
Abstract
Autism spectrum disorders (ASD) are associated with high services use, but European data on costs are scarce. Utilisation and annual costs of 385 individuals with ASD (aged 4–67 years; 18.2% females; 37.4% IQ < 85) from German outpatient clinics were assessed. Average annual costs per person were 3287 EUR, with psychiatric inpatient care (19.8%), pharmacotherapy (11.1%), and occupational therapy (11.1%) being the largest cost components. Females incurred higher costs than males (4864 EUR vs. 2936 EUR). In a regression model, female sex (Cost Ratio: 1.65), lower IQ (1.90), and Asperger syndrome (1.54) were associated with higher costs. In conclusion, ASD-related health costs are comparable to those of schizophrenia, thus underlining its public health relevance. Higher costs in females demand further research.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Autism spectrum disorder (ASD) is a pervasive neurodevelopmental disorder with a prevalence of up to 1%, which usually manifests in early childhood (Lord et al., 2020). According to the DSM-5 and ICD-11, the core symptoms of ASD are profound deficits in the domains of social interaction and communication, and restricted, repetitive, and inflexible patterns of behaviour and/or interests. About half of individuals with ASD have intellectual disability. Rates of co-occurring somatic or psychiatric disorders also are high in this population (Fortuna et al., 2016; Hossain et al., 2020; Muskens et al., 2017), leading to increased mortality (Hirvikoski et al., 2016).
As a consequence, individuals with ASD often require a broad range of support services, e.g. special education (Bürki et al., 2021), diagnostic and therapeutic health services (Jobski et al., 2017), social services (Fortuna et al., 2016; Kamp-Becker et al., 2010), and supported employment (Vogeley et al., 2013). This extensive service use yields significant societal costs: A fairly recent modelling study estimated the lifetime costs of supporting an individual with ASD without intellectual disability as US$1.4 million (United States of America (US)), and £920,000 (United Kingdom (UK)), respectively (Buescher et al., 2014).
In order to ensure appropriate planning of the afore-mentioned services and allocation of resources, it is key to have a clear understanding of the main costs associated with ASD. To date, the majority of research on ASD-related costs stems from the US: A recent review evaluated 48 relevant publications, of which more than half were from the US (Rogge & Janssen, 2019). Regarding Europe, only studies from the UK, Sweden and the Netherlands were available. For Germany, there exists only a cost-of-illness model for individuals with ASD without an intellectual disability (Bachmann et al., 2013). What most of these publications have in common is that they either present theoretical cost-of-illness models (e.g. Buescher et al. (2014)) or rely on secondary data, usually from health insurance funds, e.g. Cidav et al. (2013). Both approaches potentially affect the accuracy of the resulting findings, either through imprecision regarding the underlying estimates (in cost-of-illness models), or through uncertain validity of the coded diagnoses (in secondary data studies).
In contrast, studies on ASD-related costs based on “real-life” service use data (e.g. Barrett et al. (2015)) are scarce—to date there exist only four studies (two from the UK, one from Ireland, and one from the US), with none of these reporting data on adults with ASD.
Given the lack of real-life user data from European countries on service use and related costs in individuals with ASD—especially in adults, this study aimed to estimate health service use and associated costs in a validly diagnosed sample of German children, adolescents and adults with ASD with and without intellectual disability.
Methods
This research study was conducted within the framework of the ASD-Net, a German clinical and research network that focuses on key challenges in ASD diagnostics, therapy and health service research (Kamp-Becker et al., 2017).
Recruitment and Participants
Study data was collected in four German ASD outpatient clinics from patients with a confirmed diagnosis of a pervasive developmental disorder according to ICD-10 (F84.0, F84.1, F84.5, F84.8, and F84.9). All participants had been diagnosed by experienced clinicians using the current diagnostic gold standard in ASD, including the Autism Diagnostic Observation Schedule (ADOS), and the Autism Diagnostic Interview-Revised (ADI-R) (Bölte et al., 2006; Hayes et al., 2018; Rühl et al., 2004). Participants’ IQ had been assessed using the German versions of the following instruments: Wechsler Intelligence Scale for Children (WISC-R (Tewes, 1983), WISC-III (Tewes et al., 1999), WISC-IV (Petermann & Petermann, 2011)), Wechsler Adult Intelligence Scale (WAIS-R (Tewes, 1991), WAIS-III (von Aster et al., 2006), WAIS-IV (Petermann, 2012)), Wechsler Preschool and Primary Scale of Intelligence (WPPSI-III (Petermann et al., 2009)), Kaufman Assessment Battery for Children (Melchers & Preuß, 2009), Wortschatztest (Schmidt & Metzler, 1992), Raven’s Standard Progressive Matrices (Horn, 2009), and Raven’s Coloured Progressive Matrices (Bulheller & Häcker, 2002). While intellectual disability is defined as an IQ < 70, some studies on ASD have included “borderline intellectual functioning” (IQ = 71–84) (Baker & Blacher, 2020). Yet, according to ICD-10 (Dilling & Freyberger, 2012), an IQ between 71 and 84 is defined as a learning disability. Referring to this definition, in the current study IQ levels were dichotomised into learning disability/ intellectual disability (IQ < 85) vs. no learning disability/ intellectual disability (IQ ≥ 85).
