
Abstract
Background
Since the coronavirus disease 2019 (COVID-19) pandemic began, telemedicine use has transformed healthcare delivery. Yet there is concern that telemedicine may widen care disparities for vulnerable populations, and patient experience data are limited.
Aims
We aimed to assess patient satisfaction with hepatology-related telemedicine (telehepatology) for delivery of fatty liver disease (FLD) care in a safety-net healthcare system.
Methods
Adult patients with FLD were surveyed regarding satisfaction with telehepatology. Clinical, demographic, resources, and social determinants of health (SDoH) data were collected to identify factors associated with satisfaction through multivariable modeling.
Results
From June 2020 to March 2022, 220 participants were enrolled: the median age was 52 years, 37% were men, and 68% were Hispanic. One hundred nineteen (54%) had prior telehepatology experience. Overall, satisfaction was high; 70% reported being somewhat or very satisfied. On univariate analysis, Hispanic ethnicity (versus non-Hispanic, OR 0.34, 95% CI 0.1–0.9, p = 0.03) and limited access to personal cellphone/internet (OR 0.16, 95% CI 0.04–0.6, p = 0.01) were associated with lower satisfaction. On multivariable logistic regression modeling adjusted for pandemic duration, age, sex, severity of liver disease, and coexisting liver disease, Hispanic ethnicity and lack of personal cellphone/internet remained independently associated with lower telehepatology satisfaction (OR 0.24, 95% CI 0.07–0.9, p = 0.03 and OR 0.2, 95% CI 0.04–0.9, p = 0.04, respectively). The association remained statistically significant after inclusion of various SDoH in the multivariable model.
Conclusions
Satisfaction with telehepatology among FLD patients in a safety-net clinical setting was high overall. However, Hispanic ethnicity and lack of personal cellphone/internet were independently associated with lower telehepatology satisfaction. A better understanding of patients’ experience with telehepatology is needed to identify reasons for dissatisfaction, and in-person visits should remain an option for patients to ensure equitable care.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In the last decade, telemedicine has played a major role in the delivery of care for chronic diseases, including hypertension and diabetes [1, 2]. At the start of the coronavirus disease 2019 (COVID-19) pandemic, specialty care also transitioned to telemedicine to mitigate viral transmission. Advantages include cost effectiveness and increased accessibility to patients with transportation barriers and those living in rural areas [3,4,5]. However, there is increasing concern that telemedicine can widen the “digital divide” for vulnerable populations. In fact, recent studies suggest telemedicine may further exacerbate health inequities for the elderly, minority populations, and patients with limited English proficiency, warranting further research to understand and minimize disparities [6, 7].
Prior to the COVID-19 pandemic, telemedicine in hepatology (telehepatology) was primarily studied in the context of viral hepatitis treatment [8,9,10,11,12]. Use of telehepatology showed promising results with regard to treatment efficacy and patient experience in medically underserved communities, including prisoners and indigenous people [13, 14]. Services quickly expanded to cover other liver conditions during the pandemic, and limited data demonstrated feasibility [15, 16]. However, there has also been a growing interest in understanding factors impacting patient satisfaction with telehepatology. More specifically, early in the pandemic, an evidence-based study on a small population of patients with fatty liver disease (FLD) showed possible racial/ethnic disparities in telehepatology satisfaction [17].
FLD is an umbrella term for both nonalcoholic fatty liver disease and alcohol-associated liver disease. While these two diseases differ, they share an overlapping pathophysiology and often coexist [18]. In the last decade, FLD has become a major cause of liver-related morbidity and mortality [19], disproportionately impacting vulnerable populations. Racial/ethnic disparities in telehepatology satisfaction, partially due to structural and socioeconomic barriers, have been further exacerbated by the circumstances of the COVID-19 pandemic [20,21,22]. Given the increasing burden of FLD, it is important to understand how the transition to telehepatology can impact patient experience. However, few studies have explored telehepatology experience and satisfaction, specifically in vulnerable populations with high proportions of racial/ethnic minorities.
Therefore, the aims of this study were to (1) assess patient experience and satisfaction with telehepatology for FLD during the COVID-19 pandemic and (2) identify clinical, behavioral, and psychosocial factors associated with patient satisfaction.
