
Abstract
Introduction
With high increase in myopia prevalence, we aimed to assess whether Plusoptix_A09 can be used in myopic children over spectacles to predict visual acuity (VA) and myopic refraction changes.
Methods
Myopic children underwent a complete ophthalmological examination. Plusoptix_A09 was performed over spectacles. VA changes, refraction changes and time since previous glasses prescription, were determined. Age, current or past history of amblyopia, presence of strabismus and self-perception of VA changes were registered.
Results
In total, 199 patients were included. Spherical power (SP) and spherical equivalent (SE) measured by Plusoptix_A09 over spectacles predicted both VA changes (p < 0.001) and refraction changes (p < 0.001). Values of SP < − 0.06D or SE < − 0.22D indicated a VA decrease (AUC > 0.9, p < 0.01) for sensitivity and specificity of 85.1%, 82.1% and 82.6%, 83.3%, respectively. Age and ophthalmological comorbidities did not influence Plusoptix_A09 measurements (p > 0.05). Plusoptix_A09 over spectacles was a stronger predictor of VA changes when compared to children's self-perception, either in 4–9-year-old patients (p < 0.001 versus p = 0.628) and in 10–18-year-old children (OR < = 0.066 versus OR = 0.190). A decrease in SP and SE of − 0.10D in Plusoptix_A09 predicted a myopia progression of − 0.04D and − 0.05D, respectively.
Conclusion/Relevance
This study unveiled new features for the Plusoptix, a worldwide available photoscreener used in amblyopia screening. When Plusoptix is performed in children with their glasses on, it can rapidly predict myopia progression. For each decrease of − 0.10D in Plusoptix, a myopia progression of -0.05D is expected. Moreover, Plusoptix is more reliable than children's self-perception of visual acuity changes, making it a useful tool either in primary care or ophthalmology practice
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Myopia is continuously progressive affecting the refraction needed to reach the best-corrected visual acuity (BCVA) [1]. It is clear that myopic children who require refractive correction with glasses should be frequently reevaluated to assess myopia and VA progression [2].
Plusoptix_A09 photorefractor is a noninvasive, handheld and easy-to-use device that performs binocular real-time videoretinoscopy of reflected infrared light in order to rapidly identify refractive errors (RE) in children [3]. It measures refractive data, pupil size, interpupillary distance, asymmetry of the corneal reflexes and gaze deviation without the need to perform cycloplegia [4, 5]. During examination, Plusoptix is placed approximately 1 m from the patient and then the device produces noises and flashing lights to fix child’s gaze and the respective measurements are obtained [4]. During its standard use, children are not using any type of refractive correction [4]. The effectiveness of noncycloplegic autorefraction with Plusoptix in detecting myopia, astigmatism and anisometropia has been extensively studied, and it is reliable when compared to cycloplegic autorefraction and retinoscopy (it has lower acuity in the detection of hyperopia, though) [6]. Moreover, it has also been demonstrated that photoscreening with Plusoptix is similar to traditional chart-based screening in the detection of VA impairment and the need for glasses or a new intervention in school-age children [7].
Although Plusoptix has proven to be useful in detecting both RE and VA impairment when performed in children without correction, to our knowledge, there are no studies on the performance of Plusoptix over spectacles and its potentials as a follow-up tool in myopic children.
The purpose of this study is to evaluate the performance of PLUSOPTIX_A09 in predicting VA and myopia changes in children over their spectacles. Furthermore, we assessed whether individual and eye-related factors influence the performance of PLUSOPTIX_A09: In addition to age, which has shown to have an impact in VA progression [8], the presence of past and current history of amblyopia and the time since last glasses prescription were also included for analysis. Although the use of the photoscreener without correction is limited in children with strabismus [9], some strabismus can be totally or partially controlled with the glasses on [10], making it possible to perform a binocular measurement with the PLUSOPTIX_A09. To evaluate its influence in the PLUSOPTIX_A09 measurements, the presence of strabismus was also considered for analysis.
