
Abstract
Background
Over the last decades, brain surgery became a more frequently applied treatment for temporal lobe epilepsy (TLE). Despite its success, several studies found de-novo post-operative psychiatric symptoms in TLE surgery patients. Cognitive behavioural therapy is effective to treat brain healthy psychiatric patients but might not be translatable to patients with resections in emotion regulating networks as these areas seem to be essentially involved in successful psychotherapeutic treatment.
Methods
Here we report the case of a female patient with medically refractory medial temporal lobe epilepsy resulting in left anterior temporal lobectomy at age 35. Post operation she did not show adequate fearful response but at the same time manifested symptoms of a severe panic disorder. We investigated if this patient, despite lesions in emotion-behaviour brain circuits, can benefit from cognitive behavioural therapy.
Results
The intervention, customized to the specific resources and difficulties of the patient, was effective in stopping panic attacks and improving social functioning.
Conclusions
This case shows that MTL brain surgery patients may benefit from CBT and demonstrates the important and if yet still somewhat mysterious role of the amygdala in emotion regulation processes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
MTL Epilepsy and Treatment by Surgery
Temporal lobe epilepsy (TLE) is the most common form of focal epilepsy (Devinsky, 2004; Wiebe, 2000). A frequently diagnosed subtype of TLE is medial temporal lobe epilepsy (MTLE) where the internal (limbic) structures of the temporal lobe are involved (Williamson et al., 1993). Recurrent seizures can have a negative effect on cognitive functions including memory, language or social judgments (Golouboff et al., 2008; Ledoux & Gordon, 2011; Zeman et al., 2012; Zhao et al., 2014). The prescription of anti-epileptic drugs is the first approach to reduce seizure frequency but up to one third of all epileptic patients are refractory to medication (Kwan & Brodie, 2000; Schuele & Lüders, 2008; Spencer, 2002). For drug resistant MTLE, neurosurgery has shown promising results with up to 7 of 10 patients living seizure-free afterwards (Engel et al., 2012; McIntosh et al., 2004). Surgical options for these patients include resection of parts of the temporal lobes (i.e. anterior temporal lobe resection, resection of the amygdala or hippocampus) or lobectomy of the entire temporal lobe, depending on the epileptogenic zone (Al-Otaibi et al., 2012). Currently, the main measure of surgery success is a reduction of seizure frequency (Wieser et al., 2003). Despite the reported achievement concerning seizure outcome as well as the importance of early referral, epilepsy surgery is still seen as a treatment of last resort (Erba et al., 2012). Because of the significant functional role of the temporal lobe areas, it is not only a crucial question how TLE surgery affects seizure frequency per se, but also how it might influence the mental well-being of the patient.
Emotional Disorders Before and After Surgery
The study of fear and anxiety is challenging and there has been a long debate about how to best investigate and define these emotions and what should be considered to be part of the neuroanatomical system underlying those emotions (see for example Lang, 1969; Berridge & Kringelbach, 2008, 2011, for a discussion of the different viewpoints of the most influential contemporary scientists, see Mobbs et al., 2019). However, regarding the neuroanatomical correlates, research indicates that regions that are involved in TLE (and are thus the target of TLE surgery) also play an important role for human fear and anxiety. Regions that have been identified to process threat include the amygdala, insula, hippocampus, parts of the brainstem and the anterior cingulate cortex and have been initially summarized under the term ‘fear-network’ (Gorman et al., 2000). Other studies indicate that brain activity associated with the physiological response to a threat is distinct from the neuronal activity that leads to a conscious and subjective feeling of fear and anxiety (Bornemann et al., 2012; Feinstein et al., 2013; Hoppenbrouwers et al., 2016; Inman et al., 2020; Lang, 1969; LeDoux, 2020; Öhman, 2005). In the ‘two-systems-model’ proposed by LeDoux and Pine, the amygdala is identified as a main contributor to immediate defensive bodily reactions and actions in response to threats (LeDoux & Pine, 2016). Feelings of fear and anxiety arise from cortical circuits that are responsible for the conscious experience. The perception of fear or panic, in this perceptive, is the result of the cognitive interpretation of a situation (Barrett, 2017; LeDoux & Brown, 2017; Taschereau-Dumouchel et al, 2020).