Methods
Study Participants
From 1 June 2020 to 13 March 2022, 220 adult patients (≥ 18 years old) receiving care for FLD at hepatology clinics in the Zuckerberg San Francisco General Hospital (ZSFGH) safety-net healthcare system were surveyed regarding telehepatology experience. ZSFGH provides culturally competent care to a diverse community of patients in over 20 languages, with a focus on vulnerable populations, (e.g., uninsured, living under the poverty level, etc.) [24]. Patients with psychiatric or medical comorbidities preventing participation in the study or those unable to provide consent were excluded.
Only participants with a diagnosis of FLD defined by presence of hepatic steatosis on imaging (N = 116) or liver biopsy (N = 104) were included in this analysis. This study was approved by the Institutional Review Board of the University of California, San Francisco, and ZSFGH.
Data Collection
Baseline patient sociodemographic data were gathered using surveys [25, 26]. Patients completed surveys either by themselves on paper or with the assistance of a trained research team member over the phone. For non-English speakers, all surveys were translated into Spanish, the most prevalent non-English language in our population, and certified medical interpreters assisted with other languages. All participants were provided with $25 compensation. Clinical history and laboratory data were captured through manual electronic health record (EHR) review.
Clinical and Laboratory Data Definitions and Measures
Demographic information consisted of age, sex, race/ethnicity, and social determinants of health (SDoH) including birth country, preferred language, need for an interpreter during visits, education, annual income, employment status, access to a personal cellphone or internet, housing stability, access to healthy food, and financial insecurity (e.g., money for rent and food).
Steatosis was defined as steatosis on ultrasound, magnetic resonance (MR) proton density fat fraction ≥ 6%, or steatosis of > 5% on liver biopsy. Liver disease severity was evaluated by presence of advanced fibrosis and transaminase levels. Advanced fibrosis including cirrhosis was defined by liver contour nodularity on imaging, MR elastography liver stiffness measurement > 4.5 kilopascals, or a histologic fibrosis stage of F3–4. Clinical characteristics including medical conditions associated with FLD (i.e., diabetes, hypertension, hyperlipidemia) and etiology of liver disease were identified through the EHR. Body mass index (BMI) was also collected and race-adjusted: normal < 25 kg/m2 [< 23 kg/m2 if Asian/Pacific Islander (API)], overweight 25–29.9 kg/m2 (23–27.4 kg/m2 if API), and obese ≥ 30 kg/m2 (≥ 27.5 kg/m2 if API) [27]. Coexisting chronic liver disease (CLD) in addition to FLD was included, and was based on documentation of any other CLD in clinical notes or laboratory evidence (e.g., viral hepatitis).
Regarding categorization of race/ethnicity, this study population predominantly consisted of non-White groups, with a large proportion of Hispanic and Asian individuals, N = 149 and N = 41, respectively. As Hispanic ethnicity comprised the largest racial/ethnic group, race/ethnicity was primarily categorized as Hispanic versus non-Hispanic. Additionally, groups were further categorized into Hispanic, Asian. and White/Black/Other. Although non-Hispanic White individuals historically act as the reference group in scientific literature, due to the small number of White individuals in this population (N = 17), and the concern for causing inaccurate or skewed data due to a small reference group, the three least common racial groups—non-Hispanic White, Black or African American, and those self-identified as “Other”—were combined into a single group. The largest racial/ethnic group, Hispanic, was used as the reference, along with a category for Asian individuals.
Survey Instruments
Validated surveys and new survey items that included patient experience and satisfaction with telemedicine were used [17] Additional measures included the National Institute on Alcohol Abuse and Alcoholism (NIAAA) questionnaire, Center for Epidemiological Studies Depression ten question survey (CES-D-10) and the Patient-Reported Outcomes Measurement Information System (PROMIS) Item Bank: Emotional Distress–Anxiety to measure alcohol use, depression, and anxiety, respectively [28,29,30].
Using the NIAAA questionnaire [28], alcohol use was grouped into three categories: none, moderate (≤ 1 drink/day for women, ≤ 2 drinks/day for men), and heavy (> moderate). On the CES-D-10, a score ≥ 10 indicated severe depressive symptoms [30]. To define anxiety, the two-question PROMIS survey was used. Each question was scored between 1 and 4 points. Total scores varied from 2 to 8 points, higher scores were indicative of higher levels of anxiety [29].
