
Abstract
The Horizon2020 LifeCycle Project is a cross-cohort collaboration which brings together data from multiple birth cohorts from across Europe and Australia to facilitate studies on the influence of early-life exposures on later health outcomes. A major product of this collaboration has been the establishment of a FAIR (findable, accessible, interoperable and reusable) data resource known as the EU Child Cohort Network. Here we focus on the EU Child Cohort Network’s core variables. These are a set of basic variables, derivable by the majority of participating cohorts and frequently used as covariates or exposures in lifecourse research. First, we describe the process by which the list of core variables was established. Second, we explain the protocol according to which these variables were harmonised in order to make them interoperable. Third, we describe the catalogue developed to ensure that the network’s data are findable and reusable. Finally, we describe the core data, including the proportion of variables harmonised by each cohort and the number of children for whom harmonised core data are available. EU Child Cohort Network data will be analysed using a federated analysis platform, removing the need to physically transfer data and thus making the data more accessible to researchers. The network will add value to participating cohorts by increasing statistical power and exposure heterogeneity, as well as facilitating cross-cohort comparisons, cross-validation and replication. Our aim is to motivate other cohorts to join the network and encourage the use of the EU Child Cohort Network by the wider research community.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Non-communicable diseases (NCDs) such as cardiovascular disease, cancer, chronic respiratory disease and diabetes represent a major global health challenge and are the leading cause of death worldwide. Of the 56.9 million deaths that occurred in 2016, 40.5 million (71%) were from NCDs [1]; this number is estimated to rise to 52 million by 2030 [2]. To address the growing economic and health burden that NCDs represent, the United Nations’ Sustainable Development Goal (SDG) target 3.4 aims to reduce premature mortality due to NCDs by one third by 2030 through prevention, treatment and promotion of mental health and wellbeing [1].
Early-life offers an important window of opportunity for achieving this target. Evidence strongly suggests that environmental conditions and exposures during intrauterine and early postnatal life can influence anatomical, physiological and biochemical processes and, in so doing, impact future health [3]. Longitudinal pregnancy and child cohort studies provide a means of investigating this phenomenon, including how early-life exposures influence health trajectories, and identifying potential early-life interventions to improve health outcomes [4]. However, such studies are expensive to establish and maintain, which often prohibits the large-scale studies required to investigate rare outcomes or exposures, or conduct more advanced statistical analyses to investigate, for example, causality or lifecourse health trajectories.
Cross-cohort collaborations offer a cost-effective approach to increase the statistical power of such analyses. They also provide other benefits such as increased exposure heterogeneity, facilitated cross-cohort comparisons, the ability to cross-validate, replicate and establish the generalisability of findings, and the opportunity to share expertise and knowledge. In recent years, a number of such collaborations have been successfully established, for example the CHICOS (www.chicosproject.eu), BioSHARE [5], HELIX [6] (www.projecthelix.eu), PACE [7], EGG/EAGLE [8], ESCAPE [9] (www.escapeproject.eu) and Enrieco [10] (www.enrieco.org) projects, which have led to the identification of a number of associations that may have otherwise gone unobserved [11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28]. More recently, in 2017, building on expertise gained from these collaborations, the Horizon 2020-funded LifeCycle project was established [29] (www.lifecycle-project.eu).
LifeCycle aims to facilitate the utilisation of data from mainly European, but also some non-European, cohort studies for research. It has a particular focus on preconception, fetal and early childhood exposures and their influence on cardio-metabolic, respiratory and mental health trajectories. To achieve its aim, LifeCycle has established the EU Child Cohort Network, a sustainable data resource and infrastructure which is built around making each participating cohort’s data findable, accessible, interoperable and reusable (FAIR) [30]. The network currently holds data on approximately 250,000 children and their parents from an initial 16 European and one Australian cohort.
An overview of the EU Child Cohort Network, including the data management and governance structure on which the network is based, plus its primary research themes, was provided by Jaddoe et al. in a previous edition of this journal [29]. Here we provide a detailed description of the EU Child Cohort Network’s core variables, which are a set of basic variables, derivable by the majority of participating cohorts and required for most analyses in lifecourse research. We describe firstly the process by which the list of core variables was established; secondly the protocol developed to harmonise these core data, which defines the harmonisation process adopted generally within LifeCycle; thirdly the catalogue developed to ensure that all EU Child Cohort Network data are both findable and reusable; finally the core data themselves, including the variables harmonised by each cohort and the total number of children with harmonised data. Our aims are to: (1) enable an accurate assessment of the quality and validity of the harmonised core data through transparency of our methods; (2) motivate other cohorts to contribute to the network; (3) encourage the use of the EU Child Cohort Network’s data by the wider scientific community.
Methods
Participating cohorts
An overview of the 17 cohorts that established the EU Child Cohort Network is provided in Table 1. Further details of each cohort can be found in Jaddoe et al. [29], the EU Child Cohort Network Variable Catalogue (http://catalogue.lifecycle-project.eu) and each cohort’s profile paper [31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49]. The network is open for other cohorts to join, provided they meet the following criteria: (1) commenced before or during pregnancy or in infancy; (2) plan to follow-up or already have followed-up the cohort throughout childhood; (3) are willing to harmonise data and make them available to researchers using the network. Cohorts can join the network by contacting the coordinating centre (lifecycle@erasmusmc.nl). Similarly, proposals for research based on EU Child Cohort Network data can be put forward by both LifeCycle partners and external researchers by also contacting the coordinating centre (lifecycle@erasmusmc.nl). Proposals for research may be based on all EU Child Cohort Network cohorts or a subset of cohorts with available data; they may also include requests for further data harmonisation, which can likewise be restricted to a subset of cohorts with data.
