
Abstract
The carcinogenicity of opium consumption was recently evaluated by a Working Group convened by the International Agency for Research on Cancer (IARC). We supplement the recent IARC evaluation by conducting an extended systematic review as well as a quantitative meta-analytic assessment of the role of opium consumption and risk for selected cancers, evaluating in detail various aspects of study quality on meta-analytic findings. We searched the published literature to identify all relevant studies on opium consumption and risk of selected cancers in humans through 31 October, 2022. Meta-relative risks (mRRs) and associated 95% confidence intervals (CIs) were estimated using random-effects models for studies of cancer of the urinary bladder, larynx, lung, oesophagus, pancreas, and stomach. Heterogeneity among studies was assessed using the I2 statistic. We assessed study quality and conducted sensitivity analyses to evaluate the impact of potential reverse causation, protopathic bias, selection bias, information bias, and confounding. In total, 2 prospective cohort studies and 33 case–control studies were included. The overall pooled mRR estimated for ‘ever or regular’ versus ‘never’ use of opium ranged from 1.50 (95% CI 1.13–1.99, I2 = 0%, 6 studies) for oesophageal cancer to 7.97 (95% CI 4.79–13.3, I2 = 62%, 7 studies) for laryngeal cancer. Analyses of cumulative opium exposure suggested greater risk of cancer associated with higher opium consumption. Findings were robust in sensitivity analyses excluding studies prone to potential methodological sources of biases and confounding. Findings support an adverse association between opium consumption and cancers of the urinary bladder, larynx, lung, oesophagus, pancreas and stomach.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Opium is consumed as an illicit recreational narcotic drug, or for medicinal purposes, in more than 50 countries worldwide, with the highest prevalence observed in Western Asia [1]. Opium is typically either ingested or smoked. Opium is the dried latex from the unripe seed-pods of the opium poppy plant. Commonly consumed forms include raw (or crude) opium, opium dross (tarry residues formed after smoking raw opium), and minimally refined opium or opium sap (boiled opium dross with or without added raw opium). Opium contains several addictive alkaloids [2] and (when burned) pyrolysates and may also be contaminated with lead, chromium, and arsenic [3, 4]. Since the 1970s, epidemiological studies conducted in regions of high opium consumption have suggested a positive association between frequent use of opium and cancer risk [5,6,7]. Recent findings from the large-scale Golestan cohort study (GCS) [8]—a cohort of 50,000 individuals followed for more than a decade—have also highlighted adverse associations of opium consumption and cancer risk at several sites.
In 2020, the carcinogenicity of opium was evaluated by a Working Group convened by the International Agency for Research on Cancer (IARC), and opium consumption was classified as “carcinogenic to humans” (Group 1) with sufficient evidence of carcinogenicity in humans for cancers of the urinary bladder, larynx, and lung, and limited evidence for cancers of the oesophagus, stomach, pancreas, and pharynx [2]. Although positive associations were observed, chance, bias, and confounding could not be ruled out by the Working Group for cancer sites where limited evidence was observed [2].
Here, we aimed to supplement the recent qualitative IARC cancer hazard evaluation by conducting an extended systematic review and a quantitative meta-analytic assessment of the role of opium consumption and risk for selected cancers, including cancers of the urinary bladder, larynx, lung, oesophagus, stomach, and pancreas [9]. This analysis therefore represents the most comprehensive systematic review and meta-analysis to date [10,11,12,13,14]. We specifically considered in detail exposure assessment quality, and the impact of various potential methodological sources of bias and confounding on meta-analytic findings according to a registered protocol.
Methods
Literature search and inclusion criteria
The protocol for this systematic review and meta-analysis was registered in Prospero, number CRD42021236030. We conducted extended searches of the published literature to identify all relevant analytical epidemiological studies, comprising cohort and case–control studies on opium consumption and cancer risk in humans. Epidemiological studies that examined the association between opium consumption and cancers of the urinary bladder, larynx, lung, oesophagus, stomach, and pancreas were included because the IARC Monographs evaluation concluded that there was either sufficient or limited evidence in epidemiological studies, and there were at least 3 studies identified for each cancer site in the peer-reviewed literature. Pancreatic cancer was included in the analysis a posteriori of the Prospero protocol publication, because extended literature searches here identified additional publications since the meeting of the IARC Working Group (held during 11–20 September 2020), thereby meeting the criteria for inclusion. No language restrictions were applied. Although there are a few studies on opium use and the risk of other cancers, including cancers of the colon and rectum, brain, liver, lip, oral cavity, and pharynx, due to the small number of available studies for each of these sites, they did not meet the inclusion criteria for this review.
AMF and MCT conducted an extended search of the published literature without time restriction of start date, through 31 October 2022, by searching the following bibliographic databases, namely PubMed, EMBASE and Web of Science. The following MeSH terms were used in: PUBMED: (opium[tw] OR (8006-60-4[m]) AND (neoplasm* OR carcinogen* OR malignan* OR tumor* OR tumour* OR cancer*), and in EMBASE, Mtree-Terms-expanded included: opium:ti,ab,kw AND (neoplasm* OR carcinogen* OR malignan*OR tumor* OR tumour* OR cancer). A detailed description of the online search strategy is available in the Health Assessment Workspace Collaborative (HAWC) software [15] at the following website: https://hawcproject.iarc.fr/assessment/675/. All titles and abstracts were screened by AMF and MCT, followed by screening of the manuscript’s full text where appropriate. All studies that met the eligibility criteria were included in critical appraisal and meta-analysis. There were no exclusions due to study quality or other methodological factors. In some instances, manuscripts reported only information on the prevalence of opium consumption among study participants, but the study was included if measures of association could be calculated (see “Data extraction” below). In the case of multiple publications from the same study, only the most recent or relevant was included. In one included study (Khoo et al. [6]), the exposure reported was opium and/or heroin; there was no information on the proportion of heroin users.
In this systematic review and meta-analysis, we aimed to identify studies according to the following PECO statement, namely: Population (men and women), Exposure (opium consumption by either smoking or oral ingestion), Comparators (members of the same source population with no or minimal opium consumption), and Outcome (incident or fatal cancer of the urinary bladder, larynx, lung, oesophagus, stomach, or pancreas), considering also the time component T (aspects of follow-up, to minimize the potential for protopathic bias or reverse causation). Studies that examined opium consumption prior to cancer occurrence or mortality were identified, with studies of cancer incidence preferred to those of mortality when both were available in the same study population.