In anxiety-disorder patients, areas that regulate fear and anxiety show abnormal activity (Coplan & Lydiard, 1998; de Carvalho et al., 2010a; Etkin & Wager, 2007; Lai, 2011; Massana et al., 2003; Porto et al., 2009; Sakai et al., 2005; Sylvester et al., 2012). With respect to the underlying neurocircuitry of panic different proposal were made. Gorman proposed that these patients have a hypersensitivity with resultant hyperactivity in member areas of the fear network where especially the amygdala may foster panic disorders. This hyperactivity may counteract any inhibitory action of the frontal cortex and thus deprive the brain of an effective system to regulate fear responses (Gorman et al., 2000). This type of model is similar to the models proposed for other anxiety disorders such as PTSD. More recent functional studies on the neurocircuitry of panic disorder suggest that the abnormal activation takes place in the extended fear network (in brainstem, anterior and midcingulate cortex, insula, and lateral as well as medial parts of the prefrontal cortex) and not exclusively in the amygdala (Etkin & Wager, 2007; Feldker et al., 2016; Sobanski & Wagner, 2017).
As TLE and the fear and anxiety circuits share common regions, the comorbidity of TLE with psychiatric disorders such as depression, anxiety disorders or obsessive–compulsive disorder is not surprising (de Araujo Filho et al., 2008; Glosser et al., 2000; Hermann et al., 2000; Kanner, 2016). Panic disorder, for example, has prevalence rates ranging between 5 and 21% in TLE patients compared to 0.5–3% in the general population (Brandt et al., 2010; Mula et al., 2009). Previous studies reported contradicting results concerning the psychiatric symptom changes and de novo appearance of psychiatric disorders after surgery. In 70 TLE surgery patients, Pintor et al. (2007) found that anxiety disorders decreased from 21.5% pre-surgery to 14.2% post-surgery over the first 12 month. In contrast to that, Glosser et al. (2000) reported 25% of patients experienced de novo psychiatric symptoms or even worsening of pre-existing symptoms after TLE-surgery. Cleary et al. (2012) found in 280 patients that 38% of them had significant psychiatric problems and 18% showed de novo psychopathology over a period of 4 years after TLE surgery. Especially in patients with MTL resection postoperative anxiety significantly increased, regardless of seizure outcome (Halley et al., 2010). One frequently reported risk factor for post-operative psychiatric disease in TLE patients are pre-existing psychiatric symptoms (Anhoury et al., 2000; Devinsky et al., 2005; Wrench et al., 2011).
Despite the high prevalence of comorbid anxiety in epilepsy and postoperative anxiety and panic after TLE surgery, very little is known about optimal treatment strategies and helpful interventions for this patient group. The best established approach to treat symptoms of anxiety and panic is cognitive behavioural therapy (CBT). CBT is the recommended therapy in the guidelines for anxiety disorders (Bandelow et al., 2014). However, data on efficacy of CBT from randomized controlled trials is only available for patients without brain damage (Beck et al., 1992; Clum et al., 1993; Gould et al., 1995; Haby et al., 2006; Otte, 2011; Ougrin, 2011). In CBT the patient learns to change behavioural and thinking patterns regarding body sensations (Clark, 1986) leading to a better emotion regulation of anxiety responses (Messina et al., 2013). The main hypotheses for the effect of CBT on brain functioning suggests that it influences the interaction between prefrontal areas and the subcortical fear and anxiety circuits (de Carvalho et al., 2010b). This might be accomplished by a more effective top-down regulation of hypersensitive and limbic structures by prefrontal control networks (Gorman et al., 2000; Kennedy et al., 2007; McNally, 2007; Roffman et al., 2005). In a multicenter brain imaging study, researchers investigated CBT treatment-related neural changes in patients with panic disorders (Kircher et al., 2013). In a fear-conditioning paradigm, they found reduced activation in the amygdala, bilateral anterior insula and the left inferior frontal gyrus (IFG) for the conditioned responses. Additionally, results showed an increased connectivity between the IFG and the subcortical parts of the fear and anxiety circuits.
