
Abstract
Background
The clinical course of ulcerative colitis (UC) is variable. There is an unmet clinical need for biomarkers of UC disease behaviour. We aimed to evaluate the association between ex vivo human UC explant conditioned media (explant-CM) secreted protein profiles and UC disease behaviour.
Methods
UC patients undergoing endoscopy were prospectively recruited. Endoscopic biopsies were collected and explant-CM generated. Association between explant-CM protein secretion profiles and disease progression was evaluated. Disease progression was defined as the requirement for corticosteroid therapy, UC-related hospitalisation, UC-related surgery or the introduction of a new immunomodulatory agent. Association between explant-CM secreted protein profiles and anti-TNF failure status was also evaluated. p values < 0.05 were considered significant in analyses.
Results
Twenty-four UC patients were included (age [median, range]) 55 [21–72] years; 50% female. Disease progression during follow-up occurred in twelve (50%) patients. Multivariate analysis, including endoscopic remission status, demonstrated reduced IL-2 secretion to be independently associated with UC disease progression, p = 0.01. In univariate analysis, anti-TNF failure status was associated with significantly increased IL-17A/F (p = 0.015) and IL-12 / IL-23p40 (p = 0.044) concentrations. In multivariate analysis, there was a trend towards an association between IL-17A/F and anti-TNF failure status (p = 0.069); FLT-1 was demonstrated to be independently associated with anti-TNF failure status (p = 0.016).
Conclusion
Reduced explant-CM secreted IL-2 is associated with UC disease progression. Increased secretion of IL-23 pathway-associated cytokines was observed in anti-TNF failure status consistent with previous reports. Ex vivo human UC explants, generated from endoscopic biopsies, have potential as precision medicine tools in inflammatory bowel disease.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Ulcerative colitis (UC) is a chronic inflammatory intestinal disorder which involves the colon [1]. UC is characterized by relapsing and remitting mucosal inflammation, starting in the rectum and extending to proximal segments of the colon. The clinical course of UC is variable with a proportion of patients experiencing quiescent disease with sustained remission while others experience progressive chronic refractory disease with risk of hospitalisation and surgery [2]. The risk of colectomy is highest during the first years after diagnosis [3]. Proximal extension of proctitis or left-sided colitis may occur in 20–50% of adult patients with UC [4]. When UC exacerbations are associated with proximal disease extension, patients are more likely to need immunosuppressants, biologic therapy or surgery [5].
The aim of therapy in UC is to induce and maintain clinical and endoscopic remission, resulting in symptom and quality of life improvement and alteration of the natural history of the disease [6]. Patients who achieve early mucosal healing have better long-term outcomes, including longer relapse-free and colectomy-free survival [7]. Extensive and persistent inflammatory UC activity is associated with increased risk of colorectal cancer (CRC) [4]. Identification of patients at risk of UC disease progression is of considerable importance as it would facilitate early therapeutic intervention, with the aim of altering the natural history of the disease and improving long-term outcomes. In addition, identifying individuals at low risk of disease progression facilitates the use of therapeutic strategies appropriate to their disease behaviour with the potential to avoid treatment-related side effects.
Biologic therapy has represented a significant therapeutic advance in UC, and however, approximately one third of patients fail to respond after initiation of these therapies (primary non-response). 30–40% of patients who initially respond to treatment eventually lose response during therapy (secondary loss of response). Patients who have previously failed anti-TNF therapy demonstrate lower response and remission rates to second-line biologic therapy [8]. Considering the inter-individual variability in biologic therapy response in UC, and the increasing number of therapeutic options, a more individualized approach to therapy selection is clearly required. Consequently, there is an unmet need for biomarkers of disease behaviour and therapy response in UC. Patient-derived explants have been demonstrated to have value as a pre-clinical models for anti-cancer drug and biomarker discovery [9]. This model has not been previously evaluated as a tool to predict disease behaviour in inflammatory bowel disease (IBD) patient populations. IBD explants consist of endoscopic intestinal biopsies which are composed of multiple cell populations including intestinal epithelial, endothelial, stromal and constituent immune cells. IBD explants are, therefore, representative of the local intestinal microenvironment in UC and may facilitate biomarker discovery in this disease. The primary aim of this study was to evaluate whether ex vivo human UC explant conditioned media (explant-CM) protein secretion profiles are associated with UC disease behaviour.
Methods
Study Population
A cohort was prospectively recruited at St James’s Hospital, Dublin, following approval of the study by the institution’s research ethics board. Patients with a diagnosis of UC undergoing endoscopic assessment for evaluation of disease activity, treatment response or for surveillance were included. The diagnosis of UC was made using established clinical, endoscopic and histological criteria. Baseline demographics and information on medication exposure at the time of endoscopy were collected for each subject. A Mayo clinical subscore and endoscopic Mayo subscore were documented for each included subject.
