
Abstract
Background
Beliefs about the usefulness and controllability of emotions are associated with emotion regulation and psychological distress in the general population. Although individuals with schizophrenia-spectrum disorders evidence emotion regulation abnormalities, it is unclear whether emotional beliefs contribute to these difficulties and their associated poor clinical outcomes.
Methods
Participants included 72 individuals with schizophrenia-spectrum diagnoses (outpatients with schizophrenia n = 38; youth at clinical high-risk for psychosis, n = 34) and healthy controls (CN: n = 61) who completed the Emotional Beliefs Questionnaire, Emotion Regulation Questionnaire, and measures of clinical symptom severity.
Results
Those with schizophrenia-spectrum diagnoses reported believing that emotions were less controllable than CN; however, groups did not differ regarding beliefs about the usefulness of emotion. Greater beliefs of the uncontrollability of emotion were associated with greater use of suppression, less use of reappraisal, and increased negative symptoms. Emotion regulation partially mediated the association between emotional beliefs and negative symptoms.
Conclusions
Individuals in the schizophrenia-spectrum display superordinate beliefs that emotions are uncontrollable. These beliefs may influence emotion regulation strategy selection and success, which contributes to negative symptoms. Findings suggest that beliefs of emotional uncontrollability reflect a novel process related to both emotion regulation and negative symptoms that could be targeted in psychosocial treatments.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Emotion regulation refers to the use of strategies to influence the duration, frequency, or intensity of negative or positive emotions (Gross, 1998). Numerous psychiatric disorders display abnormalities in emotion regulation that predict the onset and maintenance of psychopathology (Sheppes, Suri, Gross, 2015). These abnormalities have been demonstrated to occur at multiple stages of the emotion regulation sequence proposed in Gross’ seminal extended process model (Gross, 2015). According to this model, separate but interactive systems exist for emotion generation and regulation. The first order emotion generation system involves four components: World (internal and external stimuli), Perception (attending to external or internal stimuli with emotional salience), Valuation (determination of whether the internal or external stimulus is motivationally relevant and whether the current emotional state differs from the desired goal state), and Action (initiation of a response designed to reduce discrepancies between current and desired emotional states). When this emotion generation cycle results in the identification of a mismatch between the current emotional state and the desired state, a second order emotion regulation system is initiated that unfolds over three consecutive stages: identification (detecting an emotional response and determining whether to make an emotion regulation attempt or not), selection (choosing an emotion regulation strategy that is contextually appropriate), and implementation (executing the selected strategy). Various disorders are thought to display distinct patterns of abnormalities at these three stages of emotion regulation. For example, at the identification stage over or under-detection of emotional response may contribute to identifying the need to regulate too frequently or not often enough. At the selection stage, individuals may represent too few or too many strategies to choose from in relation to the current context, or select strategies that are contextually maladaptive. At the implementation stage, abnormalities in effort exertion or difficulties in executing strategies may lead emotion regulation attempts to be ineffective at changing emotional states.
Given that abnormalities at any of the three stages can contribute to psychopathology, the identification of psychological mechanisms underlying emotion regulation abnormalities is of paramount importance for individual psychiatric disorders. If modifiable psychological targets are identified, psychosocial interventions can be tailored to target the precise psychological processes underlying a disorder’s specific emotion regulation profile. Unfortunately, few studies have focused on identifying modifiable psychological processes that contribute to emotion regulation abnormalities involved with specific disorders.
Emotional beliefs have emerged as a psychological process involved with several forms of psychopathology that could represent viable psychological treatment targets (Ford & Gross, 2018, 2019; Tamir et al., 2007). Two types of emotional beliefs may be of particular interest: controllability (i.e., the belief that emotions can be modified and intentionally controlled or come and go and cannot be controlled) and usefulness (i.e., the belief that emotions are good/ useful/ or bad /useless) (Becerra et al., 2020). Beliefs about controllability and usefulness may contribute to abnormalities at all three stages of the emotion regulation process, whether high or low (Ford & Gross, 2019). For example, beliefs that emotions are useless might lead to an excessive amount of emotion regulation attempts (identification), attempting strategies that are contextually maladaptive and selecting too many strategies (selection), over estimation of the efficacy of certain tactics (implementation). In contrast, beliefs that emotions are uncontrollable might lead to a failure to make emotion regulation attempts when it is most advantageous to do so (e.g., when negative emotion is high) (identification), fewer strategies being considered and contextually attempting strategies that are maladaptive (selection), under-estimation of the efficacy of certain tactics and reduced likelihood of effective execution (implementation). The cumulative effect of these emotion regulation abnormalities may be an increase in negative emotion and decrease in positive emotion, which contributes to various dimensions of psychopathology after emotion regulation failures accumulate over time. Thus, a primary means by which emotional beliefs may exert their influence on psychopathology is via an impact on individual stages of emotion regulation.
Schizophrenia (SZ) is a disorder characterized by abnormalities at each stage of emotion regulation: identification (a threshold that is too low), selection (increased rates of polyregulation, reduced selection of adaptive strategies and increased selection of maladaptive strategies), implementation (less effective use of a range of strategies to decrease negative emotion) (Chapman et al., 2020; Eack et al., 2016; Horan et al., 2013; Kimhy et al., 2020; Ludwig et al., 2020; Markela-Lerenc et al., 2009; Morris et al., 2012; Painter et al., 2019; Perry et al., 2012; Strauss et al., 2013, 2015, 2019; van der Meer et al., 2014; Visser et al., 2018). Importantly, these abnormalities are associated with a range of poor clinical outcomes, such as positive symptoms, negative symptoms, and poor functional outcome (Bartolomeo et al., 2021; Bartolomeo et al., 2022; Kimhy et al., 2012, 2014, 2020; Lincoln et al., 2015; Ludwig, Werner, & Lincoln, 2019; Macfie et al., 2022; Nittel et al., 2018; Raugh & Strauss, 2021; Strauss et al., 2013). Similar emotion regulation abnormalities have been observed in those at clinical high-risk (CHR) for psychosis (i.e., those who meet criteria for a prodromal syndrome that display attenuated positive symptoms and functional decline) (Chapman et al., 2020; Kimhy et al., 2016). Emotion regulation difficulties may therefore not only influence individual differences in the severity of clinical presentation among those with established SZ, but also serve as a vulnerability factor that increases probability of conversion among individuals at CHR for psychosis.
