
Abstract
Background
The duration of use of azathioprine (Aza) and 6-mercaptopurine (6-MP) for maintaining remission for Crohn’s disease is debatable.
Aim
To examine whether Aza/6-MP can be safely withdrawn in patients with Crohn’s disease who have been in remission.
Methods
The following databases were searched: MEDLINE (1950–September 2010), EMBASE (1980–September 2010), CINHAL (1981–September 2010), PubMed (1950–September 2010), and the Cochrane Central Register of Controlled Trials (CENTRAL). Randomised controlled and cohort studies comparing azathioprine continuation versus placebo or no treatment were eligible for inclusion. Primary outcomes were relapse rate after discontinuation of Aza/6-MP at 6, 12, and 18 months, and 5 and 10 years.
Results
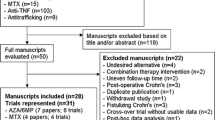
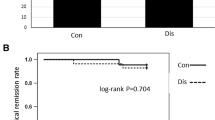
Five studies, with 256 patients and 168 controls, met the inclusion criteria. Stopping azathioprine/6-MP was found to significantly increase the risk of relapse at 6, 12, and 18 months with pooled odds ratios of 0.22 (95% CI 0.09–0.53), 0.25 (95% CI 0.11–0.56), and 0.35 (95% CI 0.21–0.6), respectively. Two trials examined relapse rate at 5 years with pooled OR 0.53 (95% CI 0.13–2.21). No trials looking at relapse rates beyond 5 years were identified.
Conclusions
There is a clear benefit of continuing Aza/6-MP for at least 18 months to maintain remission for Crohn’s disease patients who established remission. There is not enough evidence to provide clear guidance on whether or not to continue Aza/6-MP treatment beyond 18 months. Well-designed randomised controlled trials addressing this issue are needed.


Similar content being viewed by others

References
Shanahan E, Bernstien CN. The evolving epidemiology of inflammatory bowel disease. Curr Opin Gastroenterol. 2009;25:301–305.
Bernstein CN, Fried M, Krabshuis JH, et al. World Gastroenterology organization practice guidelines for the diagnosis and management of IBD in 2010. Inflamm Bowel Dis. 2010;16:112–124.
Prefontaine E, Sutherland LR, MacDonald JK, et al. Azathioprine or 6-mercaptopurine for maintenance of remission in Crohn’s Disease (Review). Cochrane Database of Systematic Reviews. 2009 Art No: CD000067.
Carter MJ, Lobo MJ, Travis SPL. British society of gastroenterology guidelines for the management of inflammatory Bowel disease in adults. Gut. 2003;53:v1–v16.
British National Formulary 60 BMJ Group and Pharmaceutical Press. 2010. http://bnf.org/bnf/bnf/current/. Accessed Sep 17 2010.
Bouknik Y, Lemann M, Mary JY, et al. Long-term follow up of patients with Crohn’s disease treated with azathioprine or 6-mercaptopurine. Lancet. 1996;347:215–219.
Treton X, Bouhnik Y, Mary JY, et al. Azathioprine withdrawal in patients with Crohn’s disease maintained on prolonged remission: A high risk of relapse. Clin Gastroenterol Hepatol. 2009;7:80–85.
Smith MA, Irving PM, Marinaki AM, et al. Review article: malignancy on thiopurine treatment with special reference to inflammatory bowel disease. Aliment Pharmacol Therap. 2010;32:1365–2036.
Korelitz BI, Mirsky FJ, Fleisher MR, et al. Malignant neoplasms subsequent to treatment of inflammatory bowel disease with 6-mercaptopurine. Am J Gastroenterol. 1999;94:3248–3253.
O’Donoghue DP, Dawson AM, Powell-Tuck J, et al. Double-blind withdrawal trial of azathioprine as maintenance treatment for Crohn’s disease. Lancet. 1978;2:955–957.
