
Abstract
Multiple pathway models propose that attention deficit hyperactivity disorder (ADHD) arises from dysfunction in separate systems comprised of a "cool" or cognitive pathway versus a “hot” or emotional/reward pathway. Interactions between these pathways and the degree of maturation may further determine functional outcomes for adolescents ranging from those diagnosed with ADHD to typical development (TD). We used a latent profile analysis on rating scales and behavioral task performance assessing emotion, irritability, impulsivity, risk-taking, future orientation, and processing speed (PS) to identify subgroups of TD adolescents and adolescents with ADHD (N = 152) based on the hot and cool pathway model. We identified four classes: 1) High-Complex Challenges; 2) Moderate-Mixed Challenges; 3) Non-Emotive Impulsivity; and 4) High Regulation and Control. A multiple pathway model of ADHD is supported with classes differing in degree of emotional lability and irritability, types of impulsivity, and ability to use future consequences to modulate impulsivity and PS. The classes differed regarding functional behavior, with the High-Complex class demonstrating the most severe functional challenges in academic-related functioning. The Moderate-Mixed class also displayed significant functional challenges but with moderate emotional lability and irritability ratings. The Non-Emotive Impulsivity class exhibited low emotionality and low irritability, yet high impulsivity with limited negative functional consequences, and was composed of a mix of ADHD and TD adolescents. Differences between classes suggest ADHD symptomatology may represent both categorical and dimensional differences. Precision health interventions may be more effective in addressing the specific challenges associated with the classes rather than a one-size-fits-all approach to treating ADHD.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Attention deficit/hyperactivity disorder (ADHD) is one of the most diagnosed neurodevelopmental disorders, affecting 3–7% of US children aged 4 to 17 (Visser et al., 2014). The Diagnostic and Statistical Manual of Mental Disorders (DSM) classifies ADHD into three categories: predominately Inattentive presentation, predominantly Hyperactive/ Impulsive presentation, and Combined presentation (American Psychiatric Association, 2013). However, considerable inter-individual heterogeneity exists in the symptom presentation of individuals diagnosed with ADHD (American Psychiatric Association, 2013; Luo et al., 2019). Symptom-based subtypes have failed to demonstrate consistent external validity. They lack stability over time, have poor interrater reliability (Arnett & Flaherty, 2022), and lack distinct neuropsychological or neurobiological patterns (Willcutt et al., 2012). Parsing heterogeneity in ADHD to identify homogenous subtypes may advance specific guidelines for treatment options for the disorder (Arnett & Flaherty, 2022).
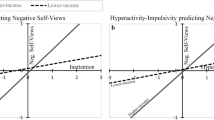
Researchers have attempted to conceptualize ADHD in various ways beyond the DSM categories (e.g., Nigg, 2017, 2022). For example, the Dual Pathway model in ADHD (Sonuga-Barke et al., 2010) emphasizes the contributions of cognitive control (“cool” processes) versus reward responsivity (“hot” processes) to explain individual variation in ADHD (Antonini et al., 2015; Castellanos et al., 2006; Skogli et al., 2017; Van Cauwenberge et al., 2015). In this model, ADHD symptoms arise from: 1) a deficit in cognitive control related to improper function of the dorsal lateral prefrontal cortex and/or; 2) an over-dependence on immediate rewards and mesolimbic dopamine dysfunction. The Triadic Model perspective for adolescent-motivated behavior (Ernst, 2014) also applies to ADHD during adolescence. It extends the Dual Pathway model by incorporating the critical role negative emotionality and irritability can have on reward-related processes (i.e., impulsivity and risk-taking) and higher-order cognitive operations. Furthermore, it incorporates the role development can play in how these systems interact with more advanced neurodevelopment associated with shifts in the balance toward higher future orientation and planned, thoughtful, cognitive control processes, away from automatic, visceral reward responding. Figure 1 presents a dynamic model of ADHD expression that considers the interaction between hot and cool processes and how their relation may change with development. The role of development is crucial to understanding ADHD, given that ADHD is associated with a delay in maturation by an average of 3 years in the cognitive control-brain systems (Shaw et al., 2007).

Dynamic model of ADHD Symptom Expression. Expression of ADHD symptoms is determined by the interactions between “hot” reward/emotion systems and “cool” cognitive control systems. Emotion/reward related processes peak earlier in adolescent development and remain steady for subgroups but decrease in other subgroups with development. Cognitive control processes increase linearly with development. Optimal regulation of emotion and behavior is achieved when cognitive control processes can effectively modulate reward/emotion processes either by reducing the pull of immediate rewards or enhancing the saliency of future, delayed rewards. Elevated ADHD symptoms may reflect either heightened reward/emotion systems, weak cognitive control systems, or a combination of the two. Elevated ADHD symptoms may also reflect emerging development with relatively immature cognitive control expected for one’s age. ADHD, attention-deficit/hyperactivity disorder
In the ADHD literature, cognitive control is often synonymous with the term “executive function” (EF) and used as an umbrella term referring to the cool cognitive processes necessary to complete goal-directed behaviors (Barkley, 2013). Children with ADHD display lower scores on cool EFs, including processing speed (PS) or how quickly an individual understands information and then acts on it (e.g., Chhabildas et al., 2001; Rucklidge & Tannock, 2002; Willcutt et al., 2005). Another cool EF is working memory (WM) performance, which involves holding information in mind and manipulating it to complete a task (Baddeley & Hitch, 1974), and it is well-documented as weaker in children with ADHD (Fassbender et al., 2011; Rapport et al., 2008; Ramos et al., 2020; Willcutt et al., 2005). On a neural level, studies have found that children with ADHD show reduced brain activation in several regions involved in WM, including the medial prefrontal cortex, the basal ganglia, and the cerebellum (Fassbender et al., 2011; Mukherjee et al., 2021). We note, however, that although WM difficulties are the most consistent cognitive impairment associated with ADHD, not all individuals with the diagnosis display challenges in WM (Kasper et al., 2012; Kofler et al., 2011; Nigg et al., 2018).
Hot EF challenges in ADHD, referring specifically to challenges in effectively managing emotions, are becoming increasingly studied and considered by some a key characteristic of the disorder (Barkley, 2015; Nigg, 2022). In addition, irritability, a narrower construct of emotional lability, defined by a short temper, low frustration tolerance, and sudden and unpredictable shifts toward negative emotions, is also progressively recognized as elevated in ADHD and associated with neural alterations (Kahle et al., 2021; Leibenluft et al., 2006; Maedgen & Carlson, 2000; Mukherjee et al., 2022; Nigg et al., 2004; Schweitzer el al., 2006).
Certain behaviors can be conceptualized as mediated by the interaction of cool and hot processes, such as risk-taking or situations involving deciding how to act toward a future reward or the absence of a reward (Lejuez et al., 2002). Weaker EF, stronger limbic-reward functioning, or reduced connectivity between EF-associated brain regions and limbic regions, as was found in typical development (e.g., amygdala, nucleus accumbens; van den Bos et al., 2015), may increase the likelihood of engaging in risky and impulsive behaviors. In everyday functioning, ADHD is associated with a plethora of risky behaviors such as higher rates of substance abuse, earlier pregnancies, lower likelihood to use protection during sex, more accidents, and emergency room visits compared to individuals without ADHD (Barkley et al., 2015).