Materials and methods
All myopic children wearing glasses, aged 4–18 years old, that attended an ophthalmology consultation between February 2020 and May 2021, in whom PLUSOPTIX_A09 was performed over their spectacles, were included. PLUSOPTIX_A09 measurements were always taken with the children wearing their current spectacles (there are no Plusoptix measurements without glasses in this work), and for that reason the expression “PLUSOPTIX_A09” in this study always refers to measurements done over current spectacles. Measurements using the Plusoptix_A09 were taken with the child wearing glasses, at the distance similar to that used for children without glasses. These measurements were taken binocularly, focusing solely on Plusoptix_A09. In cases where reflections occurred, adjustments were made by slightly rotating the child's head to ensure accurate measurements.
Plusoptix is developed and manufactured by Plusoptix GmbH, in Nuremberg, Germany. All Plusoptix devices use the measuring principle of the transillumination test; however, they avoid glare by using infrared light. The device records camera images of the illuminated pupils and measures the refraction.
Myopia or myopic astigmatism was considered present when spherical equivalent (SE) < = -0.50D and values of the spherical power (SP) < = zero [11]. All consecutive participants underwent complete ophthalmological examination performed by an experienced pediatric ophthalmologist.
Exclusion criteria were: Whenever binocular evaluation with PLUSOPTIX_A09 over spectacles was not possible (large-angle strabismus not corrected with spectacles, ptosis, corneal opacities and poor ocular fixation); RE exceeding the range of PLUSOPTIX_A09 (− 7.00D to + 5.00D); noncooperative children; inadequate clinical records.
Information collected from the electronic clinical database was: Age; Gender; Presence of current and past history of amblyopia; Presence and type of strabismus; Prescription of current glasses; Self-perception of VA changes (later described in this section); VA with correction (VAwc), which refers to patient’s VA with current glasses; Time since current glasses prescription; The average of two binocular measurements with the PLUSOPTIX_A09 (of SP, cylinder power (CP) and SE); BCVA that indicates the best-corrected visual acuity that could be achieved with a new refraction; Refractive errors obtained from subjective refraction and cycloplegic autorefraction (after instillation of 3 drops of cyclopentolate 1.0% in each eye, with 10-min interval, followed by autorefractometer, either KOWA KW-2000® or HUVITZ HRK-8000A®, measurement after 40 min).
VA was evaluated monocularly either with single surrounded thumbling E or numbers chart displayed in MediWorks C901® video system. VA was recorded in decimal notation and computed into LogMAR VAwc and LogMAR BCVA [12]. [LogMAR BCVA–LogMAR VAwc] indicates the lines of VA the patient is away from reaching the best VA possible. Since a VA test–retest variability within 0.1 LogMAR can occur [13], a new categorical dichotomic variable was established—VA status: stable VA: 0 ≤ [LogMAR BCVA–LogMAR VAwc] ≤ 0.1 LogMAR versus decreased VA: [LogMAR BCVA–LogMAR VAwc] > 0.1LogMAR.
When new refraction was different from current glasses, a new prescription of glasses was obtained, considering cycloplegic autorefraction and subjective refraction. To quantify RE progression, a new continuous variable was created: refraction changes, which corresponded to the difference between new refraction (new glasses prescription) and current refraction (previous glasses prescription) for the SP, CP and SE.
To evaluate self-perception of VA changes, children were asked “Do you think you still have a good vision with your glasses?” and answers of “yes” or “no” were registered.
In this work, reports refer to the analysis of the right eye (or left eye when the right eye was emmetrope) [14].
This project was approved by the local ethics committee.