Study Endpoint Definitions
The primary study endpoint was the association between explant-CM protein secretion profiles and UC disease progression. UC disease progression was defined as the requirement for UC-related hospitalisation, colectomy, corticosteroids or biologic therapy, at the time of the study endoscopic assessment or at a time subsequent to this assessment. A secondary endpoint assessed was the association between explant-CM protein secretion profiles and anti-TNF failure status. Patients assigned to the anti-TNF failure group were those individuals with a history of anti-TNF therapy failure. Patients assigned to the group with no history of anti-TNF failure were individuals successfully treated with anti-TNF therapy or those with no prior history of anti-TNFα exposure at the time of study endoscopic assessment. Endoscopic remission was defined as an endoscopic Mayo score of 0 or 1 on study endoscopic assessments. An elevated C reactive protein (CRP) was defined as a serum CRP concentration > 5 mg/L at the time of the study endoscopy.
Ex Vivo Ulcerative Colitis Tissue Explant Culture
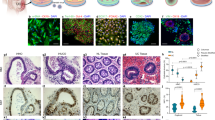
UC patients undergoing sigmoidoscopy or colonoscopy had four study-related endoscopic biopsies collected and two biopsies taken for routine histopathology. These biopsies were collected from the most severely inflamed area in the sigmoid colon approximately 20 cm from the anorectal margin. Endoscopic Mayo score from sigmoid biopsy site was documented. Histopathology reports from the biopsy site were reviewed and the presence of active inflammation was documented. Biopsies were placed in a standard specimen container which contained sterile gauze and saline. The specimen containers were immediately transported to the laboratory for processing following their collection. A single intestinal biopsy was used to generate human ulcerative colitis explants. This biopsy was washed with wash buffer (PBS (Corning, the USA), 1% Pen/Strep (Gibco, Themofisher, the USA), 1% Fungizone (Sigma-Aldrich, the USA), 0.1% Gentamicin (Lonza, Switzerland)) and then cultured in a 24 well plate with media (M199 (Gibco, Themofisher, the USA), 10% FBS (Lonza, Switzerland), 1% Pen/Strep, 1% Fungizone, 0.1% Gentamicin, 1 ug/ml Insulin (Lonza, Switzerland)) and 0.1% DMSO (Sigma-Aldrich, the USA). Biopsies were incubated for 24 h at 37 °C with 95% O2/5% CO2 humidified atmosphere to generate human UC explant-CM. After the incubation period of 24 h, snap-frozen biopsy samples and explant-CM were both stored at − 80 °C to facilitate subsequent analysis. The explant model described in this report has been previously optimised by our group in the study of ex vivo response to chemotherapies in both colorectal and oesophageal cancer, with assays confirming tissue viability for up to 72 h [10] (Fig. 1).

Human ex vivo ulcerative colitis explant model workflow
Determination of Secreted Protein Concentrations in Explant-CM
Explant-CM secreted proteins were quantified using a V-PLEX Human Biomarker 54-plex enzyme-linked immunosorbent assay (ELISA) kit, spread across 7 discrete assays (Meso Scale Diagnostics, the USA). These 7 different assays comprised of the following panels: a TH17 panel, angiogenesis panel, chemokine panel, pro-inflammatory panel, vascular injury panel, cytokine panel 1 and cytokine panel 2. These assays quantified the secretions of the following 54 proteins: CRP, Eotaxin, Eotaxin-3, bFGF, FLT-1, GM-CSF, ICAM-1, IFN-γ, IL-10, IL-12/IL-23p40, IL-12p70, IL-13, IL-15, IL-16, IL-17A, IL-17A/F, IL-17B, IL-17C, IL-17D, IL-1RA, IL-1α, IL-1β, IL-2, IL-21, IL-22, IL-23, IL-27, IL-3, IL-31, IL-4, IL-5, IL-6, IL-7, IL-8, IL-8 (HA), IL-9, IP-10, MCP-1, MCP-4, MDC, MIP-1α, MIP-1β, MIP-3α, PlGF, SAA, TARC, Tie-2, TNF-α, TNF-β, TSLP, VCAM-1, VEGF-A, VEGF-C and VEGF-D. (Supplementary Table 1 provides full protein name corresponding to abbreviations above.) All assays were performed according to manufacturer’s protocol, with an alternative procedure of overnight explant-CM incubation used for all assays except vascular injury and angiogenesis, which were performed using a single-day procedure. Explant-CM was evaluated undiluted for all assays except for vascular injury panel 2, where a one in four dilution was used, as per previous optimisation experiments. All results were reported in pg/ml. All secreted protein concentrations were normalised to total protein content of the biopsy tissue specimen by using a BCA assay (Pierce, the USA) as per manufacturers recommendations.