Although the link between emotion regulation abnormalities and psychopathology is well-established in the SZ-spectrum (i.e., among those with SZ and CHR diagnoses), it is unclear whether emotional beliefs play a role in this process. However, past research has found that SZ regulate more frequently at low levels of negative affect and less frequently at high levels of negative affect than CN (Raugh & Strauss, 2021); emotion beliefs may explain this discrepancy, such that SZ identify the need to regulate more frequently when negative emotion is low because they believe that negative emotions are not useful and fail to identify the need to regulate when negative affect is high because they believe intense emotions are uncontrollable. Additionally, those who believe emotions are less controllable have been shown to be less likely to select adaptive strategies (e.g., reappraisal) and more likely to exhibit depressive symptoms (e.g., anhedonia) (De Castella et al., 2013; Ford et al., 2018; Kneeland et al., 2020; Kneeland, Nolen- Hoeksema, Dovidio, & Gruber, 2016a, 2016b; Tamir et al., 2007; Veilleux et al., 2015). This may point to controllability beliefs as a positive factor in rates of successful emotion regulation and may be associated with negative symptom severity, considering that depression can contribute to negative symptoms. Finally, while there is scarce evidence on usefulness beliefs in clinical populations, in the general population researchers have found that greater beliefs that emotions are good/useful are associated with more motivation and reward-seeking behavior (Harmon-Jones et al., 2011; Tamir, Bigman, Rhodes, Salerno, & Schreier, 2015; Tamir & Ford, 2012; Wood et al., 2009). This may have implications for negative symptom severity in particular, such that beliefs that emotions are useless or bad may lead to lower motivation to execute goal-directed activity and less pleasure-seeking behaviors. While emotional beliefs may be particularly relevant for negative symptoms, it is also plausible that they would be associated with general symptoms and poor functioning given prior evidence that they predict anxiety, depression, stress, and functioning in community samples (Becerra et al., 2020).
The current study examined the role of emotional beliefs in emotion regulation abnormalities and symptoms among individuals with SZ-Spectrum disorders. Given that emotion regulation abnormalities have been demonstrated in both those with attenuated and full psychosis, analyses were conducted on a combined SZ-spectrum group encompassing all participants who fell on the continuum of psychotic experiences, as well as separately for outpatients with established SZ and individuals at clinical high-risk for psychosis (i.e., those who meet criteria for a prodromal syndrome characterized by subthreshold positive symptoms and functional decline or clinical distress) to explore whether different patterns emerged for the psychosis sub-groups. The following hypotheses were evaluated: (1) Individuals in the SZ-spectrum will believe that emotions are less useful and less controllable than CN; (2) Beliefs that emotions are less useful will be associated with greater severity of negative symptoms; (3) Beliefs of greater emotional uncontrollability will be associated with greater use of expressive suppression, less use of reappraisal, and greater severity of negative symptoms; (4) Habitual self-reported use of reappraisal and suppression will mediate the link between emotional beliefs and negative symptoms based on Ford and Gross’ model (Ford & Gross, 2019) proposing that emotional beliefs exert their influence on psychopathology indirectly via emotion regulation. Exploratory analyses related to sex differences were also conducted due to prior evidence that men have greater beliefs that positive emotions were useless compared to women (Becerra et al., 2020), and due to differences in clinical presentations between men and women with psychosis (e.g., negative symptoms are generally higher in men than women) (Kring & Moran, 2008). Additionally, given the novelty of the emotional beliefs construct, exploratory correlational and mediation analyses were also conducted to determine links with specific emotion regulation strategies and symptom domains.
Method
Participants
Data was collected from two samples: (1) outpatients with schizophrenia or schizoaffective disorder (SZ: n = 38) and their demographically matched healthy controls (CN: n = 31); (2) CHR participants (n = 34) and their demographically matched healthy controls (CN: n = 30). For analytic purposes, the SZ and CHR groups were evaluated in combination (n = 72) and separately by diagnostic group (SZ: n = 38; CHR: n = 34).
Outpatients with SZ were evaluated during periods of clinical stability as indicated by no self-reported change in medication type of dose within the past 4 weeks. The principal diagnosis was established via the Structured Clinical Interview for DSM-5 (SCID-5; First et al., 2014). All participants were outpatients who were primarily in the chronic phase of illness, had experienced multiple episodes, and were experiencing mild to moderate symptoms (see Table 1).
CHR participants were recruited from the Georgia Psychiatric Risk Evaluation Program (G-PREP), which receives referrals from local clinicians to perform diagnostic assessment and monitor evaluations for youth displaying psychotic experiences. CHR participants were also recruited via online and printed advertisements. CHR participants were included if they met criteria for a psychosis-risk syndrome on the Structured Interview for Psychosis-Risk Syndromes (SIPS; Miller et al., 1999). All CHR participants met SIPS criteria for Attenuated Positive Symptoms Syndrome (i.e., SIPS score of at least 3–5 on at least one positive symptom item, with a frequency of occurring at least once per week; 13 progression, 20 persistence, 1 partial remission). CHR participants did not meet lifetime criteria for a DSM-5 psychotic disorder as determined by the SCID-5. Two participants in the CHR sample were prescribed an antipsychotic medication at the time of assessment.
Healthy control participants (CN) were recruited from the community through print and online advertisements. CN completed a diagnostic clinical interview, including the SCID-5 (First et al., 2014) and SCID-5-PD (First et al., 2016) and did not meet criteria for any current psychiatric disorder or schizophrenia-spectrum personality disorder. CN also denied any family history of psychosis and did not meet lifetime criteria for any psychotic disorder.
No participants met criteria for current substance use disorders (except for nicotine) and all denied lifetime history of neurological disorders associated with cognitive impairment (e.g., traumatic brain injury, epilepsy). Individuals with SZ-Spectrum diagnoses and CN did not significantly differ in age, parental education, sex, or ethnicity; however, participants with SZ-Spectrum diagnoses had lower personal education than CN (see Table 1).
Procedures
All participants completed an online consent for a protocol approved by the University of Georgia Institutional Review Board. After completing the consent form, participants were then directed to complete a series of questionnaires administered over Qualtrics that took approximately 1 h. Subsequently, participants were scheduled to complete a semi-structured clinical interview via Zoom, which lasted approximately 10–20 min during which the Brief Negative Symptom Scale (BNSS; Kirkpatrick et al., 2011; Strauss et al., 2012a, 2012b) was completed. Interviews were administered by graduate students or laboratory staff trained to reliability standards (alpha > 0.80) using gold standard training videos developed by the authors of the BNSS. Participants received a $40 check payment for participating.
Online questionnaires covered a range of content as part of a larger study: demographics, COVID-19 health and safety behaviors, environmental factors, positive symptoms, negative symptoms, general symptoms (e.g., anxiety, depression, mania, sleep), internet/social media use, emotion beliefs, ideal affect, emotion regulation, and protective factors. Only the emotion regulation, emotional beliefs, and negative symptom data are discussed in this report.