Questionnaire and Data Collection
Sociodemographic data (including age, sex, and educational attainment) and health service utilisation was assessed through a questionnaire which included a modified version of the Client Service Receipt Inventory (CSRI). The CSRI is a well-established semi-structured interview, in which participants are asked about health services used over the preceding 12 months (Beecham & Knapp, 2001). The instrument can be administered to the service user face to face or by post for self-completion (Patel et al., 2005).
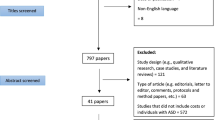
All people who had received any services in one of the four ASD clinics were invited to participate. 1419 survey documents were sent to patients with ASD or their parents/legal guardians (of these, 125 documents could not be delivered due to a wrong address). Patients and caregivers, respectively, received the questionnaire via postal mail and were asked to consent both to the study, and to the pseudonymised linkage of study data with their clinical data (e.g. clinical diagnosis, level of intellectual functioning, ADOS comparison score). Specific data on socioeconomic status and race/ethnicity was not recorded. For participants under 18 years of age, parents/legal guardians filled in the questionnaire. The questionnaire for adults with ASD was directly addressed to these. We assumed that the majority of adult participants with an IQ < 85 were assisted in filling in the questionnaire. 418 persons returned the questionnaire including a signed written consent form (response: 32.3%), of which 385 questionnaires could be evaluated. Characteristics of survey responders vs non-responders are reported in the results section.
Within the German health insurance system (Busse & Blumel, 2014), the majority of health services is largely free of charge for patients; including inpatient and outpatient health care, prescription medication, rehabilitation, non-physician practitioner services (e.g. speech therapy, occupational therapy), and—rather exceptional within Europe—psychotherapy (Signorini et al., 2017). Regarding patients with ASD, most health services (e.g. diagnostic procedures, follow-up examinations, medication, interventions for co-occurring disorders) are reimbursed by statutory health insurance funds. Nevertheless, interventions or support concerning the core symptoms of ASD are covered by integration support aid (“Eingliederungshilfe”) which is funded by social services. As these interventions are provided by different public and private institutions, comprise very diverse approaches (from facilitated communication to behavioural interventions and others), and are not part of the statutory health insurance system, we did not include them in our study.
CSRI items related to contacts with all types of healthcare professionals, and duration of all inpatient and rehabilitation treatment in the last 6 or 12 months, respectively. Outpatient drug prescriptions were assessed for the previous 4 weeks. All figures were extrapolated to a 12-month time period, under the assumption that the data were representative of the entire year.
Questionnaire data was entered by one person in an electronic Case Report Form (eCRF) created in OpenClinica® (OpenClinica Enterprise Version: 3.3), and was checked by another person.
Estimation of Service Use Costs
Based on the CSRI data, annual service use costs for inpatient and outpatient medical care were calculated, and stratified by sex, age group, diagnostic category, ADOS symptom score, intellectual functioning (IQ < 85 vs. IQ ≥ 85), and educational level. The level of education was defined in accordance with the International Standard Classification of Education (ISCED) (UNESCO, 1997, 2012), and was classified into three categories: low (ISCED level 0–2B), medium (level 2A) and high education (level 3A). Referring to the German school system, low educational level complies with 9 years of schooling or leaving school without having acquired any school-leaving qualification. Medium educational level is equivalent to 10 years of schooling, and high educational level complies with 12 or 13 years of schooling and a school-leaving qualification, which opens access to higher educational institutions (Schneider, 2008; Schroedter et al., 2011).
Direct costs were calculated by multiplying each resource use item by an appropriate unit cost (macro-costing). All costs were assessed from the perspective of the social security system and were calculated in Euros based on prices of the year 2016, obtained from a number of sources (Table S1 in Additional File 1): Where possible, medical services, including consultations of medical practitioners and non-physician practitioners (physical therapy, occupational therapy, speech therapy), as well as hospital stays and rehabilitation were valued by unit costs according to the calculation of Bock et al. (2015). Costs for outpatient hospital care as well as consultations of child and adolescent psychiatrists and psychotherapists for children were estimated by experts, using EBM-Codes (Doctors’ Fee Scale within the German Statutory Health Insurance Scheme) and/or quarterly fixed amounts. In cases of fixed amounts, a maximum of four were charged for participants who stated more than three contacts per year. For adults, the cost of medication was estimated by means of defined daily doses (DDD) using the Drug Prescription Report 2017 (Arzneiverordnungs-Report, 2017) or previous issues for example if drugs were withdrawn from the market. For children, the DDD and thereby the costs were estimated using either the Drug Prescription Report or were calculated based on the information given in the summary of product characteristics of each drug. In the latter case, the DDD were assessed based on the assumption of a twelve years old child with a weight of 41.5 kg (50th age-adjusted percentile, www.pedz.de). Finally, daily drug costs for long-time therapy drugs were multiplied by 365.25.