Time perspective may mediate the balance between current behavior and future consequences and the interaction between cool and hot processes. Children with ADHD demonstrate poor time perception (Rubia et al., 2007). Weaknesses in future time orientation in ADHD have been hypothesized to be due to impairments in WM, inhibitory control, and present-time perception (Barkley, 2013). This may lead to a preference for present-oriented behaviors, such as engaging in impulsive actions, procrastinating, and avoiding tasks that have long-term benefits but require effort in the present (Barkley, 2013). Finally, understanding how cool and hot EF might relate to school performance and peer relationships is critical, given the frequent challenges in the school setting associated with the disorder (e.g., Polderman et al., 2010; Tamm et al., 2021).
The Current Study
The present study aims to (a) use a person-centered approach to identify differential profiles of hot and cool processes and (b) characterize differences in sex, diagnosis, and performance among these profiles and relate them to areas of critical everyday functioning. We hypothesized that distinct profiles would emerge within the sample, beyond diagnostic categories—and that not all clinical participants would be rated as high on emotional variables. We then considered the relationship between profile membership and everyday functioning. This study focused on a sparsely studied group, adolescents with ADHD, Combined presentation symptoms, and TD adolescents, to enable the exploration of hot and cool processes at a time in development associated with rapid changes between these processes and in youth with heightened risk for impulsiveness and risk-taking behavior. We used latent profile analysis (LPA) to parse heterogeneity in ADHD and identify clinically meaningful subgroups. Furthermore, we applied the Research Domain Criteria framework to examine how phenotypic features associated with hot (e.g., emotional lability, irritability, risk-taking) and cool (e.g., PS, WM) functions presented beyond diagnostic categories in ADHD and TD youth, using a dimensional approach across a range of the hot versus cool measures.
Methods
Participants and Procedures
This study draws from the Mapping Impulsivity's Neurodevelopmental Trajectory (MINT) longitudinal investigation of the neurodevelopmental trajectory of impulsivity (PI: Schweitzer; Elliott et al., 2022; Kahle et al., 2021; Mukherjee et al., 2021, 2022) in adolescents and young adults. MINT collected imaging, behavioral, clinical, and academic measures for ADHD, Combined Presentation, and TD adolescents. Toward the end of the study, MINT also recruited participants with a range of ADHD symptoms between TD and the criterion for clinical diagnosis of ADHD to study ADHD symptoms on a continuum. The University of California, Davis Institutional Review Board approved this study, with written informed consent obtained from parents and written assent from participants.
Participants were recruited from the MIND Institute participant recruitment pool, MIND Institute and Departments of Psychiatry and Pediatric specialty clinics, local middle and high schools and universities, community flyers, and social media sites. Two licensed psychologists (JBS and JFD) evaluated phone screen data regarding symptoms and functioning to determine study eligibility. Eligible participants and one of their parents/caregivers completed a full psychiatric interview (Diagnostic Interview Schedule for Child and Adolescents or the M.I.N.I. International Neuropsychiatric Interview—Kid for DSM-5); parents and teachers completed rating scales (i.e., Parent [Conner-3 Parent Rating Scale—CPRS-3]) and [Teacher (Conners-3 Teacher Rating Scale—CTRS-3]). A licensed psychologist (JBS or JFD) determined whether participants met DSM criteria for ADHD, the presence of any other major psychiatric disorder, or would be best classified as “subthreshold” or TD. Subthreshold ADHD refers to a classification in which individuals exhibit the presence of symptoms characteristic of ADHD but do not meet the full diagnostic criteria as outlined in the DSM-5. Specifically, individuals categorized as subthreshold ADHD in our study present with 3–5 symptoms related to either inattentive or hyperactive/impulsive behaviors, which are representative of ADHD symptomatology. Moreover, these symptoms are accompanied by substantial functional impairment across multiple settings, indicating their significant impact on daily activities, responsibilities, and interactions.
Initially, DSM-IV-TR was used, and then DSM-5 upon its publication. However, evaluation criteria for ADHD for participants entering the study under DSM-IV-TR were re-reviewed for DSM-5 criteria for ADHD for all included participants. Inclusion criteria included an IQ ≥ 80 with additional inclusion criteria for the ADHD group meeting DSM-5 criteria for ADHD Combined presentation. Exclusion criteria included the presence of a math or reading learning disability; a history of head trauma, neurological disorder, or major medical problem as reported by the participant or their parents; taking psychoactive medication other than stimulants or atomoxetine; and meeting criteria for Axis I diagnosis except for ADHD, oppositional defiant disorder, or conduct disorder. Participants prescribed stimulant medication or atomoxetine for ADHD abstained from taking the medication for five half-lives before being tested on the Balloon Analogue Risk Task and Picture Order Memory Paradigm. The current study focuses on the adolescents in our study and includes 152 youth between 12 and 17.9 years old (99 boys, 53 girls), utilizing the data from their baseline visit.
Measures
We selected a range of measures that tap into cognitive control and reward/emotion processes and functions that integrate the two. We used multi-informant reporters, including parent and self-report scales and objective measures, representing trait and state functioning.
Conners’ Parent Rating Scale 3rd Edition
We used the long-form CPRS-3 to evaluate ADHD and associated symptoms, including the DSM Hyperactivity/Impulsivity, Emotional Lability, EF, Learning Problems, and Peer Relations scales. We also derived an Irritability measure based on summing five items (i.e., 12, 48, 73, 81, 100) from the CPRS-3 shown to highly correspond to items on the Affective Reactivity Index (Kahle et al., 2021; Stringaris et al., 2012). There is no overlap in the items included in the Emotional Lability and Irritability scales.
Barratt Impulsiveness Scale (BIS-11)
This scale is the most widely cited questionnaire designed to assess the behavioral construct of impulsiveness. It consists of 30 items based on a self-report questionnaire. We used the Motor Impulsiveness and Self-Control factors of the BIS, as these two are most consistent with our goal of studying impulsivity. The Motor Impulsiveness factor captures challenges in inhibiting acting, whereas the Self-Control factor refers more to problems with delaying gratification. Therefore, the present study extracted motor impulsiveness and self-control raw scores to use in the LPA.
Balloon Analogue Risk Task (BART)
The BART is a computerized decision-making task used to assess risk-taking behavior (Barnhart & Beulow, 2017). The BART has good internal consistency, test–retest reliability, and convergent validity (Lejuez et al., 2002). It simulates real-world situations involving risky behavior, where more balloon pumps can yield more money. However, higher pumps can result in the balloon popping, with a loss of all the money. Participants were given real money based on their performance, and the average amount earned from the BART was used in the LPA.
Wechsler Scales of Intelligence
Participants aged 12—16 years completed the full Wechsler Scale of Intelligence (WISC-IV) to assess intellectual ability; participants above 16 took the Wechsler Adult Scale of Intelligence (WAIS). We utilized the PS composite score for the LPA, composed of two subtests: coding and symbol search.
Zimbardo Time Perspective Inventory (ZTPI)
The ZTPI is a valid and reliable index of individual differences in time perspective (Sircova et al., 2014; Zimbardo & Boyd, 1999). Time perspective corresponds to an individual’s view of the past and future at a given time. The present study uses raw scores from present hedonism and future orientation in the LPA. Present hedonism refers to being drawn to a reward and satisfying oneself at the time. Future orientation refers to using future consequences to guide current behavior and involves the ability to consider the future and planning. Prior findings from our group demonstrated adolescents had lower future orientation scores than young adults (van den Bos et al., 2015), and ADHD had lower future orientation and higher present hedonism than TD youth (Elliott et al., 2022). The ZTPI was added partway through data collection; thus, we substituted data from the next available visit for participants missing this measure at baseline.