Measures
Emotional Beliefs Questionnaire
The Emotional Beliefs Questionnaire (EBQ; Becerra et al., 2020) is a 16-item self-report measure of an individual’s beliefs about emotions. The measure assesses beliefs about the controllability and usefulness of emotions as posited by Ford and Gross (2019). Self-reports are made on a Likert scale from 1 (strongly disagree) to 7 (strongly agree), with higher scores indicating beliefs that emotions are more uncontrollable and less useful (i.e., more dysfunctional beliefs about emotion). Dimensions examined include: General controllability, positive emotion controllability, negative emotion controllability, general usefulness, positive usefulness, negative usefulness. Example items include: “Once people are experiencing negative emotions, there is nothing they can do about modifying them”; “There is very little use for negative emotions”. All subscales and composite scores in the current sample have acceptable to good levels of internal consistency: general controllability (α = 0.89), positive controllability (α = 0.82), negative controllability (α = 0.82), general usefulness (α = 0.76), positive usefulness (α = 0.70), and negative usefulness (α = 0.83).
Emotion Regulation Questionnaire
The Emotion Regulation Questionnaire (ERQ; Gross & John, 2003) is a 10-item self-report questionnaire that measures the extent to which participants report using reappraisal (6 items) and expressive suppression (4 items) strategies to regulate their positive and negative emotions. Responses are made on a 1 (strongly disagree) to 7 (strongly agree) scale, with higher scores reflecting greater dispositional tendencies toward using either reappraisal or suppression across time and different contexts. The ERQ in the current sample has acceptable to good levels of internal consistency, α = 0.88 for reappraisal and α = 0.77 for suppression.
Brief Negative Symptom Scale (BNSS)
The BNSS is a 13-item clinical rating scale designed to assess the five domains of negative symptoms in individuals with SZ-spectrum diagnoses: anhedonia, avolition, asociality, alogia, and blunted affect (Kirkpatrick et al., 2011). Psychometric properties of the BNSS have previously been established in SZ, CHR, and CN populations, demonstrating good inter-rater reliability, internal consistency, test–retest reliability, convergent validity, and discriminant validity (Strauss & Chapman, 2018; Strauss et al., 2012a, 2016). Confirmatory factor analyses and network analysis indicate that the BNSS yields both a 5-factor (anhedonia, avolition, asociality, blunted affect, alogia) and hierarchical structure (i.e., two 2nd-order high level factors consisting of diminished expression [EXP] and motivation and pleasure [MAP], in addition to 5 1st order lower-level factors consisting of the 5 consensus domains: anhedonia, avolition, asociality, blunted affect, alogia) in both SZ and CHR (Ahmed et al., 2018; Chang et al., 2021; Strauss et al., 2018). Analyses in this study focused on the 5 domains. In the current sample, the five factors had good to excellent levels of internal consistency: alogia (α = 0.88), anhedonia (α = 0.89), asociality (α = 0.81), avolition (α = 0.91), and blunted affect (α = 0.89).
Negative Symptom Inventory Self-Report (NSI-SR)
Negative symptoms were also measured via the Negative Symptom Inventory Self-Report (NSI-SR; Raugh et al., under review). This 11-item self-report questionnaire measures experiential and behavioral components of anhedonia, avolition, and asociality. Experiential items are rated on a 0 (not at all) to 10 (extremely) scale, with lower scores reflecting increased negative symptoms. Behavioral frequency items are rated in relation to the number of days per week a behavior occurs (0–7). Psychometric properties of the NSI-SR are good, including internal consistency, temporal stability, convergent validity with the BNSS, and discriminant validity with measures of positive and general symptoms (Raugh et al., under review). Factor analysis supports a 3-factor structure consisting of anhedonia, avolition, and asociality. Scores were reverse coded, such that higher scores reflect more severe negative symptoms. The three factors in the current sample had questionable to good levels of internal consistency: anhedonia (α = 0.82), asociality (α = 0.81), and avolition (α = 0.68).
Data Analysis
Analyses were conducted in two steps. First, for the combined SZ-spectrum sample (n = 72). Second, analyses were repeated for the CHR and SZ samples separately (see Supplemental Materials). Group differences in EBQ subscales were analyzed using one-way ANOVA (Hypothesis 1). Bivariate correlations were used to determine associations between EBQ scores and clinical symptoms (Hypotheses 2 and 3) and the Benjamini–Hochberg method was applied to correct for multiple comparisons. Mediation analyses were conducted to test the hypothesis that emotion regulation mediates the link between emotional beliefs and negative symptoms (Hypothesis 4). The direct and indirect (i.e., mediated) effects were estimated with the Mediation package in R (Tingley et al., 2014) where confidence intervals for the mediated effect were estimated using non-parametric bootstrapping with 1000 resamples. Exploratory ANOVAs were also conducted to examine sex differences in self-reported controllability and usefulness between SZ-Spectrum and CN groups. All analyses were conducted using R (R Core Team, 2022).
Results
Hypothesis 1: Group Differences in Emotional Beliefs
Emotion beliefs regarding positive usefulness, negative usefulness, and general usefulness did not significantly differ between the broadly defined SZ-Spectrum and CN groups (see Table 2 and Fig. 1). The SZ-spectrum group scored significantly higher on general controllability, positive controllability, and negative controllability compared to CN, indicating greater beliefs that emotions are uncontrollable in the SZ-Spectrum group (see Table 2).

Group Differences in EBQ General Controllability, Positive Usefulness, Negative Usefulness, and Total Scores. EBQ Emotion Beliefs Questionnaire, SZ-spectrum schizophrenia-spectrum participants, CN healthy controls. Red point indicates mean value and red bars indicate standard error. Blue points indicate raw score values by group (Color figure online)
Sub-group analyses indicated that SZ and CHR both did not differ from their respective CN groups on general usefulness. SZ had a trend toward greater beliefs that positive emotions are uncontrollable compared to CN. CHR reported believing that positive emotions were significantly more uncontrollable than CN (see Supplemental Materials Table S3). Furthermore, exploratory analyses comparing SZ and CHR groups indicated no significant differences on EBQ variables, supporting the decision to combine the groups into a broader SZ-Spectrum group (see Table S4). Exploratory analyses examining sex differences are also presented in Table S5.
Hypotheses 2 and 3: Correlations Between Emotional Beliefs, Symptoms, and Trait Emotion Regulation
Table 3 presents correlations in the full sample between EBQ general controllability, positive and negative usefulness scores, ERQ scores (i.e., whether participants endorsed habitual use of reappraisal or suppression), and symptom severity. General controllability was associated with 4/5 negative symptom domains, less use of reappraisal, greater use of suppression, greater severity of positive symptoms, and greater severity of depression. Positive and negative controllability generally showed similar associations as general controllability and each other. General usefulness and negative usefulness were associated with asociality and positive symptoms. Positive usefulness was associated with less use of reappraisal, greater use of suppression, and positive symptoms.