A composite score was created to estimate the impact of the COVID-19 pandemic on participants’ resources. This “loss of resources score” combined the results of 11 questions asking about the impact of the pandemic on resources including employment, childcare, healthcare access, insurance, medications, and mental health and addiction treatment services (Supplemental Table 1) [31].
Lastly, we asked about prior telemedicine experience, and our primary outcome was satisfaction with telehepatology quantified using a single-item question (“If you had a telemedicine or telephone appointment for your FLD, how satisfied were you with your experience?”) on a Likert scale from 1 to 5, where 1 is “very dissatisfied” and 5 is “very satisfied.”
Statistical Analysis
Descriptive statistics including median (interquartile range) and frequency (percentage) were performed. The Kruskal–Wallis test and chi-squared or Fisher’s exact test were employed in comparative analyses for continuous and categorical variables, respectively. Patient characteristics were compared by telehepatology experience (prior versus none). The study population for the primary outcome was comprised of individuals with a prior telehepatology visit.
Univariable and Multivariable Logistic Regression Models
The primary outcome was patient satisfaction (scale 1 to 5) with telehepatology services (conducted via telephone or video). The satisfaction score was dichotomized to satisfied (includes somewhat and very satisfied) versus neutral/dissatisfied (neutral, somewhat dissatisfied, very dissatisfied). Predictors of interest were established before survey administration and included demographic characteristics, SDoH (listed above in Data Definitions), alcohol use, depression/anxiety, and clinical parameters.
A subanalysis was done using the loss of resources composite score. We assessed for an association of loss of resources with race/ethnicity, sex, and age based on numerous studies demonstrating racial/ethnic, sex, and age disparities as a result of the COVID-19 pandemic. Loss of resources was also included in our univariate analysis of factors associated with telemedicine satisfaction.
Univariate and multivariable logistic regression modeling were performed to assess the relationship between each predictor and patient satisfaction. The following factors were adjusted for in the multivariable analyses: age, sex, duration of the pandemic (defined as weeks since start of the pandemic, 1 March 2020) at the time of survey completion, presence of advanced fibrosis, and other coexisting CLD. All models were calculated at p < 0.05 (two sided) for statistical significance. STATA statistical software package version 14 was applied to statistical analyses (STATA Corp LP, College Station, TX).
Results
Cohort Characteristics
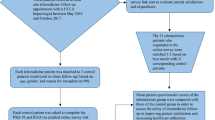
Of the 315 people contacted regarding the study, 253 agreed to participate (80% participation rate) and 33 were excluded from analysis due to the absence of confirmed FLD. A total of 220 participants were included in the study population. Table 1 summarizes participant characteristics. The median age was 52 years, 37% were men, and the majority of participants (68%) self-identified as Hispanic (19% Asian, 14% White/Black/other races) (Table 1). Most participants were born outside the USA (82%) and were non-English speakers, with Spanish being the most common preferred language (58%). Nearly two-thirds of participants completed a high school level education or less and reported an annual income of less than $30,000 per year. Metabolic risk factors were common: 62% obese, 40% with hypertension, 40% with type 2 diabetes, and 45% with hyperlipidemia. While 74% reported minimal or no alcohol use, 20% reported heavy alcohol use. Nearly one-third (31%) had advanced fibrosis.
Comparison by Receipt of Telehepatology
Among the 220 participants, 166 (75%) reported experience with any telemedicine visit, of whom 119 had telehepatology for their FLD. When comparing those with telehepatology experience to those without telehepatology or any telemedicine experience (N = 101), the groups were overall similar with respect to sociodemographic and liver disease characteristics except a greater proportion of participants with telehepatology experience were female compared with those without (69% versus 55%, respectively, p = 0.04) (Table 2). Regarding alcohol use, there was a trend toward less alcohol use among those with telehepatology experience compared with those without, 79% with none/minimal alcohol use compared with 67%, and fewer reported heavy alcohol use, 13% versus 25%, respectively (p = 0.09).
Telehepatology Satisfaction by Age, Sex, Race/Ethnicity, and Liver Disease Severity
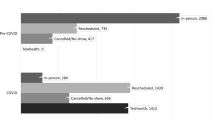
Overall, satisfaction with telehepatology was high, with 62 (52%) participants reporting “very satisfied” and 21 (18%) reporting “somewhat satisfied.” Only 26 (21%) reported being somewhat or very dissatisfied with telehepatology. Figure 1 shows participant satisfaction with telehepatology by sex, age, race/ethnicity, and severity of liver disease. A lower proportion of Hispanic participants were very satisfied with telehepatology compared with Asian and White/Black/other racial/ethnic groups (46% versus 61% versus 71%, respectively) (Fig. 1c). When comparing telehepatology experience versus telemedicine experience in the primary care setting (N = 42), participants reported similar degrees of satisfaction; namely, 30 (71%) reported being somewhat or very satisfied, while 9 (21%) reported being somewhat or very dissatisfied with primary care telemedicine.


