure from the original NPQ.
Study Two: Assessing the Psychometric Properties and Factor Structure of the PTPS
Methods
Procedure
The revised PTPS was sent to parents of children receiving related services via the REDCap survey platform. Parents were recruited through Facebook groups for parents of children with disabilities, local community organizations, and Researchmatch.org. The PTPS took roughly 5 min to complete, but the entire survey took ~ 25 min, as it was part of a larger study.
Data Analysis
The importance items on the PTPS were assessed using an exploratory factor analysis (EFA) to identify relevant factors within the overall measure. Parents of children who reported receiving at least one related service as part of special education services as well as those with complete PTPS responses were included in the analyses. The research team chose to only assess the importance ratings, as the needs met-related items were designed to serve as a needs assessment to identify items to target for improved parent engagement. With this design, each factor measures the extent to which the importance of the need identified in the included items covary together such that if one of the needs is felt to be important, the others that make up the factors are also felt to be important. In addition, the research team determined future administrations of this measure would benefit from always asking about needs fulfillment (as opposed to only asking about needs fulfillment if the needs were indicated as at least somewhat important), for ease of administration and comprehensive data collection, but the team only collected partial needs responses due to the original recommendations of Murphy & Risser (2022). Thus, conducting a factor analysis of the incomplete needs data available would not provide accurate findings that could be beneficial for future administrations.
Bartlett’s Test of Sphericity and the Kaiser-Meyer-Olkin Test were conducted to ensure that the data was suitable for an EFA. A scree plot of the eigenvalues of each item was run to identify the number of factors in the model. Principal axis factoring using an obliminal rotation was used to conduct the EFA. Items with factor loadings below 0.35 were cut from each factor.
Once a final model had been developed via the EFA, Cronbach’s Alpha was calculated to determine the internal consistency of the entire measure and of the subscales.
Results
Participants
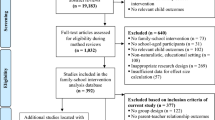
In total, 655 parents opened the survey, 406 (62%) of parents consented to participate in the survey, and 258 (39%) of parents completed the survey. The research team eliminated any responses that indicated that the respondent did not have a child receiving related services as part of their IEP or that the respondent did not complete the PTPS. As a result, 208 (32%) of responses were utilized in the following analyses.
All respondents analyzed consented to participating in the study, and all respondents indicated being the legal parent or guardian of the child[ren] with disabilities about whom they were reporting. One hundred twenty-nine participants (62%) reported being the primary caregiver for their child[ren] with disabilities, 77 (37%) reported parenting equally with their partner, and 2 (1%) reported not being the primary caregiver. One hundred eighty-five participants (89%) identified as female. When asked about their work status prior to the start of the COVID-19 pandemic, 105 (50%) of respondents reported being employed full-time, 49 (24%) of respondents reported being employed part-time, and 54 (26%) of respondents reported being unemployed.
The participants had 269 children with disabilities total, and 243 children were receiving therapeutic services as part of their special education services. Children were on average 10 years old (SD = 4.6). 88% of the children were their parent’s biological child, 10% were adopted, and 2% were under the care of a guardian. One hundred eighty-four (76%) children attended a public neighborhood school, 14 (6%) attended a therapeutic day school, and 6 (2%) were over the age of 18 but still receiving special education services, as individuals with disabilities can receive services through their 21st year. The remainder of these children attended other school settings, such as Head Start programs or private schools.
Parents reported that children had an average of 3 disabilities (SD = 2, range = 1–10), although one parent did not disclose their child’s diagnosis. Children received an average of 2 therapies (SD = 1.1, range = 1–6) in the school setting. 57% of children received outpatient services in addition to school services.
Exploratory Factor Analysis
The results of the Bartlett’s Test of Sphericity indicated that the matrix was significantly different from an identity matrix (χ2(820) = 4088.58, p < 0.001). Additionally, the Kaiser-Meyer-Olkin Test indicated that the overall MSA was equal to 0.9, and no item had an MSA value below 0.5, so no items needed to be removed before analyses. Scree plot analyses indicated a three-factor model was best suited for the data.
