
Abstract
During Covid-19 pandemic most hospitals have restricted in-person delivery of non-essential healthcare services, including genetic testing delivery, to slow the spread of the virus. Our Onco-Genetic Service also faced this challenging period and had to re-organize its clinical practice with the use of tele-health. Aim of the present paper is to understand whether and how Covid-19-related changes in medical practice influenced patients’ satisfaction about the health service provided. 125 BRCA1/2 non carriers (109/125, 87.2% female and 16/125, 12.8% male) in Istituto Tumori “Giovanni Paolo II” of Bari were enrolled. All participants were asked to choose whether they prefer in-person or remote post-test counselling session. Basing on patients’ choice, two groups of subjects were composed. One week after the post-test counselling session, participants were phone called and asked to complete: a socio-demographic form, a brief structured interview about their Covid-19 related worries and their satisfaction with the health service provided, Hospital Anxiety and Depression Scale and Fear of Covid-19 scale. Qualitative information about patients’ choice were also collected. No significant difference about patients’ satisfaction with the health service provided emerged between groups. Patients who preferred remote post-test counselling had higher anxiety, worries and fear-of Covid-19 than the others. All remote-counselling subjects preferred tele-genetics because of Covid-19 security, would choose it again and would recommend it to others. Cancer tele-genetics offers good guarantees of comfort and efficacy, but patients’ choices are related to personal and psychological variables. The use of tele-genetics has to be a patient’s choice.
Similar content being viewed by others

Introduction
Onco-genetic counselling and testing provide opportunities to identify pathogenic gene variants associated with an increased cancer risk and represents an application of standard practice “personalized medicine” [1]. Thus, genetic test disclosure is crucial to help patients understanding their genetic cancer risks and has, historically, been conducted in-person by genetics professionals [2].
Due to the COVID-19 pandemic, most clinics and hospitals have restricted in-person delivery of non-essential healthcare services (including genetic testing delivery) and created a bottleneck in scheduling and long waiting times for an appointment when in-person testing delivery can eventually be programmed. For this reason, healthcare practice changed in a matter of days [3]. Tele-genetics refers to the use of technology to support long-distance healthcare and include telephone or video counselling sessions. In some geographic regions, tele-genetics is routinely used to overcome shortages of credentialed genetics professionals [4, 5], but so far in Southern Italy the lack of tecnological Hospital infrastructures has made the use of telegenetics difficult. In fact, as a clinical practice, the provision of Oncological Genetic Counselling (OGC) in Istituto Tumori “Giovanni Paolo II” of Bari, involves a series of steps: patients receive an in-person 45-min pre-test counselling session and a psychological assessment; if genetic testing criteria [6, 7] are present, after signing the informed consent, patients are taken a blood sample in the Hospital Laboratory; within 3 months, test results are delivered in a 30–45-min post-test counselling session and a written clinical report containing personal and familiar cancer risk information is issued to patients. Currently, patients must always be present at the hospital for blood collection and genetic testing, but things may change in the case of post-test onco-genetic counselling. During COVID-19 Pandemic, our onco-genetic services turned to tele-genetics out of necessity but our activities’ reorganization aimed both at maintaining the best care standards [8] and at reducing hospital-acquired infection risk. Therefore, limited to post-test oncogenic consultations, we allowed patients to choose between two options: the genetic test report (and the related written clinical reports) could be delivered remotely at the previously scheduled time, or the appointments could be rescheduled in-person in the coming months.
Aim of the present paper is to explore whether and how the changes occurred in our medical practice due to COVID-19 pandemic restriction, had an impact on patients’ satisfaction about the health service provided.
Methods
The current study enrolled 125 subjects (109 female, 16 males) who should have carried out during Italian pandemic restrictions (May 2020—Nov 2020) post-test genetic counselling for the delivery of their BRCA1/2 genetic report inside Heredo-Family Cancer Clinic of Istituto Tumori Giovanni Paolo II in Bari. All the subjects enrolled resulted to be non-carrier for BRCA1/2 pathogenetic mutations.