Exposure evaluation
Exposure assessment in the included studies was performed either prospectively or retrospectively in relation to cancer outcomes. Prospective exposure assessment occurred where the pattern of opium consumption was captured at study enrolment, and subsequent cancer incidence was examined over follow-up time. In such studies, the risk of cancer was assessed among exposed vs unexposed participants, as well as by intensity of exposure measured at baseline (categories of duration or cumulative use, often in the local unit of nokhod-years [16]). Studies with retrospective exposure assessment were mainly case–control studies of the general population or of patients diagnosed with cancer for whom previous exposure to opium consumption had been evaluated and compared with that of persons without the cancer of interest. This meta-analysis includes only studies that assessed exposure to minimally processed forms of opium (e.g., raw opium, opium dross, minimally refined opium). Populations exposed only to other opiates (e.g., morphine, codeine), semi-synthetic opioids (e.g., heroin, oxycontin), or synthetic opioids (e.g. fentanyl) were not included here. In all primary studies, opium consumption by current or former users was captured through either self- or proxy- completed questionnaires, interviews, or extracted from patient medical records. Consumption of opium was categorized in most studies as ‘ever-user’ or ‘regular user’ versus ‘never user’ of opium. For some studies, duration (years) of opium use and/or cumulative opium consumption were available. Definitions of these categories varied across the studies. For example, in the GCS and several studies that used the GCSQ questionnaire, ‘regular’ use of opium was defined as use at least once per week for at least 6 months. Infrequent users who did not meet this definition were likely included in the ‘never’ use category.
Data extraction
Information on study characteristics, design, and results was extracted by IARC Monographs Working Group members, or by AMF and MCT for newly identified studies published after the completion of the Monographs meeting in September 2020, and verified for completeness and accuracy [2]. Information on a range of study features was extracted including: (a) opium consumption measures (form of opium, route of consumption, cumulative exposure); (b) incident cancer outcome (the only mortality studies identified were of the GCS, which was superseded by an incidence study); (c) socio-demographic characteristics of the study participants, when available; (d) information on potential confounders included in the analyses (with a primary focus on age, sex, tobacco smoking); (e) measure of association (e.g., odds ratio, hazard ratio) and associated 95% confidence intervals (CIs).
Studies in which opium exposure was assessed as "drug addiction" are assumed here to be either smoking or ingestion. Exposure referred to as “snuffing” in Bakhshaee et al. [17], was assumed to be smoking. ORs were estimated either by IARC Monographs Working Group members [18, 19], or (for Khoo and colleagues [6]) estimated elsewhere [13]. Two other included studies [20, 21] provided only the total number of cases and controls and numbers of exposed, so the point estimate and 95% CI were estimated by the authors here. In two studies [22, 23], categories of opium use were combined by the authors here. Nourbakhsh et al. [24] and Tootoonchi et al. [25] were excluded from tabulation in the Monograph [2] because they were considered minimally informative, due to a lack of information on the analysis, population characteristics, and/or exposure to opium, but are included here in our meta-analysis for completeness for the overall analysis.
Quality assessment of each included publication was performed independently by two reviewers (AMF and MCT) using five primary quality assessment criteria defined by the Working Group in relation to studies of opium consumption and cancer risk [2]. Any discrepancies between the two reviewers were resolved by a third reviewer (MSB). The study quality assessment criteria pertained to five factors, including the potential for (1) reverse causation (whether the diagnosis of a cancer type of interest causes a change in opium consumption), (2) protopathic bias (whether opium is consumed in response to symptoms of the cancer type of interest that is still undiagnosed at the time of data collection), (3) selection bias (whether enrolment of study participants is related to both opium consumption and the cancer outcome), (4) information bias (primarily considering the potential for recall bias), and (5) confounding [the extent to which major confounders (including age, sex, and tobacco smoking) were adequately considered, and whether residual confounding of findings was likely to be substantial] for each cancer outcome. Studies were classified by cancer sites into categories of either major, medium, or low concern for each of these five factors, and the potential magnitude and direction of bias were considered (see Appendix). Sensitivity analysis was conducted by excluding studies with major concern for a given factor (see Appendix) and also by including only case–control studies (more details provided in “Statistical models”).
Studies adjusted for tobacco smoking, age and sex were considered to be of higher quality. Smoking-adjusted estimates were preferred in this analysis when available; however, the assessment of the importance of tobacco smoking as a potential confounder varied depending on the strength of the association between tobacco smoking and the cancer site (e.g., for cancers of lung and larynx, tobacco smoking was considered a strong potential confounder).
Statistical analysis
Meta relative-risk (mRR) estimates and associated 95% CIs were calculated using random-effects models to integrate generic inverse variance data. The main parameter estimated is a categorical mRR for ‘ever or regular’ compared with ‘never’ consumption of opium. Given the paucity of available cohort studies, summary mRR estimates were computed using results from all case–control and cohort studies combined (using the rare disease assumption for estimates based on case–control studies [26]). We used generic inverse-variance data and pooled the estimates using random effect models. In brief, we transformed the log values for the odds ratio and relative risk. The standard error was calculated using the 95% confidence interval bounds. To estimate the variance between studies, we employed the Sidik–Jonkman adjustment, which is used in confidence interval estimation when the sample size is small [27]. The adjustment is based on an improvement of the variance parameters, which is performed by combining the variance of the sample size and the sample variance [28].
A series of sensitivity analyses was conducted by excluding studies identified during the quality assessment as having potential major bias or confounding, for example, due to failure to sufficiently account for reverse causation or protopathic bias, or lack of adjustment for important confounders (including age, sex, and tobacco smoking). Heterogeneity among the studies was evaluated using I2 and τ2 (Tau-square) values (we considered values of I2 = 0–25% as representing low heterogeneity, 26–50% moderate heterogeneity and 50–100% high heterogeneity [29]). To investigate potential publication bias we used funnel plots and Begg’s statistic tests.
