
Abstract
New technologies (NT) are increasingly used in Occupational Therapy (OT) interventions in people with Autism Spectrum Disorder (ASD). We conducted a scoping review to describe OT interventions investigated in scientific literature which use NT in children and adolescents with ASD. Two authors independently searched the scientific databases PubMed, EMBASE, Scopus and Web of Science, carried out a peer-review screening of articles and extracted data. Twenty studies met the inclusion criteria. OT interventions lasted between 1 week and 12 months, consisted of between 1 session per day and 5 sessions per week, were carried out exclusively by an occupational therapist, and the most used NT was the computer (n = 12). The duration of the interventions and assessment measures used varied greatly between studies.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Autism Spectrum Disorder (ASD) is a neurodevelopmental disorder characterized by difficulties in social communication across multiple contexts and by unusually restricted and repetitive behaviors, interests or activities [American Psychiatric Association (APA), 2013; Lai et al., 2014]. The worldwide prevalence of ASD varies between 1 and 2% of the population (Elsabbagh et al., 2012), but it is considerably higher in the United States and South Korea [World Health Organization (WHO), 2021]. In Spain, ASD prevalence has increased over the last 40 years and differs greatly between studies, showing a prevalence of between 0.02 and 1.5% (Málaga et al., 2019).
ASD has a direct impact on peoples’ occupation which limits their autonomous and independent functioning (Lamash & Josman, 2020; Weaver, 2015), especially among children and adolescents (Huang et al., 2020; Zhang, 2002). Children and adolescents with ASD have difficulty initiating and maintaining interactions with their peers, such as playing or social activities (Gal et al., 2016; Taylor et al., 2017). Play is the most important occupation for children because it contributes to all areas of child development and facilitates the acquisition of the performance skills required for activities of daily living. In addition, in adolescents, play is also a way to improve different ASD-behaviors, family relationships as well as socialization and communication skills (Lindsay et al., 2017). Play absence or impairment can, therefore, impact negatively on their occupational performance in adult life (Blázquez-Ballesteros et al., 2015). Thus, early detection of ASD and early interventions in this population are essential to reduce their limitations in daily life (Sánchez-Raya et al., 2015). In this early intervention, the occupational therapist assumes an important role as they intervene directly on the autonomy and independence of children and adolescents with ASD (Lamash & Josman, 2020; Weaver, 2015) in different settings such as home and school (Tanner et al., 2015; Tomchek et al., 2017). These professionals use occupation and meaningful activity, in this population can be playing, in a structured way as a means of rehabilitation (Muñoz & Noriega, 2016) and they develop the intervention taking into account the preferences, needs and abilities of people with ASD (Weaver, 2015).
A systematic review published in 2017 (Hollis et al., 2017) described a rapid growth and evolution of assessments and interventions using new technologies (NT) in children and adolescents with ASD, carried out by different health professionals, including occupational therapists (Hollis et al., 2017; Odom et al., 2015). NT are defined as the study and application of current digital technologies and telecommunication systems (Lorido, 2005). In particular, new technologies for rehabilitation are ‘‘newly developed mechanical or computer systems, often involving microprocessors or computer hardware and software’’ used by a therapist ‘‘to remediate impairment, promote recovery, and improve peoples’ function’’ (Chen & Bode, 2011). Intervention studies using NT have used a variety of devices such as computers, smartphones, tablets, robots, virtual reality and wearable technology, with the aim of increasing communication, social, emotional and academic skills in children and adolescents with ASD (Sandgreen et al., 2020). Specifically, scientific evidence on Occupational Therapy (OT) intervention using NT in children and adolescents with ASD has shown beneficial effects in children’s academic skills (literacy and numeracy) (Shic & Goodwin, 2015), the performance of activities of daily living (Becker et al., 2016; Shic & Goodwin, 2015) as well as in the acquisition of social skills (interaction and collaboration with their peers) (Bauminger-Zviely et al., 2013; Shic & Goodwin, 2015).
Despite the fact that the results obtained in different studies suggest a positive effect of NT for children and adolescents with ASD (Lamash & Josman, 2021; Odom et al., 2015; Sandgreen et al., 2020; Shic & Goodwin, 2015), some studies pointed out that scientific evidence on the efficacy of these interventions is still inconclusive (Lorido, 2005; Odom et al., 2015). However, NT improve access to interventions because they can be performed remotely, and therefore allow more adaptive, interactive and predictable interventions (Hollis et al., 2017). In addition, NT are a motivating and attractive intervention for children and adolescents because today, children and adolescents belong to the "digital generation" for whom technology forms part of daily life from a very early age (Odom et al., 2015). For these reasons, NT are a very useful tool to complement OT intervention for children and adolescents with ASD. Based on this background, two research questions emerged: (1) What are the most commonly used NT in OT interventions in children and adolescents with ASD in the scientific literature? (2) What are the characteristics of OT interventions with NT in children and adolescents with ASD investigated in the scientific literature? The aim of this scoping review was to describe OT interventions investigated in scientific literature which use NT in children and adolescents with ASD.
Methods
A scoping review was conducted following the standards of the Cochrane Handbooks Version 6.2, 2021 (Higgins & Thomas, 2021) and the recommendations of the PRISMA Extension for Scoping Reviews (PRISMA-ScR) (Tricco et al., 2018). We have not published a protocol of this review nor registered it on PROSPERO or any other similar scientific website.
Search Strategy
We performed a systematic literature search on the databases MEDLINE (PubMed), EMBASE, Scopus and Web of Science (WOS) on November 16, 2020. We performed an additional manual search of several OT journals indexed in the Journal Citation Reports (JCR) including those with the highest impact (indexed in the first quartile): American Journal of Occupational Therapy (AJOT); Australian Occupational Therapy Journal (AOJT); British Journal of Occupational Therapy (BJOT); Canadian Journal of Occupational Therapy (CJOT); Hong Kong Journal of Occupational Therapy (HKJOT); Journal of Occupational Rehabilitation (JOR); Occupational Therapy International (OTI); Occupation, Participation and Health (OTJR); Physical and Occupational Therapy in Pediatrics (POTP); Scandinavian Journal of Occupational Therapy (SJOT). We used the same search strategy in all the sources consulted, including all ASD disorders, ‘occupational therapy’, and different terms included in NT as search terms, combined with the Boolean operators AND and OR. Search strategies used in all databases can be found in Table 1.
Review Criteria
In this review, we included all articles that met the following inclusion criteria: (a) Studies with experimental design: non-randomized controlled trials, randomized controlled trials, quasi-experimental studies, pilot studies, case report and exploratory studies; these types of studies are included in the levels of evidence 2,3,4 established by the Oxford Centre for Evidence-Based Medicine (Centre for Evidence-Based Medicine (CEBM) n.d.); (b) children or adolescent population (under 18 years old); (c) study population with a diagnosis of ASD: Asperger's Syndrome, Rett Syndrome, Disintegrative Disorder, Classic Autistic Disorder, and Pervasive Developmental Disorder, (d) OT intervention using NT: app, tablet, iPad, mobile, virtual reality, computer, laptop, technology device, internet, video game or software. We excluded the following: (a) studies not published in English and/or Spanish; and (b) with no full-text available.
No filters by time or type of study were applied during the literature search in any of the databases and journals consulted.
