
Abstract
COVID-19 is a pandemic disease caused by severe acute respiratory syndrome corona virus 2 (SARS-CoV-2). The study area, Tamilnadu, is a southern state in India. The present study demonstrates the significance of mapping in identifying the risk zones of COVID-19 disease by taking a study of COVID-19 cases in Tamilnadu state. The main objective of the study was to identify the risk zone of COVID-19 disease in the first wave of Tamilnadu through geospatial mapping. Data on COVID-19 cases collected during March 2020 to March 2021 month wise in all 37 districts (unit area) of Tamilnadu in two-month interval wise was analysed. The study is based on secondary sources from respective office in Tamilnadu. Z-score techniques were used for standardizing data. Correlation analysis provided a measure of correlation between COVID-19 and working population. Location Quotient analysis aided the identification of COVID-19 risk zones in Tamilnadu. Present study indicates tertiary workers are more vulnerable to COVID-19 disease.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
A disease outbreak with the capability to spread across countries or continents is classified as a pandemic (Webmd, 2022).Corona virus disease (COVID-19) is a pandemic disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Mazumder et al., 2020; Krammer, 2020; Rajendran et al., 2020; Farshidpour et al., 2020; Chin et al., 2020). Coronaviruses are a family of viruses that can cause illnesses such as the common cold, severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS) (Pal et al., 2020). The disease (Coronavirus disease 2019) it causes is called COVID-19 (Chaurasiya et al., 2020; Rahamath Nisha et al., 2021a, 2021b). In 2019, a new coronavirus was identified as the cause of a disease outbreak that originated in China (Liu et al., 2020; Akula and McCubrey, 2020; Yang et al., 2020; Guo et al., 2020). Within a span of a few days, this disease became a global threat (Ali et al., 2020). It was termed as a pandemic by the World Health Organization on March 11, 2020 (Cucinotta & Vanelli, 2020; Cullen et al., 2020; Lone & Ahmad, 2020; Mocnik et al., 2020) once it became clear that it was spreading fast over a wide area and the resulting illness was severe. Since then, the disease has affected more than 1.5 core people worldwide by July 5, 2020 (Siddiqui et al., 2020) and has gone up to 6,122,496 infected cases as of March 07, 2022 (Worldometers, 2022). Kerela was the first state in India to report COVID infection on 30th January 2020 following the return of three medical students from Wuhan who tested positive for the disease (Andrews et al., 2020). Between March 11, 2020 and July 5, 2020, around 6.9 lakh people in India were infected with corona virus (Siddiqui et al., 2020).
In Tamilnadu, a resident of Kanchipuram district (45-year-old man) tested positive for coronavirus on 07 March 2022, making him the patient zero in Tamilnadu, when he returned to India from Oman (Murugesan et al., 2020). On May 13th, 2021, Tamilnadu reported the highest single day spike of 30, 987 cases which put Tamilnadu in the fourth place for the highest number of confirmed cases in India (Timeline of Events, 2022).
Symptoms of COVID-19 are variable, but often include fever, cough, fatigue, breathing difficulties, and loss of smell and taste (Luceño-Moreno et al., 2020; Rahamath Nisha et al., 2021a; 2021b). Symptoms begin one to fourteen days after exposure to the virus (He et al., 2020). Of those people who develop noticeable symptoms, most (81%) develop mild to moderate symptoms (up to mild pneumonia), while 14% develop severe symptoms (dyspnoea, hypoxia, or more than 50% lung involvement on imaging), and 5% suffer critical symptoms (respiratory failure, shock, or multiorgan dysfunction) (Gandhi et al., 2020;Jain & Yuan, 2020; Gupta et al., 2020).
The virus that causes COVID-19 spreads mainly when an infected person is in close contact with another person. Small droplets and aerosols containing the virus can spread from an infected person's nose and mouth as they breathe, cough, sneeze, sing, or speak (Desai & Patel, 2020; Rajendran & Jayagopal, 2021).