Although most of the included studies characterised exposure as a dichotomous variable (see above), some studies provided more detailed information on the amount of opium consumed, duration of consumption, and/or cumulative consumption. For these studies, meta-analysis was conducted to further explore associations between the categories of cumulative opium consumption and cancer risk. Cumulative exposure information was available for some studies of cancers of the urinary bladder [8, 30, 31, 43], larynx [8, 32], lung [8, 33, 34], pancreas [8, 35, 36] and stomach [8, 37, 55] (never versus ≤ median and > median use). Estimates of association between ≤ median and > median of cumulative opium exposure compared to never use for various cancers in the GCS [8], and for bladder cancer in the IROPICAN study [38] were obtained through personal communication with the study authors (November 2021, and April 2022, respectively). The models included adjustment for age, sex, and tobacco smoking.
Overall, results fully adjusted for confounding, including tobacco smoking, were used where available. For cancer sites with available results in three or more studies of never-users of tobacco, results were calculated where possible. Statistical analysis was performed using the library “meta” (version. 5.0) [39] in R software v4.1 [40].
Results
Study identification
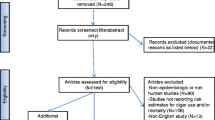
Figure 1 presents details of the inclusion and exclusion criteria to select articles for the systematic review and meta-analysis. In total, 701 studies were identified by the comprehensive literature search after removing duplicates. A total of 106 studies were retained following the first screening of titles and abstracts and the exclusion of studies that were not relevant. Following a second screen of the full text of the manuscripts, 35 studies were included (one publication [41] included two studies). These 35 studies then underwent quality assessment and data abstraction.

Flowchart showing details of the inclusion end exclusion criteria here
Characteristics of studies
Table 1 describes the studies included in the systematic review of opium consumption and cancer, by potential confounding variables considered and route of exposure. All studies were conducted in Asia, almost exclusively in Iran, and were published between the years 1969 and 2022. There were 2 prospective cohort studies and 33 case–control studies. There were a total of six new case–control studies identified following the Monographs meeting [30, 35, 38, 42,43,44]. A total of 15 studies examined the association between opium consumption and bladder cancer (1 cohort and 14 case–control), 7 for laryngeal cancer (1 cohort and 6 case–control), 6 for oesophageal cancer (1 cohort and 4 case–control, one publication [41] describes two separate studies, with different sets of cases and controls), 5 for stomach cancer (2 cohort and 3 case–control), 5 for lung cancer (1 cohort and 4 case–control), and 4 for pancreatic cancer (1 cohort and 3 case–control). The studies included approximately 8400 cancer cases, of whom 2947 reported opium consumption (bladder cancer, n = 1091; oesophageal cancer, n = 295; laryngeal cancer, n = 545; lung cancer, n = 536; pancreatic cancer, n = 231; and stomach cancer, n = 249). The main routes of opium consumption were through smoking and/or ingestion. Most studies provided estimates for both routes combined, while 62% (n = 22) of studies presented risk estimates for consumption by smoking and 40% (n = 17) for consumption by ingestion separately. Most of the studies (77%, n = 27) provided estimates adjusted for age, sex, and tobacco smoking. Most case–control studies used hospital-based controls (33 studies) and one study used neighbourhood controls. As noted above, opium consumption was primarily assessed through interview-based questionnaires. One cohort study (GCS) used a questionnaire at baseline, and exposure estimates from the questionnaire were confirmed by measuring opium consumption metabolites in urine for a sample (n = 150 participants) of the study cohort [45].
Several case–control (n = at least 9) studies also used the GCS questionnaire (GCSQ) [7, 31, 32, 34, 35, 37, 41, 52, 55]. A similarly detailed questionnaire was also used in the IROPICAN study [38, 42, 43, 52]. Other case–control studies ascertained exposure information from telephone calls, face-to-face interviews, patient records or public demographic information and usually characterised exposure as ever/never opium use [5, 17, 19, 22,23,24, 33, 46, 47, 49,50,51, 53]. The GCS [8] provided risk estimates for all the cancer sites investigated here, had high quality exposure information (collected using the GCSQ), as nokhod-years, and distinguished between ingested and smoked opium. For cancer of the oesophagus, two case–control studies had higher quality exposure information [7, 41]. Three of the four lung cancer case–control studies [33, 34, 42], two of the six laryngeal cancer case–control studies [32, 52], and one of the three pancreatic cancer case–control studies [35, 36, 44] also had higher quality exposure information with cumulative exposure estimates. Some bladder cancer case–control studies relied on patient records and did not define a minimum exposure for ‘regular’ user (hence the estimate could be interpreted as for an ‘ever’ user). For bladder cancer, three case–control studies [30, 31, 38] and for stomach cancer, three of the four case–control studies [37, 55] had a measure of intensity of exposure. Exposure quality considerations for most of these studies are extensively described in the published monograph [2].
For each study included in this review, study quality appraisal and assessment of the potential for bias and confounding are provided in the Appendix. The majority of studies were assessed as having either medium or low concern regarding reverse causation or protopathic bias, with the exception of studies of laryngeal cancer and lung cancer where there were major concerns for some studies for these items, as well for confounding. There were major concerns regarding selection and information bias (specifically, exposure misclassification) among studies of several cancer sites.
Risk estimates and heterogeneity
Figure 2 shows a pooled forest plot mRRs (n = 41 study estimates) for opium consumption and cancer from all 35 included studies. Overall, the pooled estimates ranged from 1.50 (95% CI 1.13–1.99), I2 = 0% for cancer of the oesophagus to 7.97 (95% CI 4.79–13.2), I2 = 62% for cancer of larynx. Pooled mRR estimates for ‘ever or regular’ opium consumption compared to ‘never’ consumption among only studies adjusting for tobacco smoking (n = 35 study estimates) were similar (Fig. 3). The tobacco-adjusted pooled estimates ranged from 1.42 (95% CI 1.07, 1.88), I2 = 2% for cancer of oesophagus to 7.89 (95% CI 4.45, 13.98), I2 = 68% for cancer of larynx.

Forest plot for opium consumption and cancer risk, including all studies. (Note: OR/RR = odds-ratio/rate-ratio, *Estimated by the authors, ** both tobacco-adjusted or crude estimates.)