Extraction and Quantification of Biopsy Protein Levels
Biopsy tissue specimens were added to cryovials with one metal bead and 200ul RIPA+buffer supplemented with EDTA-free protease inhibitor cocktail (Sigma-Aldrich, the USA) and phosphatase inhibitor (Roche, Switzerland). Biopsies were homogenised at 25 Hz for 2 min in a tissue lyser (Qiagen, Germany). Samples were transferred to clean Eppendorf tubes and centrifuged for 20 min at 1800 rcf at 4 °C. 10ul of each sample was added to 96 well plate in triplicates (Thermo Pierce BCA microassay, the USA) with 200ul of working reagent. The plate was incubated for 30 min at 37 °C in humidified CO2 incubator, and absorbance was read at 562 nm to quantify the total protein content of the sample.
Statistical Analysis
Baseline demographic and clinical data were presented as median and interquartile range for continuous variables and frequencies and percentages for categorical variables. Mann–Whitney U test was used to compare continuous variables between groups by endoscopic remission status, disease progression status and anti-TNF failure status. Fisher’s exact test was used to compare frequency data. Relationship between continuous variables was assessed using Pearson’s correlation. Multivariate linear regression was performed to evaluate the association between covariates and study endpoints. Multicollinearity was assessed by generating a variance inflation factor (VIF) for each covariate. Covariates with VIF greater than 5 were removed from multivariate models. Receiver operator curve analysis was performed to determine the classifying ability of secreted proteins for outcomes. p values < 0.05 considered significant in all analyses. This study was considered exploratory; therefore, we did not control for false discovery rate (FDR) in our primary statistical analysis. We performed false discovery rate control as a secondary analysis using the Benjamini–Hochberg procedure with the FDR assigned being 5% [11]. As per standard protocol, the largest p value which was less than the Benjamini–Hochberg critical value was identified. All comparisons with a p value less than or equal to this threshold p value were considered significant following FDR control. Statistical analysis was performed using SPSS (Version 26, IBM).
Results
Baseline Characteristics
Twenty-four patients were recruited age (median [range]) 55 [21–72] years; 50% female; disease duration (median [range]) 9 [1–17] years. The total Mayo score (median [range]) was 2 [0–11]. 67% (n = 16) of patients were in endoscopic remission at the time of study endoscopic assessment. At the time of study endoscopy, 83% (n = 20), 17% (n = 4) and 33% (n = 8) of patients were receiving 5-aminosalicylate (5-ASA), immunomodulator or biologic therapy, respectively. The median [range] duration of follow-up was 7.2 months [0–13.4] (Table 1).
Association Between Clinical Variables and Disease Progression
Disease progression occurred in 12 (50%) patients with a median time to disease progression of 7.5 months [range 0–13.4]. Two patients were defined as having progression at the time of study endoscopy as treatment escalation was required following this evaluation. The absence of endoscopic remission was associated with disease progression. Only 33% (n = 5) of patients achieving endoscopic remission at study endoscopy experienced disease progression, while 88% of patients with an absence of endoscopic remission experienced disease progression (p = 0.027). Patients with an elevated CRP, at the time of study endoscopy, had elevated rates of disease progression, but this did not reach statistical significance (p = 0.1) (Supplementary Fig. 1).
Comparison of Explant Secreted Protein Profiles by Endoscopic Remission Status
Explant-CM protein secretions were compared between patients with and without endoscopic remission at the time of study endoscopy. A number of IBD-associated secreted proteins were significantly elevated in patients with endoscopic activity compared with those in remission: IL-17A, IL-1α, MIP-1α, IP-10, TNF-β, CRP, IL-16, IL-12/23p40, GM-CSF, IL-1β, SAA, IL-17A/F, IL-1RA, ICAM-1, MIP-1β, IL-15, FLT-1, PIGF, IL-17C, TSLP, MIP-3α, bFGF, IL-12p70 and VCAM-1 (Table 2). There was no statistically significant difference seen between patients with endoscopic activity and those with endoscopic remission in the levels of the following IBD-associated cytokines; TNF-α, IL-2, IL-6, IL-7, IL-8, IL-13, IL-21, IL-22 or IFN- γ.