Harmonisation
The EU Child Cohort Network’s core variables are a set of basic, predominantly “lowest common denominator” variables, derivable by the majority of participating cohorts and frequently needed as covariates or exposures in lifecourse research. The process adopted in LifeCycle to establish and harmonise these core variables for the EU Child Cohort Network can be broken down into eight steps; an overview of these steps is displayed in Fig. 1. A glossary of the key elements and concepts described in this paper is also provided in Box 4.

The process adopted in LifeCycle to establish and harmonise the core variables for the EU Child Cohort Network
Step 1: establishing a preliminary list of target core variables
LifeCycle partners with expertise in a wide range of fields including lifecourse epidemiology, public health, environmental epidemiology, biology, statistics, paediatrics, obstetrics, economics, demography, epigenomics and data science, met in a dedicated workshop (June 2017) to identify a preliminary list of core early-life stressors and exposures related to cardio-metabolic, respiratory and mental health outcomes using a consensus approach. This initial list was then further modified by drawing on experiences from other previous collaborative efforts such as MOBAND [50] and CHICOS (www.chicosproject.eu), and through consulting the literature and experts in the field, before being circulated amongst LifeCycle partners for further comment.
Steps 2, 3 & 4: collating codebooks, evaluating the harmonisation potential of each variable and finalising a list of target core variables
All cohorts participating in LifeCycle were requested to provide the coordinating team with cohort metadata (codebooks, questionnaires, instrument documentation, etc.). From these, the potential for each cohort to derive each target variable was established. The core variable list was then adapted in an iterative manner to achieve a balance between precision and inclusivity, ensuring a maximum number of cohorts could contribute data for numerous variables while maintaining data validity. Where possible, international standards and classification schemes were applied. For example, the International Standard Classification of Occupation 1988 1-digit codes [51] were used to categorise parental occupation; the International Standard Classification of Education 97/2011 schemes [52, 53] were used to classify parental education; the WHO fetal growth charts [54] were used to establish size-for-gestational-age; the EUROCAT guide was used for classifying congenital anomalies. For some key exposures such as maternal smoking, breastfeeding, childcare attendance and gestational age, several variables were included, with some variables capturing more information but at the cost of fewer cohorts being able to derive the variables. Repeated measures were also included, to capture the dynamic, longitudinal nature of many variables.
Step 5: pilot harmonisation
Data harmonisation was staggered across cohorts. First, an initial pilot harmonisation was conducted among four cohorts covering the majority of target core variables (the Danish National Birth Cohort, the EDEN mother-child cohort, the Generation R study and the Southampton Women’s Survey). This enabled any potential issues in the core variable list to be identified and rectified. During the pilot harmonisation, the core variable list was revised iteratively through electronic communication, a workshop and a final teleconference.
Step 6: data harmonisation and local quality control
Harmonisation for the EU Child Cohort Network was carried out locally by each participating cohort. This avoided any transfer of data but carried the risk of harmonisation protocols being interpreted differently by different cohorts. To limit this possibility, a detailed harmonisation manual was drawn up by the coordinating team, and supervision and feedback was maintained between the coordinating centre and each of the cohorts. The harmonisation manual is available to download from the LifeCycle website (https://lifecycle-project.eu); it includes: (1) a final, annotated list of core variables, which, for each variable, includes: a variable name, a precise definition, a label, units, data type, permissible values and guidelines for what constitutes partial versus complete harmonisation (see Box 4 for definitions of partial vs. complete harmonisation); (2) relevant scale conversions; (3) relevant reference tables (e.g. WHO fetal growth charts, the EUROCAT guide for classifying congenital anomalies etc.). The harmonisation manual was circulated to cohorts in May 2018 and harmonisation of core variables by all cohorts was completed by May 2020. The duration of time that it took a cohort to harmonise all core variables ranged from three to eight months.
Once data were harmonised, each cohort was provided with detailed quality control instructions and scripts to check: (1) that variables matched the descriptions provided in the core variable list (name, datatype, values); (2) for outliers or improbable values; (3) for inconsistencies between non-repeated measures (e.g. all mothers coded as not smoking during pregnancy were also coded as smoking zero cigarettes during pregnancy); (4) for inconsistencies between repeated measures (e.g. children reducing height over time). Any inconsistencies identified were investigated on a cases-by-case basis to establish which values were legitimate and which were errors, also in light of the other data available.
Step 7a: uploading harmonisation descriptions to the EU Child Cohort Network variable catalogue
To facilitate the utilisation of EU Child Cohort Network data for research, and ensure the complete and accurate documentation of harmonisation, an online catalogue of EU Child Cohort Network variables was developed using the Molgenis platform [55] (http://catalogue.lifecycle-project.eu). This open source, searchable catalogue includes detailed descriptions of each variable included in the EU Child Cohort Network (variable name, data type, values, unit and description), as well as details of which cohorts have harmonised each variable, whether that harmonisation was complete or partial, an explanation of how the variable was harmonised, plus the syntax and descriptions of the source variables used by each cohort to derive the variable (Fig. 2). For the core variables, documentation of harmonisation was conducted by each cohort and uploaded to the catalogue after harmonisation was complete.