Given the correlative nature of brain-imaging outcomes, it remains unclear whether the observed changes in brain activity and connectivity play a causal role in the therapeutic success or put differently, it remains unclear whether the integrity of structures within the fear and anxiety circuits are an essential precondition for therapeutic success. Given the aforementioned putative reliance of CBT on the modulation of frontal and limbic area, it remains unclear whether CBT can be effective in patients with damage to those brain areas, as in the case of TLE surgery patients. After TLE brain surgery, networks and interactions that usually respond to CBT are partially or completely removed or disconnected. Crucial brain areas are decoupled by surgery, resulting in an imbalanced activity and disturbed neural signalling, perhaps leaving those brain areas unable to process and benefit from regulatory input induced by CBT. While case number of patients after TLE surgery increase with many of those patients suffering worse psychiatric symptoms after surgery than before, there is still curiously little known about the effects of psychotherapy in patients after TLE surgery. It has not been examined if CBT, primarily developed in and for patients without brain lesions, will improve or aggravate fear symptoms in patients where regions of the fear-network are neurologically compromised. Here, we want to pursue this issue by reporting the case of patient HZ who suffered from severe panic attacks and impaired emotion processing after anterior temporal lobe resection and amygdalohippocampectomy in the left hemisphere. HZ received CBT which successfully reduced and finally stopped her panic attacks, and allowed her to acquire successful coping strategies to deal with her functional deficits. After describing her case and the treatment procedure, we will also discuss the factors and implications for clinical psychologists working with patients after TLE surgery.
Case Report
Clinical History
HZ lives in a small village in Germany, is married and the mother of two children. After nine years of school, she visited a school for home economics and then took over her parent’s farm. She had no medical history of neurological complaints or psychiatric symptoms until the age of 30, when she started to have epileptic seizures. HZ’s epilepsy was diagnosed as focal epilepsy with epigastric and emotional auras and automotoric and dialeptic seizures. Seizures occurred several times a day for about 10 min each. She suffered from regular headaches with a sharp left-sided pain as well as depressive mood, irritability, sadness and insomnia.
Antiepileptic medical treatment reduced seizure frequency from 10 to 15 seizures per day to at most one seizure per week. Neurological examinations included EEG and Video-EEG examinations as well as SPECT, PET-CT and MRI. This traced the epileptic focus to the left temporal mesial region, which also corresponded to the observed seizure type. Brain imaging revealed an enlarged left amygdala with local glucose hypometabolism. The diagnostic findings suggested left temporal-lobe epilepsy with hippocampal sclerosis.
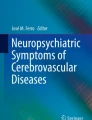
Different types of anticonvulsive medication did not reduce seizure frequency reliably long-term. HZ received an anteromedial temporal pole resection with amygdalohippocampectomy in the left hemisphere 5 years after onset of epileptic seizures. The procedure was performed without any complications. Post-operative histopathology found hippocampal sclerosis with reduced grey-white distinction and an enlarged amygdala with reactive gliosis. Figure 1 shows T1 MRI after the operation. Precautionary anticonvulsive medication was maintained. HZ was still seizure-free one year after surgery, therefore the medication was reduced and finally stopped. No seizures have occurred since.

T1 weighted imaging of HZ after amygdalohippocampectomy in the left hemisphere
In the months following the medical surgery, HZ experienced hypomania, insomnia and inner restlessness. Her mood improved but she was irritable and quick-tempered. She had difficulties to recall past events and worried about forgetting her plans unless she fixed those plans on paper. Most of all, HZ was unsettled because of a dramatic change in her ability to perceive and experience emotions. She noticed that she did not feel anxious anymore in situations she remembered as threatening from her past, for example working in great heights in the barn. She was perfectly able to identify this or other situations as potentially dangerous and realized that she risked her life in those situations while observing in herself a previously unknown lack of fear and concern. Additionally, HZ reported the absence of emotional closeness and affection towards her children and her husband. She generally felt emotionally blunt, felt estranged to others, less empathetic and was emotionally unaffected by sad events (e.g. death of a neighbour). HZ had difficulties to empathize and avoided physical contact with friends and relatives. She also reported having difficulties in interpreting facial expressions even from close family members. HZ was highly concerned and unsettled by these changes. Approximately half a year post-operation she experienced occasional episodes of intense anxiety including rapid breathing, palpitation, trembling and sweating combined with a desperate fear to faint. She had no motor phenomena, amnesia, loss of consciousness or any other neurological symptoms that could be interpreted as signs of an epileptic seizure. Her attacks primarily occurred in social situations, for example when attending church or when waiting in a queue. The discomfort would vanish as soon as she left the situation. Her initial reaction was to avoid these situations, which increasingly restricted her in her everyday life. HZ did not take any medication to treat the panic attacks.
Neuropsychological Results
Neuropsychological examinations were conducted before and after TLE surgery (see Table 1). Before surgery, HZ noticed semantic and episodic memory problems: she had difficulties to remember names and appointments and occasionally did not recall events that took place only some days or weeks in the past. She complained about word-finding difficulties in conversations. Her neuropsychological examination (Table 1) showed mostly age-appropriate cognitive performance with the exception of a significant impairment in verbal learning. Signs of a minor depression were revealed in a self-evaluation report (BDI-II).