Wechsler Individual Achievement Test (WIAT-III)
The WIAT–3rd Edition is an individually administered, norm-referenced test evaluating a range of academic skills across several domains. In the current study, we aimed to assess differences in functional outcomes of reading comprehension and math problem-solving among LPA classes.
Picture Order Memory Paradigm (POMP)
The POMP (Mukherjee et al., 2021) requires WM using a condition in which participants are shown three images sequentially, followed by instructions to recall the items in reverse order (i.e., backward) (Mukherjee et al., 2021). We used the total number correct on the task for the analysis. Our earlier work demonstrated neural and behavioral differences between TD and ADHD groups (Mukherjee et al., 2021). In this study, we assessed how the functional outcome of this WM task differs across the LPA classes.
Relation Between Classes and Broader Functional Outcomes
We used broad, day-to-day functioning measures to explore their relation with the identified classes. Measures of broader functioning included those mentioned above from the CPRS-3: ADHD Predominantly Hyperactive/Impulsive DSM-5 symptom scale, Peer Relations, Learning Problems, and Executive Functioning subscales. Additionally, the WIAT-III assessed Reading Comprehension and Math Problem-Solving abilities. Finally, we evaluated the relation between the classes and a measure of WM (POMP), requiring strong manipulation of information given that WM issues are prevalent in ADHD and hypothesized to underlie many critical EF processes in ADHD (Rapport et al., 2008).
Statistical Approach
We first used LPA to identify distinct patterns related to emotional and reward functioning and cognitive control based on CPRS-3, BIS, ZTPI, and BART scores. The maximal reliability (H) for the eight variables included in the LPA was 0.92 (95% confidence interval 0.88 to 0.95). Models were estimated using full-information maximum likelihood, allowing us to include the participants with missing data under the missing-at-random assumption. We fitted and compared models with increasing numbers of classes, starting with one and determining the optimal number of classes based on statistical goodness-of-fit criteria, considering whether the classes capture clinically meaningful features and the proportion of participants represented in the classes (Masyn, 2013; Nylund et al., 2007). Goodness-of-fit criteria included Bayesian information criterion (BIC) and sample-size adjusted BIC, Akaike Information Criterion (AIC), consistent AIC and corrected AIC, approximate weight of evidence criterion (AWE, Masyn, 2013), correct model probability (cmP), Vu-Lo-Mendell-Rubin, Lo-Mendell-Rubin adjusted (LMR), and Parametric Bootstrapped likelihood ratio tests (BLRT, Lo et al., 2001; Nylund et al., 2007). Smaller AIC, BIC, and AWE values indicate better fit. cmP allows a researcher to compare a set of more than two latent class models, and higher values indicate more robust evidence for the candidate model compared to other models (Masyn, 2013). The likelihood ratio tests compare the fit of the specified class solution to models with one fewer class, and a significant p-value indicates that the specified model is preferred. The local maximum problem was addressed using up to 2,000 starting points to replicate each model.
Each LPA model identifies the number of latent classes (subgroups) within the sample and estimates posterior probabilities for each participant’s assignment to each latent class. For descriptive analyses, the highest posterior probability from the best-fitting model was used to assign each participant to the most likely subgroup. For subsequent analyses using latent subgroup membership (i.e., examination of differences in diagnosis, sex, impulsivity, and achievement), multiple pseudo-class draws (Bandeen-Roche et al., 1997) were used to reduce bias by accounting for the uncertainty in class assignments. Differences in categorical characteristics (e.g., sex, ADHD diagnosis) across latent classes were assessed using χ2 tests. Differences in dimensional measures of functioning were assessed using general linear models, accounting for age and sex, as appropriate. Age and sex were not retained in the reported models if they did not contribute significantly to the model. Transformations were employed for variables that violated the normality assumption. We used univariate and bivariate residual plots and univariate summaries of residuals to check the normality and homoscedasticity of residuals. Participants were randomly classified into latent classes 100 times based on their distribution of posterior probabilities from the best-fitting LPA model. The subsequent analyses were performed 100 times (i.e., for each draw), and results were combined across draws using standard methods for multiple imputations for missing data (Rubin, 1987). After combining results across draws, two approaches were used to control for multiple comparisons when assessing significant differences between groups. First, overall, three-degree-of-freedom F-tests for the group were adjusted for multiple comparisons using the Benjamini–Hochberg method. Then, for all variables with significant overall F-tests for group after adjustment, a second Benjamini–Hochberg procedure was used to identify all pairs of latent groups that were significantly different out of all possible pairs. LPA was performed in Mplus version 8.0 (Muthen & Muthén, 1998-2017). All other analyses were implemented using SAS Version 9.4 (SAS Institute Inc., Cary, NC). All tests were two-sided, and p-values < 0.05 were considered statistically significant.
Results
The analyzed sample consisted of all study participants who were less than 18 years old at their baseline visit and included 152 youth (53 females, 99 males), of which n = 83 (24 females, 59 males) had ADHD, n = 6 (3 females, 3 males) had subthreshold ADHD, and n = 63 (26 females, 37 males) were TD. Of those reporting race, the sample was predominantly (90.7%) White, 19.7% Hispanic, and 78.8% had at least one parent with a college or more advanced degree.
Latent Profile Analyses
Fit indices for one-class to six-class solutions are summarized in Table 1. They provided support for the four-class as the optimal solution. Except for AIC and sample-size adjusted BIC indices, which never increased with added classes (though substantially smaller improvements were garnered after the four-class solution), the AWE, which supported a two-class solution, and the BLRT, which continued to support the larger model up to six classes, all the other criteria suggested that a four-class solution was optimal (four-class was better than three-class, and five-class was not better than four-class). In latent profile analyses, AIC and BIC may not increase with additional parameters, but the resulting models may have additional classes that are not meaningful. For example, in the five-class model, one class with impairments across modalities was differentiated into two classes that were not meaningfully different. Moreover, the five- and six-class models identified a class that included 5% or less of the sample. Thus, the four-class solution was selected as the most parsimonious model that still provided adequate fit and the most clinically meaningful distribution of classes. Based on the pattern of profiles, the four classes were named High-Complex Challenges (17.0%), Moderate-Mixed Challenges (19.9%), Non-Emotive Impulsivity (30.1%), and High Regulation and Control (32.9%). The four-class model provided good classification quality, with an entropy value of 0.87 and high average posterior probabilities of class membership: 0.98, 0.93, 0.89, and 0.91, respectively. Figure 2 illustrates the profiles for the four-class solution. To aid interpretation, before graphing the profiles, we standardized the scores. For all eight variables included in the LPA, there were significant differences across classes (Kruskal–Wallis ps < 0.01). The High-Complex Challenges showed impairment on almost all measures, but particularly on emotional lability and irritability. Challenges are also present in PS, high risk-taking, poor self-control, and low future orientation. The one area in which they displayed less impairment was on a self-rating for oversensitivity to immediate rewards (i.e., present hedonism). The Moderate-Mixed Challenges class is characterized by strong negative emotionality but to a less intense degree than the High-Complex class. This class also still displays elevated issues with self-control, including being drawn to more immediate rewards, yet somewhat higher future orientation and less risk-taking. This Moderate-Mixed class may represent a combination of moderate challenges in cognitive control and reward-related processes. The Non-Emotive Impulsivity class is consistent with immature development of cognitive control, appearing highly drawn toward immediate rewards, high risk-taking, low future orientation, and yet, strong emotional control. The High Regulation and Control class excelled in cognitive control, reward, and emotional control measures.