Supplemental tables S8 and S9 present exploratory correlations separately for SZ and CHR groups, which suggest that the SZ group was primarily driving the associations with positive symptoms noted in the full sample.
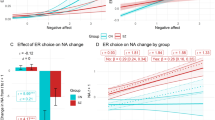
Hypothesis 4: Mediation Models
A complete reporting of mediation results is provided in supplemental materials. Of the 60 models that were run, 12 were significant. For significant models, results generally indicated that the link between controllability and negative symptoms was partially mediated by emotion regulation strategy use. A key example of this is presented in Fig. 2 which depicts the effect of the EBQ general controllability score on the BNSS total score which was partially mediated by the frequency of reappraisal. Other models using alternate negative symptom variables generally produced similar results. See supplementary materials for additional mediation analyses.

Mediation Analysis. Path analysis (N = 91). EBQ Emotion Beliefs Questionnaire, BNSS Brief Negative Symptom Scale.* = p < .05, ** = p < .01, *** = p < .001
Exploratory Analyses
Exploratory ANOVAs indicated that there were no significant interactions between sex and group on general controllability, positive usefulness, and negative usefulness scores. However, there was a significant group X sex interaction for positive controllability which indicated that in CN beliefs that positive emotions were uncontrollable were highest for males, but in SZ-spectrum beliefs that positive emotions were uncontrollable were highest for females (see supplemental materials).
Discussion
Increasing evidence points to a critical role for emotional beliefs in the development and maintenance of psychopathology (De Castella et al., 2015; Ford & Gross, 2019; Ford et al., 2018; Kneeland et al., 2016a, 2016b). Emotional beliefs may not only influence abnormalities in state emotional reactivity, but also habitual trait patterns of emotional experience and long-term mental health symptoms. Emotion regulation is thought to be the key mediating process that links emotional beliefs and psychiatric symptoms, dictating the nature of dysfunction observed at individual stages of emotion regulation (Ford & Gross, 2019). The current study extended this literature to the SZ-spectrum, finding a pattern of emotional beliefs characterized by normative beliefs about usefulness and exaggerated beliefs about the uncontrollability of emotion. Furthermore, beliefs of uncontrollability were associated with greater rates of utilizing expressive suppression (a maladaptive emotion regulation strategy), reduced rates of attempting reappraisal (an adaptive strategy), and higher severity of negative and positive symptoms. Importantly, the link between uncontrollability beliefs and negative symptoms was mediated by emotion regulation, supporting the overarching hypothesis posited by Ford and Gross (2019) that emotion regulation abnormalities dictate the effect of emotional beliefs on psychopathology.
How might emotional beliefs interact with emotion regulation processes to contribute to negative symptoms? Several explanations seem plausible. First, beliefs about emotion have long-term consequences on emotion regulation, dictating how often individuals chose to regulate, which strategies they select, and how successfully they implement those strategies (De Castella et al., 2013, 2018; Ford & Gross, 2019; Ford et al., 2018; Kneeland & Dovidio, 2020; Kneeland et al., 2016a, 2020). These emotion regulation attempts may in turn influence trait patterns of low positive and high negative emotion, which have been consistently linked to negative symptoms (Horan et al., 2006). Supporting this notion, past studies indicate that individuals who believe that emotions are controllable are more likely to use adaptive strategies, such as reappraisal, that are effective at reducing negative emotion and psychiatric symptoms (De Castella et al., 2013; Ford et al., 2018; Goodman et al., 2021; Kappes & Schikowski, 2013; Tamir et al., 2007). Our data suggests that those in the SZ-Spectrum who believe that emotions are uncontrollable are less likely to report using reappraisal, more likely to report using suppression, and more likely to exhibit a greater severity of negative symptoms, positive symptoms, and depression. Mediation analyses also clarified that emotion regulation is an intermediate process that links emotional beliefs to negative symptoms. Beliefs that emotions are uncontrollable may therefore reflect another psychological aspect of negative symptoms, similar to defeatist performance, anhedonic, and asocial beliefs. However, beliefs of uncontrollability may only lead to reductions in goal-directed, social, and recreational activity when individuals have difficulties using adaptive emotion regulation strategies to change their emotional states. It will be important for future studies to examine whether emotional beliefs are indeed a separate psychological process from asocial, anhedonic, and defeatist performance beliefs or whether they are simply a byproduct of these dysfunctional processes. One might expect that greater dysfunctional beliefs could be associated with the belief that emotions are less controllable and less useful. In line with the cognitive model of negative symptoms, there are multiple possibilities for how this association might come about. One possibility is that aversive early life experiences set the stage for developing dysfunctional beliefs which lead individuals to develop apathy and reductions in behavior that contribute to a general sense that the world is uncontrollable and useless, with emotions being but one component of that world. Another possibility is that aversive early life experiences produce early beliefs that emotions are uncontrollable and useless and these beliefs set the stage for the negative symptom related dysfunctional beliefs after repeated failures of emotion regulation. In turn, after the emotion beliefs lead to dysfunctional negative symptom beliefs, reductions in drive and apathy may become more ingrained. It is therefore possible that emotional beliefs have dysfunctional interactions with defeatist performance, asocial, and anhedonic beliefs- each of these may need to be targeted to successfully treat negative symptoms.
Second, Ford and Gross (2019) outlined a series of hypothetical interactions between uncontrollability and usefulness beliefs that could result in specific abnormalities at the identification, selection, and implementation stages defined in the extended process model (see Introduction); several of these abnormalities have been linked to negative symptoms in SZ (e.g., higher rates of identification when negative affect is low and lower rates of identification when negative affect is high; increased polyregulation at the selection stage; poorer implementation effectiveness; reduced rates of switching and delayed stopping). Thus, it is possible that beliefs that emotions are useful but uncontrollable might result in difficulties at identification, selection, implementation, and monitoring stages.
Third, prior evidence indicates that beliefs about the usefulness and controllability of emotion do not only influence emotion regulation processes and symptoms independently, but also via dynamic interactions with one another. For example, if an individual believes emotions are not useful, it would be beneficial for them to believe that emotions are controllable, if they are to initiate emotion regulation attempts that can change their emotional states. Those with depressive symptoms have been found to display an unhelpful pattern of emotional beliefs, whereby they believe that negative emotions are both not useful and uncontrollable, contributing to symptoms such as hopelessness and anergia (Alloy et al., 1999; Ford et al., 2018). Future ecological momentary assessment (EMA) studies are needed to determine whether interactive effects between controllability and usefulness have state-level effects on negative symptoms via their influence on emotion regulation.
