
Abstract
This study examined the agreement of perceived health-related quality of life (HRQOL) between caregivers and autistic children and adolescents (n = 133, 5–12 years) using the Pediatric Quality of Life Inventory Generic Core Scales, Fourth Edition (PedsQL 4.0). Results reveal good to excellent agreement over this age range across the total, physical, and psychosocial health scales. However, the emotional, social, and school functioning scores demonstrated lower agreement in dyads with children aged 5–7 than in dyads with children aged 8–12 years. Despite these differences in agreement, overall, the PedsQL 4.0 caregiver-module is a reliable instrument for measuring HRQOL in autistic individuals aged 5–12 years.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The health-related quality of life (HRQOL) has been shown as a crucial element in estimating disease burden and health planning (Kindig et al., 2010). Conceptually, it is a multidimensional construct that aims to assess an individual's overall well-being, including physical, mental, emotional, and social functioning and its relationship with the environment (WHOQOL, 1996).
Manifestations of neurodevelopmental disorders and the associated functional limitations can adversely impact HRQOL across all life of individuals (Cavanna et al., 2013; Khanna et al., 2014; Klassen et al., 2004). In this line, the impact of autism on children's functional domains has been extensively studied during the last decade (Kuhlthau et al., 2018; Potvin et al., 2015; Sikora et al., 2012; Tilford et al., 2012).
Among the growing number of instruments designed to measure the HRQOL in childhood, the generic core scales of the Pediatric Quality of Life Inventory™ (PedsQL) and the KIDSCREEN have been extensively used on autistic pediatric populations (Ravens-Sieberer et al., 2005; Varni et al., 1999). The KIDSCREEN-52 allows a detailed profile of objective and subjective elements of well-being in individuals aged from 8 to 18 years; however, its more prolonged administration time may limit its use in some clinical contexts (Egilson et al., 2017). The PedsQL is a brief, simple to apply, and appropriate tool for measuring the well-being of autistic children and adolescents, providing a parental perspective on children's performance, and focused on quantifying objective aspects of global functioning (Varni et al., 2001; Ikeda et al., 2014).
In the context of therapeutic decision-making, healthcare professionals often assume that parents' discernment about their children's functioning adequately reflects self-perception, especially for preschool and school-age individuals or those with severe communication challenges (Eiser et al., 2001; Lopez-Espejo et al., 2021a, 2021b; Upton et al., 2008). However, this axiom is not necessarily fulfilled in neurodevelopmental conditions, making it necessary to assess the reliability of adult reports as a proxy for child well-being (Rajmil et al., 2013; Walker & Zeman, 1993). For example, in a cross-sectional study exploring agreement on PedsQL scores between autistic adolescents and their parents, researchers found a higher consensus when parents indicated how they believe their adolescent child would answer compared to their own perspective on their child's well-being (Sheldrick et al., 2012). Another study conducted in Iceland showed that parents of autistic children estimated their child's HRQOL as lower on most dimensions than patients report; however, they agreed on the need for social support and physical well-being (Egilson et al., 2017).
Several factors may play a role in the discrepancies between self-report and caregiver estimation. First, children's age and developmental status seem to affect the parents' ability to estimate their children's self-perceived HRQOL, which may be lower in adolescents (Sheldrick et al., 2012). Behavioral differences between autistic boys and girls described in the literature may influence caregivers' estimation of their child's well-being (Lai & Szatmari, 2020). Furthermore, comorbid conditions and intellectual disability may differentially affect the caregiver's and child's reported HRQOL (Knüppel et al., 2018). Therefore, all the above variables need to be studied to determine the elements that potentially affect caregivers' estimation of children's HRQOL.
The current study examines the agreement between caregiver- and self-report on the PedsQL in a sample of autistic children and adolescents living in Chile and analyzes variables affecting caregiver's reports.
Methodology
Study Design, Participants, and Ethics Statement
The present is a quantitative, observational, and cross-sectional study of primary data conducted via convenience sampling of 133 dyads of autistic individuals aged 5–12 years and their main caregivers to evaluate their agreement on perceived HRQOL of children and adolescents. Participants were recruited from the Unit of Neurodevelopment, UC-CHRISTUS Clinical Hospital, an autism spectrum conditions specialized center in Santiago, Chile.