The term 'morbidity’ refers to the complications and consequences that arise out of a disease and co-morbidity refers to simultaneous presence of multiple diseases or health conditions. Previous studies (Laxminarayan et al., 2021, Sanyaolu et al., 2020, Ejaz et al., 2020, Bhandari et al., 2020, Guan et al., 2020) have established a relationship between COVID-19 and pre-existing co-morbidities. The results revealed that the major co-morbidities prevalent in patients who experienced severe COVID were Hypertension (42.46%) followed by Diabetes mellitus (39.72%), Old k-chest (20.54%), COPD/ Bronchial Asthma (16.43%), Coronary artery disease (13.69%), Chronic kidney disease (13.69%) and Valvular heart disease (6.84%). The aim and objective of the present study is to analyse the spatial variation of COVID-19 noticed in different districts in Tamilandu and to identify the risk zones in the study area in association to the working population.
Study area
The study area, Tamil Nadu, is the southernmost state in India (Fig. 1). It covers an area of about 130,058 sq.km with a population of 7, 21, 38, 958. It has a density of 555 persons per sq km with 56% of people living in rural areas against 44% in urban areas (e_governance_in_TN, 2018). The main economic activity is agriculture and 42.57% of the population is engaged in this activity. The air quality of Tamilnadu falls within acceptable levels and the number of acute respiratory infection cases in 2019 amounted to 1.98 million which was a fall from the previously reported 2.80 million cases in 2018. Following the spike in respiratory illness, specifically COVID, the Tamilnadu Health department reported that 88% cases were asymptomatic but began adopting more stringent containment strategies which included issuing of the standard operating procedure (SOP) for workplaces, factories and establishments in April 2020 ( COVID-19 Health & Family welfare Department SOP, 2020).

Location Map of the Study area
On the treatment front, the department of Heath and Welfare reported that the state has 3,371 ventilators and 29,074 beds in isolation wards as of April 2, 2020. This amounted to 1.1 hospital beds per 1000 people and 7.8 beds per 1000 people for the elderly population (Chakraborty et al., 2020) with free treatment in government facilities. Further, 25 private colleges and 110 private hospitals in the state were designated for COVID treatment (Brookings, 2020).
Database and methodology
Data was collected from secondary sources (https://stopcorona.tn.gov.in/,)district wise on monthly COVID-19 incidences in Tamil Nadu. Two important techniques namely, statistical approach and Cartographic interpretations were used in the study. The correlation matrix reveals the relationship between the incidence of COVID 19 and working population. It includes mapping of the study area using the GIS software of Arc GIS. Z-Score is a statistical measurement of a score’s relationship to the mean in a group of scores.
where χ is experimental value, μ is mean, and σ is standard deviation.Z-score of ‘0’ means the score is the same as the mean.
Apart from this, Location Quotient (LQ) is a useful tool for comparing area characteristics (Moineddin et al., 2003;Ghosh et al., 2021; Pandey et al., 2021) and its use in healthcare has been well established (Hendayana, 2003; Saravanabavan et al., 2019; Sukmawati, 2021). Most of the studies in medical geography are concerned with the description of spatial and temporal variations of a particular disease and are attempted at the regional level (Bossak & Turk, 2021; Balaj & Saravanabavan 2019, 2020; Vinothini et al., 2021; Bonner et al., 2019). In this study, LQ statistical techniques were used to find COVID-19 disease distribution and identification of population risk areas. The data on the number of infections of COVID-19 have been obtained from daily COVID-19 reports released by the Government of Tamilnadu. The data contains information on the incidence of the disease from 2020 March–2021 March.
Results
Trends in Covid-19 incidence
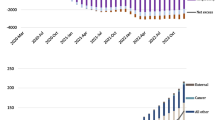
About 14,472 incidences of COVID-19 cases have been reported in the entire districts of 7Tamil Nadu from March 2020 to the end of March 2021 (https://stopcorona.tn.gov.in). COVID-19 cases gradually increased since March 2020 (67 cases) with a maximum of 5850 cases in September 2020 and decreased to 452 in March 2021. Notably, no month during the study period was free from COVID-19 incidence. On an average, 0.34% of the total population of Tamilnadu has been inflicted with this disabling disease in just about one year (March 2020-Maruch 2021) (Fig. 2).

Source https://stopcorona.tn.gov.in
Rate of Covid-19 Infected Population in Tamilnadu.
