
Abstract
Purpose
The steady-state pattern electroretinogram (ssPERG) is used to assess retinal ganglion cell function in a variety of research contexts and diagnostic applications. In certain groups of patients or study participants, stable central fixation of the stimulus is not guaranteed. The present study aimed at assessing the effects of misfixation on the ssPERG response to checkerboard reversal stimuli.
Methods
Using two check sizes (0.8° and 15°), we compared ssPERG responses for several amounts of fixation deviation, ranging from 0° to 19° horizontally and from 0° to 14° diagonally. The stimulus area extended to 15° eccentricity, stimulus reversal rate was 15/s.
Results
Up to around 7° eccentricity, there was no sizable effect of fixation deviation under most conditions. Effects were somewhat larger for nasal than for temporal deviation, in particular for small checks. Diagonal deviation was associated with a response to luminance onset/offset at 7.5 Hz (subharmonic of the reversal rate), most prominently when the interior of a large check was fixated.
Conclusion
Generally, moderate inaccuracies of fixation do not have a sizable effect on ssPERG amplitude. However, with large checks, the luminance response has to be considered.
Similar content being viewed by others
Introduction
The pattern electroretinogram (PERG) is used to record ganglion cell responses in a variety of clinical and research contexts [1, 2]. This includes not only testing of macular function [3] and early detection of glaucoma [4, 5], but also assessment of drug effects [6,7,8,9]. In cases of suspected malingering, the combination of a normal PERG and an altered visual evoked potential (VEP) response may provide decisive evidence for an organic disorder [10]. Recently, the PERG has received increased interest as a potential diagnostic biomarker for psychiatric disorders [11,12,13,14,15].
In contrast to the flash ERG, the PERG uses pattern reversal stimuli, which are particularly suitable to target retinal ganglion cells via local contrast inversion without change in mean luminance [16]. With every reversal of the pattern stimulus, local luminance responses on the retina cancel out, and only nonlinear components remain, which constitute the PERG [16]. The steady-state variant (> 10 reversals per second (rps)) of the PERG (ssPERG) is frequently used if the response magnitude, rather than the shape of the response curve, is of primary interest. It allows for efficient recording and relatively simple frequency-space response detection and statistical assessment [17].
In several fields of application, accurate central fixation is not always guaranteed. For instance, patients with central visual field defects may rely on eccentric fixation [18]. Studies in patients with psychiatric disorders (e.g., schizophrenia or depression) showed differences in the ability to maintain proper fixation compared to controls [19,20,21,22], and in cases of malingering, patients may choose to fixate improperly.
Effects of improper fixation have previously been assessed for different types of electrophysiological exams, such as multifocal ERGs [23, 24] and acuity VEPs [25]. For the transient PERG, Persson and Wagner [26] did not find a sizable effect with fixation at 4° eccentricity and check sizes of 24 arcmin.
The present study was designed to quantify the effects of different amounts of deviation from central fixation on the ssPERG in order to provide a basis for judging the relevance of fixation inaccuracies in clinical practice and research applications. We performed two experiments.
In Experiment 1, we assessed purely horizontal misfixation. In this case, as the gaze direction changed along the edge between checks, luminance changes at the time of the checkerboard reversals continued to be balanced, as a switch from black to white above the eccentric fixation point was compensated by a switch from white to black below the fixation point. However, the location of vertical edges in the stimulus changed on the retina and the stimulus pattern as a whole was displaced.
In Experiment 2, fixation was varied along the diagonal. This resulted in the gaze being directed at points that were located in the interior of a check. Thus, when considering the vicinity of the fovea, the reversals of the stimulus resulted in locally unbalanced luminance changes. Due to the eccentricity dependence of retinal circuitry [27], we expected this effect not to be fully balanced across retinal locations, potentially resulting in an undesired luminance response in the ssPERG. The imbalance should be more pronounced for larger checks.