Profiles of the four LPA classes. To help the interpretation of this graph, variables were standardized to a mean of 0 and a standard deviation of 1
Differences Among LPA Groups
Demographic and clinical characteristics for all classes are presented in Table 2. The overwhelming majority of the High-Complex Challenges class comprises ADHD-diagnosed adolescents. The Moderate-Mixed class predominantly includes adolescents diagnosed with ADHD, with somewhat lower scores on Conners’ scales than the High-Complex Challenges class. The Non-Emotive Impulsivity class comprises 59% ADHD-diagnosed adolescents, 2% subthreshold ADHD, and, interestingly, 39% TD. Finally, the High Regulation and Control class is primarily, but not exclusively, TD (82%).
Participant sex significantly differed across class membership (p = 0.03). A higher proportion of girls were classified in High Regulation and Control classes. However, the four classes were similar in age, race and ethnical composition, and parental education (Table 2).
Differences in Functional Outcomes
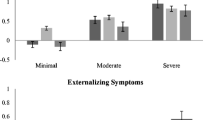
Next, we examined whether the four LPA classes differed in functional outcomes. Table 3 shows the CPRS-3, POMP, and WIAT scores for the four classes, and Fig. 3 summarizes the standardized average scores for the four groups across these variables. Table 4 shows the estimated class differences after adjusting for multiple comparisons.

Standardized mean scores for the LPA-derived classes. Standardized mean scores were calculated after rescaling every measure so that higher scores indicate more symptoms. Averages and standard errors for each subgroup were calculated after generating 100 data sets using pseudo-draws to assign group membership and pooling the results. Error bars represent ± 1 standard error
The classes differed significantly on all CPRS scales examined (all p< 0.001). After adjusting for multiple comparisons, adolescents in the High-Complex class displayed significantly higher DSM ADHD Hyperactive/Impulsive scores compared to two classes, Non-Emotive Impulsivity and High Regulation and Control (p< 0.001; Table 4). The Moderate-Mixed class had significantly higher scores than the Non-Emotive Impulsivity and High Regulation and Control classes (p = 0.03 and < 0.001, respectively). After adjusting for multiple comparisons, the High-Complex class did not significantly differ from the Moderate-Mixed class (p = 0.08). Finally, the Non-Emotive Impulsivity class had significantly higher scores than the High Regulation and Control class (p< 0.001). A similar pattern was observed for Learning Problems, with the High-Complex class scoring higher than the Non-Emotive Impulsivity and High Regulation and Control (both p < 0.001). The Moderate-Mixed class showed more Learning Problems than the Non-Emotive Impulsivity and the High Regulation and Control classes (p = 0.005 and < 0.001, respectively). Finally, the Non-Emotive Impulsivity class had higher scores on Learning Problems than the High Regulation and Control class (p = 0.002). Peer Relations from the CPRS-3 revealed significant differences with the Moderate-Mixed class, indicating higher Peer Relations scores than the High Regulation and Control class (p < 0.001). Additionally, the Non-Emotive Impulsivity class had higher Peer Relations scores than the High Regulation and Control class, but this difference was not statistically significant (p = 0.07). Finally, the High-Complex class had higher scores on the Peer Relations subscale compared to the Non-Emotive Impulsivity and High Regulation and Control classes (both p< 0.001). The pattern was similar for EF, with the High-Complex class scoring higher than the Non-Emotive Impulsivity and High Regulation and Control classes (p< 0.001). Additionally, the Moderate-Mixed class scored higher on EF than the Non-Emotive Impulsivity and High Regulation and Control classes (p = 0.007 and < 0.001, respectively). The Non-Emotive Impulsivity class scored higher on EF than the High Regulation and Control class (p < 0.001).
The groups differed significantly on the squared transformed WM task scores (p = 0.004). After further adjusting for multiple comparisons, the results showed that adolescents in the High-Complex and Moderate-Mixed classes had lower scores compared to the High Regulation and Control class (p = 0.01 and 0.004, respectively). Finally, we examined whether the LPA classes differed in academic achievement based on WIAT-III standardized Reading Comprehension and Math Problem Solving scores. As expected, the classes differed on the log-transformed WIAT-III standardized subscale scores (both p = 0.04 after adjusting for multiple comparisons). After further adjusting for multiple comparisons, the results indicated that adolescents in the High-Complex class performed significantly worse in Reading Comprehension than those in the High Regulation and Control class (p = 0.03, Table 4). For the Math Problem Solving scores, the results suggested that adolescents in the High-Complex class demonstrated worse performance than those in the High-Regulation and Control class in Math Problem-solving. Still, these differences did not reach statistical significance after adjusting for multiple comparisons (both p = 0.055, Table 4).
Discussion
This study used a dimensional approach to identify classes of performance regarding “hot” and “cold” functioning in adolescents who were primarily TD or diagnosed with ADHD Combined Presentation and to characterize further whether classes differed regarding emotionality, irritability, impulsiveness, time perspective, cognition, and risk-taking. Our results revealed four classes with varying ADHD characteristics. The High-Complex class is composed of females (32%) and males (68%) with ADHD (96%) and subthreshold ADHD (4%). The literature on male-to-female prevalence for ADHD, including for Combined Presentation, which comprises most of the ADHD group, reports a wide range for the male-to-female ratio, and the percentage of females in this class reflects the higher end of that range (Danielson et al., 2018; Willcutt et al., 2012). The relatively high percentage of females in this class is consistent with other findings (e.g., Rosch et al., 2018), where females may exhibit more severe ADHD symptoms, particularly regarding impulsivity. This group displays high levels of hot and cool processing challenges, potentially associated with overactive ventral striatum and amygdala activity and connectivity and reduced activity in cortical brain regions and connectivity between cortical and subcortical regions.
The Moderate-Mixed class comprises predominantly male individuals (73%) with a range of symptom severity, including moderate levels of lability and irritability. However, difficulties with self-control were also evident. Additionally, this class displayed somewhat lower risk-taking behaviors. Weaknesses in future orientation may weaken their self-control. We hypothesize that adolescents in this class may eventually outgrow some of their challenges and are less likely to have high comorbid disorders than those in the High-Complex class. The Non-Emotive Impulsivity class primarily comprises males (80%). This class displayed lower levels of emotionality with reduced irritability, yet difficulties with self-control, low future orientation, and high risk-taking. Their profile is somewhat consistent with a profile of younger youth, perhaps with under-developed EF and heightened responsivity to immediate rewards. Their PS was weaker, which could predict potential difficulties with tasks that require executive control (Barkley, 2013; Wilcutt et al., 2005).