Forest plot for opium consumption and cancer risk, including only studies that adjusted for tobacco smoking (Note: OR/RR = odds-ratio/rate-ratio)
Table 2 shows results of the meta-analysis and sensitivity analyses for the risk of cancer and opium consumption. Overall, there were high levels of heterogeneity observed in most analyses for cancers of larynx, pancreas, and stomach. In an analysis including all studies, heterogeneity was low in the analysis of cancer of the oesophagus (0%), but higher amounts of heterogeneity were observed in analyses of other cancer sites. In the analysis including only case–control studies, observed heterogeneity was reduced for cancers of the lung (0%, n = 3), larynx (42%, n = 5), and stomach (0%, n = 2), but not for bladder and pancreatic cancer. In results of sensitivity analysis that excluded studies of Toutounchi et al. (2000) [25] and Nourbakhsh et al. (2006) [24] that were not considered by the IARC Working Group evaluation (above), findings for bladder cancer were generally similar overall (mRR = 4.19 (95%CI 3.26–5.38), I2 = 49%, and tau2 0.09) and among studies adjusting for tobacco smoking (mRR = 4.15 (95%CI 3.22–5.36), I2 = 45%, and tau2 0.08).
Many of the studies were evaluated as having major concern for selection and information biases, ranging from 20% (stomach cancer) to 67% of studies (oesophageal cancer), and 17% (bladder cancer) to 83% (oesophageal cancer), respectively. The exclusion of studies identified with major concern for reverse causation, protopathic bias, selection bias, information bias, and confounding (primarily related to control for age, sex, tobacco smoking) did not result in important changes in the magnitude of the mRR in analysis for most cancer types and did not decrease the level of heterogeneity among the studies. Visual inspection of the funnel plot and Begg’s test for asymmetry did not suggest any important publication bias (p = 0.07). For bladder cancer (the only site with 3 or more results available among never smokers), the OR for ‘regular or ever’ (compared with ‘never’) use of opium was 3.81 (95% CI 2.70–5.37), I2 = 0% among never-users of tobacco (Table 2).
We also conducted a meta-analysis according to categories of cumulative exposure to opium consumption, comparing a lower-exposed group (≤ median) and higher-exposed group (> median) to never-users of opium where possible (Table 3). Except for lung cancer, results suggest a monotonic increase in the mRRs across the low-to-high categories of opium consumption (e.g., bladder cancer mRRs for the low and high categories of cumulative exposure were 3.70 and 4.87, respectively), but 95% CIs were wide on these estimates.
Discussion
Our study provides the most up-to-date systematic review and quantitative assessment of the association between opium consumption and cancers of the bladder, lung, larynx, pancreas, stomach and oesophagus, enhancing the evidence presented in the IARC Monographs volume 126 [2]. This meta-analysis found a positive association between ‘ever or regular’ (vs. ‘never’) exposure to opium consumption and cancers of the bladder, lung, larynx, stomach, oesophagus, and pancreas. Across the cancer sites, opium ‘ever or regular’ consumers had a 1.5–eightfold increased risk of cancer when compared with those ‘never’ consuming opium, with the strongest associations observed for cancers of the larynx and urinary bladder. These cancer sites, together with lung, may represent organs of greatest initial or elimination exposure to opium or its metabolites [2], although definitive evidence is lacking.
Substantial levels of heterogeneity were found for studies of cancer of the larynx and stomach (which were noted in the IARC Monograph to have a lower proportion of studies with good-quality exposure assessment); nevertheless, the summary mRRs remained similar in magnitude across a variety of sensitivity analyses. High levels of heterogeneity may reduce the reliability of the pooled estimates of mRR. Tobacco smoking has been previously classified as having sufficient evidence for its carcinogenicity in humans for cancers of the bladder, lung, larynx, stomach, and oesophagus [56, 57]. However, it is unlikely that residual confounding from tobacco smoking alone explains the high heterogeneity found for cancers of the stomach and larynx. Residual confounding from tobacco smoking might be expected to result in higher heterogeneity for cancer of the lung and larynx, given its strong association with these cancers. Moreover, cancers of the stomach and larynx represent a wide range of histological subtypes, mostly adenocarcinomas or squamous cell carcinomas, which have different behaviours and probable aetiology. Lack of adjustment for other known risk factors in some studies may have contributed to the heterogeneity, for example, hot beverages for oesophageal cancer [58], and Helicobacter pylori [59] for stomach cancer, although the degree of association between these factors and opium consumption is unknown. Consumption of alcoholic beverages was considered to present a minimal threat of confounding, given the low prevalence of use in the studied populations [53].
Differences in exposure assessment quality among the studies, which were substantial [2], could have contributed to the observed study heterogeneity. One major potential source of heterogeneity was the variable definition of ‘regular or ever’ opium consumption in the included studies. Furthermore, because of limitations in exposure assessment methodology, numbers for the intensity and duration of opium consumption and the cumulative exposure distribution were seldom available in the reviewed studies. Overall, our systematic review shows a wide range of exposure evaluation approaches among the studies; most studies provided only dichotomous classification, while few others provided cumulative exposure evaluation, as either quartiles or tertiles of exposure. Five studies provided median values of cumulative exposure, although they used different metrics (“hookah-years”, nokhod/day-years or g/years). Using the information on median consumption provided by four studies on bladder cancer, three studies on lung, stomach, and pancreas cancers, and two on larynx cancer, we estimated exposure–response relations for cancer risk across cumulative exposure categories (never-users vs lower-than-median and higher-than-median consumption). Our pooled estimates suggested a positive exposure–response relation for most cancer sites. Evidence from the GCS for several cancer sites [8] provides the most precise and relevant information for exposure–response associations between metrics of opium use (duration, cumulative use) and risk of lung cancer, and to a lesser extent for stomach cancer.
The GCSQ, also used in several case–control studies, provided high-quality exposure information including cumulative exposure estimates. Sheikh et al. [8] used the cumulative exposure estimates to show an exposure–response trend which is an indicator of causality. However, the cohort studies collected the opium exposure estimates at baseline, and were not updated over follow-up time; therefore, exposures may have changed.