Every participant was reached by telephone and asked to choose whether he/she preferred to receive a remote vs an in-person post-test counselling session for genetic test disclosure. Those who preferred a remote post-test counselling session were asked to sign a specific informed consent for online delivery of genetic test results. After signing the informed consent, test results and a clinical report were sent through e-mail to all participants and a post-test counselling session with a certified genetic counsellor was performed by telephone.
One week after the post-test counselling session, participants were interviewed by telephone by a trained psychologist and asked to complete (Suppl.1).
-
Hospital Anxiety and Depression scale (HADs), a self-administered questionnaire developed to detect the state of anxiety and depression in non-psychiatric patients with organic disease [9]. The scale has demonstrated satisfactory psychometric characteristics in cancer patients [10] and has been translated and validated in Italian populations [11].
-
Fear of Covid-19 Scale (FCV-19S) is a new psychometric assessment tool assessing individual’ fear of COVID-19 [12]. It is composed of seven items rated on a 5- point scale. The scale has been translated and validated in Italian population showing a good internal reliability and consistency also in the Italian version [13].
-
Participants were also asked to answer a brief structured interview, investigating:
-
The impact of COVID-19 related worries [14]: 6 questions on a 5 point likert-scale [suppl. 1] (
-
The satisfaction with OGC experience: 7 questions on a on a 5 point Likert-scale (from 1: very unsatisfied, to 5:very satisfied) taken from previous literature [15,16,17] and exploring subjects’ feelings about: (a) the general quality of OGC; (b) counsellor’s competence, (c) clarity of expressed contents, (d) counsellor’s courtesy, (e) how much the subject felt at ease, (f) protection of confidentiality, (g) personal understanding of genetic information.
Socio-demographic information (age, gender, having/not having children, being affected/unaffected by cancer, having/not having tested for COVID-19) were also collected and post-test counselling sessions have been performed between June and November 2020.
Qualitative information about our sample were also collected (suppl. 1) and all participants were asked to.
-
Answer a dichotomic question regarding whether they considered the use of telemedicine in genetic reports delivery as valid as the in-person delivery.
-
Declare the reason of their choice to receive genetic test results in-person vs in remote ((a) need for human contact with the clinicians; (b) difficult use of technology; (c). already coming at the hospital; (d) pandemic security; (e) other).
-
Participants who choose remote genetic test delivery were also asked.
-
If they would have chosen again remote genetic test disclosure.
-
If they would recommend someone else to use tele-genetics and when ((a) yes, only during pandemic; (b) yes, on all occasion; (c) no).
Statistical analysis
Discrete variables have been analyzed through chi-square test and continuous variables through wilcoxon test. The “stats” and “rstatix” R packages have been used (R version 3.6.2). The dataset used and analyzed during the current study are available from the corresponding author on reasonable request.
Results
Participants characteristics of the whole sample are shown in Table 1.
No significant socio-demographic difference between groups was found: socio-demographic variables analyzed were sex (p-value 1), age (p-value 0.63), having children (p-value 0.2), schooling (p-value 0.2) and being a cancer patient (p-value 0.5) (Table 2).
Significant different Covid-19 related worries were expressed among groups (Table 2): participants who preferred remote counselling were significantly more concerned about the probability to get Covid-19 hospital-acquired infection (p-value 5.68e-11), the probability to spread Covid-19 infection within the family (p-value 2.07e-11), the uncertainty and endurance connected to pandemic (p-value 0.0225) and feeling more vulnerable to the infection than the general population (p-value 0.000854).
No significant difference emerged among groups regarding overall perceived quality of OGC (p-value 949), counsellor’s competence (p-value 1), clarity of contents (p-value 1), counsellor’s courtesy (p-value 1), feeling comfortable during OGC (p-value 576), confidentiality (p-value 1), genetic information comprehension (p-value 1) (Table 2).
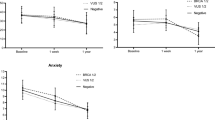
Significant differences emerged regarding FCV-19S scorings both considering the single items and the global scoring (p-value 5.68e-07): a significant higher fear of Covid-19 was found among remote test delivery group (average 25; range 34–8) than in-person test delivery group (average 16; range 33–7). Thus, in our sample significant higher HAD-A scores emerged in remote test delivery group than in-person group (p-value 0.0117). Contrarily, no significant difference emerged regarding HAD-D or HADs scorings (p-value 0,177 and 0.39 respectively) (Table 2).