Methods
General methods
ssPERG recording and stimulation procedure
Stimulation and recording was conducted with the EP2000-System [28] following the recommendations of the International Society for Clinical Electrophysiology and Vision (ISCEV) for PERG recordings [1]. ssPERG was recorded from both eyes simultaneously using DTL (Dawson, Trick and Litzkow)-like electrodes [29] placed at the lower limbus of each eye. Reference electrodes were attached to both ipsilateral canthi, with an ear-clip as ground electrode. Signals were amplified (50-fold), filtered with a first order band pass (5–100 Hz) and digitized at 1 kHz with 16 bit resolution.
Participants were placed at a distance of 57 cm from a 17-inch CRT (Cathode Ray Tube)-monitor (800 × 600 pixels, 75 Hz refresh rate). The stimuli (600 × 600 pixels) covered an area of 30° × 30° (i.e., extending to 15° horizontal and vertical eccentricity with central fixation), which corresponds to the “large field PERG” (larger than the regular 15° × 15° (± 3°) field size) as described in the ISCEV recommendations for standard PERG recordings [1].
Black/white checkerboards served as pattern stimuli with a mean luminance of 45 cd/m2 and a Michelson contrast of near 100% with a reversal rate of 15/s, which is suggested in the PERG-standard [1] for glaucoma studies and has been used previously for early detection of glaucoma [30].
In both experiments, two different check sizes (0.8° and 15°) were used in alternating blocks, with each block lasting about 5.3 s and consisting of 5 consecutive sweeps of 1065 ms duration. Each recording run consisted of 8 cycles of the alternating block presentation, resulting in a total of 40 artifact free sweeps per check size for averaging. Due to the large number of eccentric fixation locations in Experiment 1, only one recording run (40 sweeps) per check size and fixation location was performed. In Experiment 2, two recording runs (2 × 40 sweeps) were conducted, and the results averaged for each check size and each fixation target. A threshold of ± 120 µV was applied for automated rejection of artifact-contaminated individual sweeps.
Analysis
Offline analysis was performed with Igor Pro 7 (Wavemetrics Inc.). A discrete Fourier transformation was applied to the sweep average after removal of any linear trend (e.g., originating from baseline drifts) [17]. For display, a 40-Hz low-pass filter was applied to the time-series data. ssPERG amplitudes were extracted from the frequency spectrum at 15 Hz (corresponding to the reversal rate of 15/s of the stimulus) and, in Experiment 2, also at half the reversal rate in seconds to be able to estimate possible luminance responses (at the subharmonic frequency of 7.5 Hz). Amplitudes were subsequently corrected for noise [17] and tested for significance as described by Meigen and Bach [31].
In Experiment 1, data from each eye were considered separately to determine whether there was a difference in effect between inward vergence (nasal fixation deviation) and outward vergence (temporal fixation deviation). In Experiment 2, ssPERG amplitudes were averaged across eyes and recording runs.
To estimate the degree of ssPERG amplitude reduction with increasing distance from the central fixation point, without confounding effects from inter-individual variability, we normalized ssPERG amplitudes for all participants in relation to central fixation by computing the ratio (ssPERG eccentric fixation point / ssPERG central fixation point). Medians were determined and the corresponding 95% confidence intervals (CI) were estimated via bootstrapping (10,000 replicates). In Experiment 1, we expected an amplitude reduction with horizontal fixation deviation but no luminance responses; therefore, we chose one-sided CIs for the analysis. In Experiment 2, two-sided CIs were calculated.
Specific methods of Experiment 1
Participants
Sixteen (four male) neurotypical, healthy participants without known ophthalmological diseases, except for refraction errors, took part in the experiment. The age range was 21–44 years, with a mean age of 29 years (standard deviation: 7 years). For inclusion, a minimum monocular decimal visual acuity of 0.8 had to be achieved in the Freiburg visual Acuity and Contrast Test (FrACT) [32], using refractive correction if necessary.
Fixation deviation
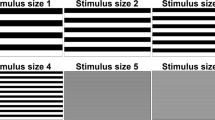
In order to quantify effects from inappropriate fixation during ssPERG recordings, we marked eleven eccentric fixation points on the horizontal axis at 0°, 1°, 2°, 4°, 7.5°, 11°, 13°, 14°, 15°, 16°, 17°, and 19° eccentricity. As exemplarily shown in Fig. 1, the set of fixation marks thus included the border of the stimulus area (15° eccentricity) as well as points outside the stimulus area (16°, 17°, and 19° eccentricity). For each eccentricity, one recording run (40 sweeps) of ssPERG was acquired. Participants were instructed to direct their gaze to the respective fixation mark without turning their head. The sequence of eccentricities was pseudo-randomized across participants, and the direction of eccentricity (left or right) was balanced across participants.