An illustration of the EU Child Cohort Network Variable Catalogue displaying the LifeCycle variable “maternal history of asthma before pregnancy”. Displayed is a description of the target EU Child Cohort Network variable and how the variable was harmonised in two separate cohorts. Note: descriptions from two separate cohorts are displayed on the same page for illustrative purposes only
The catalogue has been built using a logical tree structure, but variables can also be located using a search function (Fig. 3). There are plans to also incorporate descriptive summary statistics for each harmonised variable. Thus, the EU Child Cohort Network Variable Catalogue provides a comprehensive overview of the EU Child Cohort Network’s data, ensuring they are both findable and reusable, as well as contributing to the longer-term sustainability of the network.

An illustration of the EU Child Cohort Network Variable Catalogue’s menu structure giving an overview of the themes included in the EU Child Cohort Network and the number of variables included in each theme. 1Including yearly-repeated variables with up to 18 measures between the ages of 0 and < 18 years. 2Including weekly-repeated variables with up to 43 measures taken between gestational weeks 0 and < 43. 3Including trimester-repeated variables with separate measures for the first, second and third trimesters. 4Including separate variables indicating the type of father the variable relates to (biological, social father, social mother, unknown). 5Including separate variables relating to secondary father-figures. 6Including monthly-repeated variables with up to 216 measures between the ages of 0 and < 216 months. 7Including yearly-repeated variables with up to four measures between the ages of 0 and < 4 years. 8Including yearly-repeated variables with up to 13 measures between the ages of 0 and < 13 years
Step 7b: uploading data to a data management platform for the federated analysis of data
To help ensure the sustainability and accessibility of the EU Child Cohort Network, an IT infrastructure has been implemented enabling the federated analysis of data. Full details of this infrastructure are given elsewhere [29, 56, 57]. Briefly, this infrastructure consists of secure Opal servers [58] located either at each host institution or on outsourced IT infrastructures. Once harmonisation is complete, each cohort uploads their harmonised data to their Opal server, where they remain stored, behind secure firewalls. Individual-level data are accessed via an RStudio Open Source central analysis server (https://rstudio.com/products/rstudio/#rstudio-server) using the R-based platform DataSHIELD [56], which sends blocks of code to each Opal server and then combines the summary statistics that are sent back by each Opal server. There is no transfer of individual participant data to the researcher and a number of disclosure control filters ensure analyses are non-disclosive, thus the many ethical, legal and societal implications of transferring data from one site to another are avoided.
Step 8: central quality-control
Quality of harmonised data was assessed at the central level by creating summary statistics for each core variable in R/DataSHIELD. This was to identify outliers and improbable values and inconsistencies in data as outlined above, but also to identify large inconsistencies between cohorts. Where large inconsistencies were found, sampling and recruitment methods and differences in the instruments used to collect data were investigated, as well as the harmonisation process itself, in order to establish to what extent these differences were real versus an artefact of differing methodology.
Results
Table 1 provides an overview of the 17 cohorts currently contributing data to the EU Child Cohort Network. As of June 2020, the network holds data on just under 250,000 children and their parents, with contributing cohorts ranging in size from 967 to 76,569 children. This is an initial number and will increase as new cohorts and their parent-child triads join the network.
First and last year of recruitment of cohorts ranged between 1934 (HBCS) and 2016 (NINFEA) respectively. Mean age of children at recruitment ranged from -1084 days before birth (approximately -3 years, in SWS, which recruited mothers before conception) to 17 days postpartum (in CHOP). The majority of mothers enrolled in the cohorts were recruited during pregnancy (13 of the 17 currently participating cohorts).
Tables 2 and 3 summarise some key characteristics of the mother-child dyads from each cohort currently contributing data to the EU Child Cohort Network. Of note is the variation in the proportion of children born small and large for gestational age (ranging from 2.2% in CHOP to 11.2% in BiB and from 2.7% in CHOP to 14.2% in NFBC1986 for SGA and LGA respectively) and the proportion of children ever breastfed (ranging from 73.4% in EDEN to 99.6% in HBCS). Also of note is the variation in the proportion of mothers with a high level of education (ranging from 3.3% in NFBC1966, most likely reflecting the earlier year of recruitment of this cohort, to 67.5% in MoBa) and the proportion of mothers who smoked during their pregnancy (ranging from 7.6% in NINFEA which is based in Italy, where the prevalence of smoking among women and especially pregnant women is known to be lower [59], to 33.1% in Rhea). Multiparity ranged between 27% in NINFEA and 69% in NFBC1966.
Although we focus here on describing the EU Child Cohort Network’s core variables, the network also includes variables relating to the early-life exposome, encompassing both the external environment (socio-economic, migration, urban environment and lifestyle factors) and internal environment (determined from biological markers such as DNA methylation, RNA expression and metabolomics), and outcome variables relating to cardio-metabolic, respiratory and mental health. An overview of all the themes of the EU Child Cohort Network is provided in Fig. 3, together with estimates of the total number of variables included in each theme. Due to the fact that new variables are continuously being added to the network with the inception of new research projects, these numbers are highly conservative.
The core variables consist of a set of 130 basic, principally lowest common denominator variables, available in the majority of participating cohorts and required for many analyses within the scope of LifeCycle and other lifecourse epidemiology research themes. Of these, seven are so-called “meta variables”, consisting of mother, child, pregnancy, and cohort identifiers, and variables providing the age of recruitment and country of cohort. The remaining variables consist of 96 non-repeated variables and 17 yearly-repeated variables with up to 18 measures between the ages of 0 and < 18 years, together capturing maternal, paternal and child health, lifestyle, socio-demographic characteristics, mother’s obstetric history, birth outcomes and household exposures. There are also two trimester-repeated variables capturing maternal smoking and alcohol consumption during pregnancy, four yearly-repeated variables with up to four measures between the ages of 0 and < 4 years capturing childcare and four monthly-repeated variables with up to 216 height or weight measures between the ages of 0 and 215 months. The full list of EU Child Cohort Network core variables is provided in Online Resource 1 and also in the EU Child Cohort Network Variable Catalogue (http://catalogue.lifecycle-project.eu). Since the EU Child Cohort Network Variable Catalogue is dynamic and regularly expanded with both new variables and newly participating cohorts, the statistics reported there may differ from what is presented here.