Statistical analysis
To compare PLUSOPTIX_A09 measurements, age and time since previous glasses prescription between groups of VA status independent samples t test or Mann–Whitney U test (nonparametric alternative) were used; effect size: Cohen’s d [small 0.2, medium 0.5, large 0.8 [15]]. Pearson’s Chi-square test was performed to assess differences in the presence of ophthalmological abnormalities between groups of VA status; effect size: phi/crammer’s V [small 0.1, medium 0.3, large 0.5 [15]]. A univariate logistic regression model was estimated to assess whether PLUSOPTIX_A09 predicted VA changes. A multivariate logistic regression analysis was used to study the influence of age, time since previous prescription and the presence of ophthalmological abnormalities in the predictive power of PLUSOPTIX_A09. Since no evidence or guidelines concerning the performance of Plusoptix in children with glasses have yet been published, a receiver operating characteristic (ROC) curve analysis was performed in order to calculate cutoff points for PLUSOPTIX_A09 measurements over spectacles to identify children with stable and decreased VA [16]. To evaluate whether PLUSOPTIX_A09 were predictors of refraction changes, the following criteria were used: Pearson’s correlation coefficient and Spearman's rank correlation coefficient were calculated to assess the correlation between both measurements (when significant, Pearson’s coefficient was reported [small 0.1, medium 0.3, large 0.5 [15]); then, the PLUSOPTIX_A09 measurements that significantly correlated with refraction changes were included in a simple linear regression to assess whether PLUSOPTIX_A09 predicted refraction changes and to determine its predictive power. Pearson’s Chi-square test of independence was used to study the association between children’s self-perception of VA changes and the presence of VA changes in at least one eye detected during medical examination; effect size was phi [small 0.1, medium 0.3, large 0.5 [15]]. For this analysis, subjects were divided into two age groups: the 4–9 year old and the 10–18 year old. Then, to compare the predictive powers of the PLUSOPTIX_A09 measurements with self-perception of VA changes, the univariate logistic regression model was used to calculate the odds ratio (OR). The statistical analyses were performed using the Statistical Package for the Social Sciences (IBM SPSS®), version 27.0. Two-sided p-values < 0.05 with confidence interval (CI) of 95% were considered statistically significant.
Results
A total of 199 participants were included; 109 females (54.8%); mean age of 10.8 years old (SD = 3.2). Nineteen patients (9.5%) had past history of amblyopia, and 2 children (1%) had current history of amblyopia. Strabismus was present in 10 subjects (5%): 3 (1.5%) with esotropia and 7 (3.5%) with exotropia. The median time since previous prescription was 13.0 months (IR = 10.0). Of the total sample, 121 (60.8%) children had stable VA and 78 (39.2%) had decreased VA with current glasses.
Prediction of VA status (stable versus decreased VA)
Regarding VA status, PLUSOPTIX_A09 measurements were significantly different for SP and SE [+ 0.35 ± 0.53D versus − 0.98 ± 0.92D, t(110) = 11.58, p < 0.001, d = 1.87; and + 0.13 ± 0.51D versus − 1.21 ± 0.91D, t(108) = 11.80, p < 0.001, d = 1.92, respectively], but not for CP [p = 0.980].
As shown in Table 1, both the SP and SE measurements with PLUSOPTIX_A09 were significant independent predictors of VA changes and, in the adjusted model, their ORs even improved. Time since previous prescription was a weaker predictor than PLUSOPTIX_A09 measurements. Age, history of strabismus and amblyopia were nonsignificant in predicting VA status in the multivariate analysis (Table 1).
The ROC curve analysis showed significant predictive power of both PLUSOPTIX_A09 measurements in detecting VA changes (AUC > 0.9, p < 0.01). These results suggest that a value of SP or SE measured by PLUSOPTIX_A09 worse (more negative) than -0.06D or -0.22D, respectively, indicated that children with myopia or myopic astigmatism had decreased VA with current glasses, with a sensitivity and specificity of 85.1% and 82.1% for SP and 82.6% and 83.3% for SE (Fig. 1).

ROC curve of the performance of Plusopotix_A09 SP (left graph) and SE (right graph) in detecting visual acuity changes in children with myopia or myopic astigmatism. A value of SP or SE worse (more negative) than − 0.06D or − 0.22D, respectively, indicates a decreased VA with current glasses (sensitivity and specificity of 85.1% and 82.1% for SP and 82.6% and 83.3% for SE); AUC for SP = 0.904, 95%CI = 0.860–0.949, p < 0.01. AUC for SE = 0.910, 95%CI = 0.867–0.953, p < 0.01. Plusoptix_A09 measurements were taken over spectacles. Significant p-value (< 0.05). SP, spherical power; SE, spherical equivalent; AUC, area under the curve; CI, confidence interval.