All eligible caregiver-child dyads who attended the unit between January 2018 and May 2021 were invited to participate. Diagnosis of autism spectrum condition was formulated by a pediatric neurologist or a child and adolescent psychiatrist following Diagnostic and Statistical Manual of Mental Disorders (DSM-5) criteria (American Psychiatric Association, 2013), and all included autistic individuals scored above the clinical cutoff for autism spectrum disorder on the Autism Diagnostic Observation Schedule, Second Edition (Lord et al., 2012). Children and adolescents diagnosed with cerebral palsy, neuromuscular disorders, or progressive neurodegenerative diseases were excluded to avoid additional factors influencing the HRQOL.
The institutional ethics committee approved the study protocol (CEC-MedUC: ID 170,924,001). Children and adolescents over seven years of age agreed to participate. Regardless of age, each caregiver provided informed consent at the onset of the study.
Measures
A multidisciplinary care team composed of a psychologist, pediatric neurologists, and speech and occupational therapists obtained relevant data through interviews with parents and physical examination of children and adolescents during the first six weeks of study. Collected data were recorded in a database in compliance with institutional protocols.
Demographic data employed included the age, sex, and residence of the child or adolescent and the age and educational attainment of the caregiver. According to national statistics, a rural area was defined as a human settlement with a population less than or equal to 2000 inhabitants (INE, 2017).
Clinical information utilized included intellectual quotient (IQ), neurological disorders, medical condition of studied children and adolescents, and current use of antipsychotic or psychostimulant (methylphenidate) drugs. Ninety-four percent of participants had an IQ measurement from various Wechsler Intelligence Scale for Children versions, according to the individual's age. Epilepsy was defined following the current recommendations of the International League Against Epilepsy (Fisher et al., 2014), and attention deficit hyperactivity disorder (ADHD) was diagnosed using the diagnostic criteria proposed by the DSM-5 (American Psychiatric Association, 2013). Medical conditions were defined as disorders lasting one year or more and requiring ongoing medical attention, including asthma (14), chronic constipation (9), cow milk protein allergy (5), celiac disease (2), congenital heart disease (2), and juvenile rheumatoid arthritis (1).
HRQOL was quantified by the parental and self-report of the PedsQL, Fourth Edition, age groups 5–7 years and 8–12 years, Chile/Spanish versions (Varni et al., 2001). The questionnaire assesses, from the point of view of the interviewed, physical and psychosocial (emotional, social, and school functioning) health using a three- or five-point scale to score the answers from 0 ("never a problem") to 4 ("almost always a problem"). Scores are then converted to a 0-to-100 continuous scale (0 = 100, 1 = 75, 2 = 50, 3 = 25, and 4 = 0), with lower scores indicating greater impairment.
In children aged 5–7, the interviewer introduced the questionnaire, explained the evaluation context, and tried practice questions until there was no doubt that the child understood what was being asked. Each question was answered using a visual scale based on three facial expressions, including "it is not at all a problem" (0 points), "it is sometimes a problem" (2 points), and "it is a problem for you a lot" (4 points).
In children aged 8–12 years, the interviewer introduced and explained the questionnaire and the examination context and asked the child if he/she understood the instruction. Then, the meaning and completion of the questionnaire were explained until it became clear that the child understood the instruction.
To explore the "pandemic effect" on dyads agreement, we included in the analysis the variable "dyads evaluated during the pandemic" for questionnaires performed between April 2020 and May 2021.
The overall Cronbach's alpha of the questionaries was 0.93 for caregivers and 0.84 for children and adolescents, showing good to excellent internal consistency for the total PedsQL score.
Data Analyses
Categorical variables were presented as frequencies and percentages. Numerical variables with normal distribution were informed as means and standard deviations (SD), while those with non-normal distribution were informed as median and interquartile ranges (IQR). Normal distribution was tested with the Shapiro–Wilk test.
Two samples Wilcoxon rank-sum (Mann–Whitney) test was used to compare PedsQL scores between caregivers and children by questionnaires reporting age groups (group 1: 5–7 years vs. group 2: 8–12 years) and sex.
Given the non-normal distribution of scores in the PedsQL subscales, the magnitude of the differences between groups was measured using Cliff’s delta (Cliff, 1993). Effect sizes (delta value) < 0.147, 0.147–0.330, 0.330–0.474, and > 0.474 were considered as negligible, small, medium, and large respectively (Benjamini & Hochberg, 1995).