One important source of heterogeneity in the mRRs not explored here was the geographic variability across Iran in the prevalence and amount of opium consumption. For example, opium consumption rates are lower in the Golestan Province [60] than in some other regions of Iran where epidemiologic studies have been conducted [2]. Furthermore, cumulative exposure based on nokhods or grams consumed may not be accurate, and there is evidence that people may have underestimated opium use in nokhods and overestimated use in grams of opium consumed and that this varies by geographical region [61].
This quantitative assessment aims to supplement the qualitative conclusions made by the IARC Monographs volume 126 Working Group evaluation. The study quality appraisal here includes qualitative aspects considered by the Working Group in the evaluation of the carcinogenicity of opium consumption, with clear and transparent indicators [2]. In our approach, we classified the domains in five categories related to reverse causation, protopathic bias, selection bias, information bias, and confounding. Findings were robust in a range of sensitivity analyses excluding studies with major concern regarding bias or confounding.
Exclusion of studies that did not adjust for tobacco smoking generally had little impact on findings as did restriction of included studies for bladder cancer to those of never-users of tobacco only. Otherwise, as expected, the magnitude of the summary findings, in general, tended to decrease with exclusion of studies with major concern. For example, the strength of the association of opium consumption and cancer of the larynx decreased from 7.97 (95% CI 4.79–13.2) to 5.78 (95% CI 2.49–13.4) with exclusion of studies with major concern for either reverse causation or protopathic bias, of particular concern here as disease symptoms may be alleviated by opium use (i.e., cough). For selection bias, however, studies with major concern may be biased downwards, in the event that selection is related with opium use, for example in a case–control study using unhealthy hospital controls. We found here, however, in most instances, that estimates decreased with exclusion of studies with major concern for selection bias.
The members of the IARC Monographs Working Group calculated three ORs (two for bladder cancer [18, 19], and one for cancer of the larynx [6]). A sensitivity analysis that excluded these studies, however, did not show any significant variation in the pooled estimates or of heterogeneity compared with the main findings (data not shown).
We used a comprehensive and transparent study quality appraisal that independently evaluated major concerns for potential sources of bias and confounding instead of the GRADE system [62], which has been developed for clinical decision-making and is of questionable relevance for synthesis of observational studies of environmental exposures [63, 64]. Additionally, the studies included here were conducted almost exclusively in Iran, which could pose challenges to the generalizability of the findings and may not be representative of use in other countries. Further research to better characterize opium consumption and potential health and cancer risks more globally is warranted.
In one of the few studies performed outside of Iran [6], opium exposure was poorly defined, and an unknown number of heroin users were likely included as part of the opium addicted group. Although opium exposure was poorly defined, is it difficult to speculate how exposure misclassification may impact cases and controls (other cancers) and study findings here.
All studies included in our meta-analysis evaluated cancer risk in relation to exposure to minimally processed forms of illicit opium (e.g., sukteh, teriak). Such “street” opium may contain contaminants and adulterants that are considered integral parts of the complex mixture to which opium users are exposed. Raw opium is formed from more than 25 types of alkaloids representing the major components (10–12%), including phenanthrenes (e.g., morphine, codeine and thebaine) and benzylisoquinolines (e.g., papaverine and noscapine), and non-alkaloids (e.g., sugars, proteins, fats and water among others) [65, 66]. Raw opium is often adulterated and/or contaminated with heavy metals, including some well-known carcinogens (e.g., lead, arsenic, chromium, cadmium [67]). A recent study from the GCS found that blood lead levels were linked to opium usage, for both oral and smoking forms [3].
We observed the strongest associations for smoking-related cancers (bladder, larynx, and lung). This is consistent with findings that opium users are exposed to many of the same carcinogens as tobacco users [68]. IARC Monographs vol. 126 concluded that there was strong mechanistic evidence of genotoxicity for opium dross (sukhteh) and opium pyrolysates (solid residues of combusted opium), in both human peripheral blood mononuclear cells and Chinese hamster ovary cells [69]. Despite scant research, one study in humans exposed to opium also suggests a genotoxic effect of frequent p53 mutations in opium users [70]. More recently, a mutational signature was identified for opium among cases of oesophageal cancer in humans [71]. The carcinogenicity of opium in animal models is still unclear, as no high-quality in vivo experimental carcinogenicity studies have yet been conducted.
Despite the limitations inherent to systematic reviews and meta-analyses, we carefully conducted our review with transparent methods and inclusion and exclusion criteria defined before the data collection. Our sensitivity analysis explored several important sources of bias and heterogeneity, with minimal effects on the results. The results consider estimates adjusted for the main potential confounders (age, sex, tobacco smoking) and stratified by cancer types. Due to limitations in the reporting of most of the studies, we were not able to provide summary risk estimates by quantitative categories of cumulative opium consumption. One limitation of most studies was that the referent category might have included opium users (current and/or past) of low frequency or intensity, underestimating the risk. We found little evidence of publication bias; one notable feature of some of the studies is that opium consumption was not the main exposure being evaluated in primary studies, which may have reduced this potential bias. We also conducted an appraisal of the most important aspects of study quality, and documented a lack of cumulative exposure information, which might be further explored in future studies of opium consumption and cancer risk. Although other meta-analyses have been recently published on opium consumption and cancer risk [10,11,12,13,14], our systematic review is the most up to date, and has carefully considered a range of methodological sources of bias in findings, according to domains of study quality assessment defined by the IARC Monographs volume 126 Working Group.
Our meta-analysis findings provide further support of the IARC Monographs volume 126 Working Group, which classified opium consumption as carcinogenic to humans (Group 1), with sufficient evidence for a causal association for cancers of the bladder, lung and larynx, and limited evidence for a causal association for cancers of pancreas, stomach, and oesophagus [2, 72]. We observed, among studies that adjusted for tobacco smoking, a substantially higher risk of cancers of the bladder and larynx among ever compared with never opium consumers, and somewhat lower elevations in risk for cancers of the lung, stomach, pancreas, and oesophagus. We also observed evidence of positive exposure–response patterns for most cancer sites. The quantitative estimates provided here lend support for developing policies for cancer prevention and control, particularly increasing the awareness of associated hazards of use among opium consumers in affected regions.