Prediction of refraction changes
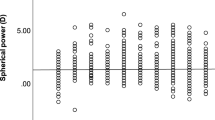
SP and SE measured with the PLUSOPTIX_A09 explained a significant amount of variance in refraction changes [SP: F(1,197) = 316.64, p < 0.001, R2 = 0.665; SE: F(1,197) = 390.21, p < 0.001, R2 = 0.665]. The regression coefficients indicated that a decrease in SP and SE of − 0.10D estimated by the PLUSOPTIX_A09 over spectacles predicted a myopia progression (a more negative SP and SE) of − 0.04D and -0.05D, respectively (SP: B = 0.418, 95%CI = 0.372–0.464; SE: B = 0.453, 95%CI = 0.408–0.498). Figure 2 illustrates the linear regression model between PLUSOPTIX_A09 measurements over spectacles and changes in the SP and SE detected during ophthalmological examination. Children with stable and decreased VA had similar CP measurements with the PS09 over spectacles [− 0.38 ± 0.31D vs. − 0.38 ± 0.38D, U = 4729.00, p = 0.980, r = 0.00].

Scatter plots illustrating the linear relationship between Plusoptix_A09 measurements over spectacles and changes in the spherical power (A) and in the spherical equivalent (B) detected during ophthalmological examination in children with myopia or myopic astigmatism. Plusoptix_A09 measurements were taken over spectacles. D, diopter. R2, R squared of linear regression
Children’s self-perception of VA changes
Self-perception of VA changes was assessed in 72 consecutive myopic patients. From those, 27 (37.5%) were 4–9 years old and 45 (62.5%) were 10–18 years old.
In the age group 4–9 years old there was no significant association between self-perception of VA changes and detected VA changes in at least one eye (p = 0.628 by Fisher’s exact test). However, results were considerably different in the age group 10–18 years old, where a significant association with a moderate effect size was found [Χ2(1, N = 72) = 5.993; p = 0.014; ɸ = − 0.365].
To compare whether PLUSOPTIX_A09 measurements or self-perception of VA changes are stronger predictors of VA changes, the univariate logistic regression model was used to calculate the ORs. For this analysis only 10–18-year-old children were considered, since prior analysis only found significant results for this age group. All variables were significant predictors of VA changes, although PLUSOPTIX_A09 measurements expressed stronger ORs when compared to children’s self-perception (Table 2).
Discussion
Refractive eye problems in children have become a global public health challenge with myopia alone being acknowledge as a growing epidemic [17, 18]. Therefore, reliable and affordable tools for monitoring myopia in children need to be developed [19].
Plusoptix is a worldwide available photoscreener, used by many pediatricians, primary care physicians and ophthalmologists [20], but has not yet been studied in children over their glasses. Thus, this is the first study, to our knowledge, to explore the potentials of the Plusoptix in children wearing spectacles. Our aim was to find new features for this extensively common photoscreener that could help ameliorate the increasing demand of specialized eye care [21].
VA changes
Based on our results, performing Plusoptix in myopic children over spectacles is an effective and easy-to-use method to rapidly identify a decrease in VA. Our results revealed that both SP and SE measured by PLUSOPTIX_A09 over spectacles are able to independently predict a decrease in VA with current glasses. As SP and SE get more negative, the odds of VA worsening significantly increase (OR = 0.061 for both SP and SE). Our ROC curve analysis of decreased versus stable VA suggests that more negative (more myopic) values of SP or SE indicate progression of myopia: For cutoffs of SP < − 0.06D and SE < − 0.22D, PLUSOPTIX_A09 over spectacles detects myopia progression with a sensitivity of 85.1% and 82.6% and a specificity of 82.1% and 83.3%, respectively. On the other hand, CP measured by PLUSOPTIX_A09 over spectacles does not predict a decrease in VA since CP is more stable over time.
As Plusoptix is an user-friendly device, it can be easily performed both at specialized and primary care levels [20, 22]. At a specialized level, the pediatric ophthalmologist can use the Plusoptix over spectacles as an initial screening tool to rapidly assess whether a myopic child has decreased their VA. At a primary care level, Plusoptix seems to be even more useful, especially because vision screening in this setting is time-consuming and has low reimbursement, besides many physicians report to be not adequately trained to perform VA testing [23]. By routinely performing Plusoptix in children over spectacles and considering the calculated cutoff points, physicians can easily and rapidly identify children who may require referral to update glasses prescription.