Telehepatology satisfaction by A sex, B age, C race/ethnicity, and D liver disease severity. Bar graphs are showing the proportion (%) of participants reporting each level of satisfaction stratified by A sex, B age using less than 65 years versus greater than/equal to 65 years old, C race/ethnicity comparing the predominant racial/ethnic groups, Hispanic versus Asian versus other/White/Black, and D severity of liver disease defined as presence of advanced fibrosis versus absence. Participants rated satisfaction with their telehepatology experience as 1 = very dissatisfied, 2 = somewhat dissatisfied, 3 = neutral, 4 = somewhat satisfied, or 5 = very satisfied
Characteristics of Dissatisfied Participants
We evaluated characteristics of the 26 individuals reporting dissatisfaction with telehepatology. Among this group, the median age was 53 years, the majority (69%) were female, 88% were Hispanic, and the remaining were Asian (12%); most (88%) were born outside the USA, 85% reported a non-English primary language, 73% had an education level at or below high school, and 54% had an annual household income of ≤ $30,000. In addition, nearly a third (27%) had advanced liver fibrosis and 3 (12%) reported heavy alcohol use.
Factors Associated with Telehepatology Satisfaction
On univariable logistic regression analysis with an outcome of satisfied compared with neutral/dissatisfied, Hispanic ethnicity (versus non-Hispanic) was associated with lower odds of telehepatology satisfaction (OR 0.34, 95% CI 0.1–0.9, p = 0.03) (Table 3). Lack of access to a personal cellphone or internet was also associated with lower odds of satisfaction with telehepatology (OR 0.16, 95% CI 0.04–0.6, p = 0.01). In addition to the factors included in Table 3, univariate analysis was also performed using diabetes, hyperlipidemia, hypertension, and BMI, as well as individual racial/ethnic categories. These predictors were not associated with telehepatology satisfaction (data not shown).
After adjusting for factors considered to be potential confounders, specifically pandemic duration, age, sex, severity of liver disease, and other coexisting CLD on multivariable analysis, race/ethnicity (Hispanic versus non-Hispanic) and personal cellphone/internet access were including in the final model based on their univariate p-value of < 0.1. Even after adjusting for other confounders, Hispanic ethnicity (OR 0.24, 95% CI 0.07–0.9, p = 0.03) and lack of personal cellphone/internet access (OR 0.2, 95% CI 0.04–0.9, p = 0.04) remained independently associated with lower odds of satisfaction (Table 3). The goodness-of-fit of this model was assessed using the Hosmer–Lemeshow test, which was not statistically significant, ruling out poor fit.
As differences by race/ethnicity are often related to SDoH (e.g., housing, income, working conditions, and education disparities) [32], we next explored the role of SDoH in the association between ethnicity and satisfaction. With inclusion of each individual SDoH measure (see Methods section) in our final multivariable model, the odds ratio for Hispanic ethnicity remained similar and statistically significant. The only exception was with the inclusion of income, which resulted in a p-value of Hispanic ethnicity increasing to > 0.05. Notably, with the inclusion of income into the model, due to missing data, which was predominantly seen among Hispanic participants (37% income missing versus 19% missing by non-Hispanic participants), there were only N = 82 included in the model. This likely resulted in bias due to missingness as well as overfitting.
We further explored the impact of provider–patient language discordance and use of interpreters on satisfaction with telehepatology. We noted that among Hispanic participants with telehepatology experience, 88% primarily spoke Spanish and 62% reported needing an interpreter for healthcare visits. Moreover, among Hispanic individuals who did not require interpreter services, 60% reported being very or somewhat satisfied with telehepatology compared with 62% satisfied among those who did require interpreter services. Thus, for additional analysis, interaction terms were created, preferred language*ethnicity and interpreter need*ethnicity, which were added into the final multivariable model for telehepatology satisfaction and were not found to be statistically significant (data not shown).
