
Abstract
Objectives We undertook this study to determine if treatment candidacy and outcomes were similar between elderly and non-elderly patients. Methods This was a prospective cohort study that screened 4,025 patients with chronic hepatitis C for HCV antiviral treatment at 24 Veterans Affairs Medical Centers throughout the country. We used multivariable logistic regression to determine whether there was an independent association between being elderly (age > 60 vs. ≤ 60) and (1) being considered a treatment candidate by clinician, and (2) achieving sustained virologic response if treated. Results 364 of the 4,025 patients (9%) were over the age of 60. Only 25% of patients over the age of 60 were considered to be treatment candidates by the evaluating clinician, and only 10% were started on treatment. After adjustment for potential confounders, older age remained associated with a lower likelihood of being considered a treatment candidate (adjusted OR = 0.43; 95% CI: 0.30–0.61). Although based on a small sample of elderly treated patients (n = 35), being elderly did not appear to be associated with a lower likelihood of achieving SVR (adjusted OR = 1.54; 95% CI: 0.46–5.15). Conclusion Among veterans over the age of 60 with chronic hepatitis C who are referred for treatment, relatively few are considered treatment candidates and an even smaller number are ultimately treated. After adjusting for co-morbidities, age remains a strong predictor of not being a treatment candidate. In contrast, older age does not seem to adversely affect treatment outcomes and side effects.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
According to national surveys, approximately 1% of Americans currently over the age of 60 years old have evidence of being infected with hepatitis C virus (HCV) [1]. Although the overall incidence of HCV continues to decrease among young persons, the most prevalent group (4.3%) of infected persons are now in the 40–49 age range and are fast approaching their fifth and sixth decades of life. Little attention, however, has been paid to the management of older patients with chronic hepatitis C and current guidelines do not specifically refer to how age should impact the evaluation and treatment of HCV [2, 3]. Given the slow rate of fibrosis associated with HCV [4, 5], treatment for HCV with interferon/ribavirin may not be indicated for many older adults in whom life expectancy is limited. However, research suggests that the rate of liver fibrosis depends on numerous factors, including duration of infection and age at infection [4–6], so older adults may also be at risk for accelerated complications. Evidence that HCV is increasingly becoming an issue for older adults is seen by the increase in complications from HCV in that age group. The average age for liver transplant has been steadily increasing such that currently at least 20% of liver transplant recipients are older than 60 years of age [7]. Likewise, the incidence of hepatocellular cancer has been increasing steadily, with the peak incidence observed among adults 75–79 years of age [8]. Therefore, for some elderly patients without substantial co-morbidities, chronic HCV may still be an important health issue. This purpose of this study was to determine if being elderly impacts treatment candidacy and outcomes among patients referred to specialty clinics for management of their chronic hepatitis C.
Methods
Study population and design
This prospective cohort study followed patients who were recruited from gastroenterology, hepatology, and infectious disease clinics at 24 Veterans Affairs (VA) Medical Centers throughout the United States between December 1999 and December 2000. Details on study sample and data collection have been described in full previously [9, 10]. Briefly, patients were eligible for this study if they were a US veteran receiving care at one of the participating study sites, were greater than 18 years of age, had a positive HCV antibody test (Ortho HCV ELISA version 3.0; Ortho-Clinical Diagnostics, Inc., Raritan, NJ), and were under consideration for HCV treatment with interferon alpha-2b and ribavirin. Patients were excluded if they had undetectable HCV RNA by polymerase-chain-reaction testing (COBAS Amplicor HCV Monitor Test, Roche Diagnostics, Branchburg, NJ). All persons provided written informed consent to participate, and the study was approved by the local institutional review board at each medical center.
Study variables
The main outcomes of interest were treatment candidacy and treatment outcomes. Treatment candidacy by clinician was determined by asking the treating clinician at each medical center “Based on your judgment, is the patient an interferon and ribavirin treatment candidate?”. Treatment candidacy criteria were based on the VA’s HCV treatment recommendations at the time of the study [11]. These did not specifically include a threshold for withholding treatment based on age. The main treatment outcome of interest was sustained virologic response (SVR), or absence of detectable HCV RNA (<100 copies/ml) measured at six months after HCV antiviral therapy (interferon alpha-2b and ribavirin) completion. Secondary analyses included the evaluation of treatment acceptance, initiation, side effects and discontinuation. Our main predictor of interest was elderly status, which we defined as age greater than 60 years. Additional covariates that were used for the descriptive and multivariate analysis were: sex, race/ethnic group (non-Hispanic white, non-Hispanic black, Hispanic/Latino, and other), education (high school education or less), income (less than $10,000/year), prior history of injection drug use (IDU), current substance abuse, drinking habits (none/<3/3–6/>6 drinks per day), psychiatric disease, HIV status, cardiac disease, medical co-morbidities in general, inability to remain compliant (in the judgement of the clinician), body mass index (BMI), HCV RNA genotype and viral load, ALT level, platelet count, and liver biopsy results.