As expected, children with stable VA were older, since myopia gradually stabilizes with age [24]. Furthermore, children with stable VA also experienced longer time since previous glasses prescription. These patients might have slower progressing myopia [25], with a less often need to update their prescription. When assessing the influence of ophthalmological comorbidities, PLUSOPTIX_A09 remains a strong predictor of VA progression even in children with current or past history of amblyopia or with strabismus (OR = 0.047 for SP and OR = 0.048 for SE, in the adjusted model). This finding looks especially interesting, because although binocular measurements with Plusoptix cannot be performed without glasses in children with significant strabismus [9], we found that binocular measurements with the photoscreener can be made in strabismic children when strabismus can be corrected with the glasses on.
Refraction changes
Manifest refraction and cycloplegic refraction are the gold standards for lens prescription in children [26]. Therefore, PLUSOPTIX_A09 measurements over spectacles were compared to the refraction measurements obtained during ophthalmological examination. We observed that PLUSOPTIX_A09 measurements over spectacles of the SP and SE strongly correlated with the changes in SP and SE detected during examination.
Moreover, this study established a linear equation to predict refraction changes from Plusoptix measurements over spectacles in children with myopia and mixed astigmatism. Currently, refraction methods only calculate the refraction the child needs to achieve BCVA and do not directly estimate the difference from previous glass prescription [26]. Our results suggest that performing PLUSOPTIX_A09 in a child with their current glasses before subjective refraction could be very helpful, as it would be an easy and rapid procedure to indicate the practitioner if the child needs to update their glasses prescription while also quantifying the adjustment in refraction the child requires.
Children’s self-perception of VA changes
Assessing children’s self-perception of visual function during anamnesis is highly recommended [27]. Good association between self-report and presence of VA disorders in adolescents has been reported in other studies [28]. Our results suggest that although asking a 10–18-year-old child if they think they still have good vision with glasses is a reliable and easy way of screening a decrease in VA, PLUSOPTIX_A09 over spectacles is a better predictor of VA changes and should be preferred. Furthermore, we found that self-perception is not reliable in younger children (4–9 years old). We believe that self-perception is not reliable in younger children because self-perception is a subjective test, so it may be easier for older children to realize a decrease in VA. Moreover, self-report of vision impairment is limited in children with autism and intellectual disabilities [29]. In this population, Plusoptix seems to be a valuable alternative [30].
Limitations and future research
Regarding a possible selection bias, we believe that if it exists, it was of minor relevance, as almost all children surveyed during this period had measurements taken with Plusoptix. Nevertheless, it is not possible to completely rule out the presence of selection bias. When performing PLUSOPTIX_A09 over spectacles, glasses manufacturing, cleaning conditions and maintenance state can also influence PLUSOPTIX_A09 readings and interfere with the detection of RE progression. Moreover, although PLUSOPTIX_A09 nonmeasurable results have proven to be important in amblyopia screening [20], these cases were excluded from the study, since only 2 have had out-of-range results, limiting its inclusion in the statistical analysis. During ophthalmological evaluation, the examiner was not blinded for PLUSOPTIX_A09 over spectacles readings, which could have biased VA evaluation. Cycloplegia was performed in 72.0% of the patients with decreased VA. In the other 28.0%, glasses were prescribed according to subjective refraction findings (of those, only 7 patients required an adjustment in refraction greater than 0.50D). Subjective refraction is less sensitive in measuring RE, as it overestimates myopia [31]. In this study, PLUSOPTIX_A09 measurements over spectacles also overestimated myopia progression: A decrease in − 0.10D in the SP and SE measured with the PLUSOPTIX_A09 over spectacles only corresponded to a decrease in refraction of − 0.04D and − 0.05D, respectively. Therefore, not performing cycloplegia in every myopic child with decreased VA may have favored PLUSOPTIX_A09 measurements in this study. Finally, when assessing self-perception of VA changes, the question’s formulation may have biased the child to give a positive answer.
Future researches with children over glasses using other photoscreeners available in the market [32] should be done, as finding more effective devices would increase worldwide accessibility to photoscreening over spectacles.