Association Between Explant Secreted Protein Profiles and Disease Progression
The top 10 associations between explant-CM secreted proteins and disease progression are summarised in Table 3. Three secreted cytokines, IL-2, IL-7 and IL-8, were significantly associated with disease progression (Table 3). The concentration of each of these cytokines was lower in patients with disease progression compared to those without disease progression (Fig. 2). The concentrations of IL-2, IL-7 and IL-8 were similar comparing patients with and without endoscopic remission. Secreted IL-2, IL-7 and IL-8 concentration were strongly correlated. The correlation coefficient for IL-2 & IL-7, IL-2 & IL-8, and IL-7 & IL-8 was 0.74 (p = 4.0 × 10–5), 0.67 (p = 3.4 × 10–5) and 0.98 (p = 1.05 × 10–16), respectively. A multivariate regression was performed including IL-2, IL-7, IL-8 and endoscopic remission status. Testing for multicollinearity demonstrated high VIF for IL-7 and IL-8, 36 and 30, respectively; therefore, these covariates were removed from the model. The final multivariate regression model included IL-2 and endoscopic remission status and demonstrated secreted IL-2 to be independently associated with disease progression (standardised beta − 0.44, p = 0.01). Receiver operator curve analysis demonstrated explant-CM secreted IL-2 to perform well as a classifier of UC disease progression AUC: 0.81, 95% CI (0.63–0.98), p = 0.01 (Fig. 3).

Association between disease progression and UC explant secreted IL-2, IL-7 and IL-8 concentrations

Receiver operator curve analysis of classifying performance of explant secreted IL-2 for UC disease progression
Association Between Explant Secreted Cytokine Profiles and Anti-TNF Therapy Failure Status
Twenty-one percent (n = 5) of patients had a history of anti-TNFα failure at the time of study endoscopy (21%). There was a significant difference in the concentration of a number of explant-CM secreted proteins comparing patients with a history of anti-TNF failure to those without a history of anti-TNF failure (Table 4, Supplementary Table 4). The concentration of IL-23 pathway cytokines IL-12/23p40 and IL-17A/F was increased in patients with a history of anti-TNFα failure compared to those without such a history (Table 4). A multivariate analysis was performed which included endoscopic remission status and the five secreted proteins with the strongest association with anti-TNF failure status in univariate analysis (IL-17 A/F, IL-10, SAA, FLT-1 and VEGF). Testing for collinearity demonstrated SSA and VEGF to have high VIFs of 13.2 and 9.9, respectively; therefore, these proteins were removed from the model. In the final multivariate analysis, FLT-1 was independently associated with anti-TNFα failure status (standardised beta 0.53, p = 0.016). There was a non-significant trend towards an independent association between IL17-A/F and anti-TNF failure status (standardised beta 0.36, p = 0.069).
Discussion
In this report, we describe a pilot study utilising human ex vivo UC explants to evaluate the association between explant secreted cytokines profiles and disease behaviour. Patient-derived UC explants have potential advantages over other IBD disease models for biomarker discovery as they have the ability to recapitulate disease biology more precisely and reflect the heterogeneity of UC patient populations more accurately. In this study we demonstrate that the secretion of multiple pro-inflammatory cytokines, previously associated with IBD pathogenesis, is elevated in UC explants from patients with endoscopic activity. We demonstrated that decreased IL-2, IL-7 and IL-8 UC explant secretions are associated with disease progression. In addition, we demonstrated an association between a number of explant secreted proteins, including IL-17 A/F and FLT-1, and anti-TNF failure status.
To validate the human ex vivo UC explant model, we evaluated the differential secretion of proteins comparing explants from patients in endoscopic remission and with endoscopic activity. We demonstrated several explant secreted proteins to be elevated in patients with endoscopic activity compared with patients in endoscopic remission. Explant secreted proteins elevated in this context included IL-1RA, IL-1α, IL-1β, IP-10, IL-12/23p40, IL-12p70, IL-15, IL-16, IL-17A, IL-17A/F, IL-17C, bFGF, MIP-1α, TNF-β, SAA, CRP, GM-CSF, ICAM-1, MIP-1β, PIGF, TSLP, MIP-3α, VCAM-1 and FLT-1. Amongst the listed secreted proteins, many have previously been associated with UC pathophysiology. IL-17 has been shown to be increased in the serum and mucosa of active UC patients. [12] Serum IL-17A and IL-1RA levels have been shown to be increased in patients with active UC compared to those in remission [13, 14]. IL-1RA, IL-1β, IP-10 and GM-CSF have been found to be increased in the intestinal epithelium of UC patients compared to healthy controls [15, 16]. PIGF, FLT-1 and IL-15 protein concentrations are higher in intestinal tissue of active UC patients compared to controls [17, 18]. SAA is an acute-phase reactant shown to have a high correlation with mucosal inflammation in UC [19]. Significant upregulation of these secreted proteins, known to be associated with mucosal inflammation, provides evidence that UC explants recapitulate UC disease biology.