After running the EFA, items in the third factor did not form a theoretically sound construct. To account for this issue, and to support the construct validity of the model, items that cross-loaded on the second factor were added to this factor and the remaining items in the third factor were dropped. Table 3 outlines the outcomes of each item in the third factor. Also, the items “That I know what the next steps are when my child ages out of school-based therapies” and “That my child’s school-based clinicians provide me with information on how my child’s disabilities will impact them in the classroom” were dropped as they did not load sufficiently onto any factor. High scores on the remaining two factor indicate that needs of this “kind” are felt to be more important by parents and the items within each factor covary.
Together, these analyses yielded a 36-item measure with two factors: Need for Support and Guidance (17 items) and Need to be Informed, Engaged Members of the Child’s Team (19 items). Table 4 provides the final items included in each factor. The mean value for b factor was calculated for each participant. The correlation between factor means was 0.69.
Internal Consistency. Internal consistency was calculated for the entire scale and the two factors using Cronbach’s Alpha. Full scale internal consistency with 36 items was adequate, alpha = 0.93. Internal consistency for Need to Be Informed, Engaged Members of the Child’s Team, and Need for Support were also adequate, 0.89 and 0.90, respectively.
Measure Availability. The revised PTPS is freely available at https://sites.northwestern.edu/familycareparentinglab/ptps/ or through contacting the corresponding author. It is also freely available online as a REDcap survey that will score responses and provide a list of needs indicated as both important and unmet for parents and providers, also available through the previously mentioned link.
Discussion
This study assessed the psychometric properties and factor structure of the PTPS. After completing an iterative revision process, the final version of the PTPS consists of 36 items that fall into two factors – Need to be Informed, Engaged Members of the Child’s Team, and Need for Support and Guidance. The internal consistency for both the entire measure and the two factors was adequate, suggesting that the measures and factors both represent sound constructs. In fact, the internal consistency of the overall measure was stronger than the original NPQ (α = 0.93 vs. α = 0.91 in Kristjánsdóttir, 1995). Furthermore, the PTPS appears to have good content validity, as parents who participated in the readability study indicated that the items represented their experiences navigating school-based therapies. Thus, this study suggests the PTPS has sound psychometric properties, supporting the use of the PTPS by school-based providers to better understand parent needs and opportunities to improve parent engagement with their child’s providers and services.
The need for support and guidance has frequently been mentioned in the literature as a commonly reported need for parents of children with disabilities (Bailey & Simeonsson, 1988; Ellis et al., 2002; Kreutzer et al., 1994; Provenzi et al., 2021). However, these needs appear to be infrequently met (Ellis et al., 2002; Galpin et al., 2018; Garshelis & McConnell, 1993; Kreutzer et al., 1994; Murphy & Risser, 2022; Srinivasan et al., 2021; Resch et al., 2010; Whiting, 2014). Adequate support for both parents’ own needs, as well as the needs of their child, is an important element in parenting children with disabilities, as addressing parents’ own needs is critical for optimizing family functioning and parent-child interactions (Silkos & Kerns, 2006). Despite this, providers, and parents themselves, tend to focus on the needs of the child, often at the expense of meeting parent needs (Garshelis & McConnell, 1993; Waaland et al., 1993). To ensure optimal therapeutic efficacy and improve outcomes, Albanese et al., (1996) state that professionals must begin with assessing the “needs and wishes of the family” (p. 100) to provide appropriate social supports. The PTPS allows providers to assess parent needs and identify opportunities to improve parent engagement, which could have significant benefits for child outcomes.
The need to be an informed member of a child’s team is also a common theme in the literature that also aligns with the goals of special education, as outlined by IDEA (2004). Parents frequently report needs for information, particularly about obtaining and engaging in services, in order to best support their children with disabilities (Bailey & Simeonsson, 1988; Brown et al., 2012; Garshelis & McConnell, 1993; Granlund & Roll-Pettersson, 2001; Ellis et al., 2002; Kreutzer et al., 1994; McLennan et al., 2008; Pickard & Ingersoll, 2016; Resch et al., 2010; Waaland et al., 1993). Parents also report having limited involvement and input in the development, implementation, and evaluation of IEP-related goals and services (Spann et al., 2003), despite equal parent participation being a core tenant of special education law (IDEA, 2004). Additionally, parents have expressed a desire to learn and implement interventions themselves, particularly following the increased parent involvement that resulted from the COVID-19 pandemic (Pickard & Ingersoll, 2016; Murphy et al., 2021). The involvement of parents in interventions for specific needs has shown to both directly target core deficits in children with specific disabilities (e.g., ASD) while also reducing parental stress (Ingersoll & Wainer, 2013; Tonge et al., 2006). Thus, addressing parents needs can promote parents’ active participation as part of the IEP team, supporting efforts to optimize child outcomes.