We hypothesize that longitudinal data of these adolescents may find that those in this group who are diagnosed with ADHD may have a remittance of symptoms as they mature. Findings from structural imaging studies (Lenroot & Giedd, 2010) suggest males are about two to three years slower in brain development than girls. We speculate that parents of a subset of this class who have concomitant lower grades and poor study habits may experience concern when their children reach high school. Specifically, parents may worry about their adolescents' maturity level and ability to compete and prepare for college, motivating them to seek an ADHD evaluation and treatment. Finally, the High Regulation and Control class is characterized by a relatively even distribution of males (45%) and females (55%), with most individuals presenting with TD profiles (82%). Overall, individuals in this class performed uniformly well across modalities but demonstrated particularly strong EF, self-control, and future orientation. However, approximately 18% of individuals within this class were diagnosed with either ADHD or sub-threshold ADHD, indicating that there may be varying degrees of core symptom manifestation. Thus, these youth are exhibiting behaviors that are sufficiently severe to warrant a diagnosis (or sub-threshold diagnosis) of ADHD. Yet, in the behaviors we examined in this analysis they were more similar to TD peers. Other studies have found that only 33% to 50% of children diagnosed with ADHD also present with executive dysfunction (Kofler et al., 2019), and only 20% to 50% of children diagnosed with ADHD experience irritability and have difficulty with emotional regulation (Shaw et al., 2014). Consequently, these findings suggest that among the 18% of individuals with ADHD in the class, it is plausible that they may not exhibit these symptoms to the same extent as other children with ADHD. They may have different strengths that allow them to compensate on a neural and/or behavioral level to control their emotions and impulsive behavior. Our findings reinforce the concept that there are important subgroups within the broad diagnostic category of “ADHD diagnosis,” even within the ADHD Combined Presentation, presenting with profiles that vary according to different strengths and weaknesses.
Our second objective was to investigate whether there were any differences between ADHD classes in terms of functional outcomes. A review of the relation between the classes and the functional variables revealed that the High-Complex class demonstrated uniformly high challenges in hyperactive/impulsive and EF behaviors and school-related issues, including Peer Relations. The Moderate-Mixed Class showed less intense emotional challenges than the High Complex-Class, a relative strength in Math Problem Solving, yet greater WM and Reading Comprehension challenges. These findings suggest a disassociation between the type of academic challenge (i.e., math versus reading) and perhaps their relation to WM performance.
Our WM task is an object span task rather than a verbal task, and it may be that a verbal WM task would have produced different results. The Non-Emotive Impulsivity class demonstrated significant differences in the Conners’ functional measures (i.e., Hyperactivity/ Impulsivity, Learning Problems, Peer Relations and EF) compared to the other classes. Yet, after controlling for multiple comparisons, their academic performance appears to be relatively intact, in comparison to the High Regulation and Control class. Future research should explore if there are different neural mechanisms associated with the degree of emotionality expressed, WM, and academic performance between the classes.
We suspect persons in the High-Complex class will likely experience the most persistent challenges. For example, Barkley and colleagues (2008) found greater emotional impulsivity and lability (frustration, annoyance, anger) in a prospective study of adults who were diagnosed with ADHD as children when their ADHD persisted to 27 years of age in comparison to adults whose childhood ADHD did not persist into their late 20s. Furthermore, work in the Hinshaw laboratory found that girls with ADHD with greater impulsivity were more likely as young adults to exhibit self-harm: suicidal ideation and attempts and serious non-suicidal severe injury (Hinshaw et al., 2012). Thus, we recommend that parents and practitioners continue to closely monitor and provide treatment for adolescents in this class, as future challenges are likely to emerge. It will be interesting to see if youth in the Non-Emotive Impulsivity class either outgrow their symptoms or learn to manage them to minimize their negative impact on other aspects of their lives.
Adolescence is a time of significant developmental changes, both biologically and socially, which can impact the presentation of ADHD symptoms. Although these individuals were selected for high ADHD hyperactive/impulsive symptoms, these symptoms tend to decline during adolescence and adulthood for some, while others continue to experience symptoms into adulthood (Barkley, 2015). This study highlights the importance of understanding how ADHD presents during different developmental periods, including adolescence, and the potential limitations of relying on a categorical diagnostic system like the DSM.
Our findings provide hints as to which aspects of functioning are more amenable to prevention and intervention. Recent research (Brotman et al., 2017) is testing ways to target irritability, which may improve long-term outcomes for those youth presenting with high irritability and emotional lability. Interventions to increase the delay of gratification in young children by using shaping techniques to increase patience while waiting for delayed rewards or reinforcing the use of alternative rewards while waiting for delayed rewards (e.g., Schweitzer & Sulzer-Azaroff, 1988, 1995) may be helpful for many children expressing high impulsivity and “present hedonism.” Episodic future thinking might be particularly useful for those adolescents who have weak future orientation (e.g., High-Complex and Moderate-Mixed classes and has received surprisingly little attention in the ADHD research community (c.f., Solanto & Scheres, 2021) but has strong empirical support for improving self-control in youth (Daniel et al., 2015) and adults struggling with addiction (Bickel et al., 2015). Similarly, adolescents in three of the four classes might have benefitted when they were younger from work from Diamond and colleagues from the “Tools of the Mind” curriculum, which targets teaching self-control in a naturalistic classroom setting (Diamond et al., 2019). Cognitive training programs, which tend to target WM or attention, may perhaps be more effective in enhancing functioning in youth who display weak PS (Schiff et al., 2021; Sonuga-Barke et al., 2014), enabling them to more rapidly perceive and act on information to guide their general behavior. It remains to be seen if targeting these narrower cognitive processes will generalize to more broad functions, including improving emotional reactivity and self-control when youth encounter seductive, immediately available rewards or are in intensely emotional situations. Researchers should also consider possible moderators and mediators to help develop personalized prevention and intervention approaches that consider biological factors (e.g., sex, hormones) and state factors (e.g., stress, sleep, type of reward [social, non-social, food, monetary]) when developing approaches for ADHD.
Future research directions include examining how these classes relate to brain function and structure. This includes more research on sex differences in relation to distinguishing between the different profiles. Although ADHD is more commonly diagnosed in males than females, recent research has suggested that females with ADHD may present differently than males, with potentially different patterns of symptoms, comorbidities, and functional impairments (Danielson et al., 2018; Skogli et al., 2013; Willcutt et al., 2012). More research on sex differences in ADHD could help refine diagnostic criteria and treatment approaches for both males and females with ADHD. Finally, exploring if these same classes are evident in adult samples will be valuable.
Limitations
This study had a relatively low sample size for a latent class approach; therefore, we had limited power to detect smaller subgroups or groups that were not well separated. This limitation impacts the generalizability of our findings to children and adolescents with ADHD. Larger studies with adequate power are needed to identify subtypes reliably. However, findings from studies with smaller sample sizes, such as ours, can still be informative and function as a foundation to guide future hypotheses. Studies with modest sample sizes often benefit from a more comprehensive, thorough characterization with multiple measures. They can also serve as a launching pad to explore more intricate phenotypes with greater depth in larger data sets. Many of the larger data sets available lack the range of measures that this project encompasses, thereby providing a richer and more comprehensive understanding of ADHD. The insights gained from this study not only contribute to the refinement of research questions but also offer valuable guidance for selecting future measures, ensuring a more nuanced investigation of ADHD symptoms. A consideration with our sample is that youth meeting the criteria for diagnoses of depression or major anxiety disorders (i.e., not phobias) were excluded from the study, thus limiting the generalization of our ADHD sample to the general ADHD population. Many of our youth, however, did endorse depressive or anxious symptoms, though insufficient to meet diagnostic criteria. Finally, while the study measures are widely used in research and clinical practice, we recognize that many are parent or self-report measures (i.e., CPRS-3, ZTPI, BIS) and are subject to shared method variance.