References
World Drug Report (United Nations publication, Sales No. E.21.XI.8). GLOBAL OVERVIEW: DRUG DEMAND DRUG SUPPLY [Internet]. 2021. Available from: https://www.unodc.org/res/wdr2021/field/WDR21_Booklet_2.pdf
IARC. Opium consumption. IARC monogr identif carcinog hazards hum. 2021;126:1–253 (Internet).
Etemadi A, Hariri S, Hassanian-moghaddam H, Poustchi H, Roshandel G, Shayanrad A, et al. Lead poisoning among asymptomatic individuals with a long-term history of opiate use in Golestan cohort study. Int J Drug Policy. 2022;104:103695.
Friesen M, O’Neill IK, Malaveille C, Garren L, Hautefeuille A, Cabral JRP, et al. Characterization and identification of 6 mutagens in opium pyrolysates implicated in oesophagel cancer in Iran. Mutat Res Mol Mech Mutagen. 1985;150(1–2):177–91.
MacLennan R, da Costa J, Day NE, Law CH, Ng YK, Shanmugaratnam K. Risk factors for lung cancer in singapore chinese, a population with high female incidence rates. Int J Cancer. 1977;20(6):854–60.
Khoo R. Radiotherapy of carcinoma of the Larynx. Ann Acad Med Singapore. 1981;10(3):307–10.
Nasrollahzadeh D, Kamangar F, Aghcheli K, Sotoudeh M, Islami F, Abnet CC, et al. Opium, tobacco, and alcohol use in relation to oesophageal squamous cell carcinoma in a high-risk area of Iran. Br J Cancer. 2008;98(11):1857–63.
Sheikh M, Shakeri R, Poustchi H, Pourshams A, Etemadi A, Islami F, et al. Opium use and subsequent incidence of cancer: results from the Golestan cohort study. Lancet Glob Health. 2020;8(5):e649–60.
IARC monographs on the evaluation of carcinogenic risks to humans. Report of the IARC advisory group to recommend on quantitative risk characterization Lyon, France: 18–19 November 2013 [Internet]. Available from: https://monographs.iarc.who.int/wp-content/uploads/2018/06/14-001.pdf
Afshari M, Janbabaei G, Bahrami MA, Moosazadeh M. Opium and bladder cancer: a systematic review and meta-analysis of the odds ratios for opium use and the risk of bladder cancer. PLoS ONE. 2017;12(6):e0178527.
Bidary MZ, Sahranavard M, Rezayat AA, Omranzadeh A, Hoseiny SH, Kabirian A, et al. Opium as a carcinogen: a systematic review and meta-analysis. EClinicalMedicine. 2021;33:100768.
Singh G, Jaiswal A, Goel A, Raghav P. Opium usage and risk of head and neck cancer: a systematic review and meta-analysis. Asian Pac J Cancer Prev. 2021;22(3):661–70.
Kamangar F, Shakeri R, Malekzadeh R, Islami F. Opium use: an emerging risk factor for cancer? Lancet Oncol. 2014;15(2):e69-77.
Mansouri M, Naghshi S, Parsaeian M, Sepanlou SG, Poustchi H, Sanat ZM, et al. Opium use and cancer risk: a comprehensive systematic review and meta-analysis of observational studies. Int J Clin Pract. 2022;2022:1–12.
HAWC: Health assessment workplace collaborative [Computer software]. 2013 [Internet]. Available from: https://hawcproject.org
Moossavi S, Mohamadnejad M, Pourshams A, Poustchi H, Islami F, Sharafkhah M, et al. Opium use and risk of pancreatic cancer: a prospective cohort study. Cancer Epidemiol Biomarkers Prev. 2018;27(3):268–73.
Bakhshaee M, Raziee HR, Afshari R, Amali A, Roopoosh M, Lotfizadeh A. Opium addiction and risk of laryngeal and esophageal carcinoma. Iran J Otorhinolaryngol. 2017;29(90):19–22.
Aliasgari MA, Kaviani A, Gachkar L, Hosseini-Nassab SR. Is bladder cancer more common among opium addicts? Urol J. 2004;1(4):253–5.
Aliramaji A, Kaseean A, Yousefnia Pasha YR, Shafi H, Kamali S, Safari M, et al. Age distribution types of bladder cancers and their relationship with opium consumption and smoking. Casp J Intern Med. 2015;6(2):82–6.
Hakami R, Etemadi A, Kamangar F, Pourshams A, Mohtadinia J, Firoozi MS, et al. Cooking methods and esophageal squamous cell carcinoma in high-risk areas of Iran. Nutr Cancer. 2014;66(3):500–5.
Sadjadi A, Derakhshan MH, Yazdanbod A, Boreiri M, Parsaeian M, Babaei M, et al. Neglected role of hookah and opium in gastric carcinogenesis: a cohort study on risk factors and attributable fractions. Int J Cancer. 2014;134(1):181–8.
Sadeghi A, Behmard S, Vesselinovitch SD. Opium: a potential urinary bladder carcinogen in man. Cancer. 1979;43(6):2315–21.
Pournaghi SJ, Hojjat SK, Barazandeh Noveyri F, Tavakkoli Ghouchani H, Ahmadi A, Hamedi A, et al. Tobacco consumption, opium use, alcohol drinking and the risk of esophageal cancer in North Khorasan. Iran J Subst Use. 2019;24(1):105–9.
Nourbakhsh A, Mohseni MG, Hatmi ZN. Opium use in transitional cell carcinoma of the urinary bladder. Acta Med Iran. 2006;44(4):263–7.
Toutounchi M, Mazdak H, Najafipour S, Soleymani B. Bladder cancer risk factors among Isfahan population: a case-control study. J Res Med Sci. 2000;5(2):151–6.
Rothman KJ, Greenland S, Lash TL. Modern epidemiology. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins; 2008.
IntHout J, Ioannidis JP, Borm GF. The Hartung-Knapp-Sidik-Jonkman method for random effects meta-analysis is straightforward and considerably outperforms the standard DerSimonian-Laird method. BMC Med Res Methodol. 2014;14(1):25.
Knapp G, Hartung J. Improved tests for a random effects meta-regression with a single covariate. Stat Med. 2003;22(17):2693–710.
Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–58.
Abdolahinia Z, Pakmanesh H, Mirzaee M, Bazrafshan A, Shafiei Bafti M, Shahesmaeili A. Opium and cigarette smoking are independently associated with bladder cancer: the findings of a matched case - control study. Asian Pac J Cancer Prev. 2021;22(10):3385–91.