Occupation structure/tertiary workers
Occupational structure refers to the percentage distribution of the workforce involved in different occupations in the society when classified based on the skill levels and economic function. Workers were classified as primary, secondary and tertiary and the raw data were standardized using the Z score index. Positive values are designated as ‘good’ and negative values as ‘bad’ in relation to the environment health (Saravanabavan et al. 2021a, 2021b, 2021c; 2022; Kranzusch et al., 2020; Martinez-Millana et al., 2018).
Primary workers (https://www.census2011.co.in) include those involved in hunting and gathering, pastoral activities, fishing, forestry, agriculture, mining and quarrying who account for 42.57%. Secondary workers are concerned with manufacturing, processing and construction (3.89%). The tertiary workers cover a wide range of activities from commerce to administration, transport, financial and real estate activities, business and personal services, education, health and social work (53.54%). (Kramer and Kramer, 2020; RahamathNisha & Saravanabavan, 2020). Tamilnadu has a maximum of settlement and residential area located in urban areas. (Saravanabavan et al., 2021b). Manufacturing workers are mostly located in class II towns that have a population averaging between 50,000 to 99,999 people (vitalstatistics.pdf—Tn.gov.in 2018). Agricultural and fishing etc. are in the plain area of small towns and villages. (https://www.census 2011.co.in) (Balasubramani et al., 2015).
Tertiary Workers are the dominant group with high intensity COVID-19 incidence (Fig. 3) (21 districts) compared to low incidence of COVID in districts with Primary (16 districts) and Secondary workers as the dominant group (Table 1). This could imply that despite higher literacy rates in the tertiary workers group, the higher population and urbanization might be one of the biggest contributors to the spread of COVID-19. Out of 15 districts only 2 districts have moderate intensity of covid-19. The remaining districts had low intensity among the majority of primary and secondary workers.

Source Statistical Handbook of Tamil Nadu 2018
Distribution of Tertiary Workers in
In addition, the main reasons behind higher COVID-19 incidence in Tertiary population areas is due to high density of population, frequency of travel and flow, business activity, education, social work and personal services thereby favoring COVID-19 spread from person to person. (Arif & Sengupta, 2021; Sarkar et al., 2021). Other minor factors including effectiveness of vaccines over time, human behavior, infection prevention policies, changes to the coronavirus itself, and the number of people who are vulnerable because they have not developed some immunity, whether from natural infection or through vaccination might also contribute to higher incidence of COVID-19.
This study highlights that Primary Workers have − 0.586 level of significance, secondary workers have 0.016 level of significance and Tertiary workers have the maximum significance level of 0.608 to COVID-19 under the 0.01 level of Correlation (Table 2). This analysis makes it clear that Tertiary workers have a more significant relation to COVID- 19 than the primary or secondary workers.
Discussion
The Location Quotient introduced the use of location quotient (LQ) as a measure of geographic concentration with in a region (Hazbavi et al., 2021). It can be calculated using the equation.
LQ = Xi/Yi/X/LWhere,
Xi = value of variable X in area i,Yi = value of variable Y in area i,X = regional value of variable X,Y = regional value of variable Y.High values indicate a high degree of concentration (LQ > 1) of a particular variable in an area. Values (LQ < 1) indicate low concentration value. LQ = 1 indicate the distribution is the same as the district average (Table 3).
This study experienced very high incidence of COVID-19 in July 2020 to September2020. During the remaining months they experienced moderate to low incidence (Figs. 4, 5, 6 and 7). From the analysis, it was observed that the densely populated area of the state experienced high COVID-19 intensity during the study period, whereas the low density area recorded low level of COVID-19 (Zhang et al., 2020; Gupta et al., 2020). Risk factor was computed in order to derive COVID-19 risk zones in the state (Fig. 8).

Source https://stopcorona.tn.gov.in
LQ Status of COVID-19 inTamilnadu State during March 2020 and May 2020.

Source https://stopcorona.tn.gov.in
LQ Status of Covid-19 in Tamilnadu State during July 2020 and September 2020.

Source https://stopcorona.tn.gov.in
LQ Status of COVID-19 in Tamilnadu State during November 2020 and January 2020.

Source https://stopcorona.tn.gov.in
Status of COVID-19 in Tamilnadu State.