Reduction in UC explant secreted IL-2, IL-7 and IL-8 was associated with disease progression in this study. The concentration of these secreted cytokines did not differ significantly between patients with endoscopic activity and remission suggesting that their association with disease behaviour was independent of endoscopic activity which is a known clinical marker of disease progression risk. In a multivariate analysis, only IL-2 remained significantly associated with disease progression. IL-2 is a pleotropic cytokine known to have immunoregulatory functions and is a key cytokine in intestinal homeostasis. IL-2 levels have been found to be higher in UC patients compared with healthy controls in previous reports [20]. To our knowledge, previous studies have not investigated the variability in IL-2 levels within UC patient populations, nor has the relationship between UC explant IL-2 secretions, endoscopic activity and disease progression previously been evaluated. The finding in our study that UC explant IL-2 secretion was reduced in patients with disease progression compared to those without progression is not necessarily contradictory to previous work that has demonstrated increased IL-2 expression in UC patient samples compared with healthy controls. Cytokine functions in IBD are context dependent and can exert opposing effects depending on disease state and stage of inflammation [21]. It may be that in chronic UC, the immunoregulatory function of IL-2 becomes particularly important and that reduced IL-2 secretion in this context contributes to disease progression. In addition, there is biological plausibility to the finding that reduced intestinal IL-2 production is associated with disease progression. IL-2 is involved in controlling differentiation, survival and function of T regulatory cells (Tregs) which are known to play a critical in the control of intestinal inflammation in murine models [22,23,24]. Loss of function mutations in the IL-2 receptor has been detected in Mendelian forms of IBD [25]. In a pre-clinical mouse model, low dose IL-2 has been shown to expand Tregs and ameliorate experimental colitis in humanised mice [26]. Furthermore, low dose IL-2 is currently being evaluated as a therapy for UC with in a phase 1b/2a clinical trial (NCT02200445). While the finding in our study requires validation, reduced IL-2 secretion in UC explants may have utility as a biomarker of disease progression risk.
While reduced IL-7 and IL-8 secretion in UC explants did not remain significantly associated with disease progression in a multivariate analysis, these cytokines also warrant follow-up in future studies as tissue markers of disease progression in UC. Both IL-7 and IL-8 have potentially immunoregulatory functions which could explain the association we observed between reduced secretion of these cytokines and disease progression. Human intestinal epithelial cells and epithelial goblet cells produce IL-7, and this cytokine is known to be essential for T-cell proliferation. Locally produced IL-7 may serve as a potent regulatory factor for intestinal mucosal lymphocytes [27]. Significantly decreased expression of IL-7 in the inflamed mucosa of the colon in patients with active UC, compared with the colonic mucosa of normal subjects or patients in remission, has previously been described [28]. Another study has shown higher serum IL-7 levels in paediatric patients with CD in remission, compared with patients with active disease [29]. IL-8 has functions in immune cell chemotaxis and angiogenesis promotion. Previous studies have described increased IL-8 in inflamed colonic mucosa of UC patients compared to healthy controls. Further investigation of these cytokines as biomarkers of UC progression is warranted [30, 31].
Thirteen explant secreted proteins exhibited differential secretion in individuals with a history of anti-TNF failure versus those with no history of anti-TNF failure. The IL-23 pathway secreted cytokines IL-17A/F and IL-12/23p40 were elevated in UC explants of patients who had a history of anti-TNF therapy failure. This finding was in concordance with a recent report from Schmitt et al. [32] which demonstrated upregulation of the IL-23 pathway in patients with resistance to anti-TNF therapy. This finding is important as it further validates the findings by Schmitt et al. and has clinical relevance as it suggests that treatment strategies targeting the IL-23 pathway have a strong rationale in IBD patients failing anti-TNF therapy. High baseline serum VEGF levels have been shown to predict poor response to anti-TNF therapy and circulating VEGF levels decrease after successful anti-TNF therapy [33]. The finding of elevated VEGF in patients with a history of anti-TNF failure is therefore not unexpected.
A number of other explant secreted proteins demonstrated a statistically significantly increase in patients with a history of anti-TNF failure, including PIGF, SAA, IL-10, TARC and Eotaxin-3. As mentioned above, increased PIGF and SAA have previously been associated with mucosal inflammation in UC [18, 19]. Eotaxin-3, TARC and IL-10 have been shown to be increased in the colonic tissue of active UC [34, 35]. To our knowledge, none of these proteins have previously been reported to be associated with anti-TNF failure. These secreted proteins warrant further assessment and validation as they may provide further insights into mechanisms of anti-TNF failure in IBD patient populations. Both TREM-1 and OSM have been described as being associated with anti-TNF failure, but we did not investigate these biomarkers in our study.
