
Abstract
Objective To investigate the relationship between the apolipoprotein E (APOE) gene and the risk of mortality in normal weight, overweight and obese individuals. Methods and Results In a population-based study of 7,983 individuals aged 55 years and older, we compared the risks of all-cause and coronary heart disease (CHD) mortality by APOE genotype, both overall and in subgroups defined by body mass index (BMI). We found significant evidence for interaction between APOE and BMI in relation to total cholesterol (p = 0.04) and HDL cholesterol (p < 0.001). Overall, APOE*2 carriers showed a decreased risk of all-cause mortality. Analyses within BMI strata showed a beneficial effect of APOE*2 only in normal weight persons (adjusted hazard ratio (HR) 0.7[95% CI 0.5–0.9]). APOE*2 was not associated with a lower risk of all-cause mortality in overweight or obese persons. The effect of APOE*2 in normal weight individuals tended to be due to the risk of CHD mortality (adjusted HR 0.5 [95% CI 0.2–1.2]). Conclusion The APOE*2 allele confers a lower risk of all-cause mortality only to normal weight individuals.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Apolipoprotein E is a plasma protein involved in the metabolism of cholesterol. The apolipoprotein E isoforms ε2, ε3 and ε4, determined by the three alleles of the apolipoprotein E gene (APOE*2, APOE*3 and APOE*4), differ in their binding affinity to serum cholesterol and hence in their ability to clear dietary fat from the blood [1]. Accordingly, total serum cholesterol levels differ between APOE genotypes, with APOE*2 carriers having lower total serum cholesterol levels and APOE*4 carriers having higher levels than APOE*3 homozygotes [1–4].
In line with the clear differences in total serum cholesterol levels associated with the APOE genotype, one would expect that APOE*2 carriers have lower risks of cardiovascular morbidity and mortality and APOE*4 carriers have higher risks. Yet, the evidence for this association is inconsistent. A recent meta-analysis showed that APOE*4 was associated with a higher risk of coronary heart disease (CHD), but found no association with APOE*2 [5]. APOE*2 has been associated with a lower risk of mortality [6] and APOE*4 with a higher risk [7–11], but also these relationships were not found by others [12–19].
A possible explanation for these inconsistencies may be found in the role of body weight. Several studies have demonstrated that the relationship between the APOE gene and lipids differs between normal weight, overweight and obese individuals [20–22]. Total serum cholesterol levels were higher among obese than among non-obese APOE*4 carriers [20], and obese APOE*2 carriers had higher serum triglycerides and higher LDL-cholesterol levels than non-obese APOE*2 carriers [20, 21]. While APOE*2 carriers generally have the lowest cholesterol levels, those with high BMI were found to have similar total serum cholesterol levels compared to APOE*3 homozygotes and APOE*4 carriers [20]. These findings suggest that the adverse effects of high body weight may outweigh the beneficial effect of APOE*2 status. If so, a protective effect of APOE*2 on mortality may be largest among normal weight individuals.
Despite this evidence for a moderating effect of body weight on the relation between the APOE gene and total serum cholesterol, no studies so far have performed a stratified analysis on the relationship between the APOE gene and the risk of mortality. The aim of the present study was to investigate the extent to which the relationship between APOE genotypes and the risk of mortality differs between normal weight, overweight and obese individuals. We examined this relationship for both all-cause and CHD mortality.
Methods
Study population and procedures
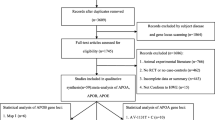
The present analyses were performed in the Rotterdam Study, an ongoing population-based study on the determinants of disease and disability among persons 55 years and older. Details of this study have been described elsewhere [23]. Baseline data were collected between 1990 and 1993. During home visits, a trained investigator obtained information on health status, medical history, medication use and lifestyle. Subsequently, participants were invited to the study center where they underwent an extensive clinical examination. The Medical Ethics Committee of the Erasmus Medical Center approved the study protocol and all participants provided written informed consent. From 10,275 eligible subjects, 7,983 (78%) individuals agreed to participate in the study and were examined at baseline.