Average LQ Value of COVID-19 during March 2020 to March 2021during March 2021
COVID-19 risk zones in Tamilnadu are demarcated based on computation of the Tamilnadu district wise COVID-19 risk factors. For this purpose, the monthly LQ values of each district is ranked into five levels: Rank 1 (< 0.5 LQ value), Rank II (LQ value 0.5–1.0), Rank III (1–1.5), Rank IV (LQ value 1.5–2), Rank V (LQ value > 2).
The rank frequencies (during how many months each value is repeated) are counted for the entire districts of Tamil Nadu. The rank frequencies are then multiplied by their respective rank values to obtain the weighted value for the disease intensity level (Hema Malini et al., 2016).
For instance, Ariyalur, ( Si No:1) district has the frequency of rank as 1,2,3 and 5 which indicates zero value and hence their weighted value are zero (rank 1 = 0,weighted value 0*1 = 0), (rank 2 = 0,weighted value 0*2 = 0), (rank3 = 0 weighted value 0*3 = 0), rank 5 = 0 weighted value o*5 = 0). Similarly the frequency of rank 1 is 4 and hence its weighted value is 4 (rank1 = 4, weighted value 4*1 = 4). Again the frequency of rank 2 is 3 and its weighted value 3*2 = 6), the sum of the frequency weighted value is 10 (rank 1 = 4 + rank2 = 6 + rank3 = 0 + rank 4 = 0 + rank 5 = 0), total weighted value = 10), for the district of Ariyallur for the entire period. This is divided by the total number of rank (5), to obtain the average annual weighted value for the districts (which in this case is 10/5 = 2) (Table 4).
Further the annual average weighted LQ values are rationally divided into 4 COVID-19 risk categories: low risk (weighted value 1–1.9), moderate risk (weighted values 2–4), and high risk value 4.1–6, very high risk (weighted value > 6). All four categories (low, moderate, high and very high) COVID-19 risk levels could be identified in Tamil Nadu. Based on COVID-19 risk levels for all districts of Tamilnadu map has been prepared with GIS software (Fig. 9).

Identification of Covid-19 risk zone in Tamilnadu
COVID-19 risk zone
The monthly intensity of COVID-19 is based on computed LQ which indicate that COVID-19 incidence of low risk level district are 10 out of 37 districts with annual average of LQ values of less than 2 (16.4%). The low intense district is mostly located in primary activities area. Based on risk analysis it was found that 23 districts out of 37 (60.2%) are moderate intense risk categories. Remaining 3 districts (namely Chenglepattu (5.8), Coimbatore (4.8), Kanchipuram (5.8)), come under high intense (16.4%) COVID-19 risk Zone. Chennai comes in very high intense risk (7%) area. These regions have more tertiary activities (97%) and less than 2% of people are engaged in primary and secondary activities. According to LQ risk zone analysis, 16.40% are low intense, moderately intense 60.20%, high intense 16.40% and very high intense 7% of COVID-19 zones in Tamilnadu.
Conclusion
The study revealed that the incidence of COVID-19 cases is distributed throughout Tamilnadu and four districts were identified as high risk zones based on LQ: Chennai (7.0%), Chengalpattu (5.8%), Kanchipuram (5.8%) and Coimbatore (4.8%) accounting for a total of 23.40%. All 4 districts were found to have a higher proportion of Tertiary workers as the geographical location and the prevailing environment makes the districts ideal for urban settlement and business. This in turn increases the migration rate and the higher case numbers in these districts can be attributed to activities like business and population density (infrastructure activities). Distribution of COVID-19 cases in districts that are predominantly occupied by primary and secondary workers was observed to be less intense owing to larger agricultural land area and sparce population. Minor factors including vaccine effectiveness and development of natural immunity might also influence the differences in the prevalence of the disease, but the biggest contributor to the spread remains to be the population density. Therefore, the study concludes that districts with higher tertiary workers would require more attention and stringent containment plans in place to reduce the impact of COVID-19 in the state of Tamilnadu.
References
Akula, S. M., & McCubrey, J. A. (2020). Where are we with understanding of COVID-19? Advances in Biological Regulation, 78, p. 100738. https://doi.org/10.1016/j.jbior.2020.100738
Ali, S. A., Baloch, M., Ahmed, N., Ali, A. A., & Iqbal, A. (2020). The outbreak of Corona virus disease 2019 (COVID-19) an emerging global health threat. Journal of Infection and Public Health, 13(4), 644–646. https://doi.org/10.1016/j.jiph.2020.02.033
Andrews, M. A., Areekal, B., Rajesh, K. R., Krishnan, J., Suryakala, R., Krishnan, B., Muraly, C. P., & Santhosh, P. V. (2020). First confirmed case of COVID-19 infection in India: A case report. The Indian Journal of Medical Research, 151(5), 490.