Certain limitations should be considered. First, although the ERQ is a very useful measure of emotion regulation, it lacks specificity. It assesses trait emotion regulation and habitual strategy use, which conflates multiple stages. It is therefore impossible to determine whether the emotion regulation abnormalities observed on the ERQ reflect problems at the specific stages of identification, selection, or implementation. Instead of administering trait measures, future studies could use EMA or laboratory-based tasks to examine individual stages of emotion regulation and how they interact with emotional beliefs. Second, the EBQ is a trait measure. It is not possible to make direct inferences about the causal effect of emotional beliefs on emotion regulation without examining both variables at the state level. Temporally dynamic measures, such as EMA and psychophysiology, could allow each emotional belief component to be examined in isolation, as well as in interaction. Veilleux and colleagues (2021) conducted an EMA study on emotion beliefs in individuals with borderline personality disorder (BPD) and found that while overall beliefs within-individuals remained relatively stable, beliefs about the usefulness and controllability of emotions differed across levels of positive and negative affect. Greater negative affect predicted beliefs that emotions are bad and destructive, whereas greater positive affect predicted beliefs that emotions are controllable. Similar interactions between state emotional experience and emotional beliefs might be expected in the SZ-spectrum. Third, mediation models were conducted on cross-sectional data. Inferences regarding causality can therefore not be made. State measures that allow for temporally dynamic assessments may account for this limitation. Fourth, our outpatients diagnosed with SZ were on average mild to moderately symptomatic, had experienced multiple episodes, and were in the chronic phase of illness. CHR participants were also studied cross-sectionally and had not been re-evaluated longitudinally at the time of testing. It is therefore unclear how results might differ among individuals with more severe symptom presentations or CHR converters versus non-converters. Fifth, although analyses conducted on the broader SZ-spectrum sample were adequately powered, the exploratory analyses conducted on the separate CHR and SZ subgroups, as well as sex differences were under-powered. Recruitment was not designed to enable adequate power to test hypotheses related to exploratory analyses and future studies should plan to recruit larger, balanced samples of men and women to replicate these exploratory findings. Finally, data was collected during the COVID-19 pandemic. Negative symptoms have increased during the pandemic among those with SZ-Spectrum diagnoses (Strauss et al., 2021). The pandemic has also resulted in global increases in stress and a sense of uncontrollability in the world. It is therefore unclear whether the current findings regarding emotional controllability and usefulness are impacted by the pandemic and whether associations reported here could be expected to hold during non-pandemic times.
Despite these limitations, findings have important clinical implications. Treatments for negative symptoms are currently stalled. Pharmacological and psychosocial interventions have yielded minimal clinical benefits (Fusar-Poli et al., 2015). This may be because key mechanistic targets have yet to be identified. Growing evidence suggests that emotional beliefs are a viable treatment target in several forms of psychopathology, and that they are malleable mechanisms of change in psychosocial treatments. For example, efficacy has been reported for both short- and long-term interventions targeting emotional beliefs in psychiatric disorders such as social anxiety disorder. These interventions have not been applied to SZ-spectrum disorders. The current findings suggest that techniques used to augment beliefs of uncontrollability could have a beneficial effect on symptoms by changing the specific types of emotion regulation abnormalities that occur in SZ. For example, Kneeland and colleagues (2016b) found that participants who were induced to view emotions as fixed (instead of controllable) were less likely to engage in emotion regulation strategies compared to participants who were induced to view emotions as controllable. Goldin and colleagues (2012) also found that reappraisal self-efficacy mediated the relationship between individually administered cognitive behavioral therapy and social anxiety symptoms. Therefore, psychosocial treatments targeting uncontrollability beliefs, such as interventions instructing patients on how and when to use cognitive reappraisal in their daily lives, could be used. This may lead to more efficient decisions regarding when to regulate under conditions of high vs low negative affect, a wider and more adaptive range of strategies selected, greater success at implementing strategies, and more persistent efforts to regulate. If controllability beliefs are successfully augmented, improvements in emotion regulation could improve the low trait positive affect and high trait negative affect that are common to those with negative symptoms (Horan et al., 2008). A combination of techniques targeting emotional beliefs, emotion regulation, and motivation/social behavior may therefore offer promise for treating anhedonia, avolition, and asociality. Additionally, determining how emotional beliefs interact with interpersonal emotion regulation processes will be important, as these have been postulated to have an important role in psychopathology (Hofmann, 2014).
Data Availability
De-identified data will be made available upon request to the corresponding author.
References
Ahmed, A. O., Strauss, G. P., Buchanan, R. W., Kirkpatrick, B., & Carpenter, W. T. (2018). Schizophrenia heterogeneity revisited: Clinical, cognitive, and psychosocial correlates of statistically-derived negative symptoms subgroups. Journal of Psychiatric Research, 97, 8–15. https://doi.org/10.1016/j.jpsychires.2017.11.004
Alloy, L. B., Abramson, L. Y., Whitehouse, W. G., Hogan, M. E., Tashman, N. A., Steinberg, D. L., Rose, D. T., & Donovan, P. (1999). Depressogenic cognitive styles: Predictive validity, information processing and personality characteristics, and developmental origins. Behaviour Research and Therapy, 37(6), 503–531. https://doi.org/10.1016/S0005-7967(98)00157-0
Bartolomeo, L. A., Chapman, H. C., Raugh, I. M., & Strauss, G. P. (2021). Delay discounting in youth at clinical high-risk for psychosis and adults with schizophrenia. Psychological Medicine, 51(11), 1898–1905. https://doi.org/10.1017/S0033291720000677
Bartolomeo, L. A., Raugh, I. M., & Strauss, G. P. (2022). Deconstructing emotion regulation in schizophrenia: The nature and consequences of abnormalities in monitoring dynamics. Schizophrenia Research, 240, 135–142. https://doi.org/10.1016/j.schres.2021.12.043
Becerra, R., Preece, D. A., & Gross, J. J. (2020). Assessing beliefs about emotions: Development and validation of the Emotion Beliefs Questionnaire. PLOS ONE, 15(4), e0231395. https://doi.org/10.1371/journal.pone.0231395
Chang, W. C., Strauss, G. P., Ahmed, A. O., Wong, S. C. Y., Chan, J. K. N., Lee, E. H. M., Chan, S. K. W., Hui, C. L. M., James, S. H., Chapman, H. C., & Chen, E. Y. H. (2021). The latent structure of negative symptoms in individuals with attenuated psychosis syndrome and early psychosis: Support for the 5 consensus domains. Schizophrenia Bulletin, 47(2), 386–394. https://doi.org/10.1093/schbul/sbaa129
Chapman, H. C., Visser, K. F., Mittal, V. A., Gibb, B. E., Coles, M. E., & Strauss, G. P. (2020). Emotion regulation across the psychosis continuum. Development and Psychopathology, 32(1), 219–227. https://doi.org/10.1017/S0954579418001682
De Castella, K., Goldin, P., Jazaieri, H., Ziv, M., Dweck, C. S., & Gross, J. J. (2013). Beliefs about emotion: links to emotion regulation, well-being, and psychological distress. Basic and Applied Social Psychology, 35(6), 497–505. https://doi.org/10.1080/01973533.2013.840632
De Castella, K., Goldin, P., Jazaieri, H., Heimberg, R. G., Dweck, C. S., & Gross, J. J. (2015). Emotion beliefs and cognitive behavioural therapy for social anxiety disorder. Cognitive Behaviour Therapy, 44(2), 128–141. https://doi.org/10.1080/16506073.2014.974665
De Castella, K., Platow, M. J., Tamir, M., & Gross, J. J. (2018). Beliefs about emotion: Implications for avoidance-based emotion regulation and psychological health. Cognition and Emotion, 32(4), 773–795. https://doi.org/10.1080/02699931.2017.1353485
Eack, S. M., Wojtalik, J. A., Barb, S. M., Newhill, C. E., Keshavan, M. S., & Phillips, M. L. (2016). Fronto-limbic brain dysfunction during the regulation of emotion in schizophrenia. PLoS ONE, 11(3), e0149297. https://doi.org/10.1371/journal.pone.0149297
First, M. B. (2014). Structured clinical interview for the DSM (SCID). The encyclopedia of clinical psychology (pp. 1–6). Hoboken: Wiley. https://doi.org/10.1002/9781118625392.wbecp351
First, M. B., Williams, J. B., Benjamin, L. S., & Spitzer, R. L. (2016). SCID-5-PD: structured clinical interview for DSM-5® personality disorders. Washington: American Psychiatric Association Publishing.