Statistical analysis
Descriptive analysis of elderly and non-elderly patients was performed, using the chi-square test to compare proportions of categorical variables. Univariate analysis evaluating the proportion of treatment candidacy and outcomes in elderly and non-elderly patients was also conducted using chi-square testing. We used logistic regression in order to assess the effects of being elderly on 1) being considered a treatment candidate by clinician and 2) likelihood of attaining SVR. Odds ratios and 95% confidence intervals were calculated for the adjusted and unadjusted association between being elderly and each outcome. The variables which we chose to adjust for in multivariable models were determined in advance based on an a priori hypothesis that they could act as confounders (both positive and negative), and results from our univariate analysis (i.e., P-value < 0.05). For the logistic model for treatment candidacy, we adjusted for sex, race/ethnicity, education, income, HIV status, abnormal ALT, history of injection drug use, current substance abuse, alcohol use, psychiatric co-morbidities, medical co-morbidities, cardiac disease and non-compliance. For the model with SVR as outcome, we adjusted for sex, race, genotype (1 vs. non-1), high viral load (>1 million copies/ml), BMI and stage of fibrosis. All analyses were conducted using SAS software (SAS Institute, Cary, NC) and a two-tailed P-value of <0.05 was considered significant for all hypothesis testing.
Results
Of the study cohort of 4,025 patients who were referred for hepatitis C treatment, 364 (9%) were older than 60 years of age. Elderly patients with chronic HCV had less education; however, there was no significant difference in income, race/ethnic groups and sex between elderly and non-elderly patients (Table 1). Elderly patients were less likely to have a history of injection drug use, and were less likely to have recently used illicit drugs. They were less likely to drink heavily (>6 drinks a day); however, there was no significant difference in the proportion reporting recent abstinence at baseline, which was low in both groups (14 vs. 16%). Elderly patients with HCV were less likely to have psychiatric co-morbidities, but were more likely to have medical co-morbidities (with the exception of HIV). Elderly patients were less likely to have abnormal ALT, but there was no significant difference in the proportion with low platelet counts. Although only a subset of patients received genotype and viral load testing, there did not appear to be any significant differences between elderly and non-elderly patients: 68 vs. 67% (chi-square P-value = 0.86) were genotype 1, and 48 vs. 60% (chi-square P-value = 0.19) had a high viral load (>1 million copies/ml). Although elderly patients were less likely to have received liver biopsies, the prevalence with advanced liver disease (greater than stage 2 fibrosis) was nearly identical among elderly and non-elderly patients (68.4 vs. 67.4%).
Elderly patients were significantly less likely to be considered a treatment candidate by the evaluating provider, compared to non-elderly patients (25 vs. 42%) (Table 2). Likewise, according to guidelines, elderly patients were also less likely to qualify for treatment (16% vs. 26%). However, like the non-elderly, elderly patients were more often considered treatment candidates by the clinician than guidelines would indicate. Using logistic regression, we observed that elderly patients who were evaluated for their chronic HCV were significantly less likely to be considered a treatment candidate (aOR 0.43; 95% CI: 0.30–0.61), even after adjusting for sex, race, education, income, HIV status, abnormal ALT, substance abuse, alcohol use, psychiatric co-morbidities, medical co-morbidities, cardiac disease and non-compliance (Table 3).
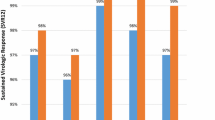
Fewer elderly patients who were considered treatment candidates agreed to be treated compared to non-elderly (63% vs. 77%). Only 10% of elderly patients who were referred for evaluation for treatment for chronic hepatitis C initiated treatment compared to 20% of non-elderly patients. There was no significant difference in the rate of side-effect and early discontinuation of treatment between elderly and non-elderly patients (Table 4): up to a quarter of patients experienced side-effects and approximately a third discontinued treatment early. Using univariate analysis of the patients treated, there was no difference in the rate of EOTR and SVR between elderly and non-elderly patients (34% vs. 29% and 20% vs. 18%, respectively). This was also confirmed by logistic regression, which showed that elderly patients did not appear to be less likely to achieve SVR compared to non-elderly patients (aOR 1.54; 95% CI: 0.46–5.15), even after adjustment for sex, race, HCV genotype, viral load, BMI, and stage of fibrosis (Table 3).