Study Selection
We downloaded and compiled all the article titles obtained from all the searches using Microsoft Excel for further review and screening. One researcher (SDL) carried out a preliminary screening which consisted of removing duplicates. Two researchers (SDL and LMCG) then reviewed and screened the articles independently. We performed three comprehensive, successive and screenings: by title, by abstract and by full text. In each screening, articles that did not meet the inclusion criteria were discarded. A third review research (MGDH) resolved discrepancies between SDL and LMCG regarding study inclusion at the end of each of the three screenings.
Data Extraction and Synthesis
Before the data extraction, all researchers designed the tables and defined the items to be included in them, in order to reduce subjectivity in the synthesis of the data. We elaborated three tables based on the Cochrane Handbook (Higgins & Thomas, 2021). Table 2, which provides information on the main characteristics of the studies included in this review through the following items: author/year, study design, sample/country, participants, intervention/comparator, evaluation, and study outcomes (Page et al., 2021). Table 3, which provides information on the main characteristics of the interventions conducted in the studies included in this review through the following items: author/year, participants, intervention, duration of intervention, sessions, intervention manager and main results (Page et al., 2021). And finally, Table 4, which provides information regarding aspects related to the risk of bias in the articles included in this review through the following items: author/year, main limitations, funding sources and declarations of interest (Boutron et al., 2021). Two researchers (SDL and LMCG) performed the data extraction independently, LTC resolved discrepancies about data extraction.
We made a descriptive synthesis of the results and used tables and figures as far as possible to present the flow of the study selection process and the characteristics of the included studies. In addition, as a multidisciplinary research team, we discussed categories to classify the different types of OT interventions using NT in children and/or adolescents with ASD used in the included studies in the results section.
Quality Assessment
The quality of the included studies was not assessed as this is not a mandatory requirement of scoping reviews (Arksey & O’Malley, 2005; Levac et al., 2010; Peters et al., 2020; Tricco et al., 2016, 2018). However, we have included a table about risk bias, as recommended in the Cochrane Handbook (Higgins & Thomas, 2021), which includes information on the main limitations reported in the included articles, funding sources and declarations of interest (Table 4) to make readers aware of these characteristics and to enable them to assess the results presented in this scoping review more critically. The main limitations reported by the authors of each included study are also discussed in the results section.
Results
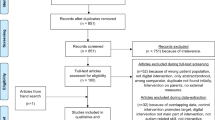
We identified 2226 published articles on OT intervention with NT in children and adolescents, which resulted in 1840 after removing duplicates. 1840 articles were screened by title, 968 by abstract and 86 by full text. Of these 86 articles, 20 met the inclusion criteria and were included in this scoping review. The study selection flowchart is shown in Fig. 1.

Flowchart of the study selection process
Participants and sample
The main characteristics of the included studies are summarized in Table 2. Nine studies were conducted in Asian countries, seven in the United States, three in Australia and one in Europe. The study population of all the included articles consisted of children or adolescents with a diagnosis of ASD but nine of them, (Campbell et al., 2015; Cosper et al., 2009; Gal et al., 2016; Henning et al., 2016; Janeslätt et al., 2014; Josman et al., 2008; Lo et al., 2009; Lorah et al., 2014; Palsbo & Hood-Szivek, 2012) in addition to children and adolescents diagnosed with ASD, also included other diagnoses such as Attention Deficit Hyperactivity Disorder (ADHD), Intellectual Disability, Infantile Cerebral Palsy, Spina Bifida, Cerebellar Hypoplasia, Auditory Processing Disorder and undiagnosed population. The sample size varied greatly between included studies, two being the lowest number of participants (Lee et al., 2013), and ninety-four the highest (Hatfield et al., 2017).
Study Design
Six of the included articles are pilot studies (two of them were randomized controlled clinical trials and four of them were quasi-experimental studies), (Henning et al., 2016; Ikuta et al., 2016; Josman et al., 2008; Lo et al., 2009; Meister & Salls, 2015; Palsbo & Hood-Szivek, 2012), five are quasi-experimental studies (Cosper et al., 2009; Gal et al., 2016; Gentry et al., 2010; Lee et al., 2016; Wuang et al., 2010), four are non-randomized clinical trials (Campbell et al., 2015; Hatfield et al., 2017; Lamash & Josman, 2021; Lee et al., 2013), three are randomized controlled clinical trials (Hochhauser et al., 2018; Janeslätt et al., 2014; Parsons et al., 2019), and two are case reports (Chen et al., 2015; Lorah et al., 2014). Only six of all included studies included a control group (Hatfield et al., 2017; Hochhauser et al., 2018; Janeslätt et al., 2014; Josman et al., 2008; Lamash & Josman, 2021; Parsons et al., 2019). In four of them (Hatfield et al., 2017; Hochhauser et al., 2018; Lamash & Josman, 2021; Parsons et al., 2019) the control group received either the usual therapy or received no intervention. In one study (Josman et al., 2008) both groups received the same intervention, the only difference being the number of sessions. Finally, in one study (Janeslätt et al., 2014) both groups received the same intervention, although the intervention group was treated before the control group, while the control group received a usual therapy. Two studies (Ikuta et al., 2016; Wuang et al., 2010) had two intervention groups, both of whom received the same intervention, although in different phases of the study or in a different order (Table 2).
Study Variables and Measuring Instruments
Activities of daily living (ADLs) and related abilities are the most studied outcome among the included studies (n = 9). Occupational performance was assessed in three studies by using different instruments such as the Child Occupational Self-Assessment (COSA) (Meister & Salls, 2015), the Canadian Occupational Performance Measure (COPM) (Gentry et al., 2010) or video analysis (Campbell et al., 2015). In nine studies, specific ADL such as shopping (Lamash & Josman, 2021), mobility in the community (crossing street) (Josman et al., 2008), mealtime (Lo et al., 2009), toothbrushing (Lo et al., 2009) and play skills (Henning et al., 2016), were assessed with the Test of grocery shopping skills (TOGSS), the Pedestrian safety scale (PSS), duration of meals and % of non-feeding behaviors through video recording, the number of brushing strokes through video recording and plaque-revealing dye, and the Test of Playfulness (ToP), respectively (Table 2).
Social skills are the second most frequent study outcome among the included studies (n = 6). Two studies (Chen et al., 2015; Lee et al., 2016) assessed emotion recognition with non-standardized assessments such as video recording observation and questions regarding video-stories. Among the rest of the studies investigating social skills, several different measurement instruments were used. One study (Henning et al., 2016) used the Conners' Comprehensive Behaviour Rating Scales-Parent (CCBRS-P) to assess social and behavioral problems. One study (Gal et al., 2016) investigated social interaction assessing it with the Friendship Observation Scale (FOS). One study (Hochhauser et al., 2018) measured conflict management and negotiation attitude using the Five Factor Negotiation Scale (FFNS) and The ConflictTalk questionnaire. Another (Parsons et al., 2019), assessed social imitation with the Communication and Symbolic Behavior Scales (CSBS) (Table 2).
Cognitive skills are the third most frequent study outcome among the included studies (n = 5). General cognitive functioning was assessed in two studies by the use of WebNeuro software (Lamash & Josman, 2021) and the Mullen Scales of Early Learning (MSEL) (Parsons et al., 2019). Specific cognitive aspects such as sustained attention (Cosper et al., 2009), time management (Janeslätt et al., 2014) and self-determination (Hatfield et al., 2017) were assessed with the Gordon Diagnostic Systems, the Kit for assessing Time-processing ability in children (KaTid-Child), and the AIR Self-Determination Scale (AIR), respectively (Table 2).