Excluding the seven meta-variables, the percentage of core variables harmonised by cohorts ranged from 21% for HBCS to 92% for ELFE (Fig. 4). Missing variables are due to cohorts not having the data required to harmonise the variable. Twelve of the 17 cohorts currently included in the EU Child Cohort Network were able to harmonise at least 50% of core variables completely, and 12 of the 17 cohorts were able to harmonise at least 75% of core variables either completely or partially.

Percentage of EU Child Cohort Network core variables harmonised by each cohort. The figure displays the percentage of the 123 core variables listed in Online Resource 1 (excluding meta-variables) harmonised by each cohort. Shading of bars displays the degree of matching within each cohort: black bars represent percentage of completely harmonised variables; dark grey bars represent percentage of partially harmonised variables; light grey bars represent percentage of variables that were not harmonizable (impossible harmonisation)
Figures 5, 6 and 7 give an overview of the number of EU Child Cohort Network children (i.e. from all cohorts combined) with harmonised core data. Of the non-repeated core variables (Fig. 5), themes with the most complete data are those relating to maternal characteristics (specifically, age at birth, height, smoking during pregnancy, parity) and child-related characteristics (specifically, sex, gestational age at birth, birth weight, birth length, size for gestational age and death of the child), with more than 217,000 children as of June 2020 having harmonised data relating to these exposures. Notably fewer children have data relating to mother and father’s country of birth and ethnic background, perhaps due to their sensitive nature [60].

Harmonised non-repeated core variables in the EU Child Cohort Network. Bars display the number of children with either a partially (grey bars) or completely (black bars) harmonised core variable for each of the main themes/exposures. The dashed line represents the total number of children (240,684), as of June 2020, contributing data to the EU Child Cohort Network with all three of the following variables harmonised: (1) birth weight, (2) sex, (3) at least one height or weight measurement taken at ≥ 1 year. COB country of birth, PE pre-eclampsia, gest. HT gestational hypertension, size for GA size for gestational age

Number of children in the EU Child Cohort Network with yearly-repeated measure core variables. Bars display the number of children with at least one measure between the ages of zero and three (child-care variables) or zero and seventeen (all other variables), either partially (grey bars) or completely (black bars) harmonised. The dashed line represents the total number of children (240,684), as of June 2020, contributing data to the EU Child Cohort Network with all three of the following variables harmonised: i) birth weight, ii) sex, iii) at least one height or weight measurement taken at ≥ 1 year

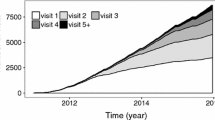
Weight and height data in the EU Child Cohort Network. Graphs display a number of children in the network with at least one weight (dark grey bars) or height (light grey bars) measure at < 3 months, 3–6 months, 6–12 months and yearly intervals from 1 to 17 years; b total number of weight (dark grey bars) and height (light grey bars) within each age band (i.e. one child may contribute multiple measurements within each age band)
An overview of the number of EU Child Cohort Network children with harmonised yearly-repeated core variables, which allow for time-varying exposure statuses, is displayed in Fig. 6. Over 80% of children in the network have at least one harmonised measure of cohabitation status, mother’s occupational status, mother’s education level, father’s occupational status, father’s education level, and child’s exposure to pets and cigarette smoke, whilst relatively few children (< 10%) have harmonised data on household income. For growth data (Fig. 7), the greatest density of measures in the network is between the ages of 0 and < 1 year, with a total of 780,993 and 732,202 weight and height measurements available between these ages respectively, an average of three weight and height measures per child. Large amounts of growth data are also available for ages 1– < 2 years and 7– < 8 years, with over 72% and 47% of children having harmonised weight and height data at these ages respectively, whilst relatively few children currently have weight and height data from 14 years and onwards, partly because many cohorts have not yet reached that age.
Discussion
The Horizon 2020 LifeCycle Project is a collaboration between scientists from more than 17 pregnancy and birth cohorts from across Europe and Australia. It builds upon the expertise gained from previous collaborations such as the CHICOS, Enrieco and BioSHARE projects in order to establish an open and sustainable data resource known as the EU Child Cohort Network so as to facilitate research on the influence of early-life stressors on later health outcomes.
Here we have described the EU Child Cohort Network, focussing on its core variables, including the protocol developed to harmonise these data and thus make them interoperable. We have also described the EU Child Cohort Network Variable Catalogue, developed to ensure that these and other data in the network are both findable and re-usable. These data will be analysed using a federated analysis platform, meaning there is no need to physically transfer data, and so data are ultimately more accessible to the researcher.
As well as the harmonised core data described here, the EU Child Cohort Network also contains data relating to the early-life exposome, and repeated measures of cardio-metabolic, respiratory and mental health. An additional feature of the network is the varied social, cultural and political environments of the cohorts. Thus, the EU Child Cohort Network constitutes an invaluable data resource, not only in terms of the number of participants included, but also in terms of its breadth, depth and diversity. This will ultimately enable the application of a range of analytical approaches to help infer causality, and identify possible target groups for improved cardio-metabolic, respiratory and mental health across the lifecourse.
