
Abstract
Facial feedback mechanisms of adolescents with Autistic Spectrum Disorders (ASD) were investigated utilizing three studies. Facial expressions, which became activated via automatic (Studies 1 and 2) or intentional (Study 2) mimicry, or via holding a pen between the teeth (Study 3), influenced corresponding emotions for controls, while individuals with ASD remained emotionally unaffected. Thus, individuals with ASD do not experience feedback from activated facial expressions as controls do. This facial feedback-impairment enhances our understanding of the social and emotional lives of individuals with ASD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Individuals with Autistic Spectrum Disorder (ASD) have qualitative impairments in social interaction and communication (American Psychiatric Association 1994); they have trouble interpreting social and emotional signals, and initiating and maintaining social relationships (Van Engeland 2000). Many studies demonstrated that social impairments in individuals with ASD rely on the ability to attend to and process information from the face (Dawson et al. 1998, 2002, 2004; Mundy et al. 1986; Sigman et al. 1992). In this article we focus on the involvement of mimicry and facial feedback processes in these impairments.
The impairments in social interactions that individuals with ASD experience, seem to resemble, in a way, the impairments people without disorders would experience when refrained from mimicking. Mimicry can be defined as ‘doing what others are doing’ copying other people. People without disorders constantly mimic each other’s postures (Bernieri 1988), mannerisms (Chartrand and Bargh 1999), facial expressions (O’Toole and Dubin 1968; Dimberg 1990), vocalizations (Kugiumutzakis 1996) and many other behaviours. Evidence for spontaneous mimicry stems from social psychological, developmental psychological and neurological research. Mimicry occurs spontaneously even when interacting with strangers (Chartrand and Bargh 1999) and may take place when the target stimuli are presented outside awareness (Dimberg et al. 2000). Mimicry has been observed in newborns as early as 42 min after birth (Meltzoff and Moore 1983, 1989), which lends support to the notion that the tendency to mimic is innate. The innate connection between observed and executed action is sustained by neurological evidence on mirror neurons (for overviews see Rizzolatti et al. 2002; Decety et al. 2002), corroborating the link between perceiving and doing already hypothesized by William James (1890). Thus, people without disorders tend to mimic others automatically and unconsciously.
This mimicry has been shown to be important in creating social bonds between people; more specifically mimicry smoothens interactions, enhances liking for each other, and creates empathy between people (Bernieri 1988; Chartrand and Bargh 1999; Stel et al. 2006). In interpersonal situations where mimicry was not present, less emotional and cognitive empathy was felt for each other, and the interaction did not proceed as smoothly than when mimicry did occur (Stel et al. 2006).
Instructed or deliberate mimicry (also termed imitation) of emotional and non-emotional expressions of individuals with ASD have been regularly studied in the past (i.e., Ozonoff et al. 1991; Rogers et al. 1996; Rogers and Pennington 1991). For instance, Loveland et al. (1994) demonstrated that individuals with ASD produced fewer recognizable facial expressions than controls when imitating a model.
However, research on mimicry behavior of individuals with ASD merely focused on the question whether they are capable of facial mimicry when instructed to do so, while spontaneous, automatic facial mimicry remained rather unexplored. Recently, McIntosh et al. (2006) investigated this and showed that individuals with ASD were impaired in automatic facial mimicry.
Although mimicry is an important mechanism for social interactions and might, in part, explain the social impairments in individuals with ASD, it remains less clear why they experience little empathy towards others (Hobson 2007; Lawson et al. 2004). Emotional responsiveness to the feelings experienced by others is normally facilitated by facial mimicry (Hatfield et al. 1992; Stel et al. 2006). Darwin (1872/1965), Izard (1977) and Tomkins (1982) have proposed that the experience of emotions is affected by feedback from the muscles that are activated in the face. This mechanism is termed facial feedback. McIntosh (1996) presented an overview of evidence that emotions are indeed modulated and initiated by activated facial muscles. For example, a study is cited of Hess et al. (1992), who demonstrated that when participants were asked only to display an emotion, subsequent changes in their subjective experience were reported.
Thus, associated emotions are re-enacted when mimicking other people’s emotional expressions (Barsalou et al. 2003). We argue that this facial feedback mechanism might work differently for individuals with ASD.
The idea that facial feedback may be different in autism was inspired by the work of Yirmiya et al. (1992), who found that children with ASD showed more neutral and less emotional expressions, and also display unique facial patterns compared to controls. This difference in displayed facial expressions might give an indication that an expression-emotion link (i.e., the relatedness and mutual influence between felt emotions and emotional expressions) is less profoundly present for individuals with ASD. If individuals with ASD have unique facial patterns and show less emotional expressions, it is possible that they may not have created a link between expressions and emotions, as individuals without disorders have. However, this has never been investigated. Of course a more processes influence people’s experience and expressions of emotions, but having a different working expression-emotion link has major implications for their own expression and experience of emotions, and for understanding emotions of others. Therefore, the present paper investigates the expression-emotion link of individuals with ASD.