Average measures of intraclass correlation coefficients (ICC) quantified the inter-rater reliability (two-way random effects, absolute agreement, multiple raters) between caregiver and child reports on the PedsQL total and subscales. ICC < 0.4, 0.4–0.6, 0.6–0.75, > 0.75 were considered as poor, fair, good, and excellent agreement, respectively (Cicchetti & Sparrow, 1981).
The statistical significance for each test was considered for p-values less than 0.05. All data were analyzed using the packages "effsize" and "psych" (Revelle, 2021; Torchiano, 2020) on the R Statistical Software (v4.1.2; R Core Team, 2021).
Results
Participants
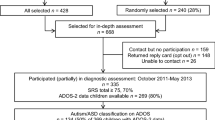
Five children failed to complete the questionnaire due to comprehension difficulties (three in group 2 and two in group 1). A total of 131 autistic individuals and their main caregivers completed the PedsQL questionnaires. The median age of children and adolescents was 89 months (IQR, 76, 106) and about three-quarters were boys (73.28%). The median age of interviewed adults was 33 years (IQR, 29, 38) and most of them were mothers (81.7%). Sixteen dyads (12.2%) were evaluated during the pandemic period. The mean IQ in 124 children and adolescents was 83.31 (SD 12.19). Of them, 16 (12.2%) with an IQ total score lower than 70, suggesting a significant limitation in intellectual functioning. Table 1 shows additional demographic and clinical characteristics of the participants.
All participants with epilepsy used one antiseizure medication: levetiracetam (7), oxcarbazepine (5), or valproic acid (2), and have been seizure-free for at least three months before the start of the study. Therefore, no children or adolescents meet the criteria for drug-resistant epilepsy according to the ILAE definition (Kwan et al., 2010).
PedsQL Scores
The total PedsQL self-report median score was 73.7 (IQR 60.9, 81.9), while 69.5 (IQR 58.9, 79.6) for caregivers. Children and adolescents reported higher median scores compared to caregivers on all scales of PedsQL (Fig. 1). These differences were significant for the physical (median score 87.5; IQR 75.0, 93.7 vs. median score 93.7; IQR 78.1, 100; p < 0.001) but not the psychosocial health scale (median score 65.0; IQR 50.0, 78.3 vs. median score 66.6; IQR 51.6, 79.1; p 0.147).

Generic Core Module PedsQL scores in 131 dyads of caregivers (white) and autistic children (gray). Box-lower boundary: 25th percentile. Box-upper boundary: 75th percentile. Horizontal box-line: 50th percentile. Whiskers above and below the box indicate the Tukey fences for outliers. Cliff’s delta for measuring the effect size. ICC (intraclass correlation coefficient) for measuring the agreement between caregiver and child. P-value based on the two samples Wilcoxon rank-sum (Mann–Whitney) test
The subgroup analysis (Table 2) showed that physical health scores differences in child-parent dyads were statistically significant in group 1 (delta = 0.27; 95% CI 0.09, 0.43), girls (delta = 0.30; 95% CI 0.02, 0.54), and boys (delta = 0.22; 95% CI 0.06, 0.37) but not in group 2 (delta = 0.19; 95% CI -0.04, 0.41). Also, in group 2, caregivers scored emotional functioning significantly lower than their children and adolescents (delta = 0.24; 95% CI 0.01, 0.45). No other differences were found even after stratifying for age and sex.
Caregiver- and self-reports in group 2 had lower median scores on all PedsQL scales and subscales than group 1. Differences in effect size between median combined scores in both age groups were medium to large for total (delta = 0.38; 95% CI 0.24, 0.51) and psychosocial (delta = 0.40; 95% CI 0.26, 0.53) scales, and not significant for the physical health domain (delta = 0.09; 95% CI -0.06, 0.24). In contrast, no differences in effect size were found when comparing median combined scores between boys and girls.
Agreement Between Caregiver and Self-report of PedsQL Scores
The agreement between parents and their children ranged from good to excellent for the entire sample in all PedsQL scales and subscales (Table 3).
In group 1, the agreement between child-caregiver dyads was good to excellent for total PedsQL score (ICC = 0.74; 95% CI 0.60, 0.83), fair to excellent for physical (ICC = 0.76; 95% CI 0.59, 0.86) and psychosocial (ICC = 0.71; 95% CI 0.55, 0.81) health scales, and fair to excellent for psychosocial subscales (Table 3).
In group 2 and girls, the agreement between caregivers and children ranged from good to excellent in all PedsQL scales and subscales, while in boys, school functioning presented the higher disagreement (ICC = 0.69; 95% CI 0.57, 0.78).