Data Analyses
Baseline data were analysed using descriptive statistics. Mean values and standard deviations for healthcare service use, stratified by type of service (inpatient services, other hospital-based services, outpatient services and non-physician practitioner services), were calculated separately for children (0–11 years), adolescents (12–17 years) and adults (≥ 18 years). To account for non-normality of cost data, average annual costs per individual and by type of service were estimated with 95% confidence intervals (95% CI), using the bias-corrected accelerated bootstrap method (Barker, 2005) based on 5000 replications. Additionally, in order to detect associations between potential predictors (sex, age, ASD diagnoses, intellectual functioning and ADOS comparison score) and total costs, a generalised linear model assuming a gamma distribution with a logarithmical link function was fitted to calculate cost ratios. All statistical analyses were performed with SAS, version 9.4 (SAS Institute, Cary, US). The underlying research data are available from the corresponding author upon reasonable request.
Results
The baseline characteristics of the sample are presented in Table 1. Of all 385 study participants, 81.8% were male (mean age: 21.6 years) and 18.2% were female (mean age: 23.8 years). Overall, 50.9% of participants were aged 18 years or older. 37.4% had a learning disability or intellectual disability (IQ < 85). The most frequent diagnosis was childhood autism (42.3%), followed by Asperger syndrome (39.5%). 43.9% of the participating adults with ASD, and 57.7% of parents of children and adolescents with ASD had a high level of education. Survey responders and non-responders did not differ markedly in terms of age, gender, or IQ, but differed with regard to the ASD subgroups, with a higher proportion of individuals with Asperger syndrome in the responder group (39.5% vs. 24.7%).
Health services use by age and type of service are shown in Table 2. Amongst inpatient services, psychiatric/psychosomatic care was used most frequently (4.7% of all participants), while dentists/orthodontists (65.9%), general practitioners (47.2%) and paediatricians (31.3%) were the most frequently consulted outpatient services. Amongst non-physician practitioner services, occupational therapy (22.8%) was the leading treatment modality.
The average annual costs for health services per individual are displayed in Table 3. The average annual cost per individual with ASD was 3287 (95% CI 2.81–4.14) EUR. Service use distinctly differed by sex, with females incurring higher costs than males (4864 EUR vs. 2936 EUR).
Costs for children with ASD (4177 EUR) were higher than for adults (3466 EUR) or adolescents (2510 EUR). Patients with an IQ < 85 yielded higher costs than those with an IQ ≥ 85 (4475 EUR vs. 2484 EUR). Costs did not differ very much by diagnosis, with costs for individuals with Asperger syndrome being only marginally higher. Higher ADOS comparison scores were not associated with higher costs.
The different cost components are shown in Table 4, with inpatient psychiatric care (19.8% of total cost), pharmacotherapy (11.1%), and occupational therapy (11.1%) being the largest components.
In the regression model, female sex (Cost Ratio (CR): 1.64), lower IQ (CR: 1.90), and Asperger syndrome (CR: 1.54) were significantly associated with higher costs (Table 5).
Discussion
The main results of this study are as follows:
-
(1)
When roughly comparing our findings to the few existing studies from Europe (Barrett et al., 2012, 2015; Roddy & O'Neill, 2019), and from the US (Lavelle et al., 2014), disregarding differences in study design, the ASD-related health costs found in this study are approximately in the medium range.
-
(2)
Regarding cost components, inpatient treatment had the largest share. Surprisingly, occupational therapy was a significant cost driver in children.
-
(3)
In terms of cost predictors, female sex was significantly associated with higher health costs, while ASD symptom severity was not.
Health Costs
The number of existing questionnaire-based studies on health costs in individuals with ASD is very scarce, Table 6 provides an overview of the four relevant studies. As comparability with older studies may be hampered by differing diagnostic criteria (e.g. ICD-9 vs. ICD-10), divergent therapeutic guidelines, different reimbursement policies, or limited availability of autism-specific health services, the table contains only studies from the last ten years. The study of Xiong et al. (2011), while matching the general comparability criteria, was excluded because not enough details for reasonable comparison were reported.
When comparing the cost figures from Table 6, it has to be kept in mind that there are considerable differences between the health systems of the respective countries. For example, while in Germany psychotherapy both for children and adults is broadly available and reimbursed by statutory health insurance funds, in the UK psychological therapies are less accessible (NHS England, 2018), with patients often paying out-of-pocket for private therapists. Also, the mental health system in the UK is designed with a much stronger focus on outpatient and/ or day-care treatment; in contrast to Germany, which is top of the table in Europe in terms of inpatient beds per 100,000 inhabitants (Signorini et al., 2017).
Moreover, study designs differ in terms of sample size, age range, diagnostic quality, included diagnostic categories, and cost composition.
In the study of Barrett et al. (2012), costs for healthcare, medication, and community social and voluntary services in UK toddlers with ASD were £1383/6 months, which is very close to our findings. As their sample only included 2- to 5-year old children, who usually do not use health services extensively, the similarity in cost sizes is probably due to substantial costs for nursery placement for most children in the Barrett et al. study.