In Study 1, we investigated the relationship between mimicked facial expressions and experienced emotions of individuals with ASD and controls. In our second study, amount of facial mimicry was manipulated to provide a more comprehensive test whether expressions and emotions are causally linked. Finally, in Study 3, facial feedback mechanisms were measured using Strack et al.’s methodology (1988), in which facial muscles were activated by holding a pen in their mouth.
Across studies, we expect that adolescents with ASD experience less feedback from activated emotional facial expressions (either via mimicry or via holding a pen in their mouth) compared to controls.
Study 1
In addition to our main investigation on the link between facial expressions and corresponding experienced emotions, we measured the automatic mimicry level of both groups. Because, to our knowledge, McIntosh, et al.’s study is the only study on automatic mimicry, we tested whether we could replicate their findings that adolescents with ASD show impaired automatic mimicry compared to controls. The difference between the study of McIntosh et al. and our study, is that they used facial EMG to measure facial mimicry, whereas we explored whether different overt mimicry levels are present for facial (copying facial movements) and behavioral mimicry (copying of gestures and movements of the body), and also make a distinction between individuals with autistic disorder according to the (DSM-IV) and with PDD-NOS.
Across the three studies of our paper, different participants were used. We did not include levels of language or cognitive development, because our studies concerned nonverbal processes, which are not influenced by language or cognitive abilities. These abilities might be relevant for answering our questionnaire, but all participants were able to understand the used methods, emotion words, 7-point Likert scales, and instructions as indicated by their IQ (>50), their teacher, our tryout questions, and Downs and Smiths’ study (2004), demonstrating that adolescents with ASD did not have impaired emotional understanding.
Method
Participants and Design
Participants were 8 individuals with autistic disorder, 15 with PDD-NOS, and 21 individuals who did not have any disorder (controls).Footnote 1 They participated on a voluntarily basis with permission from their parents, while the participants themselves were naive about the purpose of the study (mean age for individuals with autistic disorder: M = 14.63, SD = 0.57; PDDNOS: M = 14.67, SD = 0.43; controls: M = 15.67, SD = 0.40). Individuals with autistic disorder and PDD-NOS were sampled from special schools and controls from an ordinary high school. They were assigned on the basis of the diagnosis given by qualified diagnosticians according to DSM-IV, to the Diagnosis conditions in a 3 (Diagnosis; autistic disorder vs. PDD-NOS vs. control) × 2 (Mimicry: facial vs. behavioral) design with Mimicry as within-subjects factor. Controls were matched according to gender and chronological age as in McIntosh et al. (2006).
Procedure
The experiment was individually conducted in a classroom of the participants’school. Participants were videotaped with a hidden camera in front of them while they sat and watched a 5-min video in which a male student talked about his adventures in an amusement park, displaying happy expressions. After watching the video, participant’s experienced emotional state was measured by asking them on 12 different emotion items to indicate on a 7-point Likert scale to what extent they felt happy, sad, angry, tense, enthusiastic, pleased, worried, irritated, confused, cheerful, dreary, and nervous. These 12 Likert scale ratings were averaged to produce global positive and negative experienced emotion scores for each participant.
Results and Discussion
Mimicry
Two independent raters, who were blind for Diagnosis and goal of the study, coded the facial and behavioral movements of all participants. These were compared with the movements of the male student shown on the video (the target). When the movement of the participant matched the movement of the target and occurred after the target’s movement within a time block of 10 s, it was scored as a mimicry behavior. Facial movements included movements of eyes, eyebrows, lips, mouth, and head. Behavioral movements included scratching the face, resting their head on their hands, and any other hand gestures. The interobserver reliability, using alpha statistics, of facial and behavioral mimicry was, respectively, .86 and .78. No composite measure of facial and behavioral mimicry was used because of their low alpha, −.12.
We expressed the amount of mimicry as the proportion of mimicked movements out of all the participants’ movements, to take movement tendency into account; when one has a general tendency to move a lot, the amount of mimicry increases, but this is a side effect of overall movement and could have biased our results. This mimicry coding procedure has been used in our previous studies (e.g. Stel et al. 2006).
A 3 (Diagnosis) × 2 (Mimicry) repeated measures Analysis of Variance (ANOVA) with Mimicry as within subjects factor showed a main effect of Diagnosis, F (2, 41) = 4.76, p = .01, η2 = .18, which indicated that controls mimicked to a greater extent (M = 27.94%, SD = 14.37) than individuals with autistic disorder (M = 11.86%, SD = 9.33), F (1, 27) = 8.54, p = .01, η2 = .24 and with PDD-NOS (M = 16.91%, SD = 15.97), F (1, 34) = 4.70, p = .04, η2 = .12. There was no significant difference between individuals with autistic disorder and PDD-NOS, F < 1.Footnote 2
A main effect of Mimicry, F (1, 41) = 15.45, p < .001, η2 = .27, indicated that participants showed more behavioral (M = 33.22%, SD = 29.31) than facial mimicry (M = 9.30%, SD = 12.25). There was no differential influence of Diagnosis on this effect of Mimicry, F (2, 41) = 1.68, p = .20, η2 = .08 (see Fig. 1).