Nyman M, Hansson I, Eriksson S. Long term immunosuppressive treatment in Crohn’s disease. Scan J Gastroenterol. 1985;20:1197–1203.
Korelitz BI, Adler DI, Mendelsohn RA, et al. Long term experience with 6-Mercaptopurine in the treatment of Crohn’s disease. Am J Gastroenterol. 1993;88:1198–1205.
Higgins JPT, Altman DG. Chapter 8: Assessing risk of bias in included studies. In: Higgins J, Green S editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.0 (updated Feb 2008). The Cochrane Collaboration. 2008.
Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control Clin Trials. 1996;17:1–12.
Higgins JP, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses. Br Med J. 2003;327:557–560.
Daya D. Funnel plots and publication bias—work in progress? Evidence-based Obs Gyn. 2006;8:71–72.
Egger M, Davey Smith G, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. Br Med J. 1997;315:629–634.
Peters JL, Sutton AJ, Jones D, et al. Comparison of two methods to detect publication bias in meta-analysis. J Am Med Ass. 2006;295:676–680.
Kim PS, Zlatanic J, Korelitz BI, et al. Optimum duration of treatment with 6-mercaptopurine for Crohn’s disease. Am J Gastroenterol. 1999;94:3254–3257.
Lemann M, Mary J-Y, Colombel J-F, et al. A randomised, double-blind, controlled withdrawal trial in Crohn’s disease patients in long-term remission on azathioprine. Gastroenterology. 2005;128:1812–1818.
Vilien M, Dahlerup JF, Munck LK, et al. Randomised controlled azathioprine withdrawal after more than two years treatment in Crohn’s disease: Increased relapse rate the following year. Alimen Pharmacol Therap. 2004;19:1147–1152.
Sokol H, Seksik P, Nion-Larmurier I, et al. Current smoking, not duration of remission, delays Crohn’s disease relapse following azathioprine withdrawal. Inflamm Bowel Dis. 2010;16:362–363.
Markowitz J, Rosa J, Grancher K, et al. Long-term 6-mercaptopurine treatment in adolescents with Crohn’s disease. Gastroenterology. 1990;99:1347–1351.
Fraser AG, Orchard TR, Jewell DP, et al. The efficacy of azathioprine for the treatment of inflammatory bowel disease: A 30 years review. Gut. 2002;50:485–489.
McGovern D, Travis S. Thiopurine therapy: When to start and when to stop. Europ J Gastroenterol Hepatol. 2003;15:219–223.
Holtmann M, Krummenaeur F, Claas C, et al. Long-term effectiveness of azathioprine in IBD beyond 4 years: A European multicenter study in 1176 patients. Dig Dis Sci. 2006;51:1516–1524.
Pica R, Avallone EV, Cassieri C, et al. Optimal duration of maintenance treatment with azathioprine in patients with inflammatory bowel disease. Dig Liver Dis. 2010;42S:S61–S192.
Angelucci E, Cesarini M, Gentile P, et al. Azathioprine withdrawal in Crohn’s disease: A never-ending story? Dig Liver Dis. 2010;42S:S61–S192.
Candy S, Wright J, Gerber M, et al. A double-blind controlled study of azathioprine in the treatment and maintenance of remission in Crohn’s disease. Gut. 1995;37:674–678.
Acknowledgments
The authors thank Dr H Sokol and Dr P Seksik for providing supplementary data for “Sokol H, Seksik P, Nion-Larmurier I et al. Current smoking, not duration of remission, delays Crohn’s disease relapse following azathioprine withdrawal. Inflammatory Bowel Disease 2010; 16: 362–363.”
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
French, H., Mark Dalzell, A., Srinivasan, R. et al. Relapse Rate Following Azathioprine Withdrawal in Maintaining Remission for Crohn’s Disease: A Meta-Analysis. Dig Dis Sci 56, 1929–1936 (2011). https://doi.org/10.1007/s10620-011-1671-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-011-1671-5