Data collection
Clinical and laboratory assessments
The clinical examination included weight, height, systolic and diastolic blood pressure, serum glucose, total serum cholesterol and high-density lipoprotein (HDL) cholesterol levels. BMI was computed as weight (kg) divided by height squared (m2). Participants were classified as underweight (BMI < 18.5 kg/m2), normal weight (18.5 kg/m2 ≤ BMI < 25 kg/m2), overweight (25 kg/m2 ≤ BMI < 30 kg/m2) or obese (BMI ≥ 30 kg/m2) [24]. The waist and hip circumferences were measured, and the waist-hip-ratio (WHR) was calculated as indirect assessment of abdominal fat. Systolic and diastolic blood pressures were measured twice in a sitting position after 5 min rest using a random-zero sphygmomanometer. The mean of the two measurements was used for the analyses. Hypertension was defined as systolic blood pressure higher than 160 mmHg, diastolic blood pressure higher than 100 mmHg, or the use of antihypertensive medication indicated to treat high blood pressure (hypertension grades 2 and 3) [25]. Diabetes was diagnosed based on a random or post-load glucose level higher than 11.0 mmol/l and/or the use of anti-diabetic medication [26]. Total serum cholesterol and HDL-cholesterol were measured using an automated enzymatic procedure [27]. Hypercholesterolemia was defined as a total serum cholesterol level above 6.2 mmol/l [28]. The APOE genotype was determined on DNA samples using a polymerase chain reaction followed by enzymatic digestion using methods previously described [29]. The frequencies of APOE genotypes were APOE 2/2 0.8%, APOE 2/3 12.8%, APOE 2/4 2.7%, APOE 3/3 58.4%, APOE 3/4 22.9% and APOE 4/4 2.4%. The proportions of the APOE alleles and genotypes were in Hardy-Weinberg equilibrium (p = 0.71).
Mortality data
Information on the vital status of the participants was obtained at regular intervals from the municipal population registry. Causes of death were obtained from the general practitioners by means of a standardized questionnaire relating to the circumstances of death, most likely cause of death and time and place of death. Two independent research physicians coded all events according to the International Classification of Diseases, 10th edition (ICD-10) [30]. CHD mortality was defined as death from diseases coded I20–I25, I46, I50 or R96. Mortality data were available up to December 2003.
Statistical analyses
Of the 7,983 individuals who participated at baseline, 5,817 (73%) had APOE genotyped successfully and had complete information on BMI, WHR and cholesterol levels. Because persons with an extremely low BMI may suffer from life-threatening diseases such as cancer, individuals with a BMI below 18.5 kg/m2 (n = 51) were excluded from the analyses. Also, APOE 2/4 individuals were excluded from the analyses (n = 158) to distinguish the effect of the APOE alleles unambiguously. Hence, data from 5,608 participants were available for the analyses.
Differences in baseline characteristics by APOE genotypes were tested using the chi-squared statistic (categorical variables) or ANOVA (continuous variables). P for trend was obtained by testing the linearity of the sum of squares from the ANOVA analyses. Multiple linear regression analysis was used to assess the interaction between APOE genotype and BMI on total serum cholesterol and HDL-cholesterol levels. Differences in survival probabilities were examined by comparing Kaplan-Meier survival curves and tested using the log rank test. Kaplan-Meier plots were constructed using age as the time scale to take proper account of the effect of age [31, 32]. Risks of mortality were quantified as hazard ratios (HRs) using Cox proportional hazards analyses with age as the time scale. The most common genotype (APOE 3/3) was used as the reference category. The proportionality assumption of all models was verified by testing the Schoenfeld residuals [33]. Because the proportionality assumption was not met, HRs were calculated for early and late mortality using 80 years as the cut-off age. This cut-off age was selected because it led to proportionality of the models below and above the cut-off age. HRs were calculated adjusted for gender, smoking status, education level, total serum cholesterol, HDL-cholesterol, waist to hip ratio hypertension and diabetes mellitus.
Results
The mean age at entry was 68.7 years (SD = 8.7 years) and 41.8% of the participants were men. The mean follow up time was 11.1 years (SD = 3.8 years). Baseline characteristics of APOE*2 carriers, APOE*3 homozygotes and APOE*4 carriers are presented in Table 1. As expected, cholesterol levels differed significantly between the genotype groups. The prevalence of hypercholesterolaemia was lowest among APOE*2 carriers (49%) and highest among APOE*4 carriers (66%). Furthermore, there were statistically significant differences in BMI scores between the genotype groups, with APOE*2 carriers having the highest mean BMI (26.7 ± 3.6 kg/m2) and APOE*4 carriers the lowest (26.1 ± 3.4 kg/m2). There were no statistically significant differences in WHR between the genotype groups.