Motor skills were assessed less frequently than cognitive skills in the included studies (n = 3). Among the motor skills assessed, we found: motor control (Cosper et al., 2009; Palsbo & Hood-Szivek, 2012; Wuang et al., 2010) assessed with the Bruininks-Oseretsky Test of Motor Proficiency-Short Form (Cosper et al., 2009), the Beery-Buktenica Developmental Test of Visual-Motor Integration (VMI) (Palsbo & Hood-Szivek, 2012), and the Bruininks-Oseretsky Test of Motor Proficiency (BOTMP) (Wuang et al., 2010); motor coordination assessed with the Bruininks-Oseretsky Test of Motor Proficiency-Short Form (Cosper et al., 2009), and handwriting, assessed with the Test of Handwriting Skills-Revised (THS-R) and the Evaluation Tool of Children’s Handwriting (ETCH) (Palsbo & Hood-Szivek, 2012) (Table 2).
Other outcomes and questionnaires were studied to a lesser extent in the included studies. Sensory integration was assessed (Wuang et al., 2010) with the Test of Sensory Integration Function (TSIF); visual-spatial skills were assessed with the Developmental test of visual-perceptual skills-2 (DTVP-2) (Lee et al., 2013), speech generation was assessed using the Proloquo2Go trial score (Lorah et al., 2014), and intervention effectiveness was assessed using the Goal Attainment Scaling (GAS) (Ikuta et al., 2016) (Table 2).
NT Used in OT Interventions in Children and Adolescents with ASD
NT used in the OT interventions in the included studies can be categorized into three clear types: OT interventions using computers (n = 12), OT interventions using iPad™ (n = 3) and OT interventions using another NT (n = 5) such as Personal Digital Assistant (PDA) (n = 2), assistive robot (n = 1), simulated Developmental Horse-Riding Program (SDHRP) (n = 1) and earmuffs and Noise-cancelling Headphones (n = 1).
OT Interventions Using NT in Children and Adolescents with ASD
The specific characteristics of these interventions are summarized in Table 3. All interventions described in the included studies were exclusively carried out by occupational therapists (n = 20) (Campbell et al., 2015; Chen et al., 2015; Cosper et al., 2009; Gal et al., 2016; Gentry et al., 2010; Hatfield et al., 2017; Henning et al., 2016; Hochhauser et al., 2018; Ikuta et al., 2016; Janeslätt et al., 2014; Josman et al., 2008; Lamash & Josman, 2021; Lee et al., 2013, 2016; Lo et al., 2009; Lorah et al., 2014; Meister & Salls, 2015; Palsbo & Hood-Szivek, 2012; Parsons et al., 2019; Wuang et al., 2010), psychologists, teachers and research professors formed part of the intervention team in only three of them (Janeslätt et al., 2014; Palsbo & Hood-Szivek, 2012; Parsons et al., 2019). Computers were the most used NT in the included studies (n = 12). In general, intervention programs lasted between 1 and 15 weeks, although in two studies the intervention lasted 40 (Wuang et al., 2010) and 48 weeks (Hatfield et al., 2017). The intervention programs consisted of between 1 and 5 weekly sessions, but in one study there were 9 weekly sessions (Henning et al., 2016). Only two interventions carried out daily sessions (Lorah et al., 2014; Parsons et al., 2019). In general, the sessions lasted 45–60 min, except for one study (Janeslätt et al., 2014), which lasted 120 min. Some studies, did not state the duration of the intervention programs (Janeslätt et al., 2014; Josman et al., 2008; Lorah et al., 2014) or that of sessions performed (Ikuta et al., 2016).
OT Interventions Using Computers
The most frequently used device in OT interventions is the computer (n = 12) (Campbell et al., 2015; Chen et al., 2015; Cosper et al., 2009; Gal et al., 2016; Hatfield et al., 2017; Henning et al., 2016; Hochhauser et al., 2018; Josman et al., 2008; Lamash & Josman, 2021; Lee et al., 2013, 2016; Lo et al., 2009). It is a highly versatile device with different intervention options that can be differentiated as follows:
Computer Applications
Two studies (Lee et al., 2013; Lo et al., 2009) used computer applications, aimed at training basic ADLs and improving visuo-perceptual skills. In both articles the intervention was performed exclusively by an occupational therapist. The duration of the intervention varied from 1 to 6 weeks with two to three sessions per week.
Virtual Environments
Two studies (Josman et al., 2008; Lamash & Josman, 2021) conducted an intervention using computer-based virtual environments to improve instrumental ADLs and social conversations. In both articles the intervention was performed exclusively by an occupational therapist. The duration of the intervention varied from 1 to 8 weeks, with a weekly session of 45 min.
Video Modeling
Four studies (Campbell et al., 2015; Gal et al., 2016; Hochhauser et al., 2018; Lee et al., 2016) conducted a video modeling intervention focused on emotion recognition, conflict resolution, social interaction and ADLs. All the interventions were performed exclusively by an occupational therapist. The duration of the intervention varied from 4 to 8 weeks with a 1-h weekly session.
Online Programs
One study (Hatfield et al., 2017) carried out an online program to prepare children for the transition to high school. The intervention was performed exclusively by an occupational therapist and lasted 12 months.
Augmented Reality
One study (Chen et al., 2015) used an augmented reality system to train social skills. The intervention was performed exclusively by an occupational therapist. The duration of the intervention was one and a half months with a total of seven sessions.
Non-invasive PC-Based Technology
One study (Cosper et al., 2009), used non-invasive pc-based technology to improve motor coordination and sustained attention. The intervention was performed exclusively by an occupational therapist. The duration of the intervention was 15 weeks with a 1-h weekly session.
Multiuser Tabletops Technology
One study (Henning et al., 2016) used a multi-touch collaboration computer interface table to improve collaboration skills. The intervention was performed exclusively by an occupational therapist. The duration of the intervention was 3 weeks with three to four forty-five-minute weekly sessions.
OT Interventions Using iPads™
The second most used device was the iPad™ (n = 3) (Lorah et al., 2014; Meister & Salls, 2015; Parsons et al., 2019). This device was used to improve social, visuo-motor, imitation, language and ADL skills. The interventions were performed exclusively by an occupational therapist, except in one study (Parsons et al., 2019), in which a psychologist collaborated. The duration of the intervention varied from to 6 weeks to 3 months with two 25 min weekly sessions (Meister & Salls, 2015) or daily sessions (Lorah et al., 2014; Parsons et al., 2019).
Interventions Using Another NT
Personal digital assistant (PDA): Two studies (Gentry et al., 2010; Janeslätt et al., 2014) used a PDA to train time management in daily life. One intervention was performed by an occupational therapist and the other by an occupational therapist and a special educator. In one study the duration of the intervention program was 40 days (Gentry et al., 2010) and in the other the duration was not stated (Janeslätt et al., 2014). Three ninety-minute sessions (Gentry et al., 2010) and an undisclosed number of 2-h sessions (Janeslätt et al., 2014) were performed.
Assistive Robot
One study (Palsbo & Hood-Szivek, 2012) used an assistive robot with haptic interface software to improve handwriting. The intervention was performed by an occupational therapist and a research professor. The duration of the intervention was 4 to 6 weeks with 4 weekly sessions.