Percentage of mimicry by Mimicry and Diagnosis (Study 1). Error bars indicate standard errors
Correlation Mimicked Facial Expressions and Experienced Emotions
The emotion items were classified according to the combined factor analyses of Studies 1 and 2 into ‘positive’ (enthusiastic, pleased, happy, and cheerful, α = .80) and ‘negative’ (sad, angry, tense, worried, irritated, confused, dreary, and nervous, α = .79) emotions.
The number of individuals with autistic disorder was relatively low for correlational purposes, therefore, individuals with autistic disorder and PDD-NOS were combined. There was a significant correlation for controls between mimicked facial expressions and experienced positive emotions, r = .59, p = .01, N = 21, while the same comparison was non-significant for individuals with ASD, r = .11, p = .61, N = 23. These correlations differed significantly, z = −1.75, p = .04. Mimicked expressions and negative emotions were not correlated (resp. r control = −.28, p = .22, N = 21 vs. r ASD = −.16, p = .46, N = 23; z = .039, p = .35).
Actual attention. Actual attention for the video was additionally rated by the same coders as the coders of facial and behavioral movement. Raters scored whether and how many times participants did not look directly at the video. This actual attention for the video did not differ among the three conditions of Diagnosis, F < 1. Thus, differential attention for the video could not explain our results.
As hypothesized, individuals with ASD displayed less mimicry compared to controls. There is no difference in the impairment of individuals with ASD between facial and behavioral mimicry,Footnote 3 or between individuals with autistic disorder and PDD-NOS, indicating that the amount of ASD symptoms does not relate to the severity of the mimicry impairment.
The facial expressions that individuals with ASD did mimic was not related to their emotions, while mimicry of the targets’ positive facial expressions did relate to the positive emotional experience of controls. Though, it is possible that a certain amount of mimicry is necessary to produce effects, and that individuals with ASD did not reach this level. Therefore, in Study 2, we examine the expression-emotion link further by manipulating the amount of mimicry.
Study 2
Previous work has found mixed results concerning whether individuals with ASD are capable of intentional, instructed mimicry (e.g. Charman and Baron-Cohen 1994 vs. Rogers et al. 2003). The most recent study of instructed facial mimicry (McIntosh et al. 2006) demonstrated they could, thus we expected to replicate this. More importantly, we hypothesized that facial mimicry, either automatic or instructed, affects emotions of controls, but no causal link will be present for individuals with ASD. Because in Study 1 we did not find differentiating mimicry results for individuals with autistic disorder and PDD-NOS, we did not make this distinction in the following studies.
Method
Participants and Design
Participants were 33 individuals with ASD and 28 controls recruited and selected in the same way as in Study 1 (mean age for individuals with ASD: M = 14.19, SD = 1.70; controls: M = 13.46, SD = 2.73). They were randomly assigned to Mimicry instruction conditions in a 2 (Diagnosis: ASD vs. control) × 3 (Mimicry instructions: mimicry vs. no mimicry vs. no instruction) between-subjects design.
Procedure and Materials
The same procedure as in Study 1 was used; participants were videotaped while watching a video after which participant’s experienced emotional state was measured by 12 emotion items. However, in this study a different video of 3 min was used to measure the generalisability of the obtained effectsFootnote 4; a young woman displayed happy facial expressions while talking about meeting a friend. Additionally, participants received Mimicry instructions in which they were either asked to mimic the facial expressions of the target on the video, not to mimic, or did not receive an instruction. Our previous work has found these instructions to be very effective (e.g. Stel et al. 2006).
Results and Discussion
Mimicry
Only facial mimicry was assessed as in Study 1. The interobserver reliability was .99. A 2 (Diagnosis) × 3 (Mimicry instructions) ANOVA was conducted with mimicry as a dependent variable. A main effect for Mimicry instructions, F (2, 55) = 26.50, p < .001, η2 = .49, indicated that participants in the mimicry condition, mimicked the target more than participants in the no mimicry, F (1, 40) = 42.69, p < .001, η2 = .52 and the no instruction condition, F (1, 42) = 13.39, p = .001, η2 = .24. Participants in the no mimicry condition showed less mimicry than those in the no instruction condition, F (1, 34) = 4.89, p = .03, η2 = .13.