Variables Affecting the Caregiver Reported Score
Multiple linear regression models examining moderating effects of every studied covariate on caregiver reports were conducted for each PedsQL subscale as a response variable. Two significant interaction terms were found for emotional functioning and age group (ß = 0.354, 95% CI 0.08, 0.63), and for school functioning and the use of antipsychotic or psychostimulant drugs (ß = 0.308, 95% CI 0.02, 0.60).
Post-estimation predictions suggest that caregivers tend to underestimate the children’s emotional functioning self-perception in both age groups. These discrepancies are more pronounced in group 2 than group 1, especially in children who self-reported low scores (Fig. 2A). In addition, parents of children who do not receive antipsychotics or methylphenidate underestimate the poor school functioning reported by their children, whereas they tend to overestimate the negative impact on children with good self-perceived school functioning (Fig. 2B).

Post-hoc analysis. A Influence of age on reporting HRQOL. The gray line represents the scores reported by child-caregiver dyads of individuals aged 5 to 7 years. The black line represents the scores reported by dyads of children and adolescents aged 8 to 12 years. B Influence of the use of antipsychotic or psychostimulant drugs on reporting HRQOL. The gray line represents the scores of children who do not receive medication. The black line represents the scores of those who receive medication
Discussion
The present study examines the agreement in HRQOL perceptions of autistic children and adolescents and their caregivers. Although children consistently reported higher median scores on all functioning domains of the PedsQL than their caregivers, the effect size of these differences was statistically significant only for physical health in younger children and emotional functioning in older ones. Furthermore, the lowest intraclass correlation coefficients were found in psychosocial domains, revealing age-related differences in the absolute agreement between caregiver and child reports.
Comparing reports of caregivers and children from group 1 shows significant differences in physical health scores with an effect size ranging from small to medium. However, neither parent nor child median scores are over the commonly used cutoff for impaired HRQOL, indicating that this scoring discrepancy does not appear to have an evident clinical impact (Varni et al., 2003). Even though current research has highlighted the existence of developmental differences in motor skills and a wide range of muscle tone and movements abnormalities among autistic children (Lloyd et al., 2013, Whyatt & Craig, 2012), the perception of physical health in the studied dyads was good to excellent, which may reflect the greater relative importance given to psychosocial health difficulties rather than an absence of motor deficits. In fact, in a previous study of toddlers from the same population base, we found that 34.41% had generalized hypotonia and 40.86% had a delay in independent walking (Lopez-Espejo et al., 2021a, 2021b).
Emotional difficulties are a habitual characteristic in autistic individuals, directly impacting their HRQOL and behavior, as a relatively recent study based on an adult sample from the Adult Autism Spectrum Cohort-UK established (Mason et al., 2018). The discrepancies that we found in scores for emotional functioning, particularly the overreport of parents compared to children, indicate particular concern for child's self-regulation and indirectly may reflect caregiver stress. This hypothesis is further in line with recent research showing that parents of autistic children document a higher proportion of emotional and behavioral difficulties than teachers (Palmer et al., 2022). Parents may overreport problems in this area since most of these difficulties occur in daily unstructured situations when children are mainly with their families (Yorke et al., 2018). Moreover, as age increases, behavioral disturbances in children with poor emotional regulation become increasingly challenging and less tolerated by parents, which may explain the differences in scores being significant only for older children and adolescents.
Autism is a lifelong condition with psychosocial repercussions that may affect subjects' schooling and relationships. Since school integration is one of the principal sources of concern for parents and one of the most demanding aspects for autistic individuals in childhood, even with adequate therapeutic support, pharmacological intervention during the school years is not uncommon. The most used drugs are antipsychotics, but in children with ADHD as comorbidity, methylphenidate is often indicated (Howes et al., 2018). Our findings show that caregivers of children who do not receive methylphenidate or antipsychotic medication tend to overreport school difficulties and underestimate their children's self-perceived poor school functioning. Thus, this group's high parent–child school functioning domain discordance suggests an effect-modifying role of children's behavior, mediated by medication, on the caregiver's perception of their child's school functioning. Supporting this hypothesis, results from a recent cross-sectional investigation of secondary data from a large sample of a multi-center study on autistic children and adolescents showed that increased irritability is associated with poorer emotional and physical functioning, hyperactivity is associated with worse school functioning, and social withdrawal is associated with poor social functioning (Menezes & Mazurek, 2021). However, this finding should be interpreted cautiously because of the design limitation to establish causality. Thus, future longitudinal studies analyzing the effect of psychotropic drug use on the self-perceived and caregiver estimated HRQOL of autistic persons are needed.