Akbari M, Naghibzadeh-Tahami A, Khanjani N, Baneshi MR, Kamali E, Hesampour M, et al. Opium as a risk factor for bladder cancer: a population-based case-control study in Iran. Arch Iran Med. 2015;18(9):567–71.
Alizadeh H, Naghibzadeh Tahami A, Khanjani N, Yazdi-Feyzabadi V, Eslami H, Borhaninejad V, et al. Opium use and head and neck cancers: a matched case-control study in Iran. Asian Pac J Cancer Prev. 2020;21(3):783–90.
Masjedi MR, Naghan PA, Taslimi S, Yousefifard M, Ebrahimi SM, Khosravi A, et al. Opium could be considered an independent risk factor for lung cancer: a case-control study. Respir Int Rev Thorac Dis. 2013;85(2):112–8.
Naghibzadeh-Tahami A, Marzban M, Yazdi-Feyzabadi V, Dabiri S, Mohseni S, Abbasi Rayeni R, et al. Is opium use associated with an increased risk of lung cancer? A case-control study. BMC Cancer. 2020;20(1):807.
Naghibzadeh-Tahami A, Marzban M, Yazdi-Feyzabadi V, Khazaei Z, Zahedi MJ, Moazed V, et al. Opium use as an independent risk factor for pancreatic cancer: a case-control study. Cancer Epidemiol. 2021;75:102017.
Shakeri R, Kamangar F, Mohamadnejad M, Tabrizi R, Zamani F, Mohamadkhani A, et al. Opium use, cigarette smoking, and alcohol consumption in relation to pancreatic cancer. Medicine (Baltimore). 2016;95(28):e3922.
Naghibzadeh Tahami A, Khanjani N, Yazdi Feyzabadi V, Varzandeh M, Haghdoost AA. Opium as a risk factor for upper gastrointestinal cancers: a population-based case-control study in Iran. Arch Iran Med. 2014;17(1):2–6.
Hadji M, Rashidian H, Marzban M, Naghibzadeh-Tahami A, Gholipour M, Mohebbi E, et al. Opium use and risk of bladder cancer: a multi-centre case-referent study in Iran. Int J Epidemiol. 2022;51(3):830–838.
Balduzzi S, Rücker G, Schwarzer G. How to perform a meta-analysis with R: a practical tutorial. Evid Based Ment Health. 2019;22(4):153–60.
R Development Core Team. R Development Core Team. R: A language and environment for statistical computing [computer programme]. Vienna, Austria: R Foundation for Statistical Computing; 2014.
Shakeri R, Kamangar F, Nasrollahzadeh D, Nouraie M, Khademi H, Etemadi A, et al. Is opium a real risk factor for esophageal cancer or just a methodological artifact? Hospital and neighborhood controls in case-control studies. PLoS ONE. 2012;7(3):e32711.
Rashidian H, Hadji M, Gholipour M, Naghibzadeh-Tahami A, Marzban M, Mohebbi E, et al. Opium use and risk of lung cancer: a multicenter case-control study in Iran. Int J Canc. 2023;152(2):203–213.
Rashidian H, Haghdoost AA, Hadji M, Marzban M, Gholipour M, Zendehdel K. Association between opium use and bladder cancer: a case-control study in a high risk area of Iran. Clin Epidemiol Glob Health. 2021;11:100772.
Momayez Sanat Z, Masoudi S, Mansouri M, Ghamarzad Shishavan N, Jameshorani M, Pourshams A. Diabetes mellitus, obesity, and risk of pancreatic ductal adenocarcinoma: a large case-control study from Iran. Middle East J Dig Dis. 2021;13(1):15–20.
Abnet CC, Saadatian-Elahi M, Pourshams A, Boffetta P, Feizzadeh A, Brennan P, et al. Reliability and validity of opiate use self-report in a population at high risk for esophageal cancer in Golestan, Iran. Cancer Epidemiol Biomarkers Prev. 2004;13(6):1068–70.
Ghadimi T, Gheitasi B, Nili S, Karimi M, Ghaderi E. Occupation, smoking, opium, and bladder cancer: a case-control study. South Asian J Cancer. 2015;4(3):111–4.
Hosseini SY, Safarinejad MR, Amini E, Hooshyar H. Opium consumption and risk of bladder cancer: a case-control analysis. Urol Oncol. 2010;28(6):610–6.
Ketabchi A, Gharaei M, Ahmadinejad M, Meershekari T. Evaluation of bladder cancer in opium addicted patients in the Kerman province, Iran from 1999 to 2003. J Res Med Sci. 2005;10(6):355–7.
Lotfi MH, Farzaneh F, Mehrparvar AH, Fallahzadeh MH, Sadeghian MR. The effect of smoking and opium on bladder cancer in Yazd province: a case–control study. SSU. 2016;5:98–109.
Shakhssalim N, Hosseini SY, Basiri A, Eshrati B, Mazaheri M, Soleimanirahbar A. Prominent bladder cancer risk factors in Iran. Asian Pac J Cancer Prev. 2010;11(3):601–6.
Berjis N, Rogha M, Shahabeddini M. The relationship between the opium drug and the risk of laryngeal squamous cell cancer. Ambient Sci. 5 Suppl 1:16–9. https://doi.org/10.21276/ambi.2018.05.sp1.ta01
Mohebbi E, Hadji M, Rashidian H, Rezaianzadeh A, Marzban M, Haghdoost AA, et al. Opium use and the risk of head and neck squamous cell carcinoma. Int J Cancer. 2021;148(5):1066–76.
Mousavi MRA, Damghani MA, Haghdoust AA, Khamesipour A. Opium and risk of laryngeal cancer. Laryngoscope. 2003;113(11):1939–43.
Karajibani M, Montazerifar F, Dashipour A, et al. Nutritional risk factors in the gastric cancer patients attending in Imam Ali Hospital, Zahedan, Iran. RMJ. 2014;39:19–24.
Shakeri R, Malekzadeh R, Etemadi A, Nasrollahzadeh D, Aghcheli K, Sotoudeh M, et al. Opium: an emerging risk factor for gastric adenocarcinoma. Int J Cancer. 2013;133(2):455–61.