Discussion
In this national prospective study of patients referred for treatment of chronic hepatitis C at VA Medical Centers, we found that nearly 10% of referred patients were elderly (age > 60 years). The elderly patients who were referred did not appear to have indices to suggest more severe liver disease (platelets, ALT levels, fibrosis on liver biopsy). However, we found that elderly patients had different exclusionary criteria for treatment compared to younger patients: older patients were less likely to have the typical barriers such as substance abuse and psychiatric disorders; however, they were more likely to have medical co-morbidities, such as heart disease. Still, adjusting for these factors and others, we found that older age was independently associated with a lower likelihood of being considered a treatment candidate. In contrast, it appeared that being elderly was not associated with an increased likelihood of experiencing treatment side-effects or experiencing treatment failure.
This is the first study of which we are aware of to look at specific factors associated with treatment candidacy and clinician impressions of treatment candidacy among elderly patients with chronic hepatitis C. Although treatment guidelines do not specifically advise clinicians to withhold treatment for older adults, it is perhaps not surprising that older age was independently associated with a lower likelihood of being considered a treatment candidate and patient acceptance of treatment. Because chronic HCV is believed to induce liver fibrosis at a slow rate, a life expectancy of at least one or two decades should be a prerequisite for treatment in order for the benefits to be realized. However, since many patients in their 60s and 70s who are in good health can reasonably expect to live 20 years or more, treatment for chronic HCV may still be beneficial for certain patients. It is worth noting that even after adjusting for medical co-morbidities (which should help predict life-expectancy), age was still a predictor of not being considered a treatment candidate in this study.
Our finding that older age was not associated with a lower likelihood of treatment success is similar to what has been observed in prior research. Prior small observational studies conducted in Japan and the United States suggested that treatment with interferon may be equally effective in older compared to younger adults [12–14]. The largest study to date from France observed that SVR was achieved in 45% of the 170 patients 65 years of age or older who were treated with pegylated interferon and ribavirin for their chronic HCV [15]. Despite reports of more frequent cytopenias [16] and early discontinuation [13] reported in the literature, older patients in this study did not appear more likely to suffer side effects or need to discontinue treatment early due to side effects.
This study has important implication for clinical care. In the U.S., the majority of individuals infected with HCV will be entering their 60s within the next few decades [1]. Because patients with chronic hepatitis C are largely asymptomatic, many patients may not become aware of their condition until they interface with the medical system as an older adult. Therefore, the evaluation of elderly patients with HCV for treatment may become a more common scenario in the future. This study demonstrates that clinicians are less likely to treat older patients for HCV. However, it is unclear whether this disparity reflects clinicians’ accurate assessments of the life-expectancies of their patients or if physicians may unconsciously have an age bias. Furthermore, data on long-term outcomes associated with treatment are needed for all patients, including older patients. Clinicians who treat patients with HCV may benefit from a clinical framework for evaluating the need for HCV treatment in older adults, similar to what has been developed for cancer screening in older adults [17].
The strengths of this study include the large overall sample size, the inclusion of patients from multiple different medical centers throughout the United States, and its prospective design for data collection. Although an important finding of the paper, the relatively small percentage of elderly patients who ultimately received treatment for HCV (and the use of non-pegylated interferons) resulted in low rates of treatment success, and thus provided limited power for our treatment outcomes analyses. An additional limitation is the fact that this study enrolled patients who had already been referred to specialty clinics for evaluation for treatment. Therefore, the characteristics of older patients in our sample may not reflect the more general population of elderly patients with HCV who may have even higher rates of co-morbidities. However, since all patients came from this referral population, comparisons between older and younger patients should remain valid. Older patients who were treated may have been more aggressively screened for other health issues, which may have resulted in better treatment outcomes in that group. Finally, because this study was conducted among recipients of healthcare within the VA healthcare system, results may lack generalizeability.
In summary, this study of users of the VA healthcare found that only 10% of patients over the age of 60 years who were referred for management of HCV were treated. Older age was independently associated with not being considered a treatment candidate, even after adjustment for co-morbidities. Although only a small number of elderly patients were treated, results suggest that side effects, early discontinuation and, most importantly, treatment outcomes are similar between elderly and non-elderly patients. Further research is needed to determine how clinicians are using age to factor into their decisions on treatment candidacy.