In contrast, in the study of Barrett et al. (2015), costs (£500/6 months) were much lower than in our current study. This is somewhat surprising, as participants were on average 15.7 years old—an age, in which patients with ASD usually show a number of co-occurring conditions which need therapy. While costs for hospital services are roughly comparable to our findings, costs for outpatient (“community”) services are much lower than in our study, which may indicate a lower availability of these services in the UK health system.
In relation to the results of Roddy and O’Neill (2019) from Ireland, our cost figures are more than 2.4-fold higher, which may be due to the stronger focus on cheaper outpatient services within the Irish health system, and the restricted access to medical resources in this country (Thomas et al., 2014).
Finally, the “true” costs for children with ASD in the study by Lavelle et al. (2014) are most likely higher than our data, as their study only reported the additional costs for children with ASD in the US, i.e. the difference to health costs for children without an ASD diagnosis. In their sample, patients with an ASD diagnosis had significantly more outpatient visits, home healthcare visits, and prescription medication.
Remarkably, the average individual costs found in our questionnaire-based study come very close to the data from a cost-of-illness model for individuals from Germany with ASD and an IQ > 70 (0–18 years: 2473–3252 EUR, > 18 years: 3664 EUR) (Bachmann et al., 2013).
Cost Components
In our study, costs for inpatient services were the largest cost component (over all age groups: 19.8% of total cost), accounting for 36.0% of total costs in adults with ASD. At least for psychiatric healthcare services in children with ASD, the preponderance of inpatient service cost has also been shown by other researchers (Croteau et al., 2019). The afore-mentioned cost structure is similar to the health cost distribution in schizophrenia, where inpatient costs also are the greatest component of health service costs in most countries (Kovács et al., 2020), including Germany (Konnopka et al., 2009). Yet, unlike in schizophrenia, inpatient costs in ASD are potentially mainly driven by the treatment of co-occurring psychiatric conditions. The rather comparable dimension of inpatient treatment costs in ASD and schizophrenia stands in contrast to the differences of these conditions in terms of stigma (much lower in ASD) and quality of life (much higher in ASD) levels (Bachmann et al., 2019; Kamp-Becker et al., 2010). In opposition to this, the composition of health costs for individuals with ADHD shows a higher share of outpatient costs compared to inpatient costs (Daley et al., 2020).
The fact that the overall cost shares of pharmacotherapy (11.1%) and occupational therapy (11.1%) are similar is somewhat surprising, given the shaky evidence for occupational therapy for ASD-related symptoms (usually sensory features) (Watling & Hauer, 2015). Even more surprising is the proportion of occupational therapy in children, namely 26.0%, despite this treatment modality not being recommended in this age group for the treatment of ASD core symptoms (Freitag et al., 2020; National Institute for Health & Care Excellence, 2013). Given the high popularity of occupational therapy in Germany also for other neurodevelopmental disorders in children and adolescents, e.g. ADHD (Braun et al., 2013), our findings seem to be a German peculiarity, which probably reflects the good availability of these services (in contrast to e.g. early intensive behavioural interventions) and prescribers’ lacking knowledge of evidence-based interventions for ASD. Nevertheless, in our opinion, occupational therapy constitutes a rather unfounded cost driver (Haverkamp et al., 2017).
Cost Predictors
In this study, lower IQ, female sex, and Asperger syndrome were associated with higher health costs in individuals with ASD, while age or symptom severity (as indicated by the ADOS comparison score) were not. Regarding the association of lower IQ with higher costs, this result is in line with previous studies. The study of Buescher et al. (2014), for example, reported 1.6- to 1.7-fold greater lifetime costs for individuals with an ASD and intellectual disability (ID) vs. individuals with an ASD and no ID, which fits well with the cost ratio of 1.9 from our study.
The association of female sex with higher ASD health costs is a novel finding. One possible explanation are statistical effects—often, ASD studies suffer from low numbers of females (Reinders et al., 2019), therefore some gender-related effects may be difficult to detect. Another potential cause is higher psychiatric comorbidity in females with ASD, which may lead to higher healthcare costs through higher hospitalisation rates: In a German sample of adults with ASD, females had higher comorbidity rates (42%; vs. 30% in males) (Strunz et al., 2014). For children and adolescents, a Swedish study yielded similar results regarding symptom severity for comorbid ADHD, learning disabilities, and oppositional defiant disorder (Lundström et al., 2019). Yet, the existing literature regarding psychiatric comorbidity rates is not unequivocal: In a Swedish study of adults with ASD and normal intelligence (including a high portion of pervasive developmental disorder not otherwise specified), no difference between men and women in terms of lifetime psychiatric axis I diagnoses were found (Hofvander et al., 2009). Finally, the higher costs for females with ASD may be partly due to lengthy and cost-intensive diagnostic procedures, because making a correct diagnosis of ASD in females can be more complex and challenging than in males (Lundström et al., 2019; Ratto et al., 2018; Young et al., 2018). Of course, our finding needs to be replicated in a well-composed and reasonably sized sample of individuals with ASD.
The association of Asperger syndrome with higher costs is novel, too. A possible explanation for this finding is that mental health needs of other individuals with ASD, e.g. those with childhood autism and intellectual disability may be overlooked or misdiagnosed (example: signs of depression being interpreted by carers as ‘difficult behaviour’), thus leading to lower service use.