Simulated Developmental Horse-Riding Program (SDHRP)
One study (Wuang et al., 2010) used a simulated developmental horse-riding program using JOBA® which focused on the development of motor skills and sensory integration. The intervention was performed exclusively by an occupational therapist. The duration of the intervention program was two twenty-week phases with 2 weekly sessions.
Earmuffs and Noise-Cancelling Headphones
One study (Ikuta et al., 2016) used earmuffs and noise-cancelling headphones to reduce behaviors related to auditory hyperreactivity. The intervention was performed by an occupational therapist. The intervention lasted for 6 weeks.
Main Results of Included Studies
The specific results of each study are shown in Table 3. The effect of the interventions was positive in most of the articles, expressed as significant differences in the results either pre-post intervention or between the intervention group and control group. Seven studies (Campbell et al., 2015; Gentry et al., 2010; Janeslätt et al., 2014; Josman et al., 2008; Lamash & Josman, 2021; Lo et al., 2009; Meister & Salls, 2015) showed significant improvements in the performance of basic and instrumental ADLs, such as eating, personal hygiene, shopping, mobility in the community and time management in these activities. Five studies (Chen et al., 2015; Gal et al., 2016; Henning et al., 2016; Hochhauser et al., 2018; Lee et al., 2016) showed significant improvements in social skills, including collaboration, emotion recognition and conflict resolution. Two studies (Palsbo & Hood-Szivek, 2012; Wuang et al., 2010) reported significant improvements in motor skills, such as graphomotor skills and balance, and in sensory integration skills. One study (Lorah et al., 2014) showed significant improvements in communication and one study (Lee et al., 2013) found significant improvements in visual-spatial skills.
However, in some articles no significant results were reported. In two articles (Hatfield et al., 2017; Parsons et al., 2019), no significant results were reported when the groups were compared. In addition, one article (Cosper et al., 2009) only showed significant improvements in motor control, but not in the other study outcomes, sustained attention and motor coordination. In one study (Ikuta et al., 2016), of the two tools used in the intervention, only the results obtained by earmuffs were significant.
Main Limitations of Included Studies
In Table 4 we show the main limitations reported by the authors of included studies, as well as other ethical aspects that could influence the interpretations of the obtained results, such as conflict of interest and funding sources.
The main limitation in included articles is small sample size, which was reported in twelve of them (Campbell et al., 2015; Gal et al., 2016; Gentry et al., 2010; Hatfield et al., 2017; Henning et al., 2016; Ikuta et al., 2016; Janeslätt et al., 2014; Josman et al., 2008; Lamash & Josman, 2021; Lee et al., 2013, 2016; Palsbo & Hood-Szivek, 2012). In seven studies, authors reported the absence of a control group (Cosper et al., 2009; Gentry et al., 2010; Henning et al., 2016; Ikuta et al., 2016; Janeslätt et al., 2014; Meister & Salls, 2015; Wuang et al., 2010), in six studies, authors reported the lack of monitoring and/or evaluation of the transference of results to the natural context was reported (Hatfield et al., 2017; Hochhauser et al., 2018; Ikuta et al., 2016; Lamash & Josman, 2021; Lorah et al., 2014; Meister & Salls, 2015), in four studies, authors reported a limited duration of the intervention (Campbell et al., 2015; Janeslätt et al., 2014; Lee et al., 2016; Meister & Salls, 2015), in three studies, authors reported a non-randomized and non-representative sample (Gal et al., 2016; Gentry et al., 2010; Hatfield et al., 2017), in three studies, authors reported a high withdrawal rate (Hatfield et al., 2017; Janeslätt et al., 2014; Lamash & Josman, 2021), in one study the dose and fidelity of treatment was lower than prescribed (Parsons et al., 2019), and in another, 43% of the sample refused to use any of the interventions (Ikuta et al., 2016). Finally, with regard to measurement instruments, one article highlights the absence of a valid instrument (Palsbo & Hood-Szivek, 2012), one used KaTid-Child and Time Parent scales, which have not previously been used to assess long-term effects (Janeslätt et al., 2014), and one used the Five Factory Negotiation Scale, which has a low internal consistency (Hochhauser et al., 2018).
Regarding declarations of interest, in seven articles (Campbell et al., 2015; Henning et al., 2016; Ikuta et al., 2016; Janeslätt et al., 2014; Lamash & Josman, 2021; Lee et al., 2016; Parsons et al., 2019) authors declared that they had no conflict of interest. In one article (Hatfield et al., 2017), the authors declare a conflict of interest, based on the fact that the first author of the manuscript that described the efficacy of the BOOST-A program is also the developer of the program. The remaining articles did not include any information regarding conflicts of interest.
Funding sources for the articles were mostly public. Six articles (Gentry et al., 2010; Hatfield et al., 2017; Hochhauser et al., 2018; Ikuta et al., 2016; Lee et al., 2016; Palsbo & Hood-Szivek, 2012) obtained funding through grants, scholarships and support from public institutions. In one article (Campbell et al., 2015), authors stated that they had not received any financial support. The remaining articles did not provide information on funding sources.
Discussion
The present scoping review describes the characteristics of OT interventions using NT in the rehabilitation of children and/or adolescents with ASD. We reviewed the available knowledge in different databases and OT journals and identified 20 articles which investigated OT interventions using NT in children and adolescents with ASD. In the interventions described in these studies, researchers used 12 different technologies, of which the computer and iPad™ were most used. The main goal of the interventions was to increase the performance of basic and instrumental ADLs, social skills, cognitive skills, motor skills and, to a lesser extent, other abilities such as sensory integration or intervention effectiveness.
All included articles were published during the last 13 years. The fact that all of the articles were quite recent can be partly explained by the fact that the use of NT as a therapeutic tool is relatively new. In 1993 and 1997, the first medical entities for the evaluation of NT in healthcare were created, and were dedicated to examining the clinical, social, economic and legal consequences of the use of technologies (Vidal-España et al., 2007). As a result, research using NT in the health context could not begin until some years later, and even more so in those areas that have not been recognized as health professions, which is the case of OT in many countries. In fact, it is in the last 10 years that there have been published articles supporting the growth of technology in ASD interventions (Pandina, 2021), which has led to an increasing use of NT as a rehabilitation tool. To some extent, this could also be due to the current increase in the popularity of NT, the greater availability of technologies and the rapid technological development worldwide.
Among the included studies, those carried out in Asian countries (n = 9) and in the United States (n = 7) stand out. This could be explained by the fact that these countries have the highest prevalence of child-adolescent ASD in the world [World Health Organization (WHO), 2021], which makes ASD a relevant public health problem and, therefore a research priority. In contrast, the low representation of European countries, such as Spain, is noteworthy. This could be attributed, among other reasons, to the low prevalence of ASD in these countries (Málaga et al., 2019). In addition, recent studies have underlined the fact that Spain has a high level of obsolescence in terms of currently installed technological healthcare equipment [Federación Española de Empressas de Tecnología Sanitaria (Fenin) 2019] which makes research in this field difficult.
NT Used in OT Interventions in Children and Adolescents with ASD
The most commonly used device in the interventions described in the included articles was the computer, followed by the iPad™ and, other technologies such as assistive robots, PDA, earmuffs and headphones and simulated developmental horse-riding programs. One clear reason for this is that computers are the most widely owned device in the population, and are present in most ASD children’s homes and schools (Ramdoss et al., 2011). The National Statistics Institute (INE) indicates the presence of computers in 81.4% of households (Instituto Nacional de Estadística, 2021). This popularity has made computers an easy device to implement in rehabilitation centers because children and adolescents with ASD are familiar with their use. In fact, previous studies indicated a clear preference of children with ASD for computers and their screens (Moore & Calvert, 2000).