When evaluating potential differences in loss of resources during the pandemic across racial/ethnic groups, we noted Hispanic participants had a higher loss of resources score versus non-Hispanic (median score 2, IQR 1–3 versus median score 1 IQR 1–2, respectively, p = 0.0002) indicating a potential greater impact of the pandemic on this ethnic group’s financial well-being. To determine whether loss of resources may be a confounding variable on the association between Hispanic ethnicity and telehepatology satisfaction, the loss of resources composite score was included in the final model. The odds ratio for the association between Hispanic ethnicity and telehepatology satisfaction remained similar (OR 0.25, 95% CI 0.07–0.9, p = 0.04).
Discussion
The circumstances of the COVID-19 pandemic hindered accessibility to specialty care, particularly for vulnerable populations, and forced the overhaul of healthcare delivery with rapid transition to telemedicine. This introduced a novel set of challenges that disproportionately impacted at-risk individuals [33, 34]. Therefore, it is imperative to understand how these adaptations have affected patient experience and satisfaction, particularly within vulnerable populations to ensure equity in healthcare delivery. In this study, we showed that telehepatology was widely used by patients with FLD receiving care in a safety-net healthcare system in Northern California. While, overall, patients reported a high rate of satisfaction with telehepatology, Hispanic participants and individuals without personal access to a cellphone or internet were less satisfied with their experience.
High satisfaction with telehepatology reported by the majority of participants is consistent with multiple prior studies examining patient satisfaction with telemedicine among gastroenterology and hepatology patients [35,36,37]. These studies generally report patients are satisfied with their experience; some patients even consider telemedicine visits to be equivalent to in-person visits [36]. Among those in hepatology clinics, however, most often the focus has been on the use of telehepatology for viral hepatitis, specifically hepatitis C [10,11,12]. This study adds to the current literature by demonstrating that, for the majority of patients with FLD, specifically being seen in the safety-net setting where patients are often impacted by SDoH, telehepatology satisfaction was also high. While this finding is important and can inform considerations for healthcare delivery for future patient care, it is also critical to further evaluate the experiences of individuals who were not satisfied through qualitative measures.
Previously reported factors associated with decreased use and/or dissatisfaction with telemedicine have included older age, non-English preferred language, and lower socioeconomic status, as well as non-White race/ethnicity, particularly among hepatology patients [33, 34, 38]. However, we did not find an association of older age or preferred language with telehepatology satisfaction among our vulnerable population. On the other hand, we did observe that Hispanic ethnicity and lack of access to cellphone/internet, which is likely a surrogate measure for low socioeconomic status, were associated with telehepatology satisfaction. As disparate healthcare experiences by race/ethnicity are often due to SDoH, we assessed the impact of SDoH variables on this association by incorporating them into our final model. The associations between Hispanic ethnicity and lack of access to personal cellphone/internet with satisfaction remained significant and the odds ratios did not change. This detailed evaluation of SDoH among our study population indicates that differences in satisfaction by ethnicity may be attributed to unmeasured factors such as perceived bias/racism, cultural competency of providers and/or other interpersonal factors, or possibly cultural influences shared by a racial/ethnic group that may impact their interactions with providers and/or healthcare [39]. Moreover, although telehepatology has the potential to overcome geographic barriers and improve care for vulnerable populations with transportation insecurity, in-person visits should remain an option. This is particularly true for individuals without reliable access to technology required to participate in telehepatology.
Racial/ethnic disparities in patient satisfaction with healthcare have previously been reported in non-telemedicine settings where racial/ethnic minority groups report lower satisfaction scores when compared to non-Hispanic White patients [40,41,42]. Potential reported explanations for these differences in satisfaction include financial insecurity and need to delay medical treatment, insurance provider, education, feeling discriminated against, and/or personal experiences [40,41,42]. When focusing on Hispanic patients, while some studies suggest lower satisfaction than non-Hispanic White patients with primary care outpatient services [41], others report higher satisfaction in this population in the emergency department and inpatient setting [43, 44]. This highlights that future research should include qualitative methods to better understand reasons for dissatisfaction with healthcare in various settings and, specifically, the lower satisfaction with telehepatology observed in this study to prevent disparity in telehepatology FLD care.