Interestingly, in our study age was not associated with costs. This stands in clear contrast to other studies which reported higher costs in older individuals (Barrett et al., 2015; Rogge & Janssen, 2019). A possible explanation are the high costs for occupational therapy and speech therapy for children in our sample. Finally, the lacking influence of ASD symptom severity (as reflected by the ADOS comparison score) is fully in line with the available literature so far (Barrett et al., 2012, 2015; Roddy & O'Neill, 2019).
Strengths and Limitations
This study constitutes the first survey-based health cost study in adults with ASD, and is one of the few international studies that are based on real-world service use data. Moreover, the sample included a broad age range (spanning 4–67 years), and a significant proportion of females. To ensure high quality diagnoses, the diagnostic assessment of participants employed the current gold standard; which is key given the significant rates of over- and misdiagnoses in ASD (Bachmann et al., 2018).
A clear limitation of this study is the sample composition: This study is not a population-based study, but a survey of patients of four large German ASD outpatient clinics. While the patient population of these clinics is representative for a typical clinical population of individuals with ASD in Germany in terms of geography (the patients seen in the four study centres stem from all German federal states, with the exception of Mecklenburg-Vorpommern), age, male/female ratio, IQ, and level of ASD symptom severity), it only contains those service users with a formal ASD diagnosis.
Moreover, the above-average portion of individuals with Asperger syndrome in our sample may have led to a bias in health costs distribution.
Another limitation is the lack of information on co-occurring health conditions, on adaptive functioning (Szatmari et al., 2015), and on participants’ socio-economic status, which probably are important service use (Drahota et al., 2020) and cost predictors in addition to the predictors studied in this work. Also, as the CSRI time frame included service use in the previous 12 months, a recall bias is possible.
While health costs are an important cost component in ASD-related (especially regarding the potentially higher morbidity and mortality), other cost types, e.g. educational costs, can be more important cost drivers in ASD-related societal costs (Bachmann et al., 2013; Rogge & Janssen, 2019). Finally, due to differences in health systems between countries, generalisability of our results is limited.
Conclusion
Compared to the few existing studies, the ASD-related health costs found in this study are in the medium range. The level of ASD-related health costs was comparable to those of individuals with schizophrenia, thus underlining the public health relevance of ASD. The considerable share of occupational therapy costs is surprising, given the lacking evidence for the effectiveness of this method in the treatment of ASD-related symptoms. The findings regarding higher ASD health costs in females are novel and require replication.
Data availability
All data generated or analysed during this study are included in this published article.
References
Bachmann, C., Buescher, A., & Knapp, M. (2013). Autism costs in Germany: Scarce data. Retrieved from, https://blogs.lse.ac.uk/healthandsocialcare/2013/10/08/autism-costs-in-germany-scarce-data/
Bachmann, C., Gerste, B., & Hoffmann, F. (2018). Diagnoses of autism spectrum disorders in Germany: Time trends in administrative prevalence and diagnostic stability. Autism, 22(3), 283–290.
Bachmann, C., Höfer, J., Kamp-Becker, I., Küpper, C., Roessner, V., Poustka, L., Roepke, S., Roessner, V., Stroth, S., Wolff, N., & Hoffmann, F. (2019). Internalised stigma in adults with autism: A German multi-center survey. Psychiatry Research, 276, 94–99.
Baker, B. L., & Blacher, J. (2020). Brief report: Behavior disorders and social skills in adolescents with autism spectrum disorder: Does IQ matter? Journal of Autism and Developmental Disorders, 50(6), 2226–2233.
Barker, N. (2005). A practical introduction to the bootstrap using the SAS system. Oxford University Press.
Barrett, B., Byford, S., Sharac, J., Hudry, K., Leadbitter, K., Temple, K., Aldred, C., Slonims, V., & Green, J. (2012). Service and wider societal costs of very young children with autism in the UK. Journal of Autism and Developmental Disorders, 42(5), 797–804.
Barrett, B., Mosweu, I., Jones, C. R., Charman, T., Baird, G., Simonoff, E., Pickles, A., Happé, F., & Byford, S. (2015). Comparing service use and costs among adolescents with autism spectrum disorders, special needs and typical development. Autism, 19(5), 562–569.
Beecham, J., & Knapp, M. (2001). Costing psychiatric interventions. In G. Thornicroft (Ed.), Measuring mental health needs (2nd ed., pp. 200–224). Gaskell.
Bock, J. O., Brettschneider, C., Seidl, H., Bowles, D., Holle, R., Greiner, W., & König, H. H. (2015). Calculation of standardised unit costs from a societal perspective for health economic evaluation. Gesundheitswesen, 77(1), 53–61.
Bölte, S., Rühl, D., Schmötzer, G., & Poustka, F. (2006). ADI-R. Diagnostisches Interview für Autismus-Revidiert. Hans Huber.
Braun, S., Zeidler, J., Linder, R., Engel, S., Verheyen, F., & Greiner, W. (2013). Treatment costs of attention deficit hyperactivity disorder in Germany. European Journal of Health Economics, 14(6), 939–945.