In contrast, emerging NT such as robotics or augmented reality systems have been less used in the OT interventions described in included studies. This could be partly explained by the fact that OT interventions are mainly focused on the recovery of ADL in children and adolescents with ASD, and the evidence with regard to the use of emerging NT (i.e. robotics) in these children is specially related to social skills in communication (Kumazaki et al., 2020). In fact, the results of the interventions using robots showed that children with ASD achieve a higher level of task engagement when they interact with robots than with humans (Schadenberg et al., 2020). There has been too little research into the adequate necessary conditions of the interventions using emerging NT to generalize these results to human interactions (Pop et al., 2013).
OT Interventions Using NT in Children and Adolescents with ASD
Most of the interventions described in included articles have been carried out exclusively by occupational therapists, without the support of a multidisciplinary team. We are surprised that other professionals collaborated in the interventions in only three studies (Janeslätt et al., 2014; Lorah et al., 2014; Parsons et al., 2019). Most of the OT interventions using NT were mainly focused on increasing ADLs, followed by social, cognitive and motor skills. This was as expected because we searched specifically for OT interventions, and these professionals are responsible for the rehabilitation of ADLs thorough occupation (Kuhaneck et al., 2020). Similarly, the fact that ASD children present several social difficulties, such as persistent impairments in social communication and social interaction in different contexts justifies the researchers' interest in social skills as a study outcome in the included studies [American Psychiatric Association (APA), 2002].
Surprisingly, no article has studied participation, which is a characteristic concept related to OT. A reason for this can be that occupation is closely related to participation. In fact, some authors point out that occupation is the “means” to rehabilitation and participation is the “end” (Larsson-Lund & Nyman, 2017) and this is could lead to confusion between the two terms and to use them indistinctly. Participation is included as a key aspect in a number of practice models in OT and is defined in the International Classification of Functioning, Disability and Health (ICF) as “involvement in a life situation” (WHO, 2001). Children and adolescents with ASD are particularly at risk of presenting restrictions in their participation. Previous studies have shown that children and adolescents with ASD participate in activities less frequently and with less variety than their peers with other disabilities or typical development (Rodger & Umaibalan, 2011; Shattuck et al., 2011). In this sense, the digitalization of society is changing the way OT is carried out as well as people's participation (Larsson-Lund & Nyman, 2019). NT can help occupational therapists to achieve their intervention goals, thanks to the simulation of real contexts and ADLs, in a personalized, interactive and novel way; but in a safe and familiar environment for children and adolescents with ASD, which facilitates and promotes their learning (Valencia et al., 2019) and therefore, in some way, also their participation.
The characteristics of the OT interventions using NT varied greatly among included studies in terms of intervention program duration, number of sessions, duration of the sessions and technology used. It is possible that this was an effect of the inclusion of different experimental studies in our scoping review, because often a case report or exploratory studies have a shorter intervention program duration than controlled trials. The duration of the sessions is the most stable parameter among included studies, and was usually between 45 and 60 min, which is a typical session length.
OT interventions using NT described in included studies have shown positive results in different aspects of children and adolescents with ASD, such as ADLs and social skills. These results could be conditioned by the limitations reported in the included studies, such as the small sample size, the absence of a control group, the limited duration of the interventions, the lack of follow-up, the lack of evaluation of the transference of the results to the natural context, and the selection of non-randomized and non-representative samples. However, these positive effects on ADLs and social skills have also appeared in previous published reviews (Becker et al., 2016; Vidal-España et al., 2007). Although not in the OT field, the reviews by Wainer et al. (Wainer & Ingersoll, 2011) and Tanner et al. (Tanner et al., 2015), described the use of NT as adjuvants to conventional intervention to improve facial and emotion recognition, social problem solving and social behaviors in children with ASD. Therefore, NT could be seen as a useful and complementary tool to OT intervention in children and/or adolescents with ASD.
Practical and Clinical Implications
The interventions presented in this review are part of an emerging area of research, and offer occupational therapists a great opportunity for research and clinical practice. This review provides information on outcomes, types of interventions and technologies without focusing on a specific area or variable of intervention, providing a broader view of the use of NT in OT interventions in children and adolescents with ASD. Professionals could use the results to develop intervention programs based on NT, and include the different tools presented in their intervention sessions with children and adolescents with ASD. We also provide a summary of current evidence that can support the performance of evidence-based OT practice. However, occupational therapists should consider the results of this scoping review carefully before determining and developing intervention plans for their patients.
Strengths and Limitations of this Scoping Review
Our scoping review presents some limitations that should be considered when interpreting its results. Although we performed a systematic peer review to ensure scientific rigor, the lack of information reported in included studies, the publication bias which limits null results of the interventions, and the selection bias are limitations for the majority of reviews. Regarding inclusion criteria, we only included articles published in English and/or Spanish and with full text available, so we may have excluded studies that could provide relevant information published in another language. Regarding the search strategy, the terms that define ASD and NT were difficult to define. In recent years ASD classification has been modified and there is no consensus on the terminology used in existing articles. Therefore, we have used the terms included in the DSM-IV [American Psychiatric Association (APA), 2002], which categorizes ASD as: Autistic Disorder, Pervasive Developmental Disorders, Rett Syndrome, Childhood Disintegrative Disorder and Asperger Syndrome. As a result, studies using other terms such as hyperactive disorder associated with mental retardation and stereotyped movements present in the ICD-10 may have been overlooked. Something similar occurred with the included terms in NT. We decided to include different terms that had already been used in previous published reviews (Sandgreen et al., 2020; Strubbia et al., 2020). Moreover, in this review we only included those articles in which occupational therapists were one of the professionals who performed the interventions in ASD. Thus, it is possible that we overlooked articles in which occupational therapists were involved in the intervention, but this was not clearly specified in the study, which favored the selection bias. With regard to included studies, we need to point out that we have only included experimental studies which could contain biases related to this type of study design. In addition, in some of them, measurement instruments which were not validated or standardized were used (Campbell et al., 2015; Chen et al., 2015; Josman et al., 2008; Lee et al., 2013, 2016; Lo et al., 2009; Lorah et al., 2014). Moreover, we have not performed an assessment of the quality of the included studies, which means that some of the articles included in this review may have a low methodological quality. However, we have presented the main reported limitation of every included study in Table 3 and other aspects related to the quality of the results, such as conflicts of interest in Table 4. Finally, the high level of variability in terms of assessment tools, outcomes, sample size and duration of intervention among included articles makes it difficult to compare included studies and to draw conclusions. Thus, the results of this scoping review must be interpreted with caution.
Our scoping review also presents some strengths. We should highlight that we have not found other reviews in the scientific literature aimed at describing OT interventions using NT in children and adolescents with ASD. Thus, our scoping review may provide relevant information in a field that has been investigated very little. In addition, this review provides information regarding current gaps in knowledge from which to begin future lines of research: (i) OT interventions using NT in children and adolescents with ASD have been investigated very little in European countries; (ii) There has been very limited research into OT interventions using smartphones and emerging technologies such as robotics; (iii) Multidisciplinary intervention in children and adolescents with ASD using NT is scarce; (iv) OT interventions using NT in children and adolescents with ASD varied greatly in duration and number of sessions. Moreover, we underline the necessity of performing further studies with a larger sample size, containing a control group, with a representative and random sample, and in which validated assessment tools are used.