Ford, B. Q., & Gross, J. J. (2018). Emotion regulation: Why beliefs matter. Canadian Psychology/psychologie Canadienne, 59(1), 1–14. https://doi.org/10.1037/cap0000142
Ford, B. Q., & Gross, J. J. (2019). Why beliefs about emotion matter: An emotion-regulation perspective. Current Directions in Psychological Science, 28(1), 74–81. https://doi.org/10.1177/0963721418806697
Ford, B. Q., Lwi, S. J., Gentzler, A. L., Hankin, B., & Mauss, I. B. (2018). The cost of believing emotions are uncontrollable: Youths’ beliefs about emotion predict emotion regulation and depressive symptoms. Journal of Experimental Psychology: General, 147(8), 1170–1190. https://doi.org/10.1037/xge0000396
Fusar-Poli, P., Papanastasiou, E., Stahl, D., Rocchetti, M., Carpenter, W., Shergill, S., & McGuire, P. (2015). Treatments of negative symptoms in schizophrenia: Meta-analysis of 168 randomized placebo-controlled trials. Schizophrenia Bulletin, 41(4), 892–899. https://doi.org/10.1093/schbul/sbu170
Goldin, P., Ziv, M., Jazaieri, H., Werner, K., Kraemer, H., Heimberg, R. G., & Gross, J. J. (2012). Cognitive reappraisal self-efficacy mediates the effects of individual cognitive-behavioral therapy for social anxiety disorder. Journal of Consulting and Clinical Psychology, 80(6), 1034–1040. https://doi.org/10.1037/a0028555
Goodman, F. R., Kashdan, T. B., & İmamoğlu, A. (2021). Valuing emotional control in social anxiety disorder: A multimethod study of emotion beliefs and emotion regulation. Emotion, 21(4), 842–855. https://doi.org/10.1037/emo0000750
Gross, J. J. (1998). The emerging field of emotion regulation: An integrative review. Review of General Psychology., 2(3), 271–299. https://doi.org/10.1037/1089-2680.2.3.271
Gross, J. J. (2015). Emotion regulation: Current status and future prospects. Psychological Inquiry, 26(1), 1–26. https://doi.org/10.1080/1047840X.2014.940781
Gross, J. J., & John, O. P. (2003). Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. Journal of Personality and Social Psychology, 85(2), 348–362. https://doi.org/10.1037/0022-3514.85.2.348
Harmon-Jones, E., Harmon-Jones, C., Amodio, D. M., & Gable, P. A. (2011). Attitudes toward emotions. Journal of Personality and Social Psychology, 101(6), 1332–1350. https://doi.org/10.1037/a0024951
Hofmann, S. G. (2014). Interpersonal emotion regulation model of mood and anxiety disorders. Cognitive Therapy and Research, 38(5), 483–492. https://doi.org/10.1007/s10608-014-9620-1
Horan, W. P., Blanchard, J. J., Clark, L. A., & Green, M. F. (2008). Affective traits in schizophrenia and schizotypy. Schizophrenia Bulletin, 34(5), 856–874. https://doi.org/10.1093/schbul/sbn083
Horan, W. P., Hajcak, G., Wynn, J. K., & Green, M. F. (2013). Impaired emotion regulation in schizophrenia: Evidence from event-related potentials. Psychological Medicine, 43(11), 2377–2391. https://doi.org/10.1017/S0033291713000019
Horan, W. P., Kring, A. M., & Blanchard, J. J. (2006). Anhedonia in schizophrenia: A review of assessment strategies. Schizophrenia Bulletin, 32(2), 259–273. https://doi.org/10.1093/schbul/sbj009
Kappes, A., & Schikowski, A. (2013). Implicit theories of emotion shape regulation of negative affect. Cognition & Emotion, 27(5), 952–960. https://doi.org/10.1080/02699931.2012.753415
Kimhy, D., Gill, K. E., Brucato, G., Vakhrusheva, J., Arndt, L., Gross, J. J., & Girgis, R. R. (2016). The impact of emotion awareness and regulation on social functioning in individuals at clinical high risk for psychosis. Psychological Medicine, 46(14), 2907–2918. https://doi.org/10.1017/S0033291716000490
Kimhy, D., Lister, A., Liu, Y., Vakhrusheva, J., Delespaul, P., Malaspina, D., Ospina, L. H., Mittal, V. A., Gross, J. J., & Wang, Y. (2020). The impact of emotion awareness and regulation on psychotic symptoms during daily functioning. Npj Schizophrenia, 6(1), 7. https://doi.org/10.1038/s41537-020-0096-6
Kimhy, D., Vakhrusheva, J., Jobson-Ahmed, L., Tarrier, N., Malaspina, D., & Gross, J. J. (2012). Emotion awareness and regulation in individuals with schizophrenia: Implications for social functioning. Psychiatry Research, 200(2–3), 193–201. https://doi.org/10.1016/j.psychres.2012.05.029
Kimhy, D., Vakhrusheva, J., Khan, S., Chang, R. W., Hansen, M. C., Ballon, J. S., Malaspina, D., & Gross, J. J. (2014). Emotional granularity and social functioning in individuals with schizophrenia: An experience sampling study. Journal of Psychiatric Research, 53, 141–148. https://doi.org/10.1016/j.jpsychires.2014.01.020