Arif, M., & Sengupta, S. (2021). Nexus between population density and novel coronavirus (COVID-19) pandemic in the south Indian states: A geo-statistical approach. Environment, Development and Sustainability, 23(7), 10246–10274. https://doi.org/10.1007/s10668-020-01055-8
Balaji, D., & Saravanabavan, V. (2019). A geo medical analysis of dengue cases in Madurai city-Tamilnadu India. GeoJournal 85(4), 979–994. https://doi.org/10.1007/s10708-019-10006-4
Balaji, D., & Saravanabavan, V. (2020). A geo medical analysis of dengue cases in Madurai city-Tamilnadu India. GeoJournal, 85(4), 979–994.
Balasubramani, K., Veena, M., Kumaraswamy, K., & Saravanabavan, V. (2015). Estimation of soil erosion in a semi-arid watershed of Tamil Nadu (India) using revised universal soil loss equation (rusle) model through GIS. Modeling Earth Systems and Environment, 1(3), 1–17.
Bhandari, S., Singh, A., Sharma, R., Rankawat, G., Banerjee, S., Gupta, V., Dube, A., Kakkar, S., Sharma, S., Keswani, P., Agrawal, A., Tak, A., & Nawal, C. L. (2020). Characteristics, treatment outcomes and role of hydroxychloroquine among 522 COVID-19 hospitalized patients in Jaipur City: An epidemio-clinical study. J Assoc Physicians India, 68(6), 13–19.
Bonner, S. N., Clark, C., Keating, N. L., Kouri, E. M., & Freedman, R. A. (2019). Examining associations of racial residential segregation with patient knowledge of breast cancer and treatment receipt. Clinical Breast Cancer, 19(3), 178–187.
Bossak, B. H., & Turk, C. A. (2021). Spatial variability in COVID-19 mortality. International Journal of Environmental Research and Public Health, 18(11), 5892. https://doi.org/10.3390/ijerph18115892
Brookings. (2020). https://www.brookings.edu/blog/up-front/2020/03/24/is-indias-health- infrastructure-equipped-to-handle-an-epidemic/
Chakraborty, P. S., Shamika, R., & Sikim (2020). COVID-19 | Is India's health infrastructure equipped to handle an epidemic?Brookings. Archived from the original on 9 April 2020. Retrieved 16 April 2020.
Chaurasiya, P., Pandey, P., Rajak, U., Dhakar, K., Verma, M., & Verma, T. (2020). Epidemicand challenges of coronavirus disease-2019 (COVID-19): India response. Available at SSRN 3569665.
Chin, A. W., Chu, J. T., Perera, M. R., Hui, K. P., Yen, H. L., Chan, M. C., Peiris, M., & Poon, L. L. (2020). Stability of SARS-CoV-2 in different environmental conditions. The Lancet Microbe, 1(1), e10.
COVID-19 Health and Family welfare Department SOP. (2020). https://www.mohfw.gov.in/pdf/StandardOperatingProcedureSOPfortransportingasuspectorconfirmedcaseofCOVID19.pdf
Cucinotta, D., & Vanelli, M. (2020). WHO declares COVID-19 a pandemic. Acta Bio Medica: Ateneiparmensis, 91(1), 157. https://doi.org/10.23750/abm.v91i1.9397
Cullen, W., Gulati, G., & Kelly, B. D. (2020). Mental health in the COVID-19pandemic. QJM: An International Journal of Medicine, 113(5), 311–312.
Desai, A. N., & Patel, P. (2020). Stopping the spread of COVID-19. JAMA, 323(15), 1516–1516.
e_governance_in_TN. (2018). https://it.tn.gov.in/sites/default/files/2018-10/e_governance_in_TN_connect%20%281%29.pdf
Ejaz, H., Alsrhani, A., Zafar, A., Javed, H., Junaid, K., Abdalla, A. E., Abosalif, K. O., Ahmed, Z., & Younas, S. (2020). COVID- 19 and comorbidities: Deleterious impact on infected patients. Journal of Infection and Public Health, 13(2020), 1833–1839.