Buescher, A. V., Cidav, Z., Knapp, M., & Mandell, D. S. (2014). Costs of autism spectrum disorders in the United Kingdom and the United States. JAMA Pediatrics, 168(8), 721–728.
Bulheller, S., & Häcker, H. O. (2002). Coloured Progressive Matrices (CPM). (Deutsche Bearbeitung und Normierung nach J. C. Raven.). Pearson Assessment.
Bürki, L., Höfer, J., Kamp-Becker, I., Poustka, L., Roessner, V., Stroth, S.,... Bachmann, C. (2021). Special educational support in children and adolescents with autism spectrum disorder in Germany: Results from a parents’ survey. Research in Developmental Disabilities, 112, 103931. https://doi.org/10.1016/j.ridd.2021.103931.
Busse, R., & Blumel, M. (2014). Germany: Health system review. Health Systems in Transition, 16(2), 1–296.
Cidav, Z., Lawer, L., Marcus, S. C., & Mandell, D. S. (2013). Age-related variation in health service use and associated expenditures among children with autism. Journal of Autism and Developmental Disorders, 43(4), 924–931.
Croteau, C., Mottron, L., Dorais, M., Tarride, J.-E., & Perreault, S. (2019). Use, costs, and predictors of psychiatric healthcare services following an autism spectrum diagnosis: Population-based cohort study. Autism, 23(8), 2020–2030.
Daley, D., Jacobsen, R. H., Lange, A. M., Sørensen, A., & Walldorf, J. (2020). The economic burden of adult attention deficit hyperactivity disorder: A sibling comparison cost analysis. European Psychiatry, 61, 41–48.
Dilling, H., & Freyberger, H. J. (2012). Taschenführer zur ICD-10-Klassifikation psychischer Störungen. Huber.
Drahota, A., Sadler, R., Hippensteel, C., Ingersoll, B., & Bishop, L. (2020). Service deserts and service oases: Utilizing geographic information systems to evaluate service availability for individuals with autism spectrum disorder. Autism. https://doi.org/10.1177/1362361320931265
Fortuna, R. J., Robinson, L., Smith, T. H., Meccarello, J., Bullen, B., Nobis, K., & Davidson, P. W. (2016). Health conditions and functional status in adults with autism: A cross-sectional evaluation. Journal of General Internal Medicine, 31(1), 77–84.
Freitag, C. M., Jensen, K., Teufel, K., Luh, M., Todorova, A., Lalk, C., & Vllasaliu, L. (2020). Empirically based developmental and behavioral intervention programs targeting the core symptoms and language development in toddlers and preschool children with autism spectrum disorder. Zeitschrift für Kinder- und Jugendpsychiatrie und Psychotherapie, 48(3), 224–243.
Haverkamp, M. H., Cauterman, M., & Westert, G. P. (2017). Choosing Wisely should bring the cost of unnecessary care back into the discussion. BMJ Quality & Safety, 26(9), 775–776.
Hayes, J., Ford, T., Rafeeque, H., & Russell, G. (2018). Clinical practice guidelines for diagnosis of autism spectrum disorder in adults and children in the UK: A narrative review. BMC Psychiatry, 18(1), 222.
Hirvikoski, T., Mittendorfer-Rutz, E., Boman, M., Larsson, H., Lichtenstein, P., & Bölte, S. (2016). Premature mortality in autism spectrum disorder. British Journal of Psychiatry, 208(3), 232–238.
Hofvander, B., Delorme, R., Chaste, P., Nyden, A., Wentz, E., Stahlberg, O., Herbrecht, E., Stopin, A., Anckarsäter, H., Gillberg, C., Råstam, M., & Leboyer, M. (2009). Psychiatric and psychosocial problems in adults with normal-intelligence autism spectrum disorders. BMC Psychiatry, 9, 35.
Horn, R. (2009). Standard progressive matrices (SPM). (Deutsche Bearbeitung und Normierung nach J. C. Raven.) (Vol. 2). Pearson Assessment.
Hossain, M. M., Khan, N., Sultana, A., Ma, P., McKyer, E. L. J., Ahmed, H. U., & Purohit, N. (2020). Prevalence of comorbid psychiatric disorders among people with autism spectrum disorder: An umbrella review of systematic reviews and meta-analyses. Psychiatry Research, 287, 112922.
Jobski, K., Höfer, J., Hoffmann, F., & Bachmann, C. (2017). Use of psychotropic drugs in patients with autism spectrum disorders: A systematic review. Acta Psychiatrica Scandinavica, 135(1), 8–28.
Kamp-Becker, I., Poustka, L., Bachmann, C., Ehrlich, S., Hoffmann, F., Kanske, P., Kirsch, P., Krach, S., Paulus, F. M., Rietschel, M., Roepke, S., Roessner, V., Schad-Hansjosten, T., Singer, T., Stroth, S., Witt, S., & Wermter, A. K. (2017). Study protocol of the ASD-Net, the German research consortium for the study of Autism Spectrum Disorder across the lifespan: From a better etiological understanding, through valid diagnosis, to more effective health care. BMC Psychiatry, 17(1), 206.