In a multivariate analysis, FLT-1 was independently associated with anti-TNF failure status. FLT-1 is also known as VEGF receptor 1, and it binds to VEGF-A, VEGF-B and PIGF, playing an important role in cell migration, cell proliferation, angiogenesis and vasculogenesis [36, 37]. A previous study has described increased FLT-1 in colonic mucosa culture supernatant in patients with endoscopic and histological activity [18]. Increased gene expression of FLT-1 and higher FLT-1 protein concentrations have been reported in intestinal tissue of active UC patients compared to controls [38]. FLT-1 has not previously been evaluated as a marker of anti-TNF failure and requires further assessment. Assessment of explant secreted protein profiles segregated by anti-TNF failure status was not a primary focus of this study, and therefore, there are some limitations associated with this analysis. We assessed patients with a history of anti-TNF failure rather than actively recruiting patients failing anti-TNF therapy at the time of endoscopic sampling and the numbers included in the analysis were relatively small. Despite these limitations, we believe that this assessment has clinical relevance as it generates further information on the biology underlying anti-TNF failure and has provided support for biomarkers which have previously been demonstrated to be associated with anti-TNF failure status. Further work is required to follow up the associations observed in this study between explant secreted proteins and anti-TNF failure status.
More generally, our study had a number of limitations. The number of patients included was relatively small compared with traditional biomarker studies in IBD. However, by the standard of prior explant studies in colorectal cancer, our study would be considered to be of a reasonable size and adequately powered [10]. Our study design did not provide for a validation cohort which is generally required to independently confirm the validity of biomarkers in a given disease. Validation of the findings of this report will be a focus of future studies by our group. Explants were generated from one biopsy specimen per patient. Future studies should evaluate inter-individual variability in explant proteins secretions which will be essential to understand if UC explants are to be applied in translational and clinical settings. A significant proportion of explant secreted proteins associated with disease progression and a history of anti-TNF failure status were also associated with endoscopic disease activity in our study. It may therefore be the case that a proportion of explant secreted proteins associated with study endpoints are merely proxies for mucosal inflammation and not independently associated with disease progression or anti-TNF therapy resistance. To control for this potential confounder, a multivariate analysis was performed for each endpoint which included endoscopic remission status. These analyses confirmed a number of explant secreted proteins associations to be independent of endoscopic remission status.
UC is an increasingly important disease with an increasing incidence and prevalence [1]. The range of therapies for this condition has expanded considerably over the last two decades. Biomarkers which accurately predict disease behaviour and identify subpopulations of UC patients likely to respond to specific therapies are required and would significantly advance patient care. The ex vivo human UC explant model has potential to meet these needs allowing the characterisation of UC disease behaviour by profiling the UC explant secretome. Explants provide an alternative to cell-based assays and animal testing and reflect the complexity of the IBD microenvironment. Other studies have validated the use of explants to define degree of mucosal inflammation in IBD and the various effects of biological therapies. [18, 39,40,41,42] Given the inter-individual variability in biologic therapy response in UC and the increasing number of therapeutic options, this platform also has future promise in the ex vivo profiling of therapy response to UC therapeutics aiding in vivo therapy selection for patients. In summary, the human ex vivo human explant model has demonstrated discrete protein secretion profiles are associated with UC disease progression and anti-TNF failure status. While further evaluation and validation are required, the UC explant model holds the potential to act as a precision medicine tool in IBD.
References
Kobayashi T, Siegmund B, Le Berre C, Wei SC, Ferrante M, Shen B et al. Ulcerative colitis. Nat Rev Dis Primers. 2020;6:74.
Broström O. Prognosis in ulcerative colitis. Med Clin North Am. 1990;74:201–218.
Langholz E, Munkholm P, Davidsen M, Binder V. Colorectal cancer risk and mortality in patients with ulcerative colitis. Gastroenterology. 1992;103:1444–1451.
Magro F, Gionchetti P, Eliakim R, Ardizzone S, Armuzzi A, Barreiro-de Acosta M et al. Third European evidence-based consensus on diagnosis and management of ulcerative colitis: part 1: definitions, diagnosis, extra-intestinal manifestations, pregnancy, cancer surveillance, surgery, and ileo-anal pouch disorders. J Crohn’s Colitis. 2017;11:649–670.
Etchevers MJ, Aceituno M, García-Bosch O, Ordás I, Sans M, Ricart E et al. Risk factors and characteristics of extent progression in ulcerative colitis. Inflamm Bowel Dis 2009;15:1320–1325.
Colombel JF, D’Haens G, Lee WJ, Petersson J, Panaccione R. Outcomes and strategies to support a treat-to-target approach in inflammatory bowel disease: a systematic review. J Crohns Colitis. 2020;14:254–266.
Colombel JF, Rutgeerts P, Reinisch W, Esser D, Wang Y, Lang Y et al. Early mucosal healing with infliximab is associated with improved long-term clinical outcomes in ulcerative colitis. Gastroenterology. 2011;141:1194–1201.