Farshidpour, M., Kim, D., Junna, S., & Merchant, J. (2020). A brief review of liver injury in patients with Corona virus disease-19 during the pandemic. Indian Journal of Gastroenterology. https://doi.org/10.1007/s12664-020-01068-1
Gandhi, R. T., Lynch, J. B., & Del Rio, C. (2020). Mild or moderate Covid-19. New England Journal of Medicine, 383(18), 1757–1766. https://doi.org/10.1056/NEJMcp2009249
Ghosh, D., Sarkar, A., & Chouhan, P. (2021). COVID-19 second wave: District level study of concentration of confirmed cases and fatality in India. Environmental, Challenges, 5(December), 100221.
Guan, W. J., Liang, W. H., He, J. X., & Zhong, N. S. (2020). Cardiovascular comorbidity and its impact on patients with COVID-19. European Respiratory Journal, 55(6), 2001227.
Guo, Y. R., Cao, Q. D., Hong, Z. S., Tan, Y. Y., Chen, S. D., Jin, H. J., Tan, K. S., Wang, D. Y., & Yan, Y. (2020). The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak–an update on the status. Military Medical Research, 7(1), 1–10.
Gupta, R., Ghosh, A., Singh, A. K., & Misra, A. (2020). Clinical considerations for patients with diabetes in times of COVID-19 epidemic. Diabetes & Metabolic Syndrome, 14(3), 211.
Hazbavi, Z., Mostfazadeh, R., Alaei, N., & Azizi, E. (2021). Spatial and temporal analysis of the COVID-19 incidence pattern in Iran. Environmental Science and Pollution Research, 28(11), 13605–13615. https://doi.org/10.1007/s11356-020-11499-0
He, X., Lau, E. H., Wu, P., Deng, X., Wang, J., Hao, X., Lau, Y. C., Wong, J. Y., Guan, Y., Tan, X., & Mo, X. (2020). Temporal dynamics in viral shedding and transmissibility of COVID-19. Nature Medicine, 26(5), 672–675. https://doi.org/10.1038/s41591-020-0869-5
Hema Malini, M., Visweswara Reddy, B., Gangaraju, M., Tammi Naidu, G., & Nageswara Roa, K. (2016). Geospatial analysis of filariasis risk in Vizianagaram District of Andhra Pradesh India. Punjab Geographer, 12(1), 83–96.
Hendayana, R. (2003). Aplikasi metode location quotient (LQ) dalam penentuan komoditas unggulan nasional. Informatika Pertanian, 12(1), 658–675.
Jain, V., & Yuan, J. M. (2020). Predictive symptoms and comorbidities for severe COVID-19 and intensive care unit admission: A systematic review and meta-analysis. Internationaljournal of Public Health, 65(5), 533–546.
Kramer, A., & Kramer, K. Z. (2020). The potential impact of the Covid-19 pandemic on occupational status, work from home, and occupational mobility (Vol. 119). Elsevier. https://doi.org/10.1016/j.jvb.2020.103442
Krammer, F. (2020). SARS-CoV-2 vaccines in development. Nature, 586(7830), 516–527. https://doi.org/10.1038/s41586-020-2798-3
Kranzusch, R., Wiesemann, S., Zange, L., Jeuthe, S., Ferreira da Silva, T., Kuehne, T., Pieske, B., Tillmanns, C., Friedrich, M. G., Schulz-Menger, J., & Messroghli, D. R. (2020). Z-score mapping for standardized analysis and reporting of cardiovascular magnetic resonance modified Look-Locker inversion recovery (MOLLI) T1 data: Normal behavior and validation in patients with amyloidosis. Journal of Cardiovascular Magnetic Resonance, 22(1), 1–10.
Laxminarayan, R., Vinay, T. G., Kumar, K. A., Wahl, B., & Lewnard, J. A. (2021). SARS-CoV-2 infection and mortality during the first epidemic wave in Madurai, south India: A prospective, active surveillance study. The Lancet Infectious Diseases, 21(12), 1665–1676.