However, the creation of such a data resource is not without its limitations. Firstly, the resources required to create a common dataset, i.e. harmonise data, should not be underestimated. Harmonising data is difficult, time consuming and requires considerable investment by all involved. Although central harmonisation, whereby individual participant data are sent to one coordinating centre which harmonises all variables, is often viewed as the more optimal approach, this is not without its drawbacks. Firstly, there are many ethico-legal challenges surrounding the transfer of data; secondly, it takes considerable investment by the data manager to become acquainted with a cohort’s data, scaled up 17 times in the case of the EU-Child Cohort Network, potentially leading to errors. It is for these reasons, and the fact that the EU Child Cohort Network is an open network, such that new cohorts are invited to join and are continually joining, that LifeCycle opted for local harmonisation. Here, harmonisation is carried out locally by each cohort, coordinated by a central coordinating centre. This of course has the limitation that harmonisation protocols may be interpreted differently by different cohorts. We have tried to limit this possibility in LifeCycle by providing detailed instructions and maintaining regular contact with data managers. We have also implemented a number of data quality checks, applied both locally and centrally. These include checks to ensure that harmonised variables match those detailed in the harmonisation manual and to identify outliers or improbable values, or any inconsistencies in measures within or between cohorts. Good documentation of all harmonisation steps is key to diagnosing any inconsistencies, which we have ensured in LifeCycle by establishing the EU Child Cohort Network Variable Catalogue.
Another drawback of data harmonisation is that the end product is often the “lowest common denominator”. For any given variable, some cohorts will inevitably have more detailed variables than other cohorts. In an attempt to create a common variable achievable by all cohorts, more detailed variables are stripped down to simpler versions, inevitably resulting in some loss of information. This may also involve deciding that in some cohorts there is insufficient data to harmonise a variable. Harmonisation is thus a balancing act between retaining as much information as possible while ensuring data are fully comparable [61].
So, if the creation of a common dataset is such a tremendous task and the end product may, in some instances, be less detailed than the original data, why bother? Increased statistical power is one obvious advantage. Combining data from several cohorts to increase power allows rarer, but equally important and often more devastating [62], diseases and rare determinants to be studied. Larger sample sizes also allow for more powerful statistical analyses, such as exploring multiple interactions, complex nonlinear relationships, small effects or dose responses [63]. While national registers offer the possibility of creating birth cohorts of an order of magnitude larger than the EU Child Cohort (for e.g. Nordic register-based cohort studies [64, 65]), these typically lack the in-depth lifestyle and behavioural data obtained from questionnaires, or physiological data obtained from detailed clinical examinations. National register data are in addition likely to offer less diversity with respect to social, cultural and political environment. Cross-cohort collaborations also allow fine resolution biological data to be shared, such as medical images or metagenomic data, that may be prohibitively costly to obtain from the entire cohort and therefore only collected from a sub-population of the cohort.
A larger sample size is not the only benefit of cross-cohort collaborations. Combining data also offers the opportunity to study populations typically under-represented in cohort studies, for example individuals from lower socio-economic backgrounds or ethnic minority groups. Heterogeneities between cohorts can be utilised to strengthen causal inference. For example, differing confounding structures allows the untangling of true associations, whilst replication of findings across different populations with differing gene pools, and cultural and socio-economic structures, helps to rule out chance findings while also establishing the generalisability of results. Geographical, intergenerational and period effects can also be examined to find new associations and generate new hypotheses.
While it could be argued that an easier and potentially less time-consuming approach to combining data from several studies is the more conventional systematic review and meta-analysis of published data, this has a number of disadvantages compared to individual participant data (IPD) meta-analysis. Published data are often subject to selective reporting and publication bias, lack harmonised measures, and offer limited scope and flexibility in terms of statistical analysis, and few opportunities, if any, for data checking [66, 67].
The added value that the collaboration itself brings should also be highlighted: the opportunity to share ideas and methodology, learn from each other, and ultimately strengthen research outputs. Also the increased use of data and exchange opportunities for researchers. Scientific collaboration also facilitates the dissemination of both results and ideas/hypotheses, as well as creating opportunities for interdisciplinary research.
In conclusion, the EU Child Cohort Network offers an invaluable data resource for studying how early-life exposures influence health trajectories throughout the lifecourse. This is both in terms of the number of its participants, and the breadth and depth of its data. Here we share the approach taken within LifeCycle to harmonise the network’s core data and describe the EU Child Cohort Network Variable Catalogue established to ensure that the network’s data are both findable and reusable. We also highlight some of the great benefits of cross-cohort collaboration. Having hopefully convinced the reader of the benefits of the EU Child Cohort Network and similar cross-cohort collaborations, we end with a plea to other cohorts to join the network and share their data, and to researchers to utilise this incredible resource. Both cohorts and researchers can join the network by contacting lifecycle@erasmusmc.nl.
Availability of data and material
Proposals for research based on EU Child Cohort Network data can be put forward by contacting the coordinating centre (lifecycle@erasmusmc.nl).
Code availability
Available on the LifeCycle GitHub (https://github.com/lifecycle-project).
References
GBD 2017 SDG Collaborators. Measuring progress from 1990 to 2017 and projecting attainment to 2030 of the health-related Sustainable Development Goals for 195 countries and territories: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):2091–138. https://doi.org/10.1016/s0140-6736(18)32281-5.
Mendis S. Organizational update: the world health organization global status report on noncommunicable diseases 2014; one more landmark step in the combat against stroke and vascular disease. Stroke. 2015;46(5):e121–2.
Hanson MA, Gluckman PD. Early developmental conditioning of later health and disease: physiology or pathophysiology? Physiol Rev. 2014;94(4):1027–76. https://doi.org/10.1152/physrev.00029.2013.