A main effect of Diagnosis, F (1, 55) = 4.43, p = .04, η2 = .07, indicated that controls mimicked to a greater extent than individuals with ASD. This main effect of Diagnosis was qualified by Mimicry, F (2, 55) = 6.98, p = .002, η2 = .20, indicating, as shown in Fig. 2, that individuals with ASD mimicked more in the mimicry than in the no mimicry, F (1, 22) = 11.95, p = .002, η2 = .35 and no instruction condition, F (1, 22) = 22.39, p < .001, η2 = .50, while the no instruction and no mimicry condition did not differ, F (1, 16) = 2.59, p = .13, η2 = .14. In contrast, controls showed less mimicry in the no mimicry than in the mimicry, F (1, 16) = 49.18, p < .001, η2 = .76 and the no instruction condition, F (1, 16) = 22.45, p < .001, η2 = .58, while the mimicry and no instruction condition did not differ, F (1, 18) = 2.21, p = .15, η2 = .11.

Percentage of mimicry by Mimicry instructions and Diagnosis (Study 2). Error bars indicate standard errors
Additionally, the levels of mimicry of individuals with ASD and controls differed significantly in the no instruction, F (1, 18) = 22.63, p < .001, η2 = .57, marginally in the no mimicry, F (1, 17) = 3.32, p = .08, η2 = .18 and not in the mimicry condition, F < 1.
Experienced Emotions
A 2 (Diagnosis) × 3 (Mimicry instructions) × 2 (Emotion) repeated measures ANOVA was conducted with participants’ Emotion as a within-subjects factor. A main effect of Emotion, F (1, 55) = 90.29, p < .001, η2 = .62, indicated that participants felt more positive than negative.
A Diagnosis × Mimicry instructions effect, F (2, 55) = 3.71; p = .03, η2 = .12, showed that Mimicry instructions influenced emotions of controls, F (2, 25) = 4.72; p = .02, η2 = .27, while not for individuals with ASD, F < 1. This interaction effect was qualified by Emotion, F (2, 55) = 3.55; p = .04, η2 = .11, showing that Diagnosis × Mimicry instructions affected positive, F (2, 55) = 5.59; p = .01, η2 = .17, but not negative emotions, F < 1. For controls, Mimicry affected positive emotions, F (2, 25) = 4.91; p = .02, η2 = .28; they reported less positive emotions when they did not mimic the happy expressions of the target than when they did, F (1, 16) = 5.79, p = .03, η2 = .27 or than in the no instruction condition, F (1, 16) = 7.53, p = .01, η2 = .32. The difference between the mimicry and no instruction condition was not significant, F < 1. For individuals with ASD, however, Mimicry instructions did not affect positive emotions, F (2, 30) = 1.38; p = .27, η2 = .08 (see Fig. 3).

Experienced emotions by Mimicry instructions and Diagnosis (Study 2), 1 = totally not, 7 = very strong. Error bars indicate standard errors
Mimicry Mediation
Though the Mimicry instructions succeeded other variables than actual mimicry may have caused these effects. To examine whether actual mimicry mediates our effects, we used the regression method proposed by Baron and Kenny (1986). First, the dummy variables Diagnosis and Mimicry instructions produced a significant effect on positive emotions, B = 4.38, t = 25.80, p < .001. This effect reduced when we included actual mimicry in the regression, B = 3.99, t = 16.00, p < .001. In addition, the effect of actual mimicry on positive emotions is significant, B = .02, t = 2.10, p = .04. According to the Goodman version of the SOBEL test, this indirect effect of Diagnosis and Mimicry instructions on positive emotions via actual mimicry is significant, z = 2.04, p = .04.
Actual attention. Again, actual attention for the video was additionally rated. This actual attention for the video did not differ among the Mimicry instructions conditions, F < 1, neither among the Diagnosis conditions, F (2, 55) = 1.72; p = .20, η2 = .03, nor their interaction, F < 1. Attention for the video could not explain our results.
To conclude, we replicated the effect of Study 1, using a different video with a female target, that automatic mimicry is impaired for individuals with ASD, moreover, their automatic mimicry level did not differ from levels when asked not to mimic, while the automatic mimicry level of controls did not differ from the instructed-to-mimic condition. Individuals with ASD were capable of facial mimicry when instructed to do so; the amount of mimicry in the instructed-to-mimic conditions did not differ from controls. Though, our mimicry manipulations had differentiating effects; when controls mimicked the targets’ positive facial expressions, either automatically or intentionally, they felt more positive emotions than when they did not mimic, while the emotions of individuals with ASD remained unaffected.
Study 3
As the expression-emotion link was tested using mimicry to activate facial expressions in Studies 1 and 2, it is possible that our results were caused by something that was activated via mimicry. Therefore, in this study, we investigated this link using the facial feedback method of Strack et al. (1988).