Liu, S., Yang, L., Zhang, C., Xiang, Y. T., Liu, Z., Hu, S., & Zhang, B. (2020). Online mental health services in China during the COVID-19 outbreak. The Lancet Psychiatry, 7(4), e17–e18.
Lone, S. A., & Ahmad, A. (2020). COVID-19 pandemic–an African perspective. Emerging Microbes & Infections, 9(1), 1300–1308. https://doi.org/10.1080/22221751.2020.1775132
Luceño-Moreno, L., Talavera-Velasco, B., García-Albuerne, Y., & Martín-García, J. (2020). Symptoms of posttraumatic stress, anxiety, depression, levels of resilience and burnout in Spanish health personnel during the COVID-19 pandemic. International Journal of Environmental Research and Public Health, 17(15), 5514. https://doi.org/10.3390/ijerph17155514
Martinez-Millana, A., Hulst, J. M., Boon, M., Witters, P., Fernandez-Llatas, C., Asseiceira, I., Calvo-Lerma, J., Basagoiti, I., Traver, V., De Boeck, K., & Ribes-Koninckx, C. (2018). Optimisation of children z-score calculation based on new statistical techniques. PloS One, 13(12), e0208362.
Mazumder, H., Hossain, M. M., & Das, A. (2020). Geriatric care during public health emergencies: Lessons learned from novel corona virus disease (COVID-19) pandemic. Journal of Gerontological Social Work, 63(4), 257–258. https://doi.org/10.1080/01634372.2020.1746723
Mocnik, F. B., Raposo, P., Feringa, W., Kraak, M. J., & Köbben, B. (2020). Epidemics and pandemics in maps–the case of COVID-19. Journal of Maps, 16(1), 144–152. https://doi.org/10.1080/17445647.2020.1776646
Moineddin, R., Beyene, J., & Boyle, E. (2003). On the location quotient confidence interval. Geographical Analysis, 35(3), 249–256. https://doi.org/10.1111/j.1538-4632.2003.tb01112.x
Murugesan, B., Karuppannan, S., Mengistie, A. T., Ranganathan, M., & Gopalakrishnan, G. (2020). Distribution and trend analysis of COVID-19 in India: Geospatial approach. J Geogr Stud, 4(1), 1–9.
Pal, M., Berhanu, G., Desalegn, C., & Kandi, V. (2020). Severe acute respiratory syndrome Coronavirus-2 (SARS-CoV-2): an update. Cureus, 12(3).https://doi.org/10.7759/cureus.7423
Pandey, A., Prakash, A., Agur, R., & Maruvada, G. (2021). Determinants of COVID-19 pandemic in India: An exploratory study of Indian states and districts. Journal of Social and Economic Development, 23(2), 248–279.
Rahamath Nisha, R., Saravanabavan, V., & Sureshkumar, R. (2021b) Effects of population density and air pollution on Covid-19 morbidity and mortality in India using GIS. International Journal of Contemporary Medical Research, 8(8), H1–H11.
Rahamath Nisha, R., Saravanabavan, V., & Sureshkumar, R. (2021a). Emerging COVID-19 epidemiology in Tamil Nadu India using GIS. International Journal of Contemporary Medical Research, 7(8), H10–H17.
RahamathNisha, R., & Saravanabavan, V. (2020). Occupational health: a special reference to lung disease in petrochemical, metal and building material industrial workers in Melur taluk Madurai district. International Journal of Contemporary Medical Research, 7(7), G1–G6. https://doi.org/10.21276/ijcmr.2020.7.7.12
Rajendran, D. K., Rajagopal, V., Alagumanian, S., Kumar, T. S., Prabhakaran, S. S., & Kasilingam, D. (2020). Systematic literature review on novel corona virus SARS-CoV-2: a threat to human era. Virusdisease, 31(2), 161–173. https://doi.org/10.1007/s13337-020-00604-z
Rajendran, S., & Jayagopal, P. (2021). Accessing Covid19 epidemic outbreak in Tamilnadu and the impact of lockdown through epidemiological models and dynamic systems. Measurement, 169, 108432. https://doi.org/10.1016/j.measurement.2020.108432
Sanyaolu, A., Okorie, C., Marinkovic, A., Patidar, R., Younis, K., Desai, P., & Altaf, M. (2020). Comorbidity and its impact on patients with COVID-19. SN Comprehensive Clinical Medicine, 2(8), 1069–1076.