Kamp-Becker, I., Schröder, J., Remschmidt, H., & Bachmann, C. J. (2010). Health-related quality of life in adolescents and young adults with high functioning autism-spectrum disorder. GMS Psycho-Social Medicine, 7, 03.
Konnopka, A., Klingberg, S., Wittorf, A., & König, H.-H. (2009). Die Kosten der Schizophrenie in Deutschland: Ein systematischer Literaturüberblick. (The cost of schizophrenia in Germany: A systematic review of the literature). Psychiatrische Praxis, 36(05), 211–218.
Kovács, G., Almási, T., Millier, A., Toumi, M., Horváth, M., Kóczián, K., Götze, A., Kaló, Z., & Zemplényi, A. T. (2020). Direct healthcare cost of schizophrenia—European overview. European Psychiatry, 48(1), 79–92.
Lavelle, T. A., Weinstein, M. C., Newhouse, J. P., Munir, K., Kuhlthau, K. A., & Prosser, L. A. (2014). Economic burden of childhood autism spectrum disorders. Pediatrics, 133(3), e520-529.
Lord, C., Brugha, T. S., Charman, T., Cusack, J., Dumas, G., Frazier, T., Jones, E. J. H., Jones, R. M., Pickles, A., State, M. W., Taylor, J. L., & Veenstra-VanderWeele, J. (2020). Autism spectrum disorder. Nature Reviews Disease Primers, 6(1), 5.
Lundström, S., Mårland, C., Kuja-Halkola, R., Anckarsäter, H., Lichtenstein, P., Gillberg, C., & Nilsson, T. (2019). Assessing autism in females: The importance of a sex-specific comparison. Psychiatry Research, 282, 112566.
Melchers, P., & Preuß, U. (2009). Kaufman assessment battery for children, Deutsche version (8th ed.). Pearson Assessment.
Muskens, J. B., Velders, F. P., & Staal, W. G. (2017). Medical comorbidities in children and adolescents with autism spectrum disorders and attention deficit hyperactivity disorders: A systematic review. European Child & Adolescent Psychiatry, 26(9), 1093–1103.
National Institute for Health and Care Excellence. (2013). Autism spectrum disorder in under 19s: Support and management. Clinical guideline (CG170). Last reviewed 2016.
NHS England. (2018). Adult improving access to psychological therapies programme. Retrieved September 07, 2020, from https://www.england.nhs.uk/mental-health/adults/iapt/
Patel, A., Rendu, A., Moran, P., Leese, M., Mann, A., & Knapp, M. (2005). A comparison of two methods of collecting economic data in primary care. Family Practice, 22(3), 323–327.
Petermann, F. (2012). WAIS-IV. Deutschsprachige adaptation der WAIS-IV von David Wechsler. Pearson Assessment.
Petermann, F., & Petermann, U. (2011). Wechsler intelligence scale for children-IV (WISC-IV). Pearson Assessment.
Petermann, F., Ricken, G., Fritz, A., Schuck, K. D., & Preuß, U. (2009). Wechsler preschool and primary scale of intelligence—III—Deutsche version (3rd ed.). Pearson Assessment.
Ratto, A. B., Kenworthy, L., Yerys, B. E., Bascom, J., Wieckowski, A. T., White, S. W., Wallace, G. L., Pugliese, C., Schultz, R. T., Ollendick, T. H., Scarpa, A., Seese, S., Register-Brown, K., Martin, A., & Anthony, L. G. (2018). What about the girls? Sex-based differences in autistic traits and adaptive skills. Journal of Autism and Developmental Disorders, 48(5), 1698–1711.
Reinders, N. J., Branco, A., Wright, K., Fletcher, P. C., & Bryden, P. J. (2019). Scoping review: Physical activity and social functioning in young people with autism spectrum disorder. Frontiers in Psychology, 10, 120.
Roddy, A., & O’Neill, C. (2019). The economic costs and its predictors for childhood autism spectrum disorders in Ireland: How is the burden distributed? Autism, 23(5), 1106–1118.
Rogge, N., & Janssen, J. (2019). The economic costs of autism spectrum disorder: A literature review. Journal of Autism and Developmental Disorders, 49(7), 2873–2900.
Rühl, D., Bölte, S., Feineis-Matthews, S., & Poustka, F. (2004). ADOS. Diagnostische Beobachtungsskala für Autistische Störungen. Hans Huber.
Schmidt, K.-H., & Metzler, P. (1992). Wortschatztest (WST). Beltz.
Schneider, S. L. (2008). The international standard classification of education (ISCED-97): An evaluation of content and criterion validity for 15 European countries. MZES.
Schroedter, J. H., Lechert, Y., & Lüttinger, P. (2011). Die Umsetzung der Bildungsskala ISCED-1997 für die Volkszählung 1970, die Mikrozensus-Zusatzerhebung 1971 und die Mikrozensen 1976–2004 (Version 1) ZUMA-Methodenbericht. ZUMA.
Schwabe, U., Paffrath, D., Ludwig, W.-D., & Klauber, J. (Eds.). (2017). Arzneiverordnungs-Report 2017. Springer.