Furthermore, this study concludes that a decrease in Plusoptix_A09 measurements predicts myopic changes in children wearing glasses. The changes we assessed were: a change in refraction and a change in visual acuity. Both are a sign of myopia progression. However, myopia progression can also be assessed by axial length that was not used in this study. Maybe in future studies axial length could be included.
In conclusion, this study unveiled new promising features for the Plusoptix, a worldwide available photoscreener. When PLUSOPTIX_A09 is performed in children with their glasses on, it can rapidly predict myopia progression, an increasing epidemic in ophthalmology. Values of SP < − 0.06D or SE < − 0.22D indicate VA has decreased, with high sensitivity and specificity. Furthermore, Plusoptix is more reliable than children’s self-perception of VA changes, in 4- to 18-year-old myopic children already wearing glasses. In a matter of seconds, both the ophthalmologist and the primary care clinician can quickly assess whether a patient's myopia has progressed, a method far more precise than asking the child if their vision has diminished.
This study strongly recommends Plusoptix to be routinely performed as an initial assessment in children with myopia, either in primary care or in ophthalmology practice.
References
Polling JR, Klaver C, Tideman JW (2021) Myopia progression from wearing first glasses to adult age: The DREAM Study. Br J Ophthalmol. 1–5.
J Zhao J Mao R Luo F Li SR Munoz LB Ellwein 2002 The progression of refractive error in school-age children: Shunyi district China Am J Ophthalmol 134 5 735 743
AH Dahlmann-Noor K Vrotsou V Kostakis J Brown J Heath A Iron 2009 Vision screening in children by Plusoptix Vision Screener compared with gold-standard orthoptic assessment Br J Ophthalmol 93 3 342 345
NS Matta EL Singman DI Silbert 2008 Performance of the Plusoptix vision screener for the detection of amblyopia risk factors in children J AAPOS 12 5 490 492
Manual I, Vision Screener plusoptiX S09. 2016;1–45.
M Fogel-Levin R Doron T Wygnanski-Jaffe O Ancri ZI Ben 2016 A comparison of plusoptiX A12 measurements with cycloplegic refraction J AAPOS 20 4 310 314 https://doi.org/10.1016/j.jaapos.2016.04.006
E Silverstein ER McElhinny 2020 Traditional and instrument-based vision screening in third-grade students J AAPOS 24 4 232.e1 232.e6 https://doi.org/10.1016/j.jaapos.2020.04.013
P Sankaridurg X He T Naduvilath M Lv A Ho E Smith 2017 Comparison of noncycloplegic and cycloplegic autorefraction in categorizing refractive error data in children Acta Ophthalmol 95 7 e633 e640
I Sanchez S Ortiz-Toquero R Martin V Juan de 2016 Advantages, limitations, and diagnostic accuracy of photoscreeners in early detection of amblyopia: a review Clin Ophthalmol 10 1365 1373
LA Ahmed HS Shimaa M Arafa S El-Sayed 2018 Intermittent exotropia, when to recommend glasses and when to perform surgery? Med J Cairo Univ 86 289 296
V Galvis A Tello PA Camacho LM Gómez JJ Rey AA Serrano 2021 Definition of refractive errors for research studies: Spherical equivalent could not be enough J Optom 14 2 224 225 https://doi.org/10.1016/j.optom.2020.10.003
JT Holladay 1997 Proper method for calculating average visual acuity J Refract Surg 13 4 388 391
JM Holmes RW Beck MX Repka DA Leske RT Kraker RC Blair 2001 The amblyopia treatment study visual acuity testing protocol Arch Ophthalmol 119 9 1345 1353
I Murdoch 1998 People and eyes: Statistics in ophthalmology Community Eye Heal J 11 27 43
Peter W (1988) Rules of thumb on magnitudes of effect sizes. MRC Cogn Brain Sci Unit, Univ Cambridge [Internet]. 2018;5(1988):0–4. Available from: http://imaging.mrc-cbu.cam.ac.uk/statswiki/FAQ/effectSize
B Sharma R Jain 2014 Right choice of a method for determination of cut-off values: A statistical tool for a diagnostic test Asian J Med Sci 5 3 30 34