Although no significant differences were detected between the responses of caregivers and children by sex, the highest disagreement occurred in the school functioning of boys. This result is surprising since current evidence supports that camouflaging seems to be a common mechanism in autistic girls and is associated with negative repercussions in the emotional domain (Tubío-Fungueiriño et al., 2021). Nevertheless, a multivariate analysis revealed that sex is not a significantly influential variable, in combination with other clinically significant factors, on caregivers' perception of children's HRQOL. As with most autism research, our sample is mainly composed of boys. Therefore, additional studies with higher statistical power are required to analyze the agreement between caregivers and autistic girls on their HRQOL.
While our data showed no significant effect of IQ score on the caregiver-patient agreement, presumably, the low proportion of children and adolescents having IQs in a range suggestive of intellectual disability underestimated the effect of this variable on participants' HRQOL. Furthermore, the HRQOL measure in autistic individuals with intellectual disabilities requires appropriate tools to ensure outcome reliability (Gómez et al., 2020). Undoubtedly, further research exploring well-being in this subgroup of autistic children is required.
Our low pandemic period recruitment rate certainly reflects strict and extended quarantine periods instructed by Chilean health authorities in response to the first outbreak, limiting personal mobility and impeding access to social spaces, including ambulatory rehabilitation and neurodevelopmental centers. In this way, in a prior study, our group explored the effect of confinement on children's behavior and family stress through the parental report, finding that autistic children and adolescents increased the frequency and intensity of behavioral problems. Also, both mental health disorders of caregivers and children who had a family member hospitalized due to COVID-19 were independent risk factors for increased patient behavioral problems (Nuñez et al., 2021).
HRQOL is eminently subjective. Although it is not a morbidity indicator, its measurement allows short-term resource allocation planning for groups with special healthcare requirements with a dynamic approach focused on the individual needs of the child and his or her family. Furthermore, research on chronic conditions enhances the importance of self-reporting HRQOL in the pediatric population, even for younger individuals, showing differences in parental and child perceptions (Jardine et al., 2014). Hence, to efficiently prioritize allocating health resources, it seems crucial to consider age-specific needs from the autistic children's and adolescents' viewpoints. In that sense, our findings provide evidence that strengthens age-dependent commonalities and discrepancies in perceived HRQOL between caregivers and their children and adolescents.
The findings presented in this study should be interpreted within the context of respective limitations. Sampling included most individuals evaluated in the study timeframe; however, the sample size is relatively small. The current design was cross-sectional, and it is not focused on generating explanatory models for the perception of the HRQOL; hence causation cannot be inferred. Moreover, children and their families included in the study were attended in a single neurodevelopmental unit. Therefore, it is unclear if the PedsQL scores can be generalizable to the national population. In addition, our sample was predominantly urban and white Hispanic underrepresenting indigenous communities and rural groups. Given the relatively small sample size, the drugs' potential additive or synergistic effects on HRQOL perception was not evaluated. Finally, although most caregivers were mothers and had upper secondary education, future studies must investigate the effect of demographic and socioeconomic factors on the concordance among perceived HRQOL among autistic children and their caregivers.
In conclusion, our study reveals a usually good agreement between child and parent reports. However, there are age-related discrepancies between the caregiver- and self-perception of well-being. Also, the reported PedsQL scores seem to decrease with increasing age, mainly due to the child's psychosocial health impairment. Finally, caregivers' perceptions may not reflect on the emotional and social repercussions in older children and adolescents; therefore, this group's psychological and social functioning must be observed in a targeted and systematic manner, including multi-informant reporting of HRQOL.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596.
Benjamini, Y., & Hochberg, Y. (1995). Controlling the false discovery rate: A practical and powerful approach to multiple testing. Journal of the Royal Statistical Society: Series B (methodological), 57(1), 289–300. https://doi.org/10.1111/j.2517-6161.1995.tb02031.x
Cavanna, A. E., David, K., Bandera, V., Termine, C., Balottin, U., Schrag, A., & Selai, C. (2013). Health-related quality of life in Gilles de la Tourette syndrome: A decade of research. Behavioural Neurology, 27(1), 83–93. https://doi.org/10.3233/BEN-120296
Cicchetti, D. V., & Sparrow, S. A. (1981). Developing criteria for establishing interrater reliability of specific items: Applications to assessment of adaptive behavior. American Journal of Mental Deficiency, 86(2), 127–137.