Saravanabavan, V., Balaji, D., & Preethi, S. (2019). Identification of dengue risk zone: A geo-medical study on Madurai city. GeoJournal, 84(4), 1073–1087. https://doi.org/10.1007/s10708-018-9909-9
Saravanabavan, V., Balaji, D., Reshma, C. U., Sheheersha, S. K., Sudharsan, R., Vimala Vinnarasi, J., Ganesan, J., Rahamath Nisha, R., Eswari, S., & Balasubramani, K. (2021). Urban disease ecology and its spatial variation of Chikungunya in Madurai City, Tamilnadu, India: a geo-medical study. GeoJournal, 86(5), 2335–2350. https://doi.org/10.1007/s10708-020-10192-6
Saravanabavan, V., Lekha, C. A., Aparna, T., Nisha, R. R., Balaji, K. K., & Kanna, S. V. (2021). Spatio-temporal variation of dengue in Kozhikode District, Kerala: A medico geographical study. International Journal of Mosquito Research, 8(1, Part B), 130–140.
Saravanabavan, V., Reshma, C. U., & Preethi, S. (2021). Determinants of reproductive health in working women in Thrissur district Kerala. GeoJournal, 86(1), 239–253. https://doi.org/10.1007/s10708-019-10051-z
Saravanabavan, V., Vinothini, C., Balaji, D., Alok, M., Arya, M., & Athira, R. (2022). Geo-spatial approach on COVID-19 mortality in Tamil Nadu. International Journal of Geography, Geology and Environment, 4(1), 123–131.
Sarkar, P., Debnath, N., & Reang, D. (2021). Coupled human-environment system amid COVID-19 crisis: A conceptual model to understand the nexus. Science of the Total Environment, 753, 141757. https://doi.org/10.1016/j.scitotenv.2020.141757
Siddiqui, A. F., Wiederkehr, M., Rozanova, L., & Flahault, A. (2020). Situation of India in the COVID- 19 pandemic: India’s initial pandemic experience. International Journal of Environmental Research and Public Health, 17(23), 8994.
Sukmawati, N. M. H. (2021). Inpatient facility distribution and primary healthcare centers demand based on location-quotient in Bali within 2015–2019 period. WMJ (Warmadewa Medical Journal), 6(1), 20–29.
Timeline of events. (2022). https://en.wikipedia.org/wiki/COVID-19_pandemic_in_Tamil_Nadu
Vinothini, C., Saravanabavan, V., & Balaji, D. (2021). Travel pattern of health utilization to primary health care centres in Madurai district. International Journal of Geography, Geology and Environment, 3(2), 144–151.
Webmd. (2022). https://www.webmd.com/cold-and-flu/what-are-epidemics-pandemics-outbreaks
Worldmmeters. (2022). https://www.worldometers.info/coronavirus/
Yang, X., Yu, Y., Xu, J., Shu, H., Liu, H., Wu, Y., Zhang, L., Yu, Z., Fang, M., Yu, T., & Wang, Y. (2020). Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. The Lancet Respiratory Medicine, 8(5), 475–481.
Zhang, S., Wang, Z., Chang, R., Wang, H., Xu, C., Yu, X., Tsamlag, L., Dong, Y., Wang, H., & Cai, Y. (2020). COVID-19 containment: China provides important lessons for global response. Frontiers of Medicine, 14(2), 1–5. https://doi.org/10.1007/s11684-020-0766-9
Acknowledgements
The authors gratefully acknowledge the RUSA-Phase II (RashtriyaUchchatar Shiksha Abhiyan, Ref MKU/RUSA/RP/Sanc.Order/2020), Department of Geography, School of Earth and Atmospheric Sciences, Madurai Kamaraj University, Madurai, 625021 for their financial support in carrying out the publishing of this research work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical approval
Ethical approval not required.
Human or Animal rights
This article does not contain any studies with human participants or animals performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Saravanabavan, V., Emayavaramban, V., Thangamani, V. et al. Spatial variation of covid-19 morbidity status and identification of risk zone in Tamil Nadu (India) during first wave. GeoJournal 88, 1341–1354 (2023). https://doi.org/10.1007/s10708-022-10680-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10708-022-10680-x