A strength of this study is the inclusion of a diverse, vulnerable population at risk for experiencing inequitable access to telemedicine who are also disproportionately affected by CLD, particularly FLD [6, 7, 21, 22]. Additionally, this population is often underrepresented in research and an emphasis on their experience is critical to improve care. Another strength is our comprehensive assessment of numerous SDoH, which can be difficult to capture in research. Our study has several limitations. First, the study was conducted at a single, urban location, possibly limiting the generalizability of our results to other settings. However, we prioritized this study population due to the paucity of data on telehepatology use and satisfaction within the safety-net healthcare system. Other limitations include a relatively small sample size, limitations inherent to survey studies such as self-report recall bias, and response bias, as well as the lack of qualitative data, which would have allowed us to better understand unique participant experiences, explore reasons for dissatisfaction, and further evaluate the complex relationship between patient experience and SDoH.
In summary, the expansion of telehepatology in response to the COVID-19 pandemic has the potential to exacerbate already existing health inequities. Reassuringly, in this vulnerable population, most participants were satisfied with their telehepatology visits, suggesting it represents an effective mode of care delivery and should be promoted in safety-net healthcare systems. However, Hispanic ethnicity, an ethnic group disproportionately affected by FLD, was associated with lower satisfaction. While the underlying factors contributing to participant dissatisfaction were not specifically identified, we suspect this relationship is most likely due to unmeasured cultural influences, perceived bias or prejudice, and other factors related to the patient-provider interaction(s) [39]. Going forward, any dissatisfaction with telehepatology in vulnerable populations should be thoroughly explored, particularly when identified among racial/ethnic minority groups, to implement targeted strategies to ensure equitable care delivery. Future qualitative studies are needed to confirm findings in this study.
References
Cottrell E, Cox T, O’Connell P et al. Patient and professional user experiences of simple telehealth for hypertension, medication reminders and smoking cessation: a service evaluation. BMJ Open 2015;5:e007270.
Georgsson M, Staggers N. Quantifying usability: an evaluation of a diabetes mHealth system on effectiveness, efficiency, and satisfaction metrics with associated user characteristics. J Am Med Inform Assoc 2016;23:5–11.
Beard M, Orlando JF, Kumar S. Overcoming the tyranny of distance: an audit of process and outcomes from a pilot telehealth spinal assessment clinic. J Telemed Telecare 2017;23:733–739.
Charlton M, Schlichting J, Chioreso C et al. Challenges of rural cancer care in the United States. Oncology (Williston Park, N.Y.) 2015;29:633–640.
de la Torre-Díez I, López-Coronado M, Vaca C et al. Cost-utility and cost-effectiveness studies of telemedicine, electronic, and mobile health systems in the literature: a systematic review. Telemed J e-Health 2015;21:81–85.
Lam K, Lu AD, Shi Y et al. Assessing telemedicine unreadiness among older adults in the United States during the COVID-19 pandemic. JAMA Intern. Med. 2020;180:1389–1391.
Nouri S, Khoong E, Lyles C et al. Addressing equity in telemedicine for chronic disease management during the Covid-19 pandemic. NEJM Catal Innov Care Deliv. 2020. https://doi.org/10.1056/CAT.20.0123.
Arora S, Geppert CM, Kalishman S et al. Academic health center management of chronic diseases through knowledge networks: project ECHO. Acad Med. 2007;82:154–60.
Arora S, Kalishman S, Thornton K et al. Expanding access to hepatitis C virus treatment—Extension for Community Healthcare Outcomes (ECHO) project: Disruptive innovation in specialty care. Hepatology. 2010;52:1124–33.
Haridy J, Iyngkaran G, Nicoll A et al. eHealth technologies for screening, diagnosis, and management of viral hepatitis: a systematic review. Clin Gastroenterol Hepatol 2021;19:1139–1150.
Talal AH, Andrews P, McLeod A et al. Integrated, co-located, telemedicine-based treatment approaches for hepatitis C virus management in opioid use disorder patients on methadone. Clin Infect Dis 2019;69:323–331.
Sivakumar A, Madden L, DiDomizio E et al. Treatment of Hepatitis C virus among people who inject drugs at a syringe service program during the COVID-19 response: the potential role of telehealth, medications for opioid use disorder and minimal demands on patients. Int J Drug Policy 2022;101:103570.
Keogh K, Clark P, Valery PC et al. Use of telehealth to treat and manage chronic viral hepatitis in regional Queensland. J Telemed Telecare 2016;22:459–464.