Qualitative information collected in the two groups revealed significant differences regarding tele-genetics validity (p-value 1.77e-12) and choice reasons (p-value 0.000001): all remote- delivery participants (62/62, 100%) declared they preferred tele-genetics because of pandemic security, while among the in-person delivery group 38/63 (60,3%) expressed the need for human contact with the clinician, 22/63 (34,9%) already had to get to the hospital for other reasons and only 3/63 (4.8%) declared to feel uncomfortable with the use of technology.
Finally, qualitative information collected from participants belonging to the remote test disclosure group (Table 3).
Interestingly, from the spontaneous statements collected also emerged that the choice whether to recommend the use of telemedicine only during the pandemic or on any occasion depended respectively on the need for human contact and on the convenience of not having to reach the Hospital.
Discussion
Due to Covid-19 pandemic persistence, genetic services had to rearrange its clinical activity to ensure genetic test delivery despite the restriction prescribed to slow the spread of Coronavirus [18, 19]. The present paper describes and analyses the changes occurred within Onco-genetic Department of Istituto Tumori “Giovanni Paolo II” di Bari since May 2020, when Covid-19 pandemic limitations imposed to reduce the number of people accessing Hospitals.
Consistently with literature data [20, 21], our results show that there are no significant differences in satisfaction, perceived quality and genetic information understanding between in-person and remote genetic test delivery. In addition, in accordance with previous research [22,23,24], we can assume that remote delivery of onco-genetic counselling services is an acceptable alternative when in-person counselling is prohibitive.
Thus, in our sample significant differences emerged regarding tele-genetics perceived validity: unlike remote group, subjects choosing in-person post-test counselling session considered tele-genetics less valid than in-presence health service. Based on Beri et al. research about patients’ preferences [25], we hypothesize that patients need to be involved in the decision about the use of tele-genetics: patients’ will to have a remote vs in-person post-test counselling session must be fully explored and respected.
In addition, significant differences also emerged regarding anxiety, fear of Covid-19 and Covid-19 related worries: consistently with literature [12,13,14, 21, 26] participants preferring tele-genetics showed higher scores in the three variables related questions. We can argue these differences should be considered connected to patients’ choice to use tele-medicine: the higher the anxiety, worry and fear of Covid-19, the more patients prefer remote post-test counselling session. Interestingly, qualitative information collected about patients’ reason of their choice is consistent with the hypothesis that the use telemedicine is strongly influenced by personal assessments on perceived safety of the hospital, the need for human contact and the need to optimize medical treatments timing.
Although patients’ experience with tele-genetics is generally positive and promising [18,19,20,21, 23, 24, 26] it is important that clinicians who propose their patients to use tele-health make sure to address patients’ preferences leading to a really shared-decision making and to a better practice in patient-centred medical treatments [27]. The authors hypothesize that telegenetics may be integrated into current clinical practice of post-test onco-genetic counselling. Further research is needed to evaluate the extension of telegenetics to pre-test onco-genetic counselling. In contrast, the physical presence of the patient in the hospital remains necessary for genetic testing and blood sampling.
The present study has many limitations: the small numerosity of the sample analyzed and the geographic specificity of this study don’t allow us to generalize the results presented. New research in this field is required to better understand the impact of the use of telemedicine on patients undergoing OGC.
The results of the present paper show that the use of telemedicine in OGC does not affect the validity and perceived quality of the health service offered to patients. Therefore, regardless of pandemic period, remote post-test genetic counselling can be considered as valid as in-person disclosure and can be offered without compromising patients’ understanding of genetic information.
Since patients’ choice of using telemedicine seem to be strictly related to psychological and personal variables (anxiety, fear, worries, feeling at ease with technology), it is necessary to involve patients in the decision-making process regarding post-test genetic counselling session to ensure them effectiveness and satisfaction with OGC.
Cancer tele-genetic services hold promise for access to expert genetic counsellors in a one-on-one format also for patients who live very distant from the Hospital and offers guarantees of safety and comfort, but the use of tele-genetics must be a patient choice.