Conclusion
The computer was the most frequently used NT in OT interventions in children and adolescents with ASD, followed by iPad™ and other technologies such as augmented reality or robots. The interventions were mainly carried out exclusively by an occupational therapist and were focused on the improvement of ADLs and social skills. The duration of the interventions lasted between 1 week and 12 months, and the number of sessions ranged between 1 daily session to 5 per week. However, the characteristics of the OT interventions using NT in children and adolescents with ASD varied greatly between studies, so further studies are needed to help quantify and define these parameters.
References
American Psychiatric Association (APA). (2002). Diagnostic and statistical manual of mental disorders DSM-IV-TR (4th ed.). American Psychiatric Association.
American Psychiatric Association (APA). (2013). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Publishing.
Arksey, H., & O’Malley, L. (2005). Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology, 8(1), 19–32. https://doi.org/10.1080/1364557032000119616
Blázquez-Ballesteros, M. P., Mahmoud-Saleh Uceros, L., & Guerra-Redondo, L. (2015). Terapia ocupacional pediátrica, Algo más que un juego. Revista Electrónica De Terapia Ocupacional Galicia, TOG, 2(7), 7.
Bauminger-Zviely, N., Eden, S., Zancanaro, M., Weiss, P. L., & Gal, E. (2013). Increasing social engagement in children with high-functioning autism spectrum disorder using collaborative technologies in the school environment. Autism: The International Journal of Research and Practice, 17(3), 317–339. https://doi.org/10.1177/1362361312472989
Becker, E. A., Watry-Christian, M., Simmons, A., & Van Eperen, A. (2016). Occupational therapy and video modeling for children with autism. Journal of Occupational Therapy, Schools & Early Intervention, 9(3), 226–241. https://doi.org/10.1080/19411243.2016.1195603
Boutron, I., Page, M., Higgins, J., Altman, D., Lundh, A., & Hróbjartsson, A. (2021). Chapter 7: Considering bias and conflicts of interest among the included studies. In J. P. T. Higgins, J. Thomas, J. Chandler, M. Cumpston, T. Li, M. J. Page, & V. A. Welch (Eds.), Cochrane handbook for systematic reviews of interventions version 6.2. Cochrane. https://training.cochrane.org/handbook/current/chapter-07.
Campbell, J. E., Morgan, M., Barnett, V., & Spreat, S. (2015). Handheld devices and video modeling to enhance the learning of self-help skills in adolescents with autism spectrum disorder. OTJR: Occupation, Participation and Health, 35(2), 95–100. https://doi.org/10.1177/1539449215570040
Centre for Evidence-Based Medicine (CEBM). (n.d.). The Oxford levels of evidence. Retrieved December 9, 2021 from https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence.
Chen, C. C., & Bode, R. K. (2011). Factors influencing therapists’ decision-making in the acceptance of new technology devices in stroke rehabilitation. American Journal of Physical Medicine & Rehabilitation, 90(5), 415–425. https://doi.org/10.1097/PHM.0b013e318214f5d8
Chen, C.-H., Lee, I.-J., & Lin, L.-Y. (2015). Augmented reality-based self-facial modeling to promote the emotional expression and social skills of adolescents with autism spectrum disorders. Research in Developmental Disabilities, 36C, 396–403. https://doi.org/10.1016/j.ridd.2014.10.015
Cosper, S. M., Lee, G. P., Peters, S. B., & Bishop, E. (2009). Interactive Metronome training in children with attention deficit and developmental coordination disorders. International Journal of Rehabilitation Research. Internationale Zeitschrift Fur Rehabilitationsforschung. Revue Internationale De Recherches De Readaptation, 32(4), 331–336. https://doi.org/10.1097/MRR.0b013e328325a8cf
Elsabbagh, M., Divan, G., Koh, Y.-J., Kim, Y. S., Kauchali, S., Marcín, C., et al. (2012). Global prevalence of autism and other pervasive developmental disorders. Autism Research: Official Journal of the International Society for Autism Research, 5(3), 160–179. https://doi.org/10.1002/aur.239
Federación Española de Empressas de Tecnología Sanitaria (Fenin). (2019). Perfil tecnológico hospitalario y propuestas para la renovación de tecnologías sanitarias. Retrieved July 1, 2021 from https://www.fenin.es/resources/estudios/621.
Gal, E., Lamash, L., Bauminger-Zviely, N., Zancanaro, M., & Weiss, P. L. T. (2016). Using multitouch collaboration technology to enhance social interaction of children with high-functioning autism. Physical & Occupational Therapy in Pediatrics, 36(1), 46–58. https://doi.org/10.3109/01942638.2015.1040572
Gentry, T., Wallace, J., Kvarfordt, C., & Lynch, K. B. (2010). Personal digital assistants as cognitive aids for high school students with autism: Results of a community-based trial. Journal of Vocational Rehabilitation, 32(2), 101–107. https://doi.org/10.3233/JVR-2010-0499
Hatfield, M., Falkmer, M., Falkmer, T., & Ciccarelli, M. (2017). Effectiveness of the BOOST-ATM online transition planning program for adolescents on the autism spectrum: A quasi-randomized controlled trial. Child and Adolescent Psychiatry and Mental Health, 11, 54. https://doi.org/10.1186/s13034-017-0191-2
Henning, B., Cordier, R., Wilkes-Gillan, S., & Falkmer, T. (2016). A pilot play-based intervention to improve the social play interactions of children with autism spectrum disorder and their typically developing playmates. Australian Occupational Therapy Journal, 63(4), 223–232. https://doi.org/10.1111/1440-1630.12285
Higgins, J., & Thomas, J. (2021). Cochrane handbook for systematic reviews of interventions. https://training.cochrane.org/handbook/current
Hochhauser, M., Weiss, P. L., & Gal, E. (2018). Enhancing conflict negotiation strategies of adolescents with autism spectrum disorder using video modeling. Assistive Technology: The Official Journal of RESNA, 30(3), 107–118. https://doi.org/10.1080/10400435.2016.1268217
Hollis, C., Falconer, C. J., Martin, J. L., Whittington, C., Stockton, S., Glazebrook, C., & Davies, E. B. (2017). Annual Research Review: Digital health interventions for children and young people with mental health problems—a systematic and meta-review. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 58(4), 474–503. https://doi.org/10.1111/jcpp.12663
Huang, J., Du, C., Liu, J., & Tan, G. (2020). Meta-analysis on intervention effects of physical activities on children and adolescents with autism. International Journal of Environmental Research and Public Health, 17(6), 1950. https://doi.org/10.3390/ijerph17061950
Ikuta, N., Iwanaga, R., Tokunaga, A., Nakane, H., Tanaka, K., & Tanaka, G. (2016). Effectiveness of earmuffs and noise-cancelling headphones for coping with hyper-reactivity to auditory stimuli in children with autism spectrum disorder: A preliminary study. Hong Kong Journal of Occupational Therapy: HKJOT, 28(1), 24–32. https://doi.org/10.1016/j.hkjot.2016.09.001
Instituto Nacional de Estadística. (2021). Encuesta sobre Equipamiento y Uso de Tecnologías de Información y Comunicación en los Hogares. Retrieved from https://www.ine.es/dynt3/inebase/es/index.htm?padre=6899&capsel=6902.