As shown by this study, the PTPS provides an easy-to-use, parent-validated tool for school personnel, researchers, and policymakers to identify parents needs and to optimize parent engagement. The PTPS allows clinicians to identify individual areas that could be used to promote engagement with specific families. In addition, the newly created factor structure allows clinicians, schools, and researchers to monitor overarching factors for macro-level tracking and intervention. This level of analysis could support schools in identifying disparities in engagement across different categories of families and students, as well as support researchers in identifying disparities throughout different regions across the country. Finally, understanding such patterns can help to inform policy. Thus, the PTPS could be a useful tool for multiple levels of tracking, monitoring, and intervention.
Limitations
There are several limitations to these findings. First, while internal consistency was adequate, it is unknown whether this measure would be sensitive to detect changes resulting from efforts to improve parent engagement. Test-retest reliability could provide further information about the stability of the constructs and response to interventions. Second, convergent and discriminant validity in comparison to other needs assessments is recommended. Third, the sample that participated in the readability analysis was recruited from a prior study with the NPQ-SBT. Thus, it is possible that the clarity and comprehensiveness of the PTPS would not be viewed in the same manner by parents in the general population that are completely new to the measure. More work is needed to ensure that the measure adequately covers and describes the needs of parents of children with disabilities in the general population.
Conclusion
This study provides support for the Parent-Therapist Partnership Survey (PTPS) to fill a gap in the field. The PTPS has adequate internal consistency and validity as a measure of parent needs in the context of their children’s school-based therapy services. Exploratory factor analyses reveal a two-factor structure - (1) the Need to be Informed, Engaged Members of the Child’s Team, and the Need for Support and Guidance. The PTPS provides a useful resource for parents, service providers, and policy makers to optimize parent-provider collaboration in school-based therapies. Given that parent involvement in rehabilitative and habilitative therapies for children with disabilities has shown to have great benefits and that parent participation is a key component of special education practices, this measure could be a useful tool in measuring the needs parents have to optimally engage with school-based providers.
References
Albanese, A. L., San Miguel, S. K., Koegel, R. L. Social support for families. In Koegel, R. L., and Koegel, L. K. (eds.), Teaching Children With Autism: Strategies for Initiating Positive Interactions and Improving Learning Opportunities, & Brookes, P. H. (1996). Baltimore, MD, pp. 95–104
Bailey, D. B., & Simeonsson, R. J. (1988). Assessing needs of families with handicapped infants. The Journal of Special Education, 22(1), 117–127
Blue-Banning, M., Summers, J. A., Frankland, H. C., Nelson, L. L., & Beegle, G. (2004). Dimensions of family and professional partnerships: Constructive guidelines for collaboration. Exceptional Children, 70(2), 167–184
Brown, H. K., Ouellette-Kuntz, H., Hunter, D., Kelley, E., & Cobigo, V. (2012). Unmet needs of families of school-aged children with an autism spectrum disorder.Journal of Applied Research in Intellectual Disabilities,497–508
Calderón, J. L., Morales, L. S., Liu, H., & Hays, R. D. (2006). Variation in the readability of items within surveys. American Journal of Medical Quality, 21(1), 49–56
Dempsey, I. J., & Keen, D. (2008). A review of processes and outcomes in family-centered services for children with a disability.Topics in Early Childhood Special Education,42–52
Dixon, D. M. (1996). Unifying concepts in parents’ experiences with health care providers.Journal of Family Nursing
Ellis, J. T., Luiselli, J. K., Amirault, D., Byrne, S., O’Malley-Cannon, B., Taras, M., & Sisson, R. W. (2002). Families of children with developmental disabilities: Assessment and comparison of self-reported needs in relation to situational variables. Journal of Developmental and Physical Disabilities, 14(2), 191–202