Strack et al. showed that activation of facial muscles, by holding a pen between the teeth or lips, influenced people’s affective experiences in the presence of a stimulus. They demonstrated that cartoons were more positively evaluated when muscles associated with smiling were activated (by holding a pen between the teeth), and less positively when these muscles were inhibited (by holding a pen between the lips), compared to the control condition, in which participants held a pen in their nondominant hand.
Because individuals with ASD have difficulty in understanding cartoons (Emerich et al. 2003), we used illustrations. We expected no effect of facial muscle activation on ratings of the illustrations for individuals with ASD, while we expected more positive ratings when controls hold the pen between their teeth compared to in their nondominant hand.
Method
Participants and Design
Participants were 24 individuals with ASD and 24 controls (mean age for individuals with ASD: M = 14.75, SD = 1.57; controls: M = 15.58, SD = 1.86). They were randomly assigned to Feedback conditions in a 2 (Diagnosis: ASD vs. control) × 2 (Feedback: yes vs. no) between-subjects design.
Materials and Procedure
The experiment was run individually. Participants were either instructed to hold a marker between their teeth (feedback condition facilitating ‘smiling’ muscles) or in their non-dominant hand (no feedback condition). To strengthen our cover story that we investigated adolescent’s ability to use a pen with different body parts, participants were first asked to draw lines and squares between presented dots. Then, they indicated, with the marker between their teeth or in their non-dominant hand, how much they liked presented illustrations by underlining the corresponding number on 7-point Likert scale.
Results and Discussion
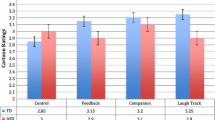
A 2 (Diagnosis) × 2 (Feedback) ANOVA was conducted with liking of the illustrations as dependent measure. A main effect of Diagnosis, F (1, 43) = 6.72, p = .01, η2 = .14, indicated that individuals with ASD generally liked the illustrations more than controls. This main effect was qualified by Feedback, F (1, 43) = 4.98, p = .03, η2 = .10, indicating that individuals with ASD were not affected by Feedback, F (1, 21) = 1.19, p = .29, η2 = .05 whereas controls were, F (1, 22) = 5.96, p = .02, η2 = .21; Controls liked the illustrations more when facial muscles were activated that are associated with feeling happy compared with the no feedback condition (see Fig. 4).

Liking for the illustrations by Feedback and Diagnosis (Study 3). Error bars indicate standard errors
To conclude, using the facial feedback manipulation of Strack et al., this study replicated the obtained effects of Studies 1 and 2 that facial expressions influenced affective reactions for controls, while adolescents with ASD remained unaffected.
General Discussion
First of all, our results showed that individuals with ASD have deficits in automatic, but not in intentional mimicry, thereby replicating the findings of McIntosh et al. (2006). Additionally, we showed that the impairment in mimicry is present for facial and behavioral mimicry, and across ASD-diagnosis (autistic disorder and PDD-NOS). Mimicry reactions are suggested to be located in a brain area serving both perception and execution of actions (e.g., Decety et al. 1994, 1997, 2002). Nishitani et al. (2004) and Oberman et al. (2005) investigated the functioning of the mirror neuron system in individuals with ASD, using respectively magnetoencephalography (MEG) and Electroencephalography (EEG). Their studies suggest that the mimicry impairment of individuals with ASD is reflected in the neurons of this brain area, the so-called mirror neurons.
More importantly, we demonstrated in three studies that, in addition to this impairment in mimicry, deficits in facial feedback play an important role in the emotional impairment of individuals with ASD; although mimicry facilitates catching other people’s emotions for controls, simply instructing individuals with ASD to mimic does not improve empathic abilities.
Across three studies, we are the first to demonstrate that facial expressions, activated via holding a pen between the teeth, or via automatic or intentional mimicry, influenced corresponding emotions for controls, while individuals with ASD remained emotionally unaffected. From this can be concluded that the facial feedback mechanism, which people without disorders experience, works differently for adolescents with ASD.
As our results showed, attention for the tasks involved could not explain our results. Neither the inability of individuals with ASD to understand the used methods, emotion words, 7-point Likert scales, and instructions could explain our effects, which was indicated by their IQ (>50), their teacher, our tryout questions, and Downs and Smiths’ study (2004), demonstrating that adolescents with ASD did not have impaired emotional understanding. Additionally, previous studies (Stel et al. 2006) showed that neither mimicry, nor the link between mimicked expressions and experienced emotions are influenced by information coming through the auditory channel.
Our results showing impairments in mimicry and experienced emotions do not simply represent the difficulty of emotion recognition that individuals with ASD experience (e.g. Gepner et al. 1994; Hobson 1989), causing the impairment. Mimicry reactions have been shown even when stimuli were presented outside awareness, and thus before participants could consciously recognize an emotion (Dimberg et al. 2000). Additionally, a study by Stel and Van Knippenberg (2002) showed that mimicry can even facilitate emotion recognition. Thus, it seems that impairments of mimicry are not caused by emotion recognition deficits of individuals with ASD, but mimicry can play a facilitating role in emotion recognition.