Larsen PS, Kamper-Jorgensen M, Adamson A, et al. Pregnancy and birth cohort resources in Europe: a large opportunity for Aetiological Child Health Research. Paediatr Perinat Epidemiol. 2013;27(4):393–414. https://doi.org/10.1111/ppe.12060.
Doiron D, Burton P, Marcon Y, et al. Data harmonization and federated analysis of population-based studies: the BioSHaRE project. Emerg Themes Epidemiol. 2013;10(1):12. https://doi.org/10.1186/1742-7622-10-12.
Maitre L, de Bont J, Casas M, et al. Human Early Life Exposome (HELIX) study: a European population-based exposome cohort. BMJ Open. 2018;8(9): https://doi.org/10.1136/bmjopen-2017-021311.
Felix JF, Joubert BR, Baccarelli AA, et al. Cohort profile: pregnancy and childhood epigenetics (PACE) consortium. Int J Epidemiol. 2018;47(1):22-3u. https://doi.org/10.1093/ije/dyx190.
Middeldorp CM, Felix JF, Mahajan A, McCarthy MI. The Early Growth Genetics (EGG) and EArly Genetics and Lifecourse Epidemiology (EAGLE) consortia: design, results and future prospects. Eur J Epidemiol. 2019;34(3):279–300. https://doi.org/10.1007/s10654-019-00502-9.
Pedersen M, Giorgis-Allemand L, Bernard C, et al. Ambient air pollution and low birthweight: a European cohort study (ESCAPE). Lancet Respir Med. 2013;1(9):695–704. https://doi.org/10.1016/S2213-2600(13)70192-9.
Vrijheid M, Casas M, Bergstrom A, et al. European birth cohorts for environmental health research. Environ Health Perspect. 2012;120(1):29–37. https://doi.org/10.1289/ehp.1103823.
Birks L, Casas M, Garcia AM, et al. Occupational exposure to endocrine-disrupting chemicals and birth weight and length of gestation: a European meta-analysis. Environ Health Perspect. 2016;124(11):1785–93. https://doi.org/10.1289/EHP208.
Casas M, den Dekker HT, Kruithof CJ, et al. Early childhood growth patterns and school-age respiratory resistance, fractional exhaled nitric oxide and asthma. Pediatr Allergy Immunol Off Publ Eur Soc Pediatr Allergy Immunol. 2016;27(8):854–60. https://doi.org/10.1111/pai.12645.
Casas M, den Dekker HT, Kruithof CJ, et al. The effect of early growth patterns and lung function on the development of childhood asthma: a population based study. Thorax. 2018;73(12):1137–45. https://doi.org/10.1136/thoraxjnl-2017-211216.
LifeCycle Project-Maternal Obesity Childhood Outcomes Study Group, Voerman E, Santos S, et al. Association of gestational weight gain with adverse maternal and infant outcomes. JAMA. 2019;321(17):1702–15. https://doi.org/10.1001/jama.2019.3820.
Gruzieva O, Xu CJ, Yousefi P, et al. Prenatal particulate air pollution and DNA methylation in newborns: an epigenome-wide meta-analysis. Environ Health Perspect. 2019;127(5):57012. https://doi.org/10.1289/EHP4522.
Haworth S, Shapland CY, Hayward C, et al. Low-frequency variation in TP53 has large effects on head circumference and intracranial volume. Nat Commun. 2019;10(1):357. https://doi.org/10.1038/s41467-018-07863-x.
Horikoshi M, Beaumont RN, Day FR, et al. Genome-wide associations for birth weight and correlations with adult disease. Nature. 2016;538(7624):248–52. https://doi.org/10.1038/nature19806.
Kupers LK, Monnereau C, Sharp GC, et al. Meta-analysis of epigenome-wide association studies in neonates reveals widespread differential DNA methylation associated with birthweight. Nat Commun. 2019;10(1):1893. https://doi.org/10.1038/s41467-019-09671-3.
Leventakou V, Roumeliotaki T, Martinez D, et al. Fish intake during pregnancy, fetal growth, and gestational length in 19 European birth cohort studies. Am J Clin Nutr. 2014;99(3):506–16. https://doi.org/10.3945/ajcn.113.067421.
Patro Golab B, Santos S, Voerman E, et al. Influence of maternal obesity on the association between common pregnancy complications and risk of childhood obesity: an individual participant data meta-analysis. Lancet Child Adolesc Health. 2018;2(11):812–21. https://doi.org/10.1016/S2352-4642(18)30273-6.
Santos S, Eekhout I, Voerman E, et al. Gestational weight gain charts for different body mass index groups for women in Europe, North America, and Oceania. BMC Med. 2018;16(1):201. https://doi.org/10.1186/s12916-018-1189-1.
Santos S, Voerman E, Amiano P, et al. Impact of maternal body mass index and gestational weight gain on pregnancy complications: an individual participant data meta-analysis of European, North American and Australian cohorts. BJOG. 2019;126(8):984–95. https://doi.org/10.1111/1471-0528.15661.
Sharp GC, Salas LA, Monnereau C, et al. Maternal BMI at the start of pregnancy and offspring epigenome-wide DNA methylation: findings from the pregnancy and childhood epigenetics (PACE) consortium. Hum Mol Genet. 2017;26(20):4067–85. https://doi.org/10.1093/hmg/ddx290.
Sonnenschein-van der Voort AM, Arends LR, de Jongste JC, et al. Preterm birth, infant weight gain, and childhood asthma risk: a meta-analysis of 147,000 European children. J Allergy Clin Immunol. 2014;133(5):1317–29. https://doi.org/10.1016/j.jaci.2013.12.1082.