Kirkpatrick, B., Strauss, G. P., Nguyen, L., Fischer, B. A., Daniel, D. G., Cienfuegos, A., & Marder, S. R. (2011). The brief negative symptom scale: Psychometric properties. Schizophrenia Bulletin, 37(2), 300–305. https://doi.org/10.1093/schbul/sbq059
Kneeland, E. T., & Dovidio, J. F. (2020). Emotion malleability beliefs and coping with the college transition. Emotion, 20(3), 452–461. https://doi.org/10.1037/emo0000559
Kneeland, E. T., Goodman, F. R., & Dovidio, J. F. (2020). Emotion beliefs, emotion regulation, and emotional experiences in daily life. Behavior Therapy, 51(5), 728–738. https://doi.org/10.1016/j.beth.2019.10.007
Kneeland, E. T., Nolen-Hoeksema, S., Dovidio, J. F., & Gruber, J. (2016a). Emotion malleability beliefs influence the spontaneous regulation of social anxiety. Cognitive Therapy and Research, 40(4), 496–509. https://doi.org/10.1007/s10608-016-9765-1
Kneeland, E. T., Nolen-Hoeksema, S., Dovidio, J. F., & Gruber, J. (2016b). Beliefs about emotion’s malleability influence state emotion regulation. Motivation and Emotion, 40(5), 740–749. https://doi.org/10.1007/s11031-016-9566-6
Kring, A. M., & Moran, E. K. (2008). Emotional response deficits in schizophrenia: Insights from affective science. Schizophrenia Bulletin, 34(5), 819–834. https://doi.org/10.1093/schbul/sbn071
Lincoln, T. M., Hartmann, M., Köther, U., & Moritz, S. (2015). Dealing with feeling: Specific emotion regulation skills predict responses to stress in psychosis. Psychiatry Research, 228(2), 216–222. https://doi.org/10.1016/j.psychres.2015.04.003
Ludwig, L., Mehl, S., Krkovic, K., & Lincoln, T. M. (2020). Effectiveness of emotion regulation in daily life in individuals with psychosis and nonclinical controls—an experience-sampling study. Journal of Abnormal Psychology, 129(4), 408–421. https://doi.org/10.1037/abn0000505
Ludwig, L., Werner, D., & Lincoln, T. M. (2019). The relevance of cognitive emotion regulation to psychotic symptoms—a systematic review and meta-analysis. Clinical Psychology Review, 72, 101746. https://doi.org/10.1016/j.cpr.2019.101746
Macfie, W. G., Spilka, M. J., Bartolomeo, L. A., Gonzalez, C. M., & Strauss, G. P. (2022). Emotion regulation and social knowledge in youth at clinical high-risk for psychosis and outpatients with chronic schizophrenia: Associations with functional outcome and negative symptoms. Early Intervention in Psychiatry, 17(1), 21–28. https://doi.org/10.1111/eip.13287
Markela-Lerenc, J., Schmidt-Kraepelin, C., Roesch-Ely, D., Mundt, C., Weisbrod, M., & Kaiser, S. (2009). Stroop interference effect in schizophrenic patients: An electrophysiological approach. International Journal of Psychophysiology, 71(3), 248–257. https://doi.org/10.1016/j.ijpsycho.2008.10.005
Miller, T. J., McGlashan, T. H., Woods, S. W., Stein, K., Driesen, N., Corcoran, C. M., Hoffman, R., & Davidson, L. (1999). Symptom assessment in schizophrenic prodromal States. Psychiatric Quarterly, 70(4), 273–287.
Morris, R. W., Sparks, A., Mitchell, P. B., Weickert, C. S., & Green, M. J. (2012). Lack of cortico-limbic coupling in bipolar disorder and schizophrenia during emotion regulation. Translational Psychiatry, 2(3), e90. https://doi.org/10.1038/tp.2012.16
Nittel, C. M., Lincoln, T. M., Lamster, F., Leube, D., Rief, W., Kircher, T., & Mehl, S. (2018). Expressive suppression is associated with state paranoia in psychosis: An experience sampling study on the association between adaptive and maladaptive emotion regulation strategies and paranoia. British Journal of Clinical Psychology, 57(3), 291–312. https://doi.org/10.1111/bjc.12174
Painter, J. M., Stellar, J. E., Moran, E. K., & Kring, A. M. (2019). A multicomponent approach toward understanding emotion regulation in schizophrenia. Journal of Clinical Psychology, 75(1), 178–189. https://doi.org/10.1002/jclp.22698
Perry, Y., Henry, J. D., Nangle, M. R., & Grisham, J. R. (2012). Regulation of negative affect in schizophrenia: The effectiveness of acceptance versus reappraisal and suppression. Journal of Clinical and Experimental Neuropsychology, 34(5), 497–508. https://doi.org/10.1080/13803395.2012.661405
R Core Team (2022). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/.
Raugh, I. M., Luther, L., Bartolomeo, L. A., Gupta, T., Ristanovic, I., Pelletier-Baldelli, A., Mittal, V. A., Walker, E. F., & Strauss, G. P. (under review). Negative symptom inventory self-report (NSI-SR): Initial development and validation.