Schematic representation of both checkerboard patterns (0.8° and 15°) and the locations of the different fixation targets (yellow-filled red circles). Experiment 1 (horizontal fixation deviation; left or right): 0°, 1°, 2°, 4°, 7.5°, 11°, 13°, 14°, 15°, 16°, 17°, and 19°. Experiment 2 (diagonal fixation deviation toward the upper right corner): 0°, 1.7°, 2.3°, 7°, 11° and 14°. During central fixation, participants had to announce the random small digits that occasionally appeared in the original fixation mark (central circular disk with a cross inside), eccentric targets were only marked by small dots
Depending on the combination of the direction of fixation deviation (left or right) and the recorded eye (also left or right), the fixation conditions were relabeled as “nasal” or “temporal”, with “nasal” corresponding to inward vergence and “temporal” corresponding to outward vergence. Importantly, by limiting eccentric fixation to horizontal deviations, all fixation targets were located on an edge between checks (except for those targets that were outside the stimulus area). Thus, even with eccentric fixation, there is no relevant overall luminance change when the checkerboard reverses.
Specific methods for Experiment 2
Participants
Twelve (three male) neurotypical, healthy participants without known ophthalmological diseases, except for refractive errors, took part in the experiment. The age range was 22–42 years, with a mean age of 28 years (standard deviation: 6 years). All participants had a monocular decimal visual acuity of ≥ 0.8 (with refraction if necessary) as confirmed with the FrACT.
Fixation deviation
As shown in Fig. 1, fixation targets were presented along the 45°-diagonal toward the upper right. The distances from the center were tested: 0°, 1.7° (center of a 0.8° check), 2.3° (where the corners of four 0.8° checks touch), 7° (\({\raise0.7ex\hbox{$1$} \!\mathord{\left/ {\vphantom {1 3}}\right.\kern-0pt} \!\lower0.7ex\hbox{$3$}}\) of a 15° check), 11° (center of a 15° check), and 14° (\({\raise0.7ex\hbox{$2$} \!\mathord{\left/ {\vphantom {2 3}}\right.\kern-0pt} \!\lower0.7ex\hbox{$3$}}\) of a 15° check).
Results
Experiment 1
ssPERG amplitudes in eccentric fixation conditions remained nearly unaffected (less than 10% decline) up to about 4° departure from central fixation (Fig. 2), independent of the check size presented. At a fixation deviation of 7.5°, the median ssPERG amplitude for the larger checks (15°) was only sightly unattenuated (< 10% reduction), whereas the ssPERG from the smaller check (0.8°) is somewhat more affected (≈ 10% reduction), in particular with nasally deviation. Toward higher eccentricities (> 7.5°), the median of the normalized ssPERG amplitudes declined continuously. Generally, ssPERG amplitudes from the temporal conditions seemed to be affected similarly for both pattern stimuli (0.8° and 15°), whereas responses from the nasal conditions tended to be more affected in case of the small check size (0.8°), compared to the larger check size (15°).

Medians and (median-based) one-sided bootstrapped 95% confidence intervals for the normalized ssPERG amplitudes, which were calculated as ratios relative to the central fixation (0°) for all eccentric fixation points (1°–19°). Data for both check sizes (0.8° and 15°) and both deviation sides (left graph nasal and right graph temporal) are depicted. Fixation points > 15° were located outside the stimulus area
Experiment 2
Up to around 7° diagonal fixation deviation, ssPERG amplitudes at 15 Hz remained relatively stable (< 10% change in amplitude). For the large checks (15°), this continued toward larger deviations (e.g., < 10% decline with 11° fixation deviation) (Fig. 3A), while ssPERGs to the smaller checks (0.8°), seemed to be slightly more affected by increasing fixation deviation (> 7°, e.g., > 10% attenuation with 11° fixation deviation).