Data availability
The dataset used and analyzed during the current study are available from the corresponding author on reasonable request.
References
Patrick-Miller L, Egleston BL, Daly M et al (2013) Implementation and outcomes of telephone disclosure of clinical BRCA1/2 test results. Patient Educ Couns 93(3):413–419. https://doi.org/10.1016/j.pec.2013.08.009
Bradbury AR, Patrick-Miller L, Fetzer D et al (2011) Genetic counselor opinions of, and experiences with telephone communication of BRCA1/2 test results. Clin Genet 79(2):125–131. https://doi.org/10.1111/j.1399-0004.2010.01540.x
Mahon SM (2020) Telegenetics: remote counseling during the COVID-19 pandemic. Clin J Oncol Nurs 24(3):244–248. https://doi.org/10.1188/20.CJON.244-248
Buchanan AH, Rahm AK, Williams JL (2016) Alternate service delivery models in cancer genetic counseling: a mini-review. Front Oncol 6:120. https://doi.org/10.3389/fonc.2016.00120
Burgess KR, Carmany EP, Trepanier AM (2016) A comparison of telephone genetic counseling and in-person genetic counseling from the genetic counselor’s perspective. J Genet Couns 25(1):112–126. https://doi.org/10.1007/s10897-015-9848-2
NCCN Clinical Practice Guidelines in Oncology. Genetic/familial high-risk assessment: breast and ovarian. Version 3.2019. http://www.nccn.org
Hilgart J, Hayward J, Coles B et al (2012) Telegenetics: a systematic review of telemedicine in genetics services. Genet Med 14:765–776. https://doi.org/10.1038/gim.2012.40
Zigmond AS, Snaith RP (1983) La scala dell’ansia e della depressione in ospedale. Acta Psychiatr Scand 67:361–430. https://doi.org/10.1111/j.1600-0447.1983.tb09716.x
Costantini M, Musso M, Viterbori P, Bonci F, Del Mastro L, Garrone O et al (1999) Detecting psychological distress in cancer patients: validity of the Italian version of the hospital anxiety and depression scale. Support Care Cancer 7:121. https://doi.org/10.1007/s005200050241
Annunziata M, Muzzatti B, Altoe G (2011) Defining hospital anxiety and depression scale (HADS) structure by confirmatory factor analysis: a contribution to validation for oncological settings. Ann Oncol 22:2330–2333. https://doi.org/10.1093/annonc/mdq750
Ahorsu DK, Lin CY, Imani V, Saffari M, Griffiths MD, Pakpour AH (2020) The fear of COVID-19 scale: development and initial validation [published online ahead of print, 2020 Mar 27]. Int J Ment Health Addict. 20:1–9. https://doi.org/10.1007/s11469-020-00270-8
Soraci P, Ferrari A, Abbiati FA, Del Fante E, De Pace R, Urso A, Griffiths MD (2020) Validation and psychometric evaluation of the Italian version of the fear of COVID-19 scale. Int J Ment Health Addict. https://doi.org/10.1007/s11469-020-00277-1
Romito F, Dellino M, Loseto G, Opinto G, Silvestris E, Cormio C, Guarini A, Minoia C (2020) Psychological distress in outpatients with lymphoma during the COVID-19 pandemic. Front Oncol 10(10):1270. https://doi.org/10.3389/fonc.2020.01270.PMID:32754447;PMCID:PMC7365920
Lobb E, Butow P, Barratt A et al (2004) Communication and information-giving in high-risk breast cancer consultations: influence on patient outcomes. Br J Cancer 90:321–327. https://doi.org/10.1038/sj.bjc.6601502
Metcalfe K, Poll A, Llacuachaqui M, Nanda S, Tulman A, Mian N, Sun P, Narod S (2010) Patient satisfaction and cancer-related distress among unselected Jewish women undergoing genetic testing for BRCA1 and BRCA2. Clin Genet 78:411–417. https://doi.org/10.1111/j.1399-0004.2010.01499.x
DeMarco TA, Peshkin BN, Mars BD, Tercyak KP (2004) Patient satisfaction with cancer genetic counseling: a psychometric analysis of the genetic counseling satisfaction scale. J Genet Counsel 13:293–304. https://doi.org/10.1023/B:JOGC.0000035523.96133.bc