Raugh, I. M., & Strauss, G. P. (2021). Deconstructing emotion regulation in schizophrenia: The nature and consequences of abnormalities at the identification stage. European Archives of Psychiatry and Clinical Neuroscience. https://doi.org/10.1007/s00406-021-01350-z
Sheppes, G., Suri, G., & Gross, J. J. (2015). Emotion regulation and psychopathology. Annual Review of Clinical Psychology, 11(1), 379–405. https://doi.org/10.1146/annurev-clinpsy-032814-112739
Strauss, G. P., & Chapman, H. C. (2018). Preliminary psychometric properties of the brief negative symptom scale in youth at clinical high-risk for psychosis. Schizophrenia Research, 193, 435–437. https://doi.org/10.1016/j.schres.2017.07.051
Strauss, G. P., Hong, L. E., Gold, J. M., Buchanan, R. W., McMahon, R. P., Keller, W. R., Fischer, B. A., Catalano, L. T., Culbreth, A. J., Carpenter, W. T., & Kirkpatrick, B. (2012a). Factor structure of the brief negative symptom scale. Schizophrenia Research, 142(1–3), 96–98. https://doi.org/10.1016/j.schres.2012.09.007
Strauss, G. P., Kappenman, E. S., Culbreth, A. J., Catalano, L. T., Lee, B. G., & Gold, J. M. (2013). Emotion regulation abnormalities in schizophrenia: cognitive change strategies fail to decrease the neural response to unpleasant stimuli. Schizophrenia Bulletin, 39(4), 872–883. https://doi.org/10.1093/schbul/sbs186
Strauss, G. P., Kappenman, E. S., Culbreth, A. J., Catalano, L. T., Ossenfort, K. L., Lee, B. G., & Gold, J. M. (2015). Emotion regulation abnormalities in schizophrenia: Directed attention strategies fail to decrease the neurophysiological response to unpleasant stimuli. Journal of Abnormal Psychology, 124(2), 288–301. https://doi.org/10.1037/abn0000017
Strauss, G. P., Keller, W. R., Buchanan, R. W., Gold, J. M., Fischer, B. A., McMahon, R. P., Catalano, L. T., Culbreth, A. J., Carpenter, W. T., & Kirkpatrick, B. (2012b). Next-generation negative symptom assessment for clinical trials: Validation of the brief negative symptom scale. Schizophrenia Research, 142(1–3), 88–92. https://doi.org/10.1016/j.schres.2012.10.012
Strauss, G. P., Macdonald, K. I., Ruiz, I., Raugh, I. M., Bartolomeo, L. A., & James, S. H. (2021). The impact of the COVID-19 pandemic on negative symptoms in individuals at clinical high-risk for psychosis and outpatients with chronic schizophrenia. European Archives of Psychiatry and Clinical Neuroscience. https://doi.org/10.1007/s00406-021-01260-0
Strauss, G. P., Nuñez, A., Ahmed, A. O., Barchard, K. A., Granholm, E., Kirkpatrick, B., Gold, J. M., & Allen, D. N. (2018). The latent structure of negative symptoms in schizophrenia. JAMA Psychiatry, 75(12), 1271. https://doi.org/10.1001/jamapsychiatry.2018.2475
Strauss, G. P., Vertinski, M., Vogel, S. J., Ringdahl, E. N., & Allen, D. N. (2016). Negative symptoms in bipolar disorder and schizophrenia: A psychometric evaluation of the brief negative symptom scale across diagnostic categories. Schizophrenia Research, 170(2–3), 285–289. https://doi.org/10.1016/j.schres.2015.12.014
Strauss, G. P., Zamani Esfahlani, F., Visser, K. F., Dickinson, E. K., Gruber, J., & Sayama, H. (2019). Mathematically modeling emotion regulation abnormalities during psychotic experiences in schizophrenia. Clinical Psychological Science, 7(2), 216–233. https://doi.org/10.1177/2167702618810233
Tamir, M., Bigman, Y. E., Rhodes, E., Salerno, J., & Schreier, J. (2015). An expectancy-value model of emotion regulation: Implications for motivation, emotional experience, and decision making. Emotion, 15(1), 90–103. https://doi.org/10.1037/emo0000021
Tamir, M., & Ford, B. Q. (2012). Should people pursue feelings that feel good or feelings that do good? Emotional Preferences and Well-Being. Emotion, 12(5), 1061–1070. https://doi.org/10.1037/a0027223
Tamir, M., John, O. P., Srivastava, S., & Gross, J. J. (2007). Implicit theories of emotion: Affective and social outcomes across a major life transition. Journal of Personality and Social Psychology, 92(4), 731–744. https://doi.org/10.1037/0022-3514.92.4.731
Tingley, D., Yamamoto, T., Hirose, K., Keele, L., & Imai, K. (2014). Mediation: R package for causal mediation analysis. Journal of Statistical Software, 59, 5. https://doi.org/10.18637/jss.v059.i05
van der Meer, L., Swart, M., van der Velde, J., Pijnenborg, G., Wiersma, D., Bruggeman, R., & Aleman, A. (2014). Neural correlates of emotion regulation in patients with schizophrenia and non-affected siblings. PLoS ONE, 9(6), e99667. https://doi.org/10.1371/journal.pone.0099667
Veilleux, J. C., Salomaa, A. C., Shaver, J. A., Zielinski, M. J., & Pollert, G. A. (2015). Multidimensional assessment of beliefs about emotion: Development and validation of the emotion and regulation beliefs scale. Assessment, 22(1), 86–100. https://doi.org/10.1177/1073191114534883
Veilleux, J. C., Warner, E. A., Baker, D. E., & Chamberlain, K. D. (2021). Beliefs about emotion shift dynamically alongside momentary affect. Journal of Personality Disorders, 35, 83–113. https://doi.org/10.1521/pedi_2020_34_491
Visser, K. F., Esfahlani, F. Z., Sayama, H., & Strauss, G. P. (2018). An ecological momentary assessment evaluation of emotion regulation abnormalities in schizophrenia. Psychological Medicine, 48(14), 2337–2345. https://doi.org/10.1017/S0033291717003865
Wood, J. V., Heimpel, S. A., Manwell, L. A., & Whittington, E. J. (2009). This mood is familiar and I don’t deserve to feel better anyway: Mechanisms underlying self-esteem differences in motivation to repair sad moods. Journal of Personality and Social Psychology, 96(2), 363–380. https://doi.org/10.1037/a0012881
Acknowledgements
The authors wish to acknowledge members of the study team who collected data and the participants who generously devoted their time and effort to completing the study.
Funding
This work was supported by the National Institute of Mental Health (Grant numbers: R21-MH122863 and R21-MH112925) to Dr. Strauss. The funding source was not involved in the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
AMB: conceptualization, formal analysis, data curation, writing—original draft, writing—review and editing, visualization, project administration. SHJ: data curation, formal analysis, writing—review and editing. IMR: data curation, writing—review and editing. GPS: conceptualization, writing—original draft, writing—review and editing, resources, supervision.
Corresponding author
Ethics declarations
Conflict of Interest
AB, SJ, and IR declare they have no financial disclosures to report. Dr. GPS is an original developer of the BNSS who receives compensation for commercial use of the scale, which is donated to the Brain and Behavior Research Foundation. In the past 2 years, he has also consulted for: Minerva, Lundbeck, Acadia, Sunovion, Otsuka, and Boeringer-Ingelheim. AMB, SHJ, IMR, GPS declare that they have no conflict of interest.
Ethical Approval
Approval was obtained from the University of Georgia Institutional Review Board. The procedures used in this study adhere to the tenets of the 1964 Helsinki Declaration and its later amendments.
Animal Rights
No animal studies were carried out by the authors for this article.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Berglund, A.M., James, S.H., Raugh, I.M. et al. Beliefs About the Uncontrollability and Usefulness of Emotion in the Schizophrenia-Spectrum: Links to Emotion Regulation and Negative Symptoms. Cogn Ther Res 47, 282–294 (2023). https://doi.org/10.1007/s10608-023-10357-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10608-023-10357-w