Figure 1 presents mean total serum cholesterol and HDL-cholesterol levels by APOE genotype in normal weight, overweight and obese persons. In all BMI strata, APOE*2 carriers had the lowest and APOE*4 carriers the highest total serum cholesterol (p for trend < 0.01). The association between HDL-cholesterol and APOE genotype was in the opposite direction (p for trend < 0.01). Note that even though APOE*2 carriers had the lowest total serum cholesterol levels in each BMI group, still 50% of the overweight and 57% of the obese APOE*2 carriers had hypercholesterolaemia compared to 41% of the normal weight APOE*2 carriers (p = 0.003). There was no significant evidence for interaction between APOE genotype and BMI in relation to total serum cholesterol (p = 0.26) and HDL-cholesterol (p = 0.25). However, when BMI was analyzed as a continuous trait, then the p value for interaction was 0.04 for total serum cholesterol and less than 0.001 for HDL-cholesterol.

Mean total serum cholesterol and HDL-cholesterol levels by APOE genotypes for normal weight, overweight and obese individuals. HDL: high-density lipoproteins
A total of 1,918 deaths occurred during follow-up. Of those, 257 occurred in 782 APOE*2 carriers (33%), 1,160 in 3,369 APOE*3 homozygotes (33%) and 501 in 1,457 APOE*4 carriers (34%). Differences between the Kaplan-Meier survival curves of the APOE*2 carriers, APOE*3 homozygotes and APOE*4 carriers were small but statistically significant (p = 0.03) with APOE*2 carriers having slightly lower mortality risks (Fig. 2). After adjustment for other cardiovascular risk factors, APOE genotype was not associated with all-cause mortality before or after 80 years of age in the overall population (Table 2). The differences between the curves were only statistically significant in normal weight individuals (p = 0.04; Fig. 3). Normal weight carriers of the APOE*2 allele had a significantly lower risk of mortality before age 80 years (HR [95% CI] = 0.7 [0.5–0.9]), but not after age 80 years (crude HR [95% CI] = 1.0 [0.8–1.4]). There were no significant differences in the risk of mortality between genotype groups among overweight or obese persons (Table 2).

Kaplan Meier survival curves for all-cause mortality by APOE genotypes

Kaplan Meier survival curves for all-cause mortality by APOE genotypes for normal weight, overweight and obese individuals
To investigate whether the lower risk of mortality observed among normal weight APOE*2 carriers was due to a lower risk of mortality from CHD, we calculated the HRs separately for CHD mortality. APOE genotype was not significantly associated with CHD mortality. Analysis within BMI strata showed that normal weight APOE*2 carriers tended to have lower risks of CHD mortality (adjusted HR [95% CI] = 0.5 [0.2–1.2]). No differences in the risk of CHD mortality between genotype groups were found in overweight or obese participants (Table 3).
Discussion
Our study shows that the APOE*2 allele has a protective effect on overall mortality. This protective effect seems to be limited to mortality from CHD. Analyses within BMI strata demonstrated that this genetic advantage of APOE*2 was observed only in normal weight individuals, but not in overweight and obese APOE*2 carriers.
The results of the present analyses may seem to contradict our earlier work in this population. We previously reported that the APOE gene was not significantly related to mortality [12]. While our findings come from the same population, the mean follow-up time of the participants has increased from 5.4 years to 11.1 years and the number of deaths increased by 53% from 18% to 34%. This extended follow-up has improved the statistical power of our study to show a modest effect of APOE genotype on overall mortality. Research on the relationship between APOE and mortality has merely provided conflicting results [6–19, 34]. Three out of eleven studies showed a protective effect of APOE*2 [6, 14, 18]. and three a deleterious effect of APOE*4 [8–10]. The latter effect may partly mediated by the increased risk of Alzheimer disease in association with APOE*4 and mortality [10, 11].