Signorini, G., Singh, S. P., Boricevic-Marsanic, V., Dieleman, G., Dodig-Ćurković, K., Franic, T., Gerritsen, S. E., Griffin, J., Maras, A., McNicholas, F., O’Hara, L., Purper-Ouakil, D., Paul, M., Santosh, P., Schulze, U., Street, C., Tremmery, S., Tuomainen, H., Verhulst, F., & de Girolamo, G. (2017). Architecture and functioning of child and adolescent mental health services: A 28-country survey in Europe. Lancet Psychiatry, 4(9), 715–724.
Strunz, S., Dziobek, I., & Roepke, S. (2014). Komorbide psychiatrische Störungen und Differenzialdiagnostik bei nicht-intelligenzgeminderten Erwachsenen mit Autismus-Spektrum-Störung [Comorbid Psychiatric Disorders and Differential Diagnosis of Patients with Autism Spectrum Disorders without Intellectual Disability] Psychotherapie, Psychosomatik, Medizinische Psychologie.
Szatmari, P., Georgiades, S., Duku, E., Bennett, T. A., Bryson, S., Fombonne, E., Mirenda, P., Roberts, W., Smith, I. M., Vaillancourt, T., Volden, J., Waddell, C., Zwaigenbaum, L., Elsabbagh, M., & Thompson, A. (2015). Developmental trajectories of symptom severity and adaptive functioning in an inception cohort of preschool children with autism spectrum disorder. JAMA Psychiatry, 72(3), 276–283.
Tewes, U. (1983). HAWIK-R. Hamburg-Wechsler-Intelligenztest für Kinder. Revision 1983. Hans Huber.
Tewes, U. (1991). Hamburg-Wechsler-Intelligenztest für Erwachsene (HAWIE-R). Hans Huber.
Tewes, U., Schallberger, P., & Rossmann, U. (1999). Hamburg-Wechsler-Intelligenztest für Kinder III (HAWIK-III). Hans Huber.
Thomas, S., Burke, S., & Barry, S. (2014). The Irish health-care system and austerity: Sharing the pain. Lancet, 383(9928), 1545–1546.
UNESCO. (1997). International standard classification of education ISCED 1997. UNESCO.
UNESCO. (2012). International Standard Classification of Education ISCED 2011. UNESCO Institute for Statistics.
Vogeley, K., Kirchner, J. C., Gawronski, A., Tebartz van Elst, L., & Dziobek, I. (2013). Toward the development of a supported employment program for individuals with high-functioning autism in Germany. European Archives of Psychiatry and Clinical Neuroscience, 263(Suppl 2), S197-203.
von Aster, M., Neubauer, A., & Horn, R. (2006). Wechsler Intelligenztest für Erwachsene WIE. Deutsche adaption des WAIS-III. Pearson Assessment.
Watling, R., & Hauer, S. (2015). Effectiveness of ayres sensory integration® and sensory-based interventions for people with autism spectrum disorder: A systematic review. American Journal of Occupational Therapy, 69(5), 1–12.
Xiong, N., Yang, L., Yu, Y., Hou, J., Li, J., Li, Y., Liu, H., Zhang, Y., & Jiao, Z. (2011). Investigation of raising burden of children with autism, physical disability and mental disability in China. Research in Developmental Disabilities, 32(1), 306–311.
Young, H., Oreve, M. J., & Speranza, M. (2018). Clinical characteristics and problems diagnosing autism spectrum disorder in girls. Archives de Pediatrie, 25(6), 399–403.
Acknowledgments
The authors would like to thank Marie Kollarczyk, Imke Garten, Gerti Gerber, Friederike Helbig and Miriam-Sophie Petasch for their assistance in the conduct of this research, and the families and individuals for participating in this study. JH, FH and CJB conceived of the study, participated in its design and coordination and drafted the manuscript; JH, FH and MD performed the statistical analysis and interpretation of the data; IKB, LP, SR, VR, SS, CK and NW participated in the coordination of the study and performed the measurements. All authors read and approved the final manuscript.
Funding
Open Access funding enabled and organized by Projekt DEAL.. This work was funded by the German Federal Ministry of Education and Research (Bundesministerium für Bildung und Forschung, FKZ 01EE1409F). The funding organisation had no influence on the design and conduct of the study, collection, management, analysis, and interpretation of the data, preparation, review, or approval of the manuscript, or the decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The study protocol was reviewed and approved by the Commission for Impact Assessment Research and Ethics, Carl von Ossietzky University Oldenburg (reference number DRs. 23/2015); and by the concerned institutional ethic committees (Heidelberg University: reference number 2015-607N-MA; Marburg University: reference number 148/15; Berlin University: reference number 941/15; Dresden University: reference number EK6012016). The data protection concept was additionally coordinated with the Data Protection Officer of the Carl von Ossietzky University, Oldenburg.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Höfer, J., Hoffmann, F., Dörks, M. et al. Health Services Use and Costs in Individuals with Autism Spectrum Disorder in Germany: Results from a Survey in ASD Outpatient Clinics. J Autism Dev Disord 52, 540–552 (2022). https://doi.org/10.1007/s10803-021-04955-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-021-04955-4