Our results seem to be neither easily explained by differential face processing of individuals with ASD, which is reflected in failure to attend to the eye region (Hadjikhani et al. 2004; Gross 2004). In our studies, the target expressed positive emotions by smiling. Thus the emotions were expressed in the lower regions of the face, of which individuals with ASD do pay attention to. However, eyetracking the participants should be necessary to entirely rule out this possibility.
Our results were obtained using methods inducing positive expressions, but we have no doubt that these can be generalized to negative expressions. First of all, Stel et al. (2006) and Strack et al. (1988) demonstrated that facial feedback manipulations activating negative, or inhibiting positive emotional expressions showed the same results for controls; i.e., experiencing more negative affect. Therefore, we do not expect differences for individuals with ASD. Secondly, individuals with ASD have more difficulty understanding negative emotions (Sigman et al. 1992), thus the results for negative emotions may be even more profound. But of course, this needs investigation.
According to Carruthers and Smith (1996), the theory of mind deficit, i.e., inability to attribute mental states, such as intentions, beliefs, and desires to themselves and other people and thereby to understand and predict behavior, is due to deficits in simulation. The simulation theory proposes that children come to understand others by taking perspective and using their own minds to simulate the mental processes that are likely to be operating in the other. From this research we cannot conclude whether impairments in mimicry and facial feedback are the causal factors influencing the theory of mind deficit, but we demonstrated that those deficits indeed play an important role in understanding others. From our perspective, simulation is an important way to become to understand others better; when individuals without disorders simulate emotional expressions (e.g. mimicking), one as a result become to feel as the other person, as we have shown in our studies, and facilitates perspective taking (Stel et al. 2006). As argued, recognition of emotion does not necessarily have to take place before simulation processes, but of course, this emotion recognition processes play an important role in the theory of mind deficit, and is also in part influenced by mimicry and feedback processes.
Because our studies focused on re-enacting emotions by activating facial expressions, future research should investigate the expressions of individuals with ASD that accompany their experienced emotions. This will further enhance our knowledge of whether there is no expression-emotion link at all, or there is ‘just’ no re-enactment of emotions via facial expressions.
Our findings that facial feedback works differently for adolescents with ASD compared to controls, does not necessarily imply that individuals with ASD do not experience feedback from facial muscles at all. As research of Yirmiya et al. (1992) demonstrated, children with ASD have unique facial expressions, which were not displayed by controls. Therefore, it is possible, that individuals with ASD have their own, differently working facial feedback mechanism. Though, keep in mind that the mimicked facial expressions they spontaneously displayed in Study 1 were not related to their emotions either.
Having a different working expression-emotion link or none at all, our findings unobtrusively show that individuals with ASD experience impairments in mimicry and facial feedback mechanisms. Thus, individuals with ASD lack a strong connection not only between observed and mimicked emotions, but also between mimicked and felt emotions. We do not argue that these impairments alone cannot explain all differences in displayed emotional expressions and experienced emotions and empathy between individuals with and without ASD, but impairments in mimicry and facial feedback mechanisms have major implications for the emotional expressions and experience of individuals with ASD, as for their understanding of other people’s emotions, and play an important role in the causes behind the impairments that individuals with ASD experience in their social and emotional lives.
Notes
Individuals with autistic disorder have impairments in all three criteria of the syndrome (social interaction, communication, and repetitive behavior), while individuals with PDD-NOS do not display all symptoms.
Analyses of specific movements did not yield significant differences in mimicry between individuals with ASD and controls.
Though both groups displayed more behavioral mimicry, one cannot conclude that behaviors are by definition more profoundly mimicked, because this depends on the kind of movements, the target, the content, and a lot more.
The Study 1 video was 5 min; the Study 2 video was 3 min in length because it took less time to tell the story.
References
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed). Washington, DC: American Psychiatric Association.
Baron, R. M., & Kenny, D. A. (1986). The moderator-mediator variable distinction in social and psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51, 1173–1182.
Barsalou, L. W., Niedenthal, P. M., Barbey, A., & Ruppert, J. (2003). Social embodiment. In B. Ross (Ed.), The psychology of learning and motivation (Vol. 43, pp. 43–92). San Diego: Academic Press.
Bernieri, F. J. (1988). Coordinated movement and rapport in teacher-student interactions. Journal of Nonverbal Behavior, 12, 120–138.
Carruthers, P., & Smith, P. K. (1996). Introduction. In: P. Carruthers & P. K. Smith (Eds.), Theories of theories of mind (pp. 1–8). Cambridge: Cambridge University Press.
Charman, T., & Baron-Cohen, S. (1994). Another look at imitation in autism. Development and Psychopathology, 6, 403–413.