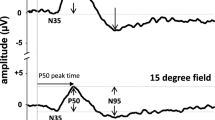
Results from Experiment 2 for diagonal fixation deviation toward the upper right corner (fixation marks: 0°, 1.7°, 2.3°, 7°, 11° and 14°) for both check sizes (0.8° and 15°). a Median and bootstrapped two-sided 95% confidence intervals for normalized ssPERG amplitudes averaged across eyes. b Exemplary ssPERG sweeps for central (0°), 1.7° and 11° fixation points from one individual, showing increased subharmonic responses (additional peaks) at 7.5 Hz with 15° checks, compared to 0.8° checks. c Median and two-sided 95% confidence intervals for ssPERG amplitudes from all participants in µV extracted at 7.5 Hz from the frequency spectrum (subharmonic responses) and averaged across eyes. d Fraction of participants [%] with significant ssPERG responses for both eyes, both recording runs and analyzed frequencies (15 Hz as stimulus reversal rate and 7.5 Hz for possible subharmonic luminance responses)
Although the ssPERG elicited by the larger checks (15°) shows a more “stable” response with increasing fixation deviation showing up at 15 Hz, an inspection of the averaged ssPERG sweeps (Fig. 3b) reveals that larger and smaller response peaks are alternating when the interior of a large check (15° check; 11° deviation) was fixated. This results in a marked subharmonic response component at 7.5 Hz, which was more pronounced for the larger checks (15°) and less prominent for the smaller checks (0.8°) (Figure 3c shows median amplitudes from all participants). The additional subharmonic responses at a frequency of 7.5 Hz were statistically significant in a number of participants (Fig. 3d). For both check sizes, subharmonic response amplitudes were largest when fixation marks fell in the center of a check (Fig. 3c; 0.8° check and 1.7° deviation; 15° check and 11° deviation; compare Fig. 1).
Discussion
The present data show that moderate fixation inaccuracies, in the order of 7 degrees, have a nearly negligible effect on the ssPERG amplitude. In particular, when the check size is large and the gaze does not fall directly in the center of a check, ssPERG amplitudes remain robust, for both tested directions of misfixation. The exact dependence of ssPERG amplitude and fixation eccentricity will obviously depend on the overall extent of the stimulus area, as the position of the outer boundary of the stimulus area can be assumed to be the main determinant of ssPERG amplitude loss. This is consistent with previous findings showing that stimulation at higher eccentricities has a relatively lower contribution to the generation of the PERG [33]. The amount of fixation inaccuracy that is tolerable in a given research context or in diagnostic use will depend on the expected effect sizes. The observed minor ssPERG amplitude alterations (< 10%) with moderate misfixation are comparable with normal PERG amplitude variations due to inter-session (coefficient of variation 6⎼16%) or diurnal (coefficient of variation ≈ 10%) variability [34].
Comparing both directions of horizontal deviation, only minor differential effects were observed on the ssPERG responses from the different eyes and thus from nasal and temporal sides. Two previous studies however reported larger PERG amplitudes with nasal compared to temporal hemifield stimulation [35, 36] and suggested that this might be due to the higher number of nasally distributed retinal ganglion cells in the peripheral retina [37]. In our case, naso-temporal differences were rather small but seemed to be stimulus-specific. With temporal fixation deviation (rightward deviation of the right eye or leftward deviation of the left eye), the ssPERG signal decreases similarly with both check sizes when misfixation increases. With nasal fixation deviation, however, ssPERG responses to the finer checks seemed to be somewhat more affected with increasing fixation deviation, compared to the responses to the larger checks. Considering the complex relationship between PERG responses and the various stimulus parameters, including check size, a definite interpretation of this effect is beyond the present study.
An inequality of the responses to both checkerboard polarities was observed in Experiment 2, particularly if the interior of a large check was fixated. This is most likely a luminance effect that originates at least partly from cell types other than ganglion cells and may need to be considered when interpreting ssPERG findings in terms of ganglion cell function. As the respective frequency of 7.5 Hz was relatively close to the lower cut-off frequency of the bandpass filter of our set-up (5 Hz), the luminance responses were possibly somewhat attenuated.