Note that our analysis showed small significant difference in the Kaplan-Meier survival curves, demonstrating a protective effect of APOE*2 before age 80. This may be due to the effect of age that becomes apparent when performing survival analysis with age as time scale, as we did in the present paper. Such finding is compatible with previous reports suggesting that genes affecting human lifespan might be age-specific [35]. Genetic and environmental interactions at older ages vary from those at early ages and therefore explain the differences in the association between APOE and mortality before and after 80 years of age. A previous report showed that among nonagenarians, APOE genotype has no effect on cognitive function, cognitive decline or survival [36].
In line with previous studies [20–22], we found that the total serum cholesterol levels associated with APOE genotype differed between normal weight, overweight and obese individuals. As expected, mean levels of total serum cholesterol increased with BMI and APOE*2 carriers had the lowest mean total serum cholesterol in each BMI group. APOE*4 carriers had higher cholesterol levels and lower HDL-cholesterol concentrations than APOE*2 carriers despite the presence of a lower BMI and equal WHR. Previous reports showed that APOE genotype, BMI and WHR determine together the lipid levels [20–22, 37]. However, in our study abdominal fat, as measured by WHR, did not have any effect on the lipid levels by APOE genotype, while BMI was an important determinant. The significant interaction between APOE genotype and BMI in relation to total serum cholesterol found previously [20], was also supported by this study. Although the mechanism of such interaction has not been yet elucidated, evidence suggests that obesity and abdominal fat increase low density lipoprotein cholesterol and therefore total cholesterol at a higher degree among APOE*4 carriers [20–22, 37]. This is in line with our observation that the deleterious effect of increased BMI prevails over the beneficial effects of the APOE*2 allele. Furthermore, previous research in the Rotterdam Study and the Dutch population indicated that among APOE*2 homozygous carriers, the expression of Hyperlipoproteinemia type III is determined to a great extent by hyperinsulinemia and the presence of insulin resistance syndrome [38], conferring and increased risk of CHD through accelerated atherosclerosis [39].
Although the association between high BMI and high cholesterol levels is well known and the APOE gene is associated with cholesterol levels as previously described, this is the first study that examined the effect of APOE genotype on mortality in BMI strata. We found that presence of the APOE*2 allele was associated with a decreased risk of mortality only in normal weight individuals and that this lower risk was partly explained by lower risk of CHD mortality. These results were in line with the lower total cholesterol and higher HDL levels among normal weight APOE*2 carriers. Our finding that the protective effect of APOE*2 was only found in normal weight individuals suggests that the negative influences of increasing BMI outweigh the positive effects of genetic predisposition. When these results are confirmed by other population-based studies, a challenging question remains whether weight loss in overweight and obese APOE*2 carriers restores the genetic advantage of their APOE status.
References
Eichner JE, Dunn ST, Perveen G, Thompson DM, Stewart KE, Stroehla BC. Apolipoprotein E polymorphism and cardiovascular disease: a HuGE review. Am J Epidemiol 2002;155:487–95.
Horejsi B, Ceska R. Apolipoproteins and atherosclerosis. Apolipoprotein E and apolipoprotein(a) as candidate genes of premature development of atherosclerosis. Physiol Res 2000;49(Suppl 1):S63–9.
Ilveskoski E, Loimaala A, Mercuri MF, Lehtimaki T, Pasanen M, Nenonen A, Oja P, Bond MG, Koivula T, Karhunen PJ, Vuori I. Apolipoprotein E polymorphism and carotid artery intima-media thickness in a random sample of middle-aged men. Atherosclerosis 2000;153:147–53.
Davignon J. Apolipoprotein E and atherosclerosis: beyond lipid effect. Arterioscler Thromb Vasc Biol 2005;25:267–9.
Song Y, Stampfer MJ, Liu S. Meta-analysis: apolipoprotein E genotypes and risk for coronary heart disease. Ann Intern Med 2004;141:137–47.
Lee JH, Tang MX, Schupf N, Stern Y, Jacobs DM, Tycko B, Mayeux R. Mortality and apolipoprotein E in Hispanic, African-American, and Caucasian elders. Am J Med Genet 2001;103:121–7.