Conclusion
In summary, our study provides evidence of distinct ADHD symptom classes in relation to emotionality, impulsivity, self-control, risk-taking, and PS in adolescents with and without ADHD. These findings could assist clinicians in identifying youth who display greater differences in ADHD and emotional symptoms, potentially aiding in the development of more effective interventions for difficulties with emotional regulation, attention, hyperactivity, and impulsivity. Our findings suggest a potential rationale for investigating the effectiveness of ADHD interventions personalized to the unique needs of individuals based on their ADHD class.
Financial Disclosures
Dr. Hinshaw receives book royalties from Guilford Press, Oxford University Press and St. Martin’s Press. Dr. Iosif has received honoraria for reviewing activities from Elsevier. Ms. Elahi, Drs. Mukherjee and Schweitzer report no competing interests.
Data Availability
Data is available upon request.
References
Antonini, T. N., Becker, S. P., Tamm, L., & Epstein, J. N. (2015). Hot and cool executive functions in dhildren with attention-deficit/hyperactivity disorder and comorbid oppositional defiant disorder. Journal of the International Neuropsychological Society, 21(8), 584–595. https://doi.org/10.1017/S1355617715000752
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
Arnett, A. B., & Flaherty, B. P. (2022). A framework for characterizing heterogeneity in neurodevelopmental data using latent profile analysis in a sample of children with ADHD. Journal of Neurodevelopmental Disorders, 14(1), 45. https://doi.org/10.1186/s11689-022-09454-w
Baddeley, A., & Hitch, G. (1974). Working memory. Psychology of Learning and Motivation, 8, 47–89. https://doi.org/10.1016/j.cub.2009.12.014
Bandeen-Roche, K., Miglioretti, D. L., Zeger, S. L., & Rathouz, P. J. (1997). Latent variable regression for multiple discrete outcomes. Journal of the American Statistical Association, 92(440), 1375–1386. https://doi.org/10.1176/appi.books.9780890425596
Barkley, R. A. (Ed.). (2015). Attention-deficit hyperactivity disorder: A handbook for diagnosis and treatment (4th Ed.). The Guilford Press.
Barkley, R. A. (2013). Distinguishing sluggish cognitive tempo from ADHD in children and adolescents: Executive functioning, impairment, and comorbidity. Journal of Clinical Child & Adolescent Psychology, 42(2), 161–173. https://doi.org/10.1080/15374416.2012.734259
Barkley, R. A., Murphy, K. R., & Fischer, M. (2008). ADHD in Adults: What the Science Says. Guilford Press.
Barnhart, W. R., & Buelow, M. T. (2017). Assessing impulsivity: Relationships between behavioral and self-report measures in individuals with and without self-reported ADHD. Personality and Individual Differences, 106, 41–45.
Bickel, W. K., Quisenberry, A. J., Moody, L., & Wilson, A. G. (2015). Therapeutic opportunities for self-control repair in addiction and related disorders: Change and the limits of change in trans-disease processes. Clinical Psychological Science: A Journal of the Association for Psychological Science, 3(1), 140–153. https://doi.org/10.1177/2167702614541260
Brotman, M. A., Kircanski, K., Stringaris, A., Pine, D. S., & Leibenluft, E. (2017). Irritability in Youths: A Translational Model. The American Journal of Psychiatry, 174(6), 520–532. https://doi.org/10.1176/appi.ajp.2016.16070839
Castellanos, F. X., Sonuga-Barke, E. J. S., Milham, M. P., & Tannock, R. (2006). Characterizing cognition in ADHD: Beyond executive dysfunction. Trends in Cognitive Sciences, 10(3), 117–123. https://doi.org/10.1016/j.tics.2006.01.011
Chhabildas, N., Pennington, B. F., & Willcutt, E. G. (2001). A comparison of the neuropsychological profiles of the DSM-IV subtypes of ADHD. Journal of Abnormal Child Psychology, 29(6), 529–540.
Daniel, T. O., Said, M., Stanton, C. M., & Epstein, L. H. (2015). Episodic future thinking reduces delay discounting and energy intake in children. Eating Behaviors, 18, 20–24. https://doi.org/10.1016/j.eatbeh.2015.03.006
Danielson, M. L., Bitsko, R. H., Ghandour, R. M., Holbrook, J. R., Kogan, M. D., & Blumberg, S. J. (2018). Prevalence of Parent-Reported ADHD Diagnosis and Associated Treatment Among U.S. Children and Adolescents, 2016. Journal of clinical child and adolescent psychology : the official journal for the Society of Clinical Child and Adolescent Psychology, American Psychological Association, Division 53, 47(2), 199–212. https://doi.org/10.1080/15374416.2017.1417860
Diamond, A., Lee, C., Senften, P., Lam, A., & Abbott, D. (2019). Randomized control trial of tools of the mind: Marked benefits to kindergarten children and their teachers. PLoS ONE, 14(9), e0222447. https://doi.org/10.1371/journal.pone.0222447
Elliott, B. L., D’Ardenne, K., Mukherjee, P., Schweitzer, J. B., & McClure, S. M. (2022). Limbic and executive meso- and nigrostriatal tracts predict impulsivity differences in attention-deficit/hyperactivity disorder. Biological Psychiatry. Cognitive Neuroscience and Neuroimaging, 7(4), 415–423. https://doi.org/10.1016/j.bpsc.2021.05.002
Ernst, M. (2014). The triadic model perspective for the study of adolescent motivated behavior. Brain and Cognition, 89, 104–111. https://doi.org/10.1016/j.bandc.2014.01.006
Fassbender, C., Schweitzer, J. B., Cortes, C. R., Tagamets, M. A., Windsor, T. A., Reeves, G. M., & Gullapalli, R. (2011). Working Memory in Attention Deficit/Hyperactivity Disorder is Characterized by a Lack of Specialization of Brain Function. PLoS ONE, 6(11), e27240. https://doi.org/10.1371/journal.pone.0027240
Hinshaw, S. P., Owens, E. B., Zalecki, C., Huggins, S. P., Montenegro-Nevado, A. J., Schrodek, E., & Swanson, E. N. (2012). Prospective follow-up of girls with attention-deficit/hyperactivity disorder into early adulthood: Continuing impairment includes elevated risk for suicide attempts and self-injury. Journal of Consulting and Clinical Psychology, 80(6), 1041–1051. https://doi.org/10.1037/a0029451
Kahle, S., Mukherjee, P., Dixon, J. F., Leibenluft, E., Hinshaw, S. P., & Schweitzer, J. B. (2021). Irritability predicts hyperactive/impulsive symptoms across adolescence for females. Research on Child and Adolescent Psychopathology, 49(2), 185–196. https://doi.org/10.1007/s10802-020-00723-7
Kasper, L. J., Alderson, R. M., & Hudec, K. L. (2012). Moderators of working memory deficits in children with attention-deficit/hyperactivity disorder (ADHD): A meta-analytic review. Clinical Psychology Review, 32(7), 605–617. https://doi.org/10.1016/j.cpr.2012.07.001
Kofler, M. J., Irwin, L. N., Soto, E. F., Groves, N. B., Harmon, S. L., & Sarver, D. E. (2019). Executive functioning heterogeneity in pediatric ADHD. Journal of Abnormal Child Psychology, 47(2), 273–286. https://doi.org/10.1007/s10802-018-0438-2
Kofler, M. J., Rapport, M. D., Bolden, J., Sarver, D. E., Raiker, J. S., & Alderson, R. M. (2011). Working memory deficits and social problems in children with ADHD. Journal of Abnormal Child Psychology, 39(6), 805–817. https://doi.org/10.1007/s10802-011-9492-8
Leibenluft, E., Cohen, P., Gorrindo, T., Brook, J. S., & Pine, D. S. (2006). Chronic versus episodic irritability in youth: A community-based, longitudinal study of clinical and diagnostic associations. Journal of Child and Adolescent Psychopharmacology, 16(4), 456–466. https://doi.org/10.1089/cap.2006.16.456
Lejuez, C. W., Read, J. P., Kahler, C. W., Richards, J. B., Ramsey, S. E., Stuart, G. L., Strong, D. R., & Brown, R. A. (2002). Evaluation of a behavioral measure of risk taking: The Balloon Analogue Risk Task (BART). Journal of Experimental Psychology. Applied, 8(2), 75–84. https://doi.org/10.1037//1076-898x.8.2.75
Lenroot, R. K., & Giedd, J. N. (2010). Sex differences in the adolescent brain. Brain and Cognition, 72(1), 46–55. https://doi.org/10.1016/j.bandc.2009.10.008
Lo, Y., Mendell, N. R., & Rubin, D. B. (2001). Testing the number of components in a normal mixture. Biometrika, 88(3), 767–778.