Using a relatively large stimulus extent, as in the present study (30° × 30°), can be useful when fixation problems are expected (as implicated by Sakaue et al. [38] and Junghardt et al. [39]), if the purpose of the recording does not require a smaller stimulated area. We estimate that the present results would in principle also hold for the standard stimulus extent (15° mean width and height) with the acceptable angle of misfixation scaled correspondingly (e.g., up to around 3° misfixation).
The present study addressed the question of static fixation inaccuracies. Clearly, eye movements might have additional undesired effects on ssPERG signal quality, arising from the electroretinographic response to the moving retinal image [40] and the intrusion of electrooculographic artifacts [41]. However, standard threshold-based artifact detection combined with frequency-domain response analysis should normally ensure that eye movements do not have a sizable effect on the test outcome.
In summary, the present study suggests that moderate fixation inaccuracies do not have a major impact on the outcome of ssPERG recordings.
Data availability
All data collected, analyzed, or generated in this study are available upon request from the corresponding author EF.
References
Bach M, Brigell MG, Hawlina M et al (2013) ISCEV standard for clinical pattern electroretinography (PERG): 2012 update. Doc Ophthalmol 124:1–13. https://doi.org/10.1007/s10633-012-9353-y
Robson AG, Nilsson J, Li S et al (2018) ISCEV guide to visual electrodiagnostic procedures. Doc Ophthalmol 136:1–26. https://doi.org/10.1007/s10633-017-9621-y
Holder GE (2001) Pattern electroretinography (PERG) and an integrated approach to visual pathway diagnosis. Prog Retin Eye Res 20:531–561
Bach M, Hoffmann MB (2008) Update on the pattern electroretinogram in glaucoma. Optom Vis Sci 85:386–395
Ventura LM, Porciatti V (2006) Pattern electroretinogram in glaucoma. Curr Opin Ophthalmol 17:196–202. https://doi.org/10.1097/01.icu.0000193082.44938.3c
Gottlob I, Weghaupt H, Vass C, Auff E (1989) Effect of levodopa on the human pattern electroretinogram and pattern visual evoked potentials. Graefe’s Arch Clin Exp Ophthalmol 227:421–427. https://doi.org/10.1007/BF02172892
Sen A, Tugcu B, Coskun C et al (2014) Effects of levodopa on retina in Parkinson disease. Eur J Ophthalmol 24:114–119. https://doi.org/10.5301/ejo.5000338
Anders L-M, Heinrich SP, Lagrèze WA, Joachimsen L (2019) Little effect of 0.01% atropine eye drops as used in myopia prevention on the pattern electroretinogram. Doc Ophthalmol 138:85–95. https://doi.org/10.1007/s10633-019-09671-0
Rossi GCM, Rolle T, De Silvestri A et al (2022) Multicenter, prospective, randomized, single blind, cross-over study on the effect of a fixed combination of cITICOLINE 500 mg Plus Homotaurine 50 mg on Pattern Electroretinogram (PERG) in patients with open angle glaucoma on well controlled intraocular pressure. Front Med 9:882335. https://doi.org/10.3389/fmed.2022.882335
Röver J, Bach M (1987) Pattern electroretinogram plus visual evoked potential: a decisive test in patients suspected of malingering. Doc Ophthalmol 66:245–251. https://doi.org/10.1007/BF00145238
Bubl E, Kern E, Ebert D et al (2010) Seeing gray when feeling blue? Depression can be measured in the eye of the diseased. Biol Psychiatry 68:205–208. https://doi.org/10.1016/j.biopsych.2010.02.009
Bubl E, Ebert D, Kern E et al (2012) Effect of antidepressive therapy on retinal contrast processing in depressive disorder. Br J Psychiatry 201:151–158. https://doi.org/10.1192/bjp.bp.111.100560
Schwitzer T, Schwan R, Bubl E et al (2017) Looking into the brain through the retinal ganglion cells in psychiatric disorders: a review of evidences. Prog Neuro-Psychopharmacol 76:155–162. https://doi.org/10.1016/j.pnpbp.2017.03.008