Strandberg-Larsen K, Poulsen G, Bech BH, et al. Association of light-to-moderate alcohol drinking in pregnancy with preterm birth and birth weight: elucidating bias by pooling data from nine European cohorts. Eur J Epidemiol. 2017;32(9):751–64. https://doi.org/10.1007/s10654-017-0323-2.
Stratakis N, Roumeliotaki T, Oken E, et al. Fish intake in pregnancy and child growth: a pooled analysis of 15 European and US Birth Cohorts. JAMA Pediatr. 2016;170(4):381–90. https://doi.org/10.1001/jamapediatrics.2015.4430.
Voerman E, Santos S, Patro Golab B, et al. Maternal body mass index, gestational weight gain, and the risk of overweight and obesity across childhood: an individual participant data meta-analysis. PLoS Med. 2019;16(2): https://doi.org/10.1371/journal.pmed.1002744.
Warrington NM, Beaumont RN, Horikoshi M, et al. Maternal and fetal genetic effects on birth weight and their relevance to cardio-metabolic risk factors. Nat Genet. 2019;51(5):804–14. https://doi.org/10.1038/s41588-019-0403-1.
Jaddoe VWV, Felix JF, Andersen AN, et al. The LifeCycle Project-EU Child Cohort Network: a federated analysis infrastructure and harmonized data of more than 250,000 children and parents. Eur J Epidemiol. 2020;35(7):709–24. https://doi.org/10.1007/s10654-020-00662-z.
Wilkinson MD, Dumontier M, Aalbersberg IJ, et al. The FAIR guiding principles for scientific data management and stewardship. Sci Data. 2016;3: https://doi.org/10.1038/sdata.2016.18.
Boyd A, Golding J, Macleod J, et al. Cohort profile: the ‘children of the 90 s’—the index offspring of the avon longitudinal study of parents and children. Int J Epidemiol. 2013;42(1):111–27. https://doi.org/10.1093/ije/dys064.
Fraser A, Macdonald-Wallis C, Tilling K, et al. Cohort profile: the avon longitudinal study of parents and children—ALSPAC mothers cohort. Int J Epidemiol. 2013;42(1):97–110. https://doi.org/10.1093/ije/dys066.
Wright J, Small N, Raynor P, et al. Cohort profile: the Born in Bradford multi-ethnic family cohort study. Int J Epidemiol. 2013;42(4):978–91. https://doi.org/10.1093/ije/dys112.
Koletzko B, von Kries R, Closa R, et al. Lower protein in infant formula is associated with lower weight up to age 2 y: a randomized clinical trial. Am J Clin Nutr. 2009;89(6):1836–45. https://doi.org/10.3945/ajcn.2008.27091.
Olsen J, Melbye M, Olsen SF, et al. The Danish National Birth Cohort—its background, structure and aim. Scand J Public Health. 2001;29(4):300–7. https://doi.org/10.1177/14034948010290040201.
L’Abee C, Sauer PJ, Damen M, Rake JP, Cats H, Stolk RP. Cohort profile: the GECKO Drenthe study, overweight programming during early childhood. Int J Epidemiol. 2008;37(3):486–9. https://doi.org/10.1093/ije/dym218.
Chatzi L, Plana E, Daraki V, et al. Metabolic syndrome in early pregnancy and risk of preterm birth. Am J Epidemiol. 2009;170(7):829–36. https://doi.org/10.1093/aje/kwp211.
Eriksson JG, Forsen T, Tuomilehto J, Osmond C, Barker DJ. Early growth and coronary heart disease in later life: longitudinal study. BMJ. 2001;322(7292):949–53. https://doi.org/10.1136/bmj.322.7292.949.
Jaddoe VW, van Duijn CM, Franco OH, et al. The generation R study: design and cohort update 2012. Eur J Epidemiol. 2012;27(9):739–56. https://doi.org/10.1007/s10654-012-9735-1.
Guxens M, Ballester F, Espada M, et al. Cohort profile: the INMA–INfancia y Medio Ambiente–(environment and childhood) project. Int J Epidemiol. 2012;41(4):930–40. https://doi.org/10.1093/ije/dyr054.
Magnus P, Irgens LM, Haug K, et al. Cohort profile: the Norwegian Mother and Child Cohort Study (MoBa). Int J Epidemiol. 2006;35(5):1146–50. https://doi.org/10.1093/ije/dyl170.
Jarvelin MR, Hartikainen-Sorri AL, Rantakallio P. Labour induction policy in hospitals of different levels of specialisation. Br J Obstet Gynaecol. 1993;100(4):310–5. https://doi.org/10.1111/j.1471-0528.1993.tb12971.x.
Jarvelin MR, Sovio U, King V, et al. Early life factors and blood pressure at age 31 years in the 1966 northern Finland birth cohort. Hypertension. 2004;44(6):838–46. https://doi.org/10.1161/01.HYP.0000148304.33869.ee.
Richiardi L, Baussano I, Vizzini L, et al. Feasibility of recruiting a birth cohort through the Internet: the experience of the NINFEA cohort. Eur J Epidemiol. 2007;22(12):831–7. https://doi.org/10.1007/s10654-007-9194-2.
Newnham JP, Evans SF, Michael CA, Stanley FJ, Landau LI. Effects of frequent ultrasound during pregnancy: a randomised controlled trial. Lancet. 1993;342(8876):887–91. https://doi.org/10.1016/0140-6736(93)91944-h.
Inskip HM, Godfrey KM, Robinson SM, et al. Cohort profile: the Southampton Women’s survey. Int J Epidemiol. 2006;35(1):42–8. https://doi.org/10.1093/ije/dyi202.