Nazareth S, Kontorinis N, Muwanwella N et al. Successful treatment of patients with hepatitis C in rural and remote Western Australia via telehealth. J Telemed Telecare 2013;19:101–106.
Mauro E, Marciano S, Torres MC et al. Telemedicine improves access to hepatology consultation with high patient satisfaction. J Clin Exp Hepatol 2020;10:555–562.
Verma N, Mishra S, Singh S et al. Feasibility, outcomes, and safety of telehepatology services during the COVID-19 pandemic. Hepatol Commun 2022;6:65–76.
Kim RG, Medina SP, Magee C et al. Fatty liver and the coronavirus disease 2019 pandemic: health behaviors, social factors, and telemedicine satisfaction in vulnerable populations. Hepatol Commun 2022;6:1045–1055.
Idalsoaga F, Kulkarni AV, Mousa OY et al. Non-alcoholic fatty liver disease and alcohol-related liver disease: two intertwined entities. Front Med (Lausanne) 2020;7:448.
Paik JM, Golabi P, Biswas R et al. Nonalcoholic fatty liver disease and alcoholic liver disease are major drivers of liver mortality in the United States. Hepatol Commun 2020;4:890–903.
Garcia MA, Homan PA, García C et al. The color of COVID-19: structural racism and the disproportionate impact of the pandemic on older black and Latinx adults. J Gerontol Ser B 2021;76:75–80.
Kim D, Kim W, Adejumo AC et al. Race/ethnicity-based temporal changes in prevalence of NAFLD-related advanced fibrosis in the United States, 2005–2016. Hepatol Int 2019;13:205–213.
Rich NE, Oji S, Mufti AR et al. Racial and ethnic disparities in nonalcoholic fatty liver disease prevalence, severity, and outcomes in the united states: a systematic review and meta-analysis. Clin Gastroenterol Hepatol 2018;16:198–210.
UCSF. SF General and UCSF: partners in public health. Published February 10, 2006. https://www.ucsf.edu/news/2006/02/6572/sf-general-and-ucsf-partners-public-health#:~:text=Social%20Responsibility,families%2C%20immigrants%20and%20the%20elderly. Accessed 2/21/22.
Zuckerberg San Francisco General Hospital and Trauma Center. San Francisco Department of Public Health - More About Us. Accessed August 30, 2023. https://www.sfdph.org/dph/comupg/oservices/medsvs/sfgh/MoreAboutUs.asp.
Surjadi M, Torruellas C, Ayala C et al. Formal patient education improves patient knowledge of hepatitis C in vulnerable populations. Dig Dis Sci 2011;56:213–219.
Wong RJ, Khalili M. A patient-centered hepatitis B virus (HBV) educational intervention improves HBV care among underserved safety-net populations. J Clin Gastroenterol 2020;54:642–647.
Consultation WHOE. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet (London, England) 2004;363:157–163.
National Institute on Alcohol Abuse and Alcoholism. National Institute on Alcohol Abuse and Alcoholism. Alcohol Consumption Questionnaire. https://www.niaaa.nih.gov/research/nesarc-iii/questionnaire. Accessed 2/21/22.
HealthMeasures. PROMIS Banks v1.0 – Anxiety. http://www.healthmeasures.net/index.php?option=com_instruments&view=measure&id=64&I. Accessed 2/21/22.
Zhang W, O’Brien N, Forrest JI et al. Validating a shortened depression scale (10 item CES-D) among HIV-positive people in British Columbia, Canada. PLoS ONE 2012;7:e40793.
D’Souza G, Springer G, Gustafson D et al. COVID-19 symptoms and SARS-CoV-2 infection among people living with HIV in the US: the MACS/WIHS Combined Cohort Study. HIV Res Clin Pract. 2020;21:130–139.
World Health O. Social determinants of health. 2022.
Wahid N, Rosenblatt R. Disparities in telehealth for liver disease: revealing what was hidden in plain sight. Dig Dis Sci. 2022;67:3–5.
Wu T, Simonetto DA, Halamka JD et al. The digital transformation of hepatology: The patient is logged in. Hepatology (Baltimore, Md.) 2022;75:724–739.
Dobrusin A, Hawa F, Gladshteyn M et al. Gastroenterologists and patients report high satisfaction rates with telehealth services during the novel coronavirus 2019 pandemic. Clin Gastroenterol Hepatol 2020;18:2393–2397.