Youssef P, Nath S, Chaimowitz GA, Prat SS (2019) Electroretinography in psychiatry: a systematic literature review. Eur psychiatr 62:97–106. https://doi.org/10.1016/j.eurpsy.2019.09.006
Friedel EBN, Tebartz van Elst L, Schmelz C et al (2021) Replication of reduced pattern electroretinogram amplitudes in depression with improved recording parameters. Front Med 8:732222. https://doi.org/10.3389/fmed.2021.732222
Bach M, Hoffmann MB (2006) The origin of the pattern electroretinogram (PERG). In: Heckenlively J, Arden G (eds) Principles and practice of clinical electrophysiology of vision. MIT Press, Cambridge, pp 185–196
Bach M, Meigen T (1999) Do’s and don’ts in Fourier analysis of steady-state potentials. Doc Ophthalmol 99:69–82. https://doi.org/10.1023/A:1002648202420
Crossland MD, Engel SA, Legge GE (2011) The preferred retinal locus in macular disease: toward a consensus definition. Retina 31:2109–2114. https://doi.org/10.1097/IAE.0b013e31820d3fba
Barton JJS, Pandita M, Thakkar K et al (2008) The relation between antisaccade errors, fixation stability and prosaccade errors in schizophrenia. Exp Brain Res 186:273–282. https://doi.org/10.1007/s00221-007-1235-2
Vingolo EM (2014) Eye-fixation behavior in major depressive disorder and the influence of pharmacological therapy: a microperimetric study. Int J Ophthalmol Clin Res 1:1. https://doi.org/10.23937/2378-346X/1410004
Li Y, Xu Y, Xia M et al (2016) Eye movement indices in the study of depressive disorder. Shanghai Arch Psychiatry 28:326–334. https://doi.org/10.11919/j.issn.1002-0829.216078
Liu X, Li Y, Xu L et al (2023) Spatial and temporal abnormalities of spontaneous fixational saccades and their correlates with positive and cognitive symptoms in schizophrenia. Schizophr Bull 50:78–88. https://doi.org/10.1093/schbul/sbad039
Chu PHW, Chan HHL, Leat SJ (2006) Effects of unsteady fixation on multifocal electroretinogram (mfERG). Graefe’s Arch Clin Exp Ophthalmol 244:1273–1282. https://doi.org/10.1007/s00417-006-0304-8
Pedersen KB, Sjølie AK, Vestergaard AH et al (2016) Fixation stability and implication for multifocal electroretinography in patients with neovascular age-related macular degeneration after anti-VEGF treatment. Graefe’s Arch Clin Exp Ophthalmol 254:1897–1908. https://doi.org/10.1007/s00417-016-3323-0
Elgohary AA, Heinrich SP (2021) Minor effect of inaccurate fixation on VEP-based acuity estimates. Doc Ophthalmol 142:275–282. https://doi.org/10.1007/s10633-020-09796-7
Persson HE, Wanger P (1982) Pattern-reversal electroretinograms in squint amblyopia, artificial anisometropia and simulated eccentric fixation. Acta Ophthalmol (Copenh) 60:123–132. https://doi.org/10.1111/j.1755-3768.1982.tb05788.x
Joselevitch C (2008) Human retinal circuitry and physiology. Psychol Neurosci 1:141–165. https://doi.org/10.3922/j.psns.2008.2.008
Bach M (2007) Freiburg evoked potentials. http://www.michaelbach.de/ep2000.html. Accessed 19 Aug 2013
Dawson WW, Trick GL, Litzkow CA (1979) Improved electrode for electroretinography. Invest Ophthalmol Vis Sci 18:988–991
Bach M (2001) Electrophysiological approaches for early detection of glaucoma. Eur J Ophthalmol 11:41–49. https://doi.org/10.1177/112067210101102S05
Meigen T, Bach M (1999) On the statistical significance of electrophysiological steady-state responses. Doc Ophthalmol 98:207–232
Bach M (1996) The Freiburg visual acuity test–automatic measurement of visual acuity. Optom Vis Sci 73:49–53. https://doi.org/10.1097/00006324-199601000-00008
Aylward GW, Billson VFA (1989) The wide-angle pattern electroretinogram: relation between pattern electroretinogram amplitude and stimulus area using large stimuli. Doc Ophthalmol 73:275–283. https://doi.org/10.1007/BF00155096