Raiha I, Marniemi J, Puukka P, Toikka T, Ehnholm C, Sourander L. Effect of serum lipids, lipoproteins, and apolipoproteins on vascular and nonvascular mortality in the elderly. Arterioscler Thromb Vasc Biol 1997;17:1224–32.
Vogt MT, Cauley JA, Kuller LH. Apolipoprotein E phenotype, arterial disease, and mortality among older women: the study of osteoporotic fractures. Genet Epidemiol 1997;14:147–56.
Stengard JH, Zerba KE, Pekkanen J, Ehnholm C, Nissinen A, Sing CF. Apolipoprotein E polymorphism predicts death from coronary heart disease in a longitudinal study of elderly Finnish men. Circulation 1995;91:265–9.
Tilvis RS, Kahonen-Vare MH, Jolkkonen J, Valvanne J, Pitkala KH, Strandberg TE. Predictors of cognitive decline and mortality of aged people over a 10-year period. J Gerontol A Biol Sci Med Sci 2004;59:268–74.
Hayden KM, Zandi PP, Lyketsos CG, Tschanz JT, Norton MC, Khachaturian AS, Pieper CF, Welsh-Bohmer KA, Breitner JC. Apolipoprotein E genotype and mortality: findings from the Cache County Study. J Am Geriatr Soc 2005;53:935–42.
Slooter AJ, Cruts M, Van Broeckhoven C, Hofman A, van Duijn CM. Apolipoprotein E and longevity: the Rotterdam Study. J Am Geriatr Soc 2001;49:1258–9.
Kuusisto J, Mykkanen L, Kervinen K, Kesaniemi YA, Laakso M. Apolipoprotein E4 phenotype is not an important risk factor for coronary heart disease or stroke in elderly subjects. Arterioscler Thromb Vasc Biol 1995;15:1280–6.
Koivisto AM, Lempiainen P, Koivisto K, Helkala EL, Mykkanen L, Kuusisto J, Kervinen K, Kesaniemi YA, Laakso M, Soininen H. Apolipoprotein E phenotype alone does not influence survival in Alzheimer’s disease: a population-based longitudinal study. Neuroepidemiology 2000;19:327–32.
Heijmans BT, Slagboom PE, Gussekloo J, Droog S, Lagaay AM, Kluft C, Knook DL, Westendorp RG. Association of APOE epsilon2/epsilon3/epsilon4 and promoter gene variants with dementia but not cardiovascular mortality in old age. Am J Med Genet 2002;107:201–8.
Juva K, Verkkoniemi A, Viramo P, Polvikoski T, Kainulainen K, Kontula K, Sulkava R. APOE epsilon4 does not predict mortality, cognitive decline, or dementia in the oldest old. Neurology 2000;54:412–5.
Skoog I, Hesse C, Aevarsson O, Landahl S, Wahlstrom J, Fredman P, Blennow K. A population study of apoE genotype at the age of 85: relation to dementia, cerebrovascular disease, and mortality. J Neurol Neurosurg Psychiatry 1998;64:37–43.
Fillenbaum GG, Burchett BM, Lee JH, Blazer DG. Mortality, apolipoprotein E in African-American, and White elders: an attempted replication. Am J Med Genet 2003;119A:141–6.
Schupf N, Costa R, Luchsinger J, Tang MX, Lee JH, Mayeux R. Relationship between plasma lipids and all-cause mortality in nondemented elderly. J Am Geriatr Soc 2005;53:219–26.
Marques-Vidal P, Bongard V, Ruidavets JB, Fauvel J, Hanaire-Broutin H, Perret B, Ferrieres J. Obesity and alcohol modulate the effect of apolipoprotein E polymorphism on lipids and insulin. Obes Res 2003;11:1200–6.
Srinivasan SR, Ehnholm C, Elkasabany A, Berenson GS. Apolipoprotein E polymorphism modulates the association between obesity and dyslipidemias during young adulthood: the Bogalusa Heart Study. Metabolism 2001;50:696–702.
Boer JM, Ehnholm C, Menzel HJ, Havekes LM, Rosseneu M, O’Reilly DS, Tiret L. Interactions between lifestyle-related factors and the ApoE polymorphism on plasma lipids and apolipoproteins. The EARS Study. European Atherosclerosis Research Study. Arterioscler Thromb Vasc Biol 1997;17:1675–81.