Cliff, N. (1993). Dominance statistics: Ordinal analyses to answer ordinal questions. Psychological Bulletin, 114(3), 494.
Eiser, C., & Morse, R. (2001). Can parents rate their child’s health-related quality of life? Results of a systematic review. Quality of Life Research: An International Journal of Quality of Life Aspects of Treatment, Care and Rehabilitation, 10(4), 347–357. https://doi.org/10.1023/A:1012253723272
Egilson, S. T., Ólafsdóttir, L. B., Leósdóttir, T., & Saemundsen, E. (2017). Quality of life of high-functioning children and youth with autism spectrum disorder and typically developing peers: Self- and proxy-reports. Autism: THe International Journal of Research and Practice, 21(2), 133–141. https://doi.org/10.1177/1362361316630881
Fisher, R. S., Acevedo, C., Arzimanoglou, A., Bogacz, A., Cross, J. H., Elger, C. E., Engel, J., Jr., Forsgren, L., French, J. A., Glynn, M., Hesdorffer, D. C., Lee, B. I., Mathern, G. W., Moshé, S. L., Perucca, E., Scheffer, I. E., Tomson, T., Watanabe, M., & Wiebe, S. (2014). ILAE official report: A practical clinical definition of epilepsy. Epilepsia, 55(4), 475–482. https://doi.org/10.1111/epi.12550
Gómez, L. E., Morán, M. L., Alcedo, M. Á., Arias, V. B., & Verdugo, M. Á. (2020). Addressing quality of life of children with autism spectrum disorder and intellectual disability. Intellectual and Developmental Disabilities, 58(5), 393–408. https://doi.org/10.1352/1934-9556-58.5.393
Howes, O. D., Rogdaki, M., Findon, J. L., Wichers, R. H., Charman, T., King, B. H., Loth, E., McAlonan, G. M., McCracken, J. T., Parr, J. R., Povey, C., Santosh, P., Wallace, S., Simonoff, E., & Murphy, D. G. (2018). Autism spectrum disorder: Consensus guidelines on assessment, treatment and research from the British Association for Psychopharmacology. Journal of Psychopharmacology (oxford, England), 32(1), 3–29. https://doi.org/10.1177/0269881117741766
INE. (2017). Resultados Censo 2017. Instituto Nacional de Estadística.
Jardine, J., Glinianaia, S. V., McConachie, H., Embleton, N. D., & Rankin, J. (2014). Self-reported quality of life of young children with conditions from early infancy: A systematic review. Pediatrics, 134(4), e1129–e1148. https://doi.org/10.1542/peds.2014-0352
Khanna, R., Jariwala-Parikh, K., West-Strum, D., & Mahabaleshwarkar, R. (2014). Health-related quality of life and its determinants among adults with autism. Research in Autism Spectrum Disorders, 8(3), 157–167. https://doi.org/10.1016/j.rasd.2013.11.003
Kindig, D. A., Booske, B. C., & Remington, P. L. (2010). Mobilizing Action Toward Community Health (MATCH): Metrics, incentives, and partnerships for population health. Preventing Chronic Disease, 7(4), A68.