Luo, Y., Weibman, D., Halperin, J. M., & Li, X. (2019). A Review of Heterogeneity in Attention Deficit/Hyperactivity Disorder (ADHD). Frontiers in Human Neuroscience, 13, 42. https://doi.org/10.3389/fnhum.2019.00042
Maedgen, J. W., & Carlson, C. L. (2000). Social functioning and emotional regulation in the attention deficit hyperactivity disorder subtypes. Journal of Clinical Child Psychology, 29(1), 30–42. https://doi.org/10.1207/S15374424jccp2901_4
Masyn, K. E. (2013). Latent class analysis and finite mixture modeling. Oxford University Press. https://doi.org/10.1093/oxfordhb/9780199934898.013.0025
Mukherjee, P., Hartanto, T., Iosif, A.-M., Dixon, J. F., Hinshaw, S. P., Pakyurek, M., van den Bos, W., Guyer, A. E., McClure, S. M., Schweitzer, J. B., & Fassbender, C. (2021). Neural basis of working memory in ADHD: Load versus complexity. NeuroImage: Clinical, 30, 102662. https://doi.org/10.1016/j.nicl.2021.102662
Mukherjee, P., Vilgis, V., Rhoads, S., Chahal, R., Fassbender, C., Leibenluft, E., Dixon, J. F., Pakyurek, M., van den Bos, W., Hinshaw, S. P., Guyer, A. E., & Schweitzer, J. B. (2022). Associations of irritability with functional connectivity of amygdala and nucleus accumbens in adolescents and young adults with ADHD. Journal of Attention Disorders, 26(7), 1040–1050. https://doi.org/10.1177/10870547211057074
Muthén, K. L., Muthén, B. O. (1987-2017). Mplus User's Guide. Eight Edition. Los Angeles, CA: Muthén & Muthén.
Nigg, J. T. (2017). Annual Research Review: On the relations among self-regulation, self-control, executive functioning, effortful control, cognitive control, impulsivity, risk-taking, and inhibition for developmental psychopathology. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 58(4), 361–383. https://doi.org/10.1111/jcpp.12675
Nigg, J. T. (2022). Parsing ADHD with temperament traits. Current Directions in Psychological Science, 31(4), 324–332. https://doi.org/10.1177/09637214221098079
Nigg, J. T., Goldsmith, H. H., & Sachek, J. (2004). Temperament and Attention Deficit Hyperactivity Disorder: The development of a multiple pathway model. Journal of Clinical Child & Adolescent Psychology, 33(1), 42–53. https://doi.org/10.1207/S15374424JCCP3301_5
Nigg, J. T., Gustafsson, H. C., Karalunas, S. L., Ryabinin, P., McWeeney, S. K., Faraone, S. V., Mooney, M. A., Fair, D. A., & Wilmot, B. (2018). Working memory and vigilance as multivariate endophenotypes related to common genetic risk for Attention-Deficit/Hyperactivity Disorder. Journal of the American Academy of Child & Adolescent Psychiatry, 57(3), 175–182. https://doi.org/10.1016/j.jaac.2017.12.013
Nylund, K. L., Asparouhov, T., & Muthén, B. O. (2007). Deciding on the number of classes in latent class analysis and growth mixture modeling: A Monte Carlo simulation study. Structural Equation Modeling: A Multidisciplinary Journal, 14(4), 535–569.
Polderman, T. J. C., Boomsma, D. I., Bartels, M., Verhulst, F. C., & Huizink, A. C. (2010). A systematic review of prospective studies on attention problems and academic achievement: Attention problems and academic achievement. Acta Psychiatrica Scandinavica, 122(4), 271–284. https://doi.org/10.1111/j.1600-0447.2010.01568.x
Ramos, A. A., Hamdan, A. C., & Machado, L. (2020). A meta-analysis on verbal working memory in children and adolescents with ADHD. The Clinical neuropsychologist, 34(5), 873–898. https://doi.org/10.1080/13854046.2019.1604998
Rapport, M. D., Alderson, R. M., Kofler, M. J., Sarver, D. E., Bolden, J., & Sims, V. (2008). Working memory deficits in boys with attention-deficit/hyperactivity disorder (ADHD): The contribution of central executive and subsystem processes. Journal of Abnormal Child Psychology, 36(6), 825–837. https://doi.org/10.1007/s10802-008-9215-y
Rosch, K. S., Mostofsky, S. H., & Nebel, M. B. (2018). ADHD-related sex differences in fronto-subcortical intrinsic functional connectivity and associations with delay discounting. Journal of Neurodevelopmental Disorders, 10(1), 34. https://doi.org/10.1186/s11689-018-9254-9
Rubia, K., Smith, A., & Taylor, E. (2007). Performance of children with attention deficit hyperactivity disorder (ADHD) on a test battery of impulsiveness. Child Neuropsychology, 13(3), 276–304. https://doi.org/10.1080/09297040600770761
Rubin, D. (1987). Multiple imputation for nonresponse in surveys. Wiley.