Hofman A, Grobbee DE, de Jong PT, van den Ouweland FA. Determinants of disease and disability in the elderly: the Rotterdam Elderly Study. Eur J Epidemiol 1991;7:403–22.
Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser 2000;894:i–xii, 1–253.
1999 World Health Organization-International Society of Hypertension Guidelines for the Management of Hypertension. Guidelines Subcommittee. J Hypertens 1999;17:151–83.
Report of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care 2003;26 Suppl 1:S5–20.
van Gent CM, van der Voort HA, de Bruyn AM, Klein F. Cholesterol determinations. A comparative study of methods with special reference to enzymatic procedures. Clin Chim Acta 1977;75:243–51.
Executive summary of the third report of the national cholesterol education program (NCEP) Expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III). JAMA 2001;285:2486–97.
Slooter AJ, Houwing-Duistermaat JJ, van Harskamp F, Cruts M, Van Broeckhoven C, Breteler MM, Hofman A, Stijnen T, van Duijn CM. Apolipoprotein E genotype and progression of Alzheimer’s disease: the Rotterdam Study. J Neurol 1999;246(4):304–8.
WHO. International Statistical classification of diseases and related health problems. Geneva: World Health Organization; 1992.
Cheung YB, Gao F, Khoo KS. Age at diagnosis and the choice of survival analysis methods in cancer epidemiology. J Clin Epidemiol 2003;56:38–43.
Korn EL, Graubard BI, Midthune D. Time-to-event analysis of longitudinal follow-up of a survey: choice of the time-scale. Am J Epidemiol 1997;145:72–80.
Schoenfeld D. Partial residuals for the proportional hazards regression model. Biometrika 1982;69:239–41.
Schachter F, Faure-Delanef L, Guenot F, Rouger H, Froguel P, Lesueur-Ginot L, Cohen D. Genetic associations with human longevity at the APOE and ACE loci. Nat Genet 1994;6:29–32.
Christensen K, Johnson TE, Vaupel JW. The quest for genetic determinants of human longevity: challenges and insights. Nat Rev Genet 2006;7:436–48.
Bathum L, Christiansen L, Jeune B, Vaupel J, McGue M, Christensen K. Apolipoprotein E genotypes: relationship to cognitive functioning, cognitive decline, and survival in nonagenarians. J Am Geriatr Soc 2006;54:654–8.
Pouliot MC, Despres JP, Moorjani S, Lupien PJ, Tremblay A, Bouchard C. Apolipoprotein E polymorphism alters the association between body fatness and plasma lipoproteins in women. J Lipid Res 1990;31:1023–9.
de Beer F, Stalenhoef AF, Hoogerbrugge N, Kastelein JJ, Gevers Leuven JA, van Duijn CM, Havekes LM, Smelt AH. Expression of type III hyperlipoproteinemia in apolipoprotein E2 (Arg158 → Cys) homozygotes is associated with hyperinsulinemia. Arterioscler Thromb Vasc Biol 2002;22:294–9.
Mahley RW, Huang Y, Rall SC Jr. Pathogenesis of type III hyperlipoproteinemia (dysbetalipoproteinemia). Questions, quandaries, and paradoxes. J Lipid Res 1999;40:1933–49.
Acknowledgements
The Rotterdam Study is supported by the Erasmus Medical Center and Erasmus University Rotterdam, the Netherlands Organization for Scientific Research (NWO), the Netherlands Organization for Health Research and Development (ZonMw), the Research Institute for Diseases in the Elderly (RIDE), the Ministry of Education, Culture and Science, the Ministry of Health, Welfare and Sports, the European Commission (DGXII), the Municipality of Rotterdam, and the Centre for Medical Systems Biology (CMSB). The contributions of the general practitioners and pharmacists of the Ommoord district to the Rotterdam Study are greatly acknowledged.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Pardo Silva, M.C., Janssens, A.C.J.W., Hofman, A. et al. Apolipoprotein E gene is related to mortality only in normal weight individuals: The Rotterdam study. Eur J Epidemiol 23, 135–142 (2008). https://doi.org/10.1007/s10654-007-9202-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10654-007-9202-6