Otto T, Bach M (1996) Retest variability and diurnal effects in the pattern electroretinogram. Doc Ophthalmol 92:311–323. https://doi.org/10.1007/BF02584085
Porrello G, Falsini B (1999) Retinal ganglion cell dysfunction in humans following post-geniculate lesions: specific spatio–temporal losses revealed by pattern ERG. Vis Res 39:1739–1748. https://doi.org/10.1016/S0042-6989(98)00272-7
Yoshii M, Päärmann A (1989) Hemiretinal stimuli elicit different amplitudes in the pattern electroretinogram. Doc Ophthalmol 72:21–30. https://doi.org/10.1007/BF00155210
Curcio CA, Allen KA (1990) Topography of ganglion cells in human retina. J Comp Neurol 300:5–25. https://doi.org/10.1002/cne.903000103
Sakaue H, Katsumi O, Mehta M, Hirose T (1990) Simultaneous pattern reversal ERG and VER recordings: effect of stimulus field and central scotoma. Invest Ophthalmol Vis Sci 31:506–511
Junghardt A, Wildberger H, Robert Y, Török B (1993) Pattern electroretinogram and visual evoked potential amplitudes are influenced by different stimulus field sizes and scotomata. Doc Ophthalmol 83:139–149. https://doi.org/10.1007/BF01206212
Bach M, Hoffmann MB (2000) Visual motion detection in man is governed by non-retinal mechanisms. Vision Res 40:2379–2385. https://doi.org/10.1016/S0042-6989(00)00106-1
Berninger T, Arden GB (1991) The pattern electroretinogram. In: Heckenlively JR, Arden GB (eds) Principles and practice of clinical electrophysiology of vision. Mosby Year Book, St. Louis, pp 291–300
Acknowledgements
The study was supported by the Deutsche Forschungsgemeinschaft (project# 462923710). Furthermore, we would like to thank Verena Gauggel for her support with data collection. Kathrin Nickel is funded by the Berta-Ottenstein-Program for Advanced Clinician Scientists, Faculty of Medicine, University of Freiburg.
Funding
Open Access funding enabled and organized by Projekt DEAL. This study was supported by the Deutsche Forschungsgemeinschaft (project# 462923710).
Author information
Authors and Affiliations
Contributions
SH and MB elaborated the research question. SH, LTvE, KN and EF conceptualized the study and secured financing. Implementation of the study was accompanied by SH and EF. JH recruited participants and conducted measurements. MB provided stimulation and evaluation software. Data analysis and visualization were conducted by JH and EF with input by SH. SH and EF drafted the manuscript. All authors have read and critically reviewed the manuscript and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
Evelyn B. N. Friedel has no conflict of interest; Julia Haldina has no conflict of interest; Ludger Tebartz van Elst involved in advisory boards, lectures, or travel grants within the last three years: Roche, Eli Lilly, Janssen-Cilag, Novartis, Shire, UCB, GSK, Servier, Janssen and Cyberonics, and Kathrin Nickel have no conflict of interest; Michael Bach has no conflict of interest; Sven P. Heinrich has no conflict of interest.
Ethical approval
The study protocol was approved by the local Ethics Committee of the University of Freiburg (Approval ID: 314/18).
Informed consent
All participants provided written informed consent to participate in the study.
Statement of human rights
All procedures performed in the scope of the study were in agreement with the local ethical standards, as well as in accordance with the tenets of the Declaration of Helsinki.
Statement on the welfare of animal rights
No animal experiments were conducted for the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Friedel, E.B.N., Haldina, J., Nickel, K. et al. Effect of eccentric fixation on the steady-state pattern electroretinogram. Doc Ophthalmol 148, 87–95 (2024). https://doi.org/10.1007/s10633-024-09967-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10633-024-09967-w