Singh S, George J, Boland BS, Vande Casteele N, Sandborn WJ. Primary non-response to tumor necrosis factor antagonists is associated with inferior response to second-line biologics in patients with inflammatory bowel diseases: a systematic review and meta-analysis. J Crohn’s Colitis. 2018;12:635–643.
Powley IR, Patel M, Miles G, Pringle H, Howells L, Thomas A et al. Patient-derived explants (PDEs) as a powerful preclinical platform for anti-cancer drug and biomarker discovery. Br J Cancer. 2020;122:735–744.
Murphy AG, Casey R, Maguire A, Tosetto M, Butler CT, Conroy E et al. Preclinical validation of the small molecule drug quininib as a novel therapeutic for colorectal cancer. Sci Rep. 2016;6:34523.
Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc Ser B 1995;57:289–300.
Fujino S, Andoh A, Bamba S, Ogawa A, Hata K, Araki Y et al. Increased expression of interleukin 17 in inflammatory bowel disease. Gut. 2003;52:65–70.
Krawiec P, Pac-Kożuchowska E. Serum interleukin 17A and interleukin 17F in children with inflammatory bowel disease. Sci Rep 2020;10:12617.
Martinez-Fierro ML, Garza-Veloz I, Rocha-Pizaña MR, Cardenas-Vargas E, Cid-Baez MA, Trejo-Vazquez F et al. Serum cytokine, chemokine, and growth factor profiles and their modulation in inflammatory bowel disease. Medicine. 2019;98:e17208.
Sartor RB. Cytokines in intestinal inflammation: pathophysiological and clinical considerations. Gastroenterology. 1994;106:533–539.
Mayer L, Sandborn WJ, Stepanov Y, Geboes K, Hardi R, Yellin M et al. Anti-IP-10 antibody (BMS-936557) for ulcerative colitis: a phase II randomised study. Gut. 2014;63:442–450.
Liu Z, Geboes K, Colpaert S, D’Haens GR, Rutgeerts P, Ceuppens JL. IL-15 is highly expressed in inflammatory bowel disease and regulates local T cell-dependent cytokine production. J Immunol. 2000;164:3608–3615.
Algaba A, Linares PM, Fernández-Contreras ME, Ordoñez A, Trápaga J, Guerra I et al. Relationship between levels of angiogenic and lymphangiogenic factors and the endoscopic, histological and clinical activity, and acute-phase reactants in patients with inflammatory bowel disease. J Crohn’s Colit. 2013;7:e569–e579.
Wakai M, Hayashi R, Tanaka S, Naito T, Kumada J, Nomura M et al. Serum amyloid A is a better predictive biomarker of mucosal healing than C-reactive protein in ulcerative colitis in clinical remission. BMC Gastroenterology. 2020;20:85.
Brand RM, Moore BA, Zyhowski A, Siegel A, Uttam S, Metter EJ et al. Tofacitinib inhibits inflammatory cytokines from ulcerative colitis and healthy mucosal explants and is associated with pSTAT1/3 reduction in T-cells. Am J Physiol Gastrointest Liver Physiol. 2021;320:G396-g410.
Friedrich M, Pohin M, Powrie F. Cytokine networks in the pathophysiology of inflammatory bowel disease. Immunity. 2019;50:992–1006.
Sadlack B, Merz H, Schorle H, Schimpl A, Feller AC, Horak I. Ulcerative colitis-like disease in mice with a disrupted interleukin-2 gene. Cell. 1993;75:253–261.
Chinen T, Kannan AK, Levine AG, Fan X, Klein U, Zheng Y et al. An essential role for the IL-2 receptor in T(reg) cell function. Nat Immunol. 2016;17:1322–1333.
Klatzmann D, Abbas AK. The promise of low-dose interleukin-2 therapy for autoimmune and inflammatory diseases. Nat Rev Immunol. 2015;15:283–294.
Bouzid D, Amouri A, Fourati H, Marques I, Abida O, Tahri N et al. Polymorphisms in the IL2RA and IL2RB genes in inflammatory bowel disease risk. Genet Test Mol Biomarkers. 2013;17:833–839.
Lee H, Son YS, Lee M-O, Ryu J-W, Park K, Kwon O et al. Low-dose interleukin-2 alleviates dextran sodium sulfate-induced colitis in mice by recovering intestinal integrity and inhibiting AKT-dependent pathways. Theranostics. 2020;10:5048–5063.
Watanabe M, Ueno Y, Yajima T, Iwao Y, Tsuchiya M, Ishikawa H et al. Interleukin 7 is produced by human intestinal epithelial cells and regulates the proliferation of intestinal mucosal lymphocytes. J Clin Invest. 1995;95:2945–2953.
Watanabe M, Watanabe N, Iwao Y, Ogata H, Kanai T, Ueno Y et al. The serum factor from patients with ulcerative colitis that induces T cell proliferation in the mouse thymus is interleukin-7. J Clin Immunol. 1997;17:282–292.