Klassen, A. F., Miller, A., & Fine, S. (2004). Health-related quality of life in children and adolescents who have a diagnosis of attention-deficit/hyperactivity disorder. Pediatrics, 114(5), e541–e547. https://doi.org/10.1542/peds.2004-0844
Knüppel, A., Telléus, G. K., Jakobsen, H., & Lauritsen, M. B. (2018). Quality of life in adolescents and adults with autism spectrum disorder: Results from a nationwide Danish survey using self-reports and parental proxy-reports. Research in Developmental Disabilities, 83, 247–259. https://doi.org/10.1016/j.ridd.2018.09.004
Kuhlthau, K. A., McDonnell, E., Coury, D. L., Payakachat, N., & Macklin, E. (2018). Associations of quality of life with health-related characteristics among children with autism. Autism: THe International Journal of Research and Practice, 22(7), 804–813. https://doi.org/10.1177/1362361317704420
Kwan, P., Arzimanoglou, A., Berg, A. T., Brodie, M. J., Allen Hauser, W., Mathern, G., Moshé, S. L., Perucca, E., Wiebe, S., & French, J. (2010). Definition of drug resistant epilepsy: Consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia, 51(6), 1069–1077. https://doi.org/10.1111/j.1528-1167.2009.02397.x
Lai, M. C., & Szatmari, P. (2020). Sex and gender impacts on the behavioural presentation and recognition of autism. Current Opinion in Psychiatry, 33(2), 117–123. https://doi.org/10.1097/YCO.0000000000000575
Lloyd, M., MacDonald, M., & Lord, C. (2013). Motor skills of toddlers with autism spectrum disorders. Autism: THe International Journal of Research and Practice, 17(2), 133–146. https://doi.org/10.1177/1362361311402230
Lopez-Espejo, M. A., Nuñez, A. C., Moscoso, O. C., & Escobar, R. G. (2021a). Brief report: Health-related quality of life in preschoolers with autism spectrum disorder is related to diagnostic age and autistic symptom severity. Journal of Autism and Developmental Disorders, 51(12), 4704–4710. https://doi.org/10.1007/s10803-021-04909-w
Lopez-Espejo, M. A., Nuñez, A. C., Moscoso, O. C., & Escobar, R. G. (2021b). Clinical characteristics of children affected by autism spectrum disorder with and without generalized hypotonia. European Journal of Pediatrics, 180(10), 3243–3246. https://doi.org/10.1007/s00431-021-04038-7
Lord, C., Rutter, M., DiLavore, P. C., Risi, S., Gotham, K., & Bishops, S. (2012). Autism diagnosis observation schedule Torrance. CA: Western Psychological Services.
Mason, D., McConachie, H., Garland, D., Petrou, A., Rodgers, J., & Parr, J. R. (2018). Predictors of quality of life for autistic adults. Autism Research: Official Journal of the International Society for Autism Research, 11(8), 1138–1147. https://doi.org/10.1002/aur.1965
Menezes, M., & Mazurek, M. O. (2021). Associations between domains of health-related quality of life and comorbid emotional and behavioral problems in youth with autism spectrum disorder. Research in Autism Spectrum Disorders, 82, 101740. https://doi.org/10.1016/j.rasd.2021.101740
Nuñez, A., Le Roy, C., Coelho-Medeiros, M. E., & López-Espejo, M. (2021). Factors affecting the behavior of children with ASD during the first outbreak of the COVID-19 pandemic. Neurological Sciences: Official Journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology, 42(5), 1675–1678. https://doi.org/10.1007/s10072-021-05147-9
Palmer, M., Tarver, J., Carter Leno, V., Paris Perez, J., Frayne, M., Slonims, V., Pickles, A., Scott, S., Charman, T., & Simonoff, E. (2022). Parent, teacher and observational reports of emotional and behavioral problems in young autistic children. Journal of Autism and Developmental Disorders. https://doi.org/10.1007/s10803-021-05421-x
Potvin, M. C., Snider, L., Prelock, P. A., Wood-Dauphinee, S., & Kehayia, E. (2015). Health-related quality of life in children with high-functioning autism. Autism: THe International Journal of Research and Practice, 19(1), 14–19. https://doi.org/10.1177/1362361313509730
R Core Team. (2021). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. https://www.R-project.org/. Accessed 13 January 2022.
Rajmil, L., López, A. R., López-Aguilà, S., & Alonso, J. (2013). Parent-child agreement on health-related quality of life (HRQOL): A longitudinal study. Health and Quality of Life Outcomes, 11, 101. https://doi.org/10.1186/1477-7525-11-101
Ravens-Sieberer, U., Gosch, A., Rajmil, L., Erhart, M., Bruil, J., Duer, W., Auquier, P., Power, M., Abel, T., Czemy, L., Mazur, J., Czimbalmos, A., Tountas, Y., Hagquist, C., Kilroe, J., & Kidscreen Group, E. (2005). KIDSCREEN-52 quality-of-life measure for children and adolescents. Expert Review of Pharmacoeconomics & Outcomes Research, 5(3), 353–364. https://doi.org/10.1586/14737167.5.3.353
Revelle W (2021). psych: Procedures for psychological, psychometric, and personality research. Northwestern University, Evanston, Illinois. R package version 2.1.9, https://CRAN.R-project.org/package=psych. Accessed 13 January 2022.