Shannon KM, Emmet MM, Rodgers LH, Wooters M, Seidel ML (2020) Transition to telephone genetic counseling services during the COVID-19 pandemic. J Genet Couns. https://doi.org/10.1002/jgc4.1365
Pagliazzi A, Mancano G, Forzano G et al (2020) Genetic counseling during COVID-19 pandemic: Tuscany experience. Mol Genet Genomic Med 8:e1433. https://doi.org/10.1002/mgg3.1433
Norman ML, Malcolmson J, Randall Armel S, Gillies B, Ou B, Thain E, McCuaig JM, Kim RH (2020) Stay at home: implementation and impact of virtualising cancer genetic services during COVID-19. J Med Genet. https://doi.org/10.1136/jmedgenet-2020-107418
Shaverdian N, Gillespie EF, Cha E, Kim SY, Benvengo S, Chino F, Kang JJ, Li Y, Atkinson TM, Lee N, Washington CM, Cahlon O, Gomez DR (2021) Impact of telemedicine on patient satisfaction and perceptions of care quality in radiation oncology. J Natl Compr Canc Netw. https://doi.org/10.6004/jnccn.2020.7687
McDonald E, Lamb A, Grillo B, Lucas L, Miesfeldt S (2014) Acceptability of telemedicine and other cancer genetic counseling models of service delivery in geographically remote settings. J Genet Couns 23(2):221–228. https://doi.org/10.1007/s10897-013-9652-9
Tarver WL, Haggstrom DA (2019) The use of cancer-specific patient-centered technologies among underserved populations in the united states: systematic review. J Med Internet Res 21(4):e10256. https://doi.org/10.2196/10256.PMID:31012855;PMCID:PMC6658273
Vrečar I, Hristovski D, Peterlin B (2017) Telegenetics: an update on availability and use of telemedicine in clinical genetics service. J Med Syst. 41(2):21. https://doi.org/10.1007/s10916-016-0666-3
Beri N, Patrick-Miller LJ, Egleston BL, Hall MJ, Domchek SM, Daly MB, Ganschow P, Grana G, Olopade OI, Fetzer D, Brandt A, Chambers R, Clark DF, Forman A, Gaber R, Gulden C, Horte J, Long J, Lucas T, Madaan S, Mattie K, McKenna D, Montgomery S, Nielsen S, Powers J, Rainey K, Rybak C, Savage M, Seelaus C, Stoll J, Stopfer JE, Yao XS, Bradbury AR (2019) Preferences for in-person disclosure: Patients declining telephone disclosure characteristics and outcomes in the multicenter communication of genetic test results by telephone study. Clin Genet. 95(2):293–301. https://doi.org/10.1111/cge.13474
Bracke X, Roberts J, McVeigh TP (2020) A systematic review and meta-analysis of telephone vs in-person genetic counseling in BRCA1/BRCA2 genetic testing. J Genet Couns 00:1–11. https://doi.org/10.1002/jgc4.1343
Cunniff C, Bassetti J (2019) Advances in genetic medicine and shared-decision making. J Commun Healthc 12:82–85. https://doi.org/10.1080/17538068.2019.1641279
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
SC interviewed participants, collected their data and is a major contributor in writing the manuscript. MD and MP selected participants for the enrollment. SDS and LM performed statistical analyses. MP performed the internal revision of the paper. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no “competing interest”.
Ethical approval
The current study was reviewed and approved (Prot. n° 897/CE) by Ethical Committee of the IRCCS Istituto Tumori “Giovanni Paolo II”, Bari.
Consent to participate
All participants signed an informed consent.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Costanzo, S., De Summa, S., Maurmo, L. et al. Remote vs in-person BRCA1/2 non-carriers test disclosure: patients’ choice during Covid-19 pandemic restriction. Familial Cancer 22, 43–48 (2023). https://doi.org/10.1007/s10689-022-00307-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10689-022-00307-y