Kader HA, Tchernev VT, Satyaraj E, Lejnine S, Kotler G, Kingsmore SF et al. Protein microarray analysis of disease activity in pediatric inflammatory bowel disease demonstrates elevated serum PLGF, IL-7, TGF-beta1, and IL-12p40 levels in Crohn’s disease and ulcerative colitis patients in remission versus active disease. Am J Gastroenterol. 2005;100:414–423.
Daig R, Andus T, Aschenbrenner E, Falk W, Schölmerich J, Gross V. Increased interleukin 8 expression in the colon mucosa of patients with inflammatory bowel disease. Gut. 1996;38:216–222.
Mitsuyama K, Toyonaga A, Sasaki E, Watanabe K, Tateishi H, Nishiyama T et al. IL-8 as an important chemoattractant for neutrophils in ulcerative colitis and Crohn’s disease. Clin Exp Immunol. 1994;96:432–436.
Schmitt H, Billmeier U, Dieterich W, Rath T, Sonnewald S, Reid S et al. Expansion of IL-23 receptor bearing TNFR2+ T cells is associated with molecular resistance to anti-TNF therapy in Crohn’s disease. Gut. 2019;68:814–828.
Algaba A, Linares PM, Encarnación Fernández-Contreras M, Figuerola A, Calvet X, Guerra I et al. The effects of infliximab or adalimumab on vascular endothelial growth factor and angiopoietin 1 angiogenic factor levels in inflammatory bowel disease: serial observations in 37 patients. Inflamm Bowel Dis. 2014;20:695–702.
Christophi GP, Rong R, Holtzapple PG, Massa PT, Landas SK. Immune markers and differential signaling networks in ulcerative colitis and Crohn’s disease. Inflamm Bowel Dis. 2012;18:2342–2356.
Takahashi K, Imaeda H, Fujimoto T, Ban H, Bamba S, Tsujikawa T et al. Regulation of eotaxin-3/CC chemokine ligand 26 expression by T helper type 2 cytokines in human colonic myofibroblasts. Clin Exp Immunol. 2013;173:323–331.
Fischer C, Mazzone M, Jonckx B, Carmeliet P. FLT1 and its ligands VEGFB and PlGF: drug targets for anti-angiogenic therapy? Nat Rev Cancer. 2008;8:942–956.
Weddell JC, Chen S, Imoukhuede PI. VEGFR1 promotes cell migration and proliferation through PLCγ and PI3K pathways. Syst Biol Appl 2017;4:1.
Frysz-Naglak D, Fryc B, Klimacka-Nawrot E, Mazurek U, Suchecka W, Kajor M et al. Expression, localization and systemic concentration of vascular endothelial growth factor (VEGF) and its receptors in patients with ulcerative colitis. Int Immunopharmacol. 2011;11:220–225.
Meijer MJ, Mieremet-Ooms MA, van Duijn W, van der Zon AM, Hanemaaijer R, Verheijen JH et al. Effect of the anti-tumor necrosis factor-alpha antibody infliximab on the ex vivo mucosal matrix metalloproteinase-proteolytic phenotype in inflammatory bowel disease. Inflamm Bowel Dis. 2007;13:200–210.
Vadstrup K, Galsgaard ED, Gerwien J, Vester-Andersen MK, Pedersen JS, Rasmussen J et al. Validation and optimization of an ex vivo assay of intestinal mucosal biopsies in crohn’s disease: reflects inflammation and drug effects. PLOS ONE. 2016;11:e0155335.
Fina D, Franzè E, Rovedatti L, Corazza GR, Biancone L, Sileri PP et al. Interleukin-25 production is differently regulated by TNF-α and TGF-β1 in the human gut. Mucosal Immunol. 2011;4:239–244.
Petito V, Lopetuso LR, Arena V, Stigliano E, Boninsegna A, Bibbò S et al. Direct effect of infliximab on intestinal mucosa sustains mucosal healing: exploring new mechanisms of action. Dig Liver Dis. 2016;48:391–398.
Acknowledgments
I would like to thank the patients of James’s Hospital who kindly consented to give their samples, without which this research would not be possible.
Funding
Open Access funding provided by the IReL Consortium.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
There are no financial disclosures or conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
10620_2022_7411_MOESM1_ESM.tiff
Supplementary Figure 1. Association between disease progression and endoscopic remission status and serum CRP concentration. (TIFF 858 KB)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Corcoran, R.M., MacDonagh, P., O’Connell, F. et al. Association Between Ex Vivo Human Ulcerative Colitis Explant Protein Secretion Profiles and Disease Behaviour. Dig Dis Sci 67, 5540–5550 (2022). https://doi.org/10.1007/s10620-022-07411-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-022-07411-0