Galpin, J., Barratt, P., Ashcroft, E., Greathead, S., Kenny, L., & Pellicano, E. (2018). ‘The dots just don’t join up’: Understanding the support needs of families of children on the autism spectrum. Autism: The International Journal of Research and Practice, 22(5), 571–584
Garshelis, J. A., & McConnell, S. R. (1993). Comparison of family needs assessed by mothers, individual professionals, and interdisciplinary teams. Journal of Early Intervention, 17(1), 36–49
Granlund, M. & Roll-Pettersson, L. (2001). The perceived needs of support of parents and classroom teachers - A comparison of needs in two Microsystems. European Journal of Special Needs Education, 16(3), 225–244
Gunning, C., Holloway, J., Fee, B., Breathnach, Ó., Bergin, C. M., Greene, I., & Bheoláin, R. N. (2019). A systematic review of generalization and maintenance outcomes of social skills intervention for preschool children with autism spectrum disorder. Review Journal of Autism and Developmental Disorders, 6, 1–28
Hand, A., Raghallaigh, C. N., Cuppage, J., Coyle, S., & Sharry, J. (2012). A controlled clinical evaluation of the Parents Plus Children’s Programme for parents of children aged 6–12 with mild intellectual disability in a school setting. Clinical Child Psychology and Psychiatry, 18(4), 536–555
Harry, B. (2008). Collaboration with culturally and linguistically diverse families: Ideal versus reality. Exceptional Children, 74(3), 372–388
Houtrow, A., Murphy, N., Council on Children with Disabilities, Kuo, D. Z., Apkon, S., Brei, T. J., Davidson, L. F., Davis, B. E., Ellerbeck, K. A., Hyman, S. L., O’Connor Leppert, M., Noritz, G. H., Stille, C. J., & Yin, L. (2019). Prescribing physical, occupational, and speech therapy services for children with disabilities.Pediatrics, 143(4)
Hudson, A. M., Matthews, J. M., Gavidia-Payne, S. T., Cameron, C. A., Mildon, R. L., Radler, G. A., & Nankervis, K. L. (2003). Evaluation of an intervention system for parents of children with intellectual disability and challenging behaviour. Journal of Intellectual Disability Research, 47(4–5), 238–249. https://doi.org/10.1046/j.1365-2788.2003.00486.x
Individuals with Disabilities Education Act (IDEA), 20 U.S.C. § 1400 (2004).
Ingersoll, B., & Wainer, A. (2013). Initial efficacy of project ImPACT: A parent-mediated social communication intervention for young children with ASD. Journal of Autism and Developmental Disorders, 43(12), 2943–2952
Jung, A. W. (2011). Individual Education Programs (IEPs) and barriers for parents from culturally and linguistically diverse backgrounds. Multicultural Education, 19(3), 21–25
Kreutzer, J. S., Serio, C. D., & Bergquist, S. (1994). Family needs after brain injury: A quantitative analysis. Journal of Head Trauma Rehabilitation, 9(3), 104–115
Kristjánsdóttir, G. (1995). Perceived importance of needs expressed by parents of hospitalized two- to six-year-olds. Scandinavian Journal of Caring Sciences, 9, 95–103
McIntyre, L. L. (2008). Parent training for young children with developmental disabilities: Randomized controlled trial. American Journal on Mental Retardation, 113(5), 356–368
McLennan, J. D., Huculak, S., & Sheehan, D. (2008). Brief report: Pilot investigation of service receipt by young children with autistic spectrum disorders. Journal of Autism and Developmental Disorders, 38(6), 1192–1196
Murphy, A. N., & Risser, H. J. (2022). Perceived parent needs in engaging with therapeutic supports for children with disabilities in school settings: An exploratory study. Research in developmental disabilities, 123, 104183. https://doi.org/10.1016/j.ridd.2022.104183
Murphy, A., Pinkerton, L. M., Bruckner, E., & Risser, H. J. (2021). The Impact of the Novel Coronavirus Disease 2019 on Therapy Service Delivery for Children with Disabilities. The Journal of pediatrics, 231, 168–177.e1. https://doi.org/10.1016/j.jpeds.2020.12.060
Newmann, F. M., & Wehlage, G. G. (1995). Successful school structuring: A report to the public and educators. American Federation of Teachers
Novak, I., & Honan, I. (2019). Effectiveness of paediatric occupational therapy for children with disabilities: A systematic review. Australian occupational therapy journal, 66(3), 258–273