IARC. Tobacco smoke and involuntary smoking. IARC Monogr Identif Carcinog Hazards Hum. 2004;83:1–1438 (Internet).
IARC (2012). Personal habits and indoor combustions. IARC Monogr Eval Carcinog Risks Hum, 100E:1–575. [Internet]. Place of publication not identified: International Agency for Research on Cancer; 2012 [cited 2022 May 11]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK304391
IARC. Drinking coffee, mate, and very hot beverages. IARC Monogr Eval Carcinog Risks Hum. 2018;116:1–499 (Internet).
IARC (1994). Schistosomes, liver flukes, and Helicobacter pylori. IARC Monogr Eval Carcinog Risks Hum, 61:1–270. [Internet]. Lyon; 1994. 270 p. (IARC monographs on the evaluation of carcinogenic risks to humans). Available from: https://www.ncbi.nlm.nih.gov/books/NBK304391
Khademi H, Malekzadeh R, Pourshams A, Jafari E, Salahi R, Semnani S, et al. (2012) Opium use and mortality in Golestan cohort study: prospective cohort study of 50,000 adults in Iran. BMJ. 2012;344(apr 17 2):e2502.
Mohebbi E, Kamangar F, Rahimi-Movaghar A, Haghdoost AA, Etemadi A, Amirzadeh S, et al. An exploratory study of units of reporting opium usein Iran: implications for epidemiologic studies. Arch Iran Med. 2019;22(10):541–5.
Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–6.
Steenland K, Schubauer-Berigan MK, Vermeulen R, Lunn RM, Straif K, Zahm S, et al. Risk of bias assessments and evidence syntheses for observational epidemiologic studies of environmental and occupational exposures: strengths and limitations. Environ Health Perspect. 2020;128(9):095002.
Schubauer-Berigan MK, Richardson DB, Fox MP, Fritschi L, Guseva Canu I, Pearce N, Stayner LT, Berrington de Gonzalez A. IARC-NCI Workshop on an epidemiological toolkit to assess biases in human cancer studies for hazard identification: beyond the algorithm. Occup Environ Med. 2023 Jan 30:108724.
Lim H-Y, Kwok S-F. Differentiation and comparison of raw, prepared and dross opium. Vienna: United Nations Office on Drugs and Crime; 1981.
Labanca F, Ovesnà J, Milella L. Papaver somniferum L. taxonomy, uses and new insight in poppy alkaloid pathways. Phytochem Rev. 2018;17(4):853–71.
Cogliano VJ, Baan R, Straif K, Grosse Y, Lauby-Secretan B, El Ghissassi F, et al. Preventable exposures associated with human cancers. J Natl Cancer Inst. 2011;103(24):1827–39.
Etemadi A, Poustchi H, Calafat AM, Blount BC, De Jesús VR, Wang L, et al. Opiate and tobacco use and exposure to carcinogens and toxicants in the Golestan cohort study. Cancer Epidemiol Biomark Prev Publ Am Assoc Cancer Res Cosponsored Am Soc Prev Oncol. 2020;29(3):650–8.
Perry PE, Thomson EJ, Vijayalaxmi, Evans HJ, Day NE, Bartsch H. Induction of SCE by opium pyrolysates in CHO cells and human peripheral blood lymphocytes. Carcinogenesis. 1983;4(2):227–30.
Abedi-Ardekani B, Kamangar F, Sotoudeh M, Villar S, Islami F, Aghcheli K, et al. Extremely high Tp53 mutation load in esophageal squamous cell carcinoma in Golestan Province, Iran. PLoS ONE. 2011;6(12): e29488.
Moody S, Senkin S, Islam SMA, Wang J, Nasrollahzadeh D, Cortez Cardoso Penha R, et al. Mutational signatures in esophageal squamous cell carcinoma from eight countries with varying incidence. Nat Genet. 2021;53(11):1553–63.
Warnakulasuriya S, Cronin-Fenton D, Jinot J, Kamangar F, Malekzadeh R, Dar NA, et al. Carcinogenicity of opium consumption. Lancet Oncol. 2020;21(11):1407–8.
Acknowledgements
Michelle C. Turner is funded by a Ramón y Cajal fellowship (RYC-2017-01892) from the Spanish Ministry of Science, Innovation, and Universities and is co-funded by the European Social Fund. ISGlobal acknowledges support from the Spanish Ministry of Science and Innovation through the “Centro de Excelencia Severo Ochoa 2019-2023” Program (CEX2018-000806-S), and support from the Generalitat de Catalunya through the CERCA Program. The IARC Monographs programme receives funding from the National Cancer Institute (3U01CA033193-38S1).
Author information
Authors and Affiliations
Contributions
AMF, MCT, and MSB designed the protocol and the analysis plan and conducted an extended search of the published literature. AMF and MCT extracted data from original manuscripts and performed the quality assessment. AMF conducted the data analysis. All authors made substantial contributions to the conception or design of the work or the acquisition, analysis, or interpretation of data. AMF, MCT, and MSB drafted the manuscript. All co-authors participated in revising the manuscript. All authors approved the final version.
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare no competing interests.
Ethical approval
Where authors are identified as personnel of the International Agency for Research on Cancer/World Health Organization, the authors alone are responsible for the views expressed in this article and they do not necessarily represent the decisions, policy or views of the International Agency for Research on Cancer/World Health Organization.
Consent to participate
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Appendix
Appendix
List 1. Quality appraisal in cohort and case–control studies of opium exposure and cancer. (Three main categories: major concern, medium concern, low concern)
-
1.
Reverse causation (defined outcome of interest causes a change in the exposure of interest)
-
2.
Protopathic bias (if a person uses opium in response to a symptom of an outcome of interest that is, at the time of exposure, still undiagnosed; and, if those with symptoms have a higher probability of the outcome).
-
3.
Selection bias.
-
4.
Information bias, including recall bias.
-
5.
Confounding.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
M. Filho, A., Turner, M.C., Warnakulasuriya, S. et al. The carcinogenicity of opium consumption: a systematic review and meta-analysis. Eur J Epidemiol 38, 373–389 (2023). https://doi.org/10.1007/s10654-023-00969-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10654-023-00969-7