Janeslätt, G., Kottorp, A., & Granlund, M. (2014). Evaluating intervention using time aids in children with disabilities. Scandinavian Journal of Occupational Therapy, 21(3), 181–190. https://doi.org/10.3109/11038128.2013.870225
Josman, N., Ben-Chaim, H. M., Friedrich, S., & Weiss, P. L. (2008). Effectiveness of virtual reality for teaching street-crossing skills to children and adolescents with autism. International Journal on Disability and Human Development, 7(1), 49–56. https://doi.org/10.1515/IJDHD.2008.7.1.49
Kuhaneck, H., Spitzer, S. L., & Bodison, S. C. (2020). A systematic review of interventions to improve the occupation of play in children with autism. OTJR: Occupation, Participation and Health, 40(2), 83–98. https://doi.org/10.1177/1539449219880531
Kumazaki, H., Muramatsu, T., Yoshikawa, Y., Matsumoto, Y., Ishiguro, H., Kikuchi, M., et al. (2020). Optimal robot for intervention for individuals with autism spectrum disorders. Psychiatry and Clinical Neurosciences, 74(11), 581–586. https://doi.org/10.1111/pcn.13132
Lai, M.-C., Lombardo, M. V., & Baron-Cohen, S. (2014). Autism. The Lancet, 383(9920), 896–910. https://doi.org/10.1016/S0140-6736(13)61539-1
Lamash, L., & Josman, N. (2020). Full-information factor analysis of the daily routine and autonomy (DRA) questionnaire among adolescents with autism spectrum disorder. Journal of Adolescence, 79, 221–231. https://doi.org/10.1016/j.adolescence.2020.01.011
Lamash, L., & Josman, N. (2021). A metacognitive intervention model to promote independence among individuals with autism spectrum disorder: Implementation on a shopping task in the community. Neuropsychological Rehabilitation, 31(2), 189–210. https://doi.org/10.1080/09602011.2019.1682621
Larsson-Lund, M., & Nyman, A. (2017). Participation and occupation in occupational therapy models of practice: A discussion of possibilities and challenges. Scandinavian Journal of Occupational Therapy, 24(6), 393–397. https://doi.org/10.1080/11038128.2016.1267257
Larsson-Lund, M., & Nyman, A. (2019). Occupational challenges in a digital society: A discussion inspiring occupational therapy to cross thresholds and embrace possibilities. Scandinavian Journal of Occupational Therapy. https://doi.org/10.1080/11038128.2018.1523457
Lee, S. C., Grey, C., Gurfinkel, M., Leb, O., Stern, V., & Sytner, G. (2013). The effect of computer-based intervention on enhancing visual perception of preschool children with autism: A single-subject design study. Journal of Occupational Therapy, Schools, & Early Intervention, 6(1), 31–43. https://doi.org/10.1080/19411243.2013.776425
Lee, I.-J., Chen, C.-H., & Lin, L.-Y. (2016). Applied cliplets-based half-dynamic videos as intervention learning materials to attract the attention of adolescents with autism spectrum disorder to improve their perceptions and judgments of the facial expressions and emotions of others. Springerplus, 5(1), 1211. https://doi.org/10.1186/s40064-016-2884-z
Levac, D., Colquhoun, H., & O’Brien, K. K. (2010). Scoping studies: Advancing the methodology. Implementation Science, 5(1), 69. https://doi.org/10.1186/1748-5908-5-69
Lindsay, S., Hounsell, K. G., & Cassiani, C. (2017). A scoping review of the role of LEGO® therapy for improving inclusion and social skills among children and youth with autism. Disability and Health Journal, 10(2), 173–182. https://doi.org/10.1016/j.dhjo.2016.10.010
Lo, J.-L., Chi, P., Chu, H.-H., Wang, H.-Y., & Chou, S.-C.T. (2009). Pervasive computing in play-based occupational therapy for children. IEEE Pervasive Computing, 8(3), 66–73. https://doi.org/10.1109/MPRV.2009.52
Lorah, E. R., Parnell, A., & Speight, D. R. (2014). Acquisition of sentence frame discrimination using the iPadTM as a speech generating device in young children with developmental disabilities. Research in Autism Spectrum Disorders, 8(12), 1734–1740. https://doi.org/10.1016/j.rasd.2014.09.004
Lorido, M. P. (2005). Nuevas tecnologías y educación. Cadernos De Psicopedagogia, 5(9).
Málaga, I., Blanco Lago, R., Hedrera-Fernández, A., Álvarez-Álvarez, N., Oreña-Ansonera, V. A., & Baeza-Velasco, M. (2019). Prevalencia de los trastornos del espectro autista en niños en Estados Unidos, Europa y España: Coincidencias y discrepancias. Medicina (b.aires), 79, 4–9.
Meister, C., & Salls, J. (2015). Video modeling for teaching daily living skills to children with autism spectrum disorder: A pilot study. Journal of Occupational Therapy, Schools & Early Intervention, 8(4), 307–318. https://doi.org/10.1080/19411243.2015.1107005
Moore, M., & Calvert, S. (2000). Brief report: Vocabulary acquisition for children with autism: Teacher or computer instruction. Journal of Autism and Developmental Disorders, 30(4), 359–362. https://doi.org/10.1023/a:1005535602064
Muñoz, A. I. M., & Noriega, M. A. (2016). Revisión de la práctica profesional de terapia ocupacional en autismo. Revista Electrónica De Terapia Ocupacional Galicia, TOG, 24, 14.
Odom, S. L., Thompson, J. L., Hedges, S., Boyd, B. A., Dykstra, J. R., Duda, M. A., et al. (2015). Technology-aided interventions and instruction for adolescents with autism spectrum disorder. Journal of Autism and Developmental Disorders, 45(12), 3805–3819. https://doi.org/10.1007/s10803-014-2320-6
Page, M., Cumpston, M., Chandler, J., & Lasserson, T. (2021). Chapter III: Reporting the review. In J. P. T. Higgins, J. Thomas, J. Chandler, M. Cumpston, T. Li, M. J. Page, & V. A. Welch (Eds.), Cochrane handbook for systematic reviews of interventions version 6.2. Cochrane. https://training.cochrane.org/handbook/current/chapter-iii.