Sheldrick, R. C., Neger, E. N., Shipman, D., & Perrin, E. C. (2012). Quality of life of adolescents with autism spectrum disorders: Concordance among adolescents’ self-reports, parents’ reports, and parents’ proxy reports. Quality of Life Research : An International Journal of Quality of Life Aspects of Treatment, Care and Rehabilitation, 21(1), 53–57. https://doi.org/10.1007/s11136-011-9916-5
Sikora, D. M., Vora, P., Coury, D. L., & Rosenberg, D. (2012). Attention-deficit/hyperactivity disorder symptoms, adaptive functioning, and quality of life in children with autism spectrum disorder. Pediatrics, 130(Suppl 2), S91–S97. https://doi.org/10.1542/peds.2012-0900G
Tilford, J. M., Payakachat, N., Kovacs, E., Pyne, J. M., Brouwer, W., Nick, T. G., Bellando, J., & Kuhlthau, K. A. (2012). Preference-based health-related quality-of-life outcomes in children with autism spectrum disorders: A comparison of generic instruments. PharmacoEconomics, 30(8), 661–679. https://doi.org/10.2165/11597200-000000000-00000
Torchiano, M. (2020). effsize: Efficient effect size computation. https://doi.org/10.5281/zenodo.1480624.
Tubío-Fungueiriño, M., Cruz, S., Sampaio, A., Carracedo, A., & Fernández-Prieto, M. (2021). Social camouflaging in females with autism spectrum disorder: A systematic review. Journal of Autism and Developmental Disorders, 51(7), 2190–2199. https://doi.org/10.1007/s10803-020-04695-x
Upton, P., Lawford, J., & Eiser, C. (2008). Parent-child agreement across child health-related quality of life instruments: A review of the literature. Quality of Life Research : An International Journal of Quality of Life Aspects of Treatment, Care and Rehabilitation, 17(6), 895–913. https://doi.org/10.1007/s11136-008-9350-5
Varni, J. W., Seid, M., & Rode, C. A. (1999). The PedsQL: Measurement model for the pediatric quality of life inventory. Medical Care, 37(2), 126–139. https://doi.org/10.1097/00005650-199902000-00003
Varni, J. W., Burwinkle, T. M., Seid, M., & Skarr, D. (2003). The PedsQL 4.0 as a pediatric population health measure: feasibility, reliability, and validity. Ambulatory Pediatrics: the Official Journal of the Ambulatory Pediatric Association, 3(6), 329–341.
Varni, J. W., Seid, M., & Kurtin, P. S. (2001). PedsQL 4.0: Reliability and validity of the Pediatric Quality of Life Inventory version 4.0 generic core scales in healthy and patient populations. Medical Care, 39(8), 800–812.
Walker, L. S., & Zeman, J. L. (1992). Parental response to child illness behavior. Journal of Pediatric Psychology, 17(1), 49–71. https://doi.org/10.1093/jpepsy/17.1.49
WHOQOL. (1996). What quality of life? The WHOQOL Group. World Health Forum, 17, 354.
Whyatt, C. P., & Craig, C. M. (2012). Motor skills in children aged 7–10 years, diagnosed with autism spectrum disorder. Journal of Autism and Developmental Disorders, 42(9), 1799–1809. https://doi.org/10.1007/s10803-011-1421-8
Yorke, I., White, P., Weston, A., Rafla, M., Charman, T., & Simonoff, E. (2018). The association between emotional and behavioral problems in children with autism spectrum disorder and psychological distress in their parents: A systematic review and meta-analysis. Journal of Autism and Developmental Disorders, 48(10), 3393–3415. https://doi.org/10.1007/s10803-018-3605-y
Acknowledgments
The authors thank UC-CHRISTUS Clinical Hospital speech and occupational therapists and participants for their important contributions to this work.
Funding
The authors received no specific funding for this work.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study's conception and design. Also, all authors contributed to the material preparation. Data collection was performed by MAL, MR, VS, and OCM. MAL performed the analysis and wrote the first draft of the manuscript. All authors commented on previous versions and read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no competing interests exist. There is not any change in the authors' affiliation subsequent to the time of the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Lopez-Espejo, M.A., Nuñez, A.C., Ruz, M. et al. Caregiver-Child Agreement in Health-Related Quality of Life of Autistic Children and Adolescents. J Autism Dev Disord 53, 977–986 (2023). https://doi.org/10.1007/s10803-022-05689-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-022-05689-7