Chartrand, T. T., & Bargh, J. A. (1999). The chameleon effect: The perception-behavior link and social interaction. Journal of Personality and Social Psychology, 76, 893–910.
Darwin, C. (1965). The expressions of the emotions in man and animals. Chicago: University of Chicago Press. (Original work was published in 1872).
Dawson, G., Carver, L. J., Meltzoff, A. N., Panagiotides, H., McPartland, J., & Webb, S. J. (2002). Neural correlates of face recognition in young children with autism spectrum disorder. Child Development, 73, 700–717.
Dawson, G., Meltzoff, A., Osterling, J., Rinaldi, J., & Brown, E. (1998). Children with autism fail to orient to naturally occurring social stimuli. Journal of Autism and Developmental Disorders, 28, 479–485.
Dawson, G., Toth, K., Abbott, R., Osterling, J., Munson, J., & Estes, A. (2004). Defining the early social attention impairments in autism: Social orienting, joint attention, and attention to distress. Developmental Psychology, 40, 271–283.
Decety, J., Chaminade, T., Grezes, J., & Meltzoff, A. N. (2002). A PET exploration of the neural mechanisms involved in reciprocal imitation. NeuroImage, 15, 265–272.
Decety, J., Grezes, J., Costes, N., Perani, D., Jeannerod, M., Procyk, E., Grassi F., & Fazio, F. (1997). Brain activity during observation of actions. Influence of action content and subject’s strategy. Brain, 120, 1763–1777.
Decety, J., Perani, D., Jeannerod, M., Bettinardi, V., Tadary, B., Woods, R., Mazziotta, J. C., & Fazio, F. (1994). Mapping motor representations with PET. Nature, 371, 600–602.
Dimberg, U. (1990). Facial electromyography and emotional reactions. Psychophysiology, 27, 481–494.
Dimberg, U., Thunberg, M., & Elmehed, K. (2000). Unconscious facial reactions to emotional facial expressions. Psychological Science, 11, 86–89.
Downs, A., & Smith, T. (2004). Emotional understanding, cooperation, and social behavior in high-functioning children with autism. Journal of Autism and Developmental Disorders, 34(6), 625–634.
Emerich, D. M., Creaghead, N. A., Grether, S. M., Murray, D., & Grasha, C. (2003). The comprehension of humorous materials by adolescents with high-functioning autism and Asperger’s Syndrome. Journal of Autism and Developmental Disorders, 33, 253–257.
Gepner, B., de Schonen, S., & Buttin, C. (1994). Face processing in young autistic children. Infant Behavior and Development, 17, 661.
Gross, T. (2004). The perception of four basic emotions in human and nonhuman faces by children with autism and other developmental disabilities. Journal of Abnormal Child Psychology, 32, 469–480.
Hadjikhani, N., Joseph, R. M., Snyder, J., Chabris, C. F., Clark, J., Steele, S., McGrath, L., Vangel, M., Aharon, I., Feczko, E., Harris, G. J., & Tager-Flusberg, H. (2004). Activation of the fusiform gyrus when individuals with autism spectrum disorder view faces. Neuroimage, 22, 1141–1150.
Hatfield, E., Cacioppo, J. T., & Rapson, L. R. (1992). Primitive emotional contagion. In M. S. Clark (Ed.), Review of personality and social psychology: Emotion and social behavior (Vol. 14, pp. 151–177). Newbury Park, CA: Sage.
Hess, U., Kappas, A., McHugo, G. J., Lanzetta, J. T., & Kleck, R. E. (1992). The facilitative effect of facial expression on the self-generation of emotion. International Journal of Psychophysiology, 12, 251–265.
Hobson, R. P. (1989). Beyond cognition: A theory of autism. In G. Dawson (Ed.), Autism: Nature, diagnosis and treatment (pp. 22–8). New York: Guilford.
Hobson, P. (2007). Empathy and altruism. In: T. F. D. Farrow & P. W. R. Woodruff (Eds.), Empathy in mental illness (pp. 126–143). Cambridge: Cambridge University Press.
Izard, C. E. (1977). Human emotions. New York: Plenum.
James, W. (1890). Principles of psychology. New York: Holt.
Kugiumutzakis, G. (1996). The development of facial and vocal imitation in early infancy [Le developpement de l’imitation precoce de modeles de faciaux et vocaux]. Enfance, 1, 21–25.
Lawson, J., Baron-Cohen, S., & Wheelwright, S. (2004). Empathizing and systemizing in adults with and without Asperger syndrome. Journal of Autism and Developmental Disorders, 34(3), 301–310.
Loveland, K., Tunali-Kotoski, B., Pearson, D., Brelsford, K., Ortegon, J., & Chen, R. (1994). Imitation and expression of facial affect in autism. Development and Psychopathology, 6, 433–444.