Dobrusin A, Hawa F, Montagano J et al. Patients with gastrointestinal conditions consider telehealth equivalent to in-person care. Gastroenterology 2023;164:156–158.
Serper M, Nunes F, Ahmad N et al. Positive early patient and clinician experience with telemedicine in an academic gastroenterology practice during the COVID-19 pandemic. Gastroenterology 2020;159:1589–1591.
Wegermann K, Wilder JM, Parish A et al. Racial and socioeconomic disparities in utilization of telehealth in patients with liver disease during COVID-19. Dig Dis Sci. 2022;67:93–99.
Baummer-Carr A, Nicolau DP. The challenges of patient satisfaction: influencing factors and the patient—provider relationship in the United States. Expert Rev Anti-infect Ther 2017;15:955–962.
Chung S, Mujal G, Liang L et al. Racial/ethnic differences in reporting versus rating of healthcare experiences. Medicine 2018;97:e13604.
Deshpande SP. The impact of race on patient satisfaction with primary care physicians. Health Care Manag. 2017;36:29–38.
Sorkin DH, Ngo-Metzger Q, De Alba I. Racial/ethnic discrimination in health care: impact on perceived quality of care. J. Gen. Internal Med. 2010;25:390–396.
Figueroa JF, Reimold KE, Zheng J et al. Differences in patient experience between Hispanic and non-Hispanic White patients across U.S. hospitals. J Healthcare Qual. 2018;40:292–300.
Morgan MW, Salzman JG, LeFevere RC et al. Demographic, operational, and healthcare utilization factors associated with emergency department patient satisfaction. West J Emerg Med 2015;16:516–526.
Acknowledgments
This work was in part supported by NIH, R01AA029312 (M.K., D.D.S.), T32DK060414 (R.G.K.), K24AA022523 (M.K.), K24AA025703 (D.D.S.), U24MD017250, UCSF COVID-19 Rapid Response Pilot Grant (M.K., R.G.K.), and Zuckerberg San Francisco General Hospital Foundation Hearts Grant (C.M., M.K.). Mr. Daniel Gonzalez, Mr. Dylan Bush, Mr. Noah Stapper, and Ms. Claudia Ayala assisted with survey administration and data collection.
Author information
Authors and Affiliations
Contributions
RGK (rebecca.g.kim@hsc.utah.edu): designed the study, collected data, performed data analysis, wrote the manuscript, approved final submission. SP (shyam.patel@ucsf.edu): reviewed statistical analysis, wrote the manuscript, approved final submission. DDS (derek.satre@ucsf.edu): contributed to study design, reviewed and edited the manuscript, approved final submission. MS (martha.shumway@ucsf.edu): reviewed statistical analysis, reviewed and edited the manuscript, approved final submission. JYC (jennifer.chen4@ucsf.edu): reviewed and edited the manuscript, approved final submission. CM (catherine.magee@sfdph.org): collected data, reviewed and edited the manuscript, approved final submission. RJW (rwong123@stanford.edu): reviewed and edited the manuscript, approved final submission. AM (alex.monto@ucsf.edu): reviewed and edited the manuscript, approved final submission. RC (rcheung@stanford.edu): reviewed and edited the manuscript, approved final submission. MK (mandana.khalili@ucsf.edu): designed the study, provided material support, reviewed statistical analyses, edited the manuscript, approved final submission.
Corresponding author
Ethics declarations
Conflict of interest
M.K. is a recipient of research grants (to her institution) from Gilead Sciences and Intercept Pharmaceuticals, and she has served as a consultant for Gilead Sciences. J.Y.C received research support from Merck and Pliant Therapeutics. R.J.W. is a recipient of research grants (to his institution) from Gilead Sciences and Exact Sciences, and he has served as consultant for Gilead Sciences and Intercept Pharmaceuticals. R.C received research support from Siemen Healthineers. R.G.K, S.P., D.D.S., M.S., C.M., and A.M. do not have any disclosures relevant to this manuscript.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Kim, R.G., Patel, S., Satre, D.D. et al. Telehepatology Satisfaction Is Associated with Ethnicity: The Real-World Experience of a Vulnerable Population with Fatty Liver Disease. Dig Dis Sci 69, 732–742 (2024). https://doi.org/10.1007/s10620-023-08222-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-023-08222-7