Palsbo, S. E., & Hood-Szivek, P. (2012). Effect of robotic-assisted three-dimensional repetitive motion to improve hand motor function and control in children with handwriting deficits: A nonrandomized phase 2 device trial. The American Journal of Occupational Therapy: Official Publication of the American Occupational Therapy Association, 66(6), 682–690. https://doi.org/10.5014/ajot.2012.004556
Pandina, G. (2021). The role of digital medicine in autism spectrum disorder. European Neuropsychopharmacology: The Journal of the European College of Neuropsychopharmacology, 48, 42–44. https://doi.org/10.1016/j.euroneuro.2021.02.016
Parsons, D., Cordier, R., Lee, H., Falkmer, T., & Vaz, S. (2019). A randomised controlled trial of an information communication technology delivered intervention for children with autism spectrum disorder living in regional Australia. Journal of Autism and Developmental Disorders, 49(2), 569–581. https://doi.org/10.1007/s10803-018-3734-3
Peters, M. D. J., Marnie, C., Tricco, A. C., Pollock, D., Munn, Z., Alexander, L., et al. (2020). Updated methodological guidance for the conduct of scoping reviews. JBI Evidence Synthesis, 18(10), 2119–2126. https://doi.org/10.11124/jbies-20-00167
Pop, C., Simut, R., Pintea, S., Saldien, J., Rusu, A., Vanderfaeillie, J., et al. (2013). Social robots vs. computer display: Does the way social stories are delivered make a difference for their effectiveness on ASD children? Journal of Educational Computing Research, 49(3), 381–401. https://doi.org/10.2190/EC.49.3.f
Ramdoss, S., Lang, R., Mulloy, A., Franco, J., O’Reilly, M. F., Didden, R., & Lancioni, G. (2011). Use of computer-based interventions to teach communication skills to children with autism spectrum disorders: A systematic review. Journal of Behavioral Education, 20(1), 55–76. https://doi.org/10.1007/s10864-010-9112-7
Rodger, S., & Umaibalan, V. (2011). The routines and rituals of families of typically developing children compared with families of children with autism spectrum disorder: An exploratory study. British Journal of Occupational Therapy, 74(1), 20–27.
Sánchez-Raya, M. A., Martínez-Gual, E., Moriana Elvira, J. A., Luque Salas, B., & Alós Cívico, F. J. (2015). La atención temprana en los trastornos del espectro autista (TEA). Educational Psychology, 21(1), 55–63. https://doi.org/10.1016/j.pse.2014.04.001
Sandgreen, H., Frederiksen, L. H., & Bilenberg, N. (2020). Digital interventions for autism spectrum disorder: A meta-analysis. Journal of Autism and Developmental Disorders. https://doi.org/10.1007/s10803-020-04778-9
Schadenberg, B. R., Reidsma, D., Heylen, D. K. J., & Evers, V. (2020). Differences in spontaneous interactions of autistic children in an interaction with an adult and humanoid robot. Frontiers in Robotics and AI, 7, 28. https://doi.org/10.3389/frobt.2020.00028
Shattuck, P. T., Orsmond, G. I., Wagner, M., & Cooper, B. P. (2011). Participation in social activities among adolescents with an autism spectrum disorder. PLoS ONE, 6(11), e27176. https://doi.org/10.1371/journal.pone.0027176
Shic, F., & Goodwin, M. (2015). Introduction to technologies in the daily lives of individuals with autism. Journal of Autism and Developmental Disorders, 45(12), 3773–3776. https://doi.org/10.1007/s10803-015-2640-1
Strubbia, C., Levack, W., Grainger, R., Takahashi, K., & Kounosuke, T. (2020). Use of technology in supporting goal setting in rehabilitation for adults: A scoping review. British Medical Journal Open. https://doi.org/10.1136/bmjopen-2020-041730
Tanner, K., Hand, B. N., O’Toole, G., & Lane, A. E. (2015). Effectiveness of interventions to improve social participation, play, leisure, and restricted and repetitive behaviors in people with autism spectrum disorder: A systematic review. The American Journal of Occupational Therapy: Official Publication of the American Occupational Therapy Association. https://doi.org/10.5014/ajot.2015.017806
Taylor, J. L., Adams, R. E., & Bishop, S. L. (2017). Social participation and its relation to internalizing symptoms among youth with autism spectrum disorder as they transition from high school. Autism Research: Official Journal of the International Society for Autism Research, 10(4), 663–672. https://doi.org/10.1002/aur.1709
Tomchek, S., Koenig, K. P., Arbesman, M., & Lieberman, D. (2017). Occupational therapy interventions for adolescents with autism spectrum disorder. The American Journal of Occupational Therapy: Official Publication of the American Occupational Therapy Association, 71(1), 7101395010p1-7101395010p3. https://doi.org/10.5014/ajot.2017.711003
Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K., Colquhoun, H., Kastner, M., et al. (2016). A scoping review on the conduct and reporting of scoping reviews. BMC Medical Research Methodology, 16, 15. https://doi.org/10.1186/s12874-016-0116-4
Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K. K., Colquhoun, H., Levac, D., et al. (2018). PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Annals of Internal Medicine, 169(7), 467–473. https://doi.org/10.7326/M18-0850
Valencia, K., Rusu, C., Quiñones, D., & Jamet, E. (2019). The impact of technology on people with autism spectrum disorder: A systematic literature review. Sensors (basel, Switzerland), 19(20), E4485. https://doi.org/10.3390/s19204485
Vidal-España, F., Leiva-Fernández, F., Prados-Torres, J. D., Perea-Milla, E., Gallo-García, C., & Irastorza-Aldasoro, A. (2007). Identificación de tecnologías nuevas y emergentes. Atención Primaria, 39(12), 641–646. https://doi.org/10.1157/13113954
Wainer, A. L., & Ingersoll, B. R. (2011). The use of innovative computer technology for teaching social communication to individuals with autism spectrum disorders. Research in Autism Spectrum Disorders, 5(1), 96–107. https://doi.org/10.1016/j.rasd.2010.08.002
Weaver, L. L. (2015). Effectiveness of work, activities of daily living, education, and sleep interventions for people with autism spectrum disorder: A systematic review. The American Journal of Occupational Therapy Official Publication of the American Occupational Therapy Association, 69(5), 6905180020p1-6905180020p11. https://doi.org/10.5014/ajot.2015.017962
WHO. (2001). International classification of functioning, disability and health (ICF). Retrieved December 13, 2021 from https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health.
World Health Organization (WHO). (2021). Autism spectrum disorders. Retrieved July 1, 2021 from https://www.who.int/news-room/fact-sheets/detail/autism-spectrum-disorders.
Wuang, Y.-P., Wang, C.-C., Huang, M.-H., & Su, C.-Y. (2010). The effectiveness of simulated developmental horse-riding program in children with autism. Adapted Physical Activity Quarterly: APAQ, 27(2), 113–126. https://doi.org/10.1123/apaq.27.2.113
Zhang, W. X. (2002). Developmental psychology: Children and adolescence. Shandong People’s Publishing House.
Acknowledgments
We would like to acknowledge the English revision made by Jessica Gorlin.
Funding
Open Access funding provided thanks to the CRUE-CSIC agreement with Springer Nature. This study was supported by the UNIVERSIA-INDRA foundation with funding from the ANTICIPA-TEA project, coordinated by Manuela Garcia de la Hera.
Author information
Authors and Affiliations
Contributions
All authors developed the idea of this review. SDL and LMCG performed the literature search. SDL, LMCG and MGH carried out the articles screening. Before the data extraction, all authors elaborated the tables and items to include in them. SDL, LMCG and LTC performed de data extraction. All authors collaborated in the synthesis of the results and the classification of the OT interventions. The first draft of the manuscript was written by SDL and LMCG, and all authors critically commented on previous versions of the manuscript. MGH supervised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
Ethical Approval
Approval was obtained from the ethics committee of University Miguel Hernández de Elche (Code:TFM.MTO.MGDLH.SDL.201126).
Informed Consent
This article does not contain any studies with human participants or animals conducted by the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Domínguez-Lucio, S., Compañ-Gabucio, L.M., Torres-Collado, L. et al. Occupational Therapy Interventions Using New Technologies in Children and Adolescents with Autism Spectrum Disorder: A Scoping Review. J Autism Dev Disord 53, 332–358 (2023). https://doi.org/10.1007/s10803-022-05431-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-022-05431-3