Onwuegbuzie, A. J., Mallette, M. H., Hwang, E., & Slate, J. R. (2013). Editorial: Evidence-based guidelines for avoiding poor readability in manuscripts submitted to journals for review for publication. Research in the Schools, 20(1), i–xi
Pears, K. C., Kim, H. K., Healey, C. V., Yoerger, K., & Fisher, P. A. (2015). Improving child self-regulation and parenting in families of pre-kindergarten children with developmental disabilities and behavioral difficulties. Prevention Science, 16, 222–232
Pickard, K. E., & Ingersoll, B. R. (2015). Quality versus quantity: The role of socioeconomic status on parent-reported service knowledge, service use, unmet service needs, and barriers to service use. Autism, 106–115
Pickard, K. E., & Ingersoll, B. R. (2016). Quality versus quantity: The role of socioeconomic status on parent-reported service knowledge, service use, unmet service needs, and barriers to service use. Autism : the international journal of research and practice, 20(1), 106–115. https://doi.org/10.1177/1362361315569745
Provenzi, L., Grumi, S., Rinaldi, E., & Giusti, L. (2021). The porridge-like framework: A multidimensional guidance to support parents of children with developmental disabilities. Research in Developmental Disabilities, 117, 104048
Resch, J. A., Mireles, G., Benz, M. R., Grenwelge, C., Peterson, R., & Zhang, D. (2010). Giving parents a voice: A qualitative study of the challenges experienced by parents of children with disabilities. Rehabilitation Psychology, 55(2), 139–150
Roberts, C., Mazzucchelli, T., Studman, L., & Sanders, M. R. (2006). Behavioral family intervention for children with developmental disabilities and behavioral problems. Journal of Clinical Child & Adolescent Psychology, 35(2), 180–193
Siklos, S., & Kerns, K. A. (2006). Assessing need for social support in parents of children with autism and down syndrome. Journal of Autism and Developmental Disorders, 36(7), 921–923
Sofronoff, K., & Farbotko, M. (2002). The effectiveness of parent management training to increase self-efficacy in parents of children with Asperger syndrome. Autism, 6(3), 271–286
Spann, S. J., Kohler, F. W., & Soenksen, D. (2003). Examining parents’ involvement in and perceptions of special education services: An interview with families in a parent support group. Focus on Autism and Other Developmental Disabilities, 18(4), 228–237
Srinivasan, S., Ekbladh, A., Freedman, B., & Bhat, A. (2021). Needs assessment in unmet healthcare and family support services: A survey of caregivers of children and youth with autism spectrum disorder in Delaware. Autism Research: Official Journal of the International Society for Autism Research, 14(8), 1736–1758
Stuttard, L., Beresford, B., Clarke, S., Beecham, J., & Morris, A. (2016). An evaluation of the Cygnet Parenting Support Programme for parents of children with autism spectrum conditions. Research in Autism Spectrum Disorders, 23, 166–178
Stuttard, L., Beresford, B., Clarke, S., Beecham, J., Todd, S., & Bromley, J. (2014). Riding the Rapids: Living with autism or disability—an evaluation of a parenting support intervention for parents of disabled children. Research in Developmental Disabilities, 35(10), 2371–2383
Tonge, B., Brereton, A., Kiomall, M., Mackinnon, A., King, N., & Rinehart, N. (2006). Effects on parental mental health of an education and skills training program for parents of young children with autism: a randomized controlled trial. Journal of the American Academy of Child and Adolescent Psychiatry, 45(5), 561–569
Waaland, P. K., Burns, C., & Cockrell, J. (1993). Evaluation of needs of high- and low-income families following paediatric traumatic brain injury. Brain injury, 7(2), 135–146
Whiting, M. (2014). Support requirements of parents caring for a child with disability and complex health needs. Nursing Children and Young People, 26(4), 24–27
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Murphy, A.N., Pinkerton, L.M., Morford, A.E. et al. Parent-Therapist Partnership Survey: Parent Feedback and Psychometric Properties. J Autism Dev Disord 54, 532–543 (2024). https://doi.org/10.1007/s10803-022-05782-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-022-05782-x