J Flanagan T Fricke P Morjaria S Yasmin 2019 Myopia: a growing epidemic Community Eye Heal J 32 105 9 9
BA Holden TR Fricke DA Wilson M Jong KS Naidoo P Sankaridurg 2016 Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050 Ophthalmology 123 5 1036 1042 https://doi.org/10.1016/j.ophtha.2016.01.006
RPL Wisse MB Muijzer F Cassano DA Godefrooij YFDM Prevoo N Soeters 2019 Validation of an independent web-based tool for measuring visual acuity and refractive error via the MORE (manifest versus online refractive evaluation) trial: prospective open-label noninferiority clinical trial J Med Internet Res 21 11 2 3
S Guimarães A Soares P Costa E Silva 2019 How many Plusoptix S04 measures yield the most sensitive amblyopia screening? J Pediatr Ophthalmol Strabismus 56 5 305 312
LB Williams SG Prakalapakorn Z Ansari R Goldhardt 2020 Impact and trends in global ophthalmology Curr Ophthalmol Rep 8 3 136 143
Magalhães AA, Costa, Andreia Silva da Alexandre A, Tavares F, Ferreira GC, Lopes H, Murta JN, et al. (2018) Estratégia Nacional para a Saúde da Visão. Sns [Internet]. 1–126. Available from: https://www.sns.gov.pt/noticias/2018/06/26/estrategia-nacional-para-a-saude-da-visao/
TD Le RA Raashid L Colpa J Noble A Ali A Wong 2018 Paediatric vision screening in the primary care setting in Ontario Paediatr Child Heal 23 3 e33 e39
R Hardy A Hillis D Mutti R Stone C Taylor LM Dong 2013 Myopia stabilization and associated factors among participants in the correction of myopia evaluation trial (COMET) Investig Ophthalmol Vis Sci 54 13 7871 7883
DI Flitcroft M He JB Jonas M Jong K Naidoo K Ohno-Matsui 2019 IMI – Defining and classifying myopia: a proposed set of standards for clinical and epidemiologic studies Investig Ophthalmol Vis Sci 60 3 M20 30
Kolker R (2015) Refraction: subjective refraction and prescribing glasses. Rev B. 1–82. Available from: papers3://publication/uuid/DAB78AC8–779A-42B5-ADEB-869CDF3C198E
Direcção de Serviços de Cuidados de Saúde/Comissão de Coordenação do Programa Nacional para a Saúde da Visão. Boas Práticas em Oftalmologia - Elementos Clínicos de Avaliação e Referenciação. 2008;83.
V Tadić A Cooper P Cumberland G Lewando-Hundt JS Rahi 2013 Development of the functional vision questionnaire for children and young people with visual impairment: the FVQ-CYP Ophthalmology 120 12 2725 2732
M Butchart JJ Long M Brown A McMillan J Bain T Karatzias 2017 Autism and visual Impairment: a review of the literature Rev J Autism Dev Disord 4 2 118 131
E Singman N Matta A Fairward D Silbert 2013 Evaluation of plusoptiX photoscreening during examinations of children with autism Strabismus 21 2 103 105
H Hashemi M Khabazkhoob A Asharlous S Soroush AA Yekta N Dadbin 2016 Cycloplegic autorefraction versus subjective refraction: the Tehran eye study Br J Ophthalmol 100 8 1122 1127
RW Arnold AW Arnold MD Armitage JM Shen TEWT Hepler 2013 Pediatric photoscreeners in high risk patients 2012 a comparison study of Plusoptix, Iscreen and SPOT Binocul Vis Strabol Q Simms Rom 28 1 20 28
Acknowledgements
The authors acknowledge all the ophthalmology team.
Funding
Open access funding provided by FCT|FCCN (b-on).
Author information
Authors and Affiliations
Contributions
Sandra Guimaraes had the idea, prepared the data and wrote the main manuscript text. Maria Vieira and José Vilas Boas prepared the data and made the statistical results. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have not disclosed any competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Guimaraes, S., Vieira, M.J. & Boas, J.M.V. Predicting myopic changes in children wearing glasses using the Plusoptix photoscreener. Int Ophthalmol 44, 84 (2024). https://doi.org/10.1007/s10792-024-02954-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10792-024-02954-9