Rucklidge, J. J., & Tannock, R. (2002). Neuropsychological profiles of adolescents with ADHD: Effects of reading difficulties and gender. Journal of Child Psychology and Psychiatry, 43(8), 988–1003. https://doi.org/10.1111/1469-7610.00227
Schiff, S., Egglefield, D. A., Motter, J. N., Grinberg, A., Rushia, S. N., Rutherford, B. R., & Sneed, J. R. (2021). Who benefits from computerized cognitive training? Lower processing speed predicts greater cognitive improvement. Journal of Affective Disorders Reports, 5, 100149. https://doi.org/10.1016/j.jadr.2021.100149
Schweitzer, J. B., Hanford, R. B., & Medoff, D. R. (2006). Working memory deficits in adults with ADHD: Is there evidence for subtype differences. Behavioral and Brain Functions, 2(1), 43. https://doi.org/10.1186/1744-9081-2-43
Schweitzer, J. B., & Sulzer-Azaroff, B. (1988). Self-control: Teaching tolerance for delay in impulsive children. Journal of the Experimental Analysis of Behavior, 50(2), 173–186. https://doi.org/10.1016/j.jadr.2021.100149
Schweitzer, J. B., & Sulzer-Azaroff, B. (1995). Self-control in boys with attention deficit hyperactivity disorder: Effects of added stimulation and time. Journal of Child Psychology and Psychiatry, 36(4), 671–686. https://doi.org/10.1111/j.1469-7610.1995.tb02321.x
Shaw, P., Eckstrand, K., Sharp, W., Blumenthal, J., Lerch, J. P., Greenstein, D., Clasen, L., Evans, A., Giedd, J., & Rapoport, J. L. (2007). Attention-deficit/hyperactivity disorder is characterized by a delay in cortical maturation. Proceedings of the National Academy of Sciences of the United States of America, 104(49), 19649–19654. https://doi.org/10.1073/pnas.0707741104
Shaw, P., Stringaris, A., Nigg, J., & Leibenluft, E. (2014). Emotion dysregulation in attention deficit hyperactivity disorder. American Journal of Psychiatry, 171(3), 276–293. https://doi.org/10.1176/appi.ajp.2013.13070966
Sircova, A., van de Vijver, F. J. R., Osin, E., Milfont, T. L., Fieulaine, N., Kislali-Erginbilgic, A., Zimbardo, P. G., Djarallah, S., Chorfi, M. S., Leite, U. do R., Lin, H., Lv, H., Bunjevac, T., Tomaš, T., Punek, J., Vrlec, A., Matić, J., Bokulić, M., Klicperová-Baker, M., … Boyd, J. N. (2014). A global look at time: A 24-country study of the equivalence of the zimbardo time perspective inventory. SAGE Open, 4(1). https://doi.org/10.1177/2158244013515686
Skogli, E. W., Andersen, P. N., Hovik, K. T., & Øie, M. (2017). Development of hot and cold executive function in boys and girls with ADHD: A 2-year longitudinal study. Journal of Attention Disorders, 21(4), 305–315. https://doi.org/10.1177/1087054714524984
Skogli, E. W., Teicher, M. H., Andersen, P. N., Hovik, K. T., & Øie, M. (2013). ADHD in girls and boys – gender differences in co-existing symptoms and executive function measures. BMC Psychiatry, 13(1), 298. https://doi.org/10.1186/1471-244X-13-298
Solanto, M. V., & Scheres, A. (2021). Feasibility, acceptability, and effectiveness of a new cognitive-behavioral intervention for college students with ADHD. Journal of Attention Disorders, 25(14), 2068–2082. https://doi.org/10.1177/1087054720951865
Sonuga-Barke, E., Bitsakou, P., & Thompson, M. (2010). Beyond the dual pathway model: Evidence for the dissociation of timing, inhibitory, and delay-related impairments in Attention-Deficit/Hyperactivity Disorder. Adolescent Psychiatry, 49(4).
Sonuga-Barke, E., Brandeis, D., Holtmann, M., & Cortese, S. (2014). Computer-based cognitive training for ADHD. Child and Adolescent Psychiatric Clinics of North America, 23(4), 807–824.
Stringaris, A., Goodman, R., Ferdinando, S., Razdan, V., Muhrer, E., Leibenluft, E., & Brotman, M. A. (2012). The affective reactivity index: A concise irritability scale for clinical and research settings. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 53(11), 1109–1117. https://doi.org/10.1111/j.1469-7610.2012.02561
Tamm, L., Loren, R. E. A., Peugh, J., & Ciesielski, H. A. (2021). The association of executive functioning with academic, behavior, and social performance ratings in children with ADHD. Journal of Learning Disabilities, 54(2), 124–138. https://doi.org/10.1177/0022219420961338
Van Cauwenberge, V., Sonuga-Barke, E. J. S., Hoppenbrouwers, K., Van Leeuwen, K., & Wiersema, J. R. (2015). “Turning down the heat”: Is poor performance of children with ADHD on tasks tapping “hot” emotional regulation caused by deficits in “cool” executive functions? Research in Developmental Disabilities, 47, 199–207. https://doi.org/10.1016/j.ridd.2015.09.012
van den Bos, W., Rodriguez, C. A., Schweitzer, J. B., & McClure, S. M. (2015). Adolescent impatience decreases with increased frontostriatal connectivity. Proceedings of the National Academy of Sciences, 112(29). https://doi.org/10.1073/pnas.1423095112
Visser, S. N., Danielson, M. L., Bitsko, R. H., Holbrook, J. R., Kogan, M. D., Ghandour, R. M., Perou, R., & Blumberg, S. J. (2014). Trends in the parent-report of health care provider-diagnosed and medicated attention-deficit/hyperactivity disorder: United States, 2003–2011. Journal of the American Academy of Child & Adolescent Psychiatry, 53(1), 34-46.e2. https://doi.org/10.1016/j.jaac.2013.09.001
Willcutt, E. G., Doyle, A. E., Nigg, J. T., Faraone, S. V., & Pennington, B. F. (2005). Validity of the executive function theory of attention-deficit/hyperactivity disorder: A meta-analytic review. Biological Psychiatry, 57(11), 1336–1346. https://doi.org/10.1016/j.biopsych.2005.02.006
Willcutt, E. G., Nigg, J. T., Pennington, B. F., Solanto, M. V., Rohde, L. A., Tannock, R., Loo, S. K., Carlson, C. L., McBurnett, K., & Lahey, B. B. (2012). Validity of DSM-IV attention deficit/hyperactivity disorder symptom dimensions and subtypes. Journal of Abnormal Psychology, 121(4), 991–1010. https://doi.org/10.1037/a0027347
Zimbardo, P. G., & Boyd, J. N. (1999). Putting time in perspective: A valid, reliable individual-differences metric. Journal of Personality and Social Psychology, 77(6), 1271–1288.
Acknowledgements
We would like to acknowledge the kind support of all our research participants and their families, as well as several research coordinators, staff, and colleagues who provided assistance or input, including Jared Borden, Lauren Boyle, Maria B.E. Bradshaw, Catrina A. Calub, Erin Calfee, Laurel Cavallo, Linda Chen, William Elms, Ian Farnsworth, Catherine Fassbender, Taddeus Arthur Hartanto, Samuel M. McClure, Jessica Nguyen, Juan Ramos, Steven J. Riley, Ellen Leibenluft, Wouter van den Bos, and J. Faye Dixon.
Funding
This work was supported by the National Institutes of Health grants R01 MH091068 (Schweitzer), U54 HD079125 (Abbeduto), and P50 MH106438 (Carter).
Author information
Authors and Affiliations
Contributions
Heather Elahi, M.A. Conceptualization, Investigation, Writing—original draft. Ana-Maria Iosif, Ph.D. Conceptualization, Methodology, Formal analysis, Data curation, Investigation, Writing—original draft, Visualization. Prerona Mukherjee, Ph.D. Conceptualization, Methodology, Investigation, Writing—original draft, Project administration, Supervision. Stephen P. Hinshaw, Ph.D. Conceptualization, Methodology, Supervision of analysis, Writing – Editing. Julie Schweitzer, Ph.D. Conceptualization, Methodology, Supervision of Formal analysis, Investigation, Writing—original draft, Project administration, Resources (including clinical staff) Supervision, Funding acquisition.
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Elahi, H., Iosif, AM., Mukherjee, P. et al. Using Hot and Cool Measures to Phenotype and Predict Functional Outcomes Across Dimensions of ADHD and Typical Development in Adolescents. Res Child Adolesc Psychopathol 52, 579–593 (2024). https://doi.org/10.1007/s10802-023-01149-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10802-023-01149-7