McIntosh, D. N. (1996). Facial feedback hypotheses: Evidence, implications, and directions. Motivation and Emotion, 20, 121–147.
McIntosh, D. N., Reichmann-Decker, A., Winkielman, P., & Wilbarger, J. L. (2006). When the social mirror breaks: Deficits in automatic, but not voluntary, mimicry of emotional facial expressions in autism. Developmental Science, 9, 295–302.
Meltzoff, A. N., & Moore, N. K. (1983). Newborn infants imitate adult facial gestures. Child Development, 54, 702–709.
Meltzoff, A. N., & Moore, N. K. (1989). Imitation in newborn infants: Exploring the range of gestures imitated and the underlying mechanisms. Developmental Psychology, 25, 954–962.
Mundy, M., Sigman, P., Ungerer, T., & Sherman, J. (1986). Social interactions of autistic, mentally retarded and normal children and their caregivers. Journal of Child Psycholology and Psychiatry, 27, 647–655.
Nishitani, N., Avikainen, S., & Hari, R. (2004). Abnormal imitation-related cortical activation sequences in Asperger’s syndrome. Annual of Neurology, 55, 558–562.
Oberman, L. M., Hubbard, E. M., McCleery, J. P., Ramachandran, V. S., & Pineda, J. A. (2005). EEG evidence for mirror neuron dysfunction in autism spectrum disorders. Cognitive Brain Research, 24, 190–198.
O’Toole, R., & Dubin, R. (1968). Baby feeding and body sway: An experiment in George Herbert Mead’s “taking the role of the other”. Journal of Social and Personality Psychology, 10, 59–65.
Ozonoff, S., Pennington, B. F., & Rogers, S. J. (1991). Executive function deficits in high-functioning autistic individuals: Relationship to theory of mind. Journal of Child Psychology and Psychiatry, 7, 1081–1105.
Rizzolatti, G., Fadiga, L., Fogassi, L., & Gallese, V. (2002). From mirror neurons to imitation: Facts and speculations. In A. N. Meltzoff & W. Prinz (Eds.), The iimitative mind: Development, evolution, and brain bases. Cambridge UK: Cambridge University Press.
Rogers, S. J., Bennetto, L., McEvoy, R., & Pennington, B. F. (1996). Imitation and pantomime in high-functioning adolescents with autism spectrum disorders. Child Development, 67, 2060–2073.
Rogers, S. J., Hepburn, S. L., Stackhouse, T., & Wehner, E. (2003). Imitation performance in toddlers with autism and those with other developmental disorders. Journal of Child Psychology and Psychiatry, 44, 763–781.
Rogers S. J., & Pennington B. F. (1991). A theoretical approach to the deficits in infantile autism. Developmental Psychopathology, 3, 137–162.
Sigman, M. D., Kasari, C., Kwon, J. H., & Yirmiya, N. (1992). Responses to the negative emotions of others by autistic, mentally retarded, and normal children. Child Development, 63, 796–807.
Stel, M., & Van Knippenberg, A. (2002). The role of facial mimicry in emotion recognition [De rol van gezichtsimitatie in de herkenning van emoties]. In D. A. Stapel, M. Hagedoorn, & E. Van Dijk (Eds.), Jaarboek Sociale Psychologie 2001 (pp 215–226). Delft: Eburon.
Stel, M., Vonk, R., & Smeets, R. C. (2006). The experience and communication of prosocial feelings due to mimicry in social interactions: Effects for perceivers and targets. Poster presented at the 7th general meeting of the Society for Personality and Social Psychology, January 2006, Palm Springs, California.
Strack, F., Martin, L. L., & Stepper, S. (1988). Inhibiting and facilitating conditions of the human smile: A nonobtrusive test of the facial feedback hypothesis. Journal of Personality and Social Psychology, 54, 768–777.
Tomkins, S. S. (1982). Affect theory. In P. Ekman (Ed.), Emotion in the human face (2nd ed., pp. 353–395). Cambridge: Cambridge University Press.
Van Engeland, H. (2000). Autisme en psychosen. In W. Vandereycken, C. A. L. Hoogduin, & P. M.G. Emmelkamp (Eds.), Handboek psychopathologie: deel 1 Basisbegrippen (pp. 469–489). Houten/Diegem: Bohn Stafleu Van Loghum.
Yirmiya, N., Sigman, M., Kasari, C., & Mundy, P. (1992). Empathy and cognition in high functioning children with autism. Child Development, 63, 150–160.
Acknowledgments
We thank Evelien Kinds, Anne Wevers, Vincent van Kempen for insightful discussions and to Tom Wingens and Manja Landman for the production of video materials.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Stel, M., van den Heuvel, C. & Smeets, R.C. Facial Feedback Mechanisms in Autistic Spectrum Disorders. J Autism Dev Disord 38, 1250–1258 (2008). https://doi.org/10.1007/s10803-007-0505-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-007-0505-y