References
Armstrong GL, Wasley A, Simard EP et al (2006) The prevalence of hepatitis C virus infection in the United States, 1999 through 2002. Ann Intern Med 144:705–714
NIH Consensus Statement on Management of Hepatitis C: (2002) NIH Consens State Sci Statements 19:1–46
Strader DB, Wright T, Thomas DL et al (2004) Diagnosis, management, and treatment of hepatitis C. Hepatology 39:1147–1171
Marcellin P, Asselah T, Boyer N (2002) Fibrosis and disease progression in hepatitis C. Hepatology 36:S47–S56
Poynard T, Ratziu V, Benmanov Y et al (2000) Fibrosis in patients with chronic hepatitis C: detection and significance. Semin Liver Dis 20:47–55
Seeff LB (2002) Natural history of chronic hepatitis C. Hepatology 36:S35–S46
Regev A, Schiff ER (2001) Liver disease in the elderly. Gastroenterol Clin North Am 30:547–63, x–xi
El-Serag HB, Mason AC (1999) Rising incidence of hepatocellular carcinoma in the United States. N Engl J Med 340:745–750
Bini EJ, Brau N, Currie S et al (2005) Prospective multicenter study of eligibility for antiviral therapy among 4,084 U.S. veterans with chronic hepatitis C virus infection. Am J Gastroenterol 100:1772–1779
Brau N, Bini EJ, Currie S et al (2006) Black patients with chronic hepatitis C have a lower sustained viral response rate than non-Blacks with genotype 1, but the same with genotypes 2/3, and this is not explained by more frequent dose reductions of interferon and ribavirin. J Viral Hepat 13:242–249
VA Centers of Excellence in Hepatitis C Research and Education. VA Treatment Recommendations for Patients with Chronic Hepatitis C: version 1.2. 2-25-1999
Horiike N, Masumoto T, Nakanishi K et al (1995) Interferon therapy for patients more than 60 years of age with chronic hepatitis C. J Gastroenterol Hepatol 10:246–249
Koyama R, Arase Y, Ikeda K et al (2006) Efficacy of interferon therapy in elderly patients with chronic hepatitis C. Intervirology 49:121–126
Van Thiel DH, Friedlander L, Caraceni P, Molloy PJ, Kania RJ (1995) Treatment of hepatitis C virus in elderly persons with interferon alpha. J Gerontol A Biol Sci Med Sci 50:M330–M333
Thabut D, Le Calvez S, Thibault V et al (2006) Hepatitis C in 6,865 patients 65 year or older: a severe and neglected curable disease? Am J Gastroenterol 101:1260–1267
Nudo C, Gupta S, Alpert E et al Elderly patients are at greater risk for cytopenia during anitviral therapy for hepatitis C. CDDW 2004 abstract, accessed at: http://www.cagacg.org/cddw/cddw2004/abs/abs048.htm
Walter LC, Covinsky KE (2001) Cancer screening in elderly patients: a framework for individualized decision making. Jama 285:2750–2756
Acknowledgements
Other Members of the VA-HCV-001 Study Group: Richard Moseley, Ann Arbor; Curt Hagedorn, Atlanta; David Johnson, Bay Pines; Marcos Pedrosa, Boston; Ayse Aytaman, Brooklyn; Charles Mendenhall, Cincinnati; Bhupinder Anand, Houston; Paul King, Columbia (MO); Franz Simon, Denver; Warren Schmidt, Iowa City; Ke-Qin Hu, Loma Linda; Timothy Morgan, Long Beach; Bradford Waters, Memphis; Lennox Jeffers, Miami; Samuel Ho, Minneapolis; Joseph Awad, Nashville; Ramsey Cheung, Palo Alto; Kyong-Mi Chang, Philadelphia; Jawad Ahmad, Pittsburgh; Anna Sasaki, Portland; Doris Strader/Ken Hirsch, Washington DC. This study was funded in part by the VA National HIV/Hepatitis Program and Schering-Plough Corporation. The authors also wish to thank Roche Molecular Systems, Inc. for providing Amplicor kits for HCV RNA testing for this study.
Author information
Authors and Affiliations
Consortia
Corresponding author
Rights and permissions
About this article
Cite this article
Tsui, J.I., Currie, S., Shen, H. et al. Treatment Eligibility and Outcomes in Elderly Patients with Chronic Hepatitis C: Results from the VA HCV-001 Study. Dig Dis Sci 53, 809–814 (2008). https://doi.org/10.1007/s10620-007-9926-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-007-9926-x