Magnus P, Birke C, Vejrup K, et al. Cohort profile update: the Norwegian Mother and Child Cohort Study (MoBa). Int J Epidemiol. 2016;45(2):382–8. https://doi.org/10.1093/ije/dyw029.
Heude B, Forhan A, Slama R, et al. Cohort Profile: the EDEN mother-child cohort on the prenatal and early postnatal determinants of child health and development. Int J Epidemiol. 2016;45(2):353–63. https://doi.org/10.1093/ije/dyv151.
Charles MA, Thierry X, Lanoe JL, et al. Cohort Profile: the French national cohort of children (ELFE): birth to 5 years. Int J Epidemiol. 2020;49(2):368-9j. https://doi.org/10.1093/ije/dyz227.
Tollanes MC, Strandberg-Larsen K, Forthun I, et al. Cohort profile: cerebral palsy in the Norwegian and Danish birth cohorts (MOBAND-CP). BMJ Open. 2016;6(9): https://doi.org/10.1136/bmjopen-2016-012777.
International Labour Organization. ISCO International Standard Classification of Occupations. 2004. https://www.ilo.org/public/english/bureau/stat/isco/isco88/index.htm. Accessed May 2018
Schneider S. The International Standard Classification of Education 2011. Comp Soc Res. 2013;30:365–79. https://doi.org/10.1108/S0195-6310(2013)0000030017.
United Nations Educational, Scientific and Cultural Organisation. International Standard Classification of Education ISCED1997.
Kiserud T, Piaggio G, Carroli G, et al. The World Health Organization fetal growth charts: a multinational longitudinal study of ultrasound biometric measurements and estimated fetal weight. PLoS Med. 2017;14(1): https://doi.org/10.1371/journal.pmed.1002220.
Swertz MA, Dijkstra M, Adamusiak T, et al. The MOLGENIS toolkit: rapid prototyping of biosoftware at the push of a button. BMC Bioinform. 2010;11(Suppl 12):S12. https://doi.org/10.1186/1471-2105-11-S12-S12.
Gaye A, Marcon Y, Isaeva J, et al. DataSHIELD: taking the analysis to the data, not the data to the analysis. Int J Epidemiol. 2014;43(6):1929–44. https://doi.org/10.1093/ije/dyu188.
Wilson R, Butters O, Avraam D, Burton PR, et al. DataSHIELD—new directions and dimensions. Data Sci J. 2017;16(21):1–21.
Open Source Software for BioBanks. http://www.obiba.org/.
Chatenoud L, Chiaffarino F, Parazzini F, Benzi G, La Vecchia C. Prevalence of smoking among pregnant women is lower in Italy than England. BMJ. 1999;318(7189):1012. https://doi.org/10.1136/bmj.318.7189.1012.
Hasnain-Wynia R, Baker DW. Obtaining data on patient race, ethnicity, and primary language in health care organizations: current challenges and proposed solutions. Health Serv Res. 2006;41(4 Pt 1):1501–18. https://doi.org/10.1111/j.1475-6773.2006.00552.x.
Fortier I, Doiron D, Burton P, Raina P. Invited commentary: consolidating data harmonization—how to obtain quality and applicability? Am J Epidemiol. 2011;174(3):261–4. https://doi.org/10.1093/aje/kwr194.
The Lancet Diabetes Endocrinol. Spotlight on rare diseases. Lancet Diabetes Endocrinol. 2019;7(2):75. https://doi.org/10.1016/s2213-8587(19)30006-3.
Lin MF, Lucas HC, Shmueli G. Too big to fail: large samples and the p-value problem. Inform Syst Res. 2013;24(4):906–17. https://doi.org/10.1287/isre.2013.0480.
Bengtsson J, Dich N, Rieckmann A, Hulvej Rod N. Cohort profile: the DANish LIFE course (DANLIFE) cohort, a prospective register-based cohort of all children born in Denmark since 1980. BMJ Open. 2019;9(9): https://doi.org/10.1136/bmjopen-2018-027217.
Mortensen LH, Cnattingius S, Gissler M, et al. Sex of the first-born and obstetric complications in the subsequent birth. A study of 2.3 million second births from Denmark, Finland, Norway, and Sweden. Acta Obstet Gynecol Scand. 2020. https://doi.org/10.1111/aogs.13872.
Stewart LA, Tierney JF. To IPD or not to IPD? Advantages and disadvantages of systematic reviews using individual patient data. Eval Health Prof. 2002;25(1):76–97. https://doi.org/10.1177/0163278702025001006.
Stewart LA, Tierney JF, Clarke M, on behalf of the Cochrane Individual Patient Data Meta-analysis Methods Group. Reviews of individual patient data. Higgins JPT, Green S, editors. Chichester: Wiley; 2008.
Funding
The LifeCycle project received funding from the European Union’s Horizon 2020 research and innovation programme (Grant Agreement No. 733206 LifeCycle). All study specific acknowledgements and funding are presented in the supplementary material. This manuscript reflects only the author’s view and the Commission is not responsible for any use that may be made of the information it contains.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
Study-specific ethics approval statements are available in the supplementary material
Consent to participate
Study-specific informed consent statements are available in the supplementary material
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Pinot de Moira, A., Haakma, S., Strandberg-Larsen, K. et al. The EU Child Cohort Network’s core data: establishing a set of findable, accessible, interoperable and re-usable (FAIR) variables. Eur J Epidemiol 36, 565–580 (2021). https://doi.org/10.1007/s10654-021-00733-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10654-021-00733-9