Post-operative neuropsychological examinations found verbal learning ability improved; verbal retrieval was only mildly impaired. On the basis of her psychiatric symptoms and her subjective description of difficulties in emotional perception (see H.Z.’s clinical history), she was tested with neuropsychological tests on emotion and face perception. The Ekman 60 Faces Test (Young et al., 2002) was used to evaluate emotional face perception. This test uses 60 photographs of six different male and female emotional faces displaying anger, disgust, fear, happiness, sadness and surprise. There is a maximum of 60 correct responses, 10 for each emotion. Each face is shown for 5 s, responses are recorded by mouse click to the on-screen buttons. HZ assigned none of the fearful faces correctly. Instead, fearful faces where seen as anger (3), disgust (4), sadness (1) or surprise (2). HZ chose fear as response, albeit incorrectly (the correct emotion would have been sadness), in only one instance. The emotion perception deficit is not due to a general face perception impairment as face perception tests (Benton Facial Recognition Test, Cambridge Face Memory Test) showed no impairment in face recognition abilities.
Cognitive Behavioural Therapy
Because HZ’s panic attacks persisted for several months and she was concerned about the impact on her everyday life, she sought psychotherapeutic help. HZ had exploratory sessions with a licensed psychotherapist. After these sessions the therapist had doubts about the chance of success of any behavioural therapy intervention to treat HZ’s panic disorder. Due to HZ’s brain lesion, CBT process-relevant brain areas might be damaged and prevent therapy effect. HZ then started CBT with the co-author of this report (PM), a licensed psychotherapist with background in clinical neuropsychology. Therapy started in 2015 (14-month post-surgery). CBT lasted for 2.5 years. The first six month sessions were scheduled weekly. After, frequency of sessions was reduced to one session every few weeks or whenever necessary. Until now HZ had about 50 sessions CBT. Her health insurance company confirmed the need for therapy and covered the costs of her treatment. HZ was very motivated throughout therapy. She wrote a daily journal during the time of therapy, which she also used to record notes of her emotional state and to keep track of changes she observed.
Therapy focused on HZ’s disrupted emotional experience after amygdalohippocampectomy, which most prominently led to (1) indifferent feelings towards close persons and (2) severe panic in inadequate situations. The characteristics of her recurrent episodes of anxiety met the DSM-5 criteria for agoraphobia with panic attacks (American Psychiatric Association 2013). The therapeutic goals were to support her in coping with these changes, extend her understanding of her brain impairment and to reduce and ideally stop panic attacks. Concerning the second goal, the therapist’s approach was to attend to HZ’s panic disorder using the standard CBT components for treatment panic disorder: (I) psychoeducation, (II) cognitive therapy, (III) relaxation methods, and (IV) exposure therapy (Bandelow et al., 2014; Heinrichs et al., 2009). The gradual exposure to situations that might induce panic attacks consisted of exercises (i.e. going to church or shopping) which HZ and her therapist carefully planned and prepared during therapy sessions. HZ reported the outcome in her following session and HZ and her therapist analysed HZ’s experience to prepare the next exercise.
The therapeutic progress included the following steps:
-
1.
Develop therapeutic relationship, anamnesis and address resources
Discuss personal and family history, typical behaviour and attitude, guiding principles in life, support system (family, friends) and other resources.
HZ brought photographs of her close family, her home and photographs of special occasions in her life into the first sessions. She described her husband, children and friends as being very supportive, caring and sympathetic. She felt supported by her local church community. Apart from information on social resources, the therapist and HZ collected information on activities that might help HZ to relax.
-
2.
Analysis of the current state
Address the patient’s own concept of her complaints. Under which circumstances do these complaints occur?
HZ was alarmed by her lack of emotions towards her family and the occurrence of anxiety and panic in objectively harmless situations (see SORC model illustrating one situation, below). She worried that due to increasing anticipatory anxiety she would withdraw from social life and consequently not be able to support her children as she wished to. In the following we will provide an example of one SORC model for one specific panic-inducing situation, namely sitting in church.
S: Situation = HZ is sitting in church during a mass in the middle of a church pew.
O: Organism = “I don’t feel so good. I want to leave now. This will draw attention. Everyone would look at me and wonder why I leave.”
R: Reaction = increasing heartbeat, sweaty hands, abdominal discomfort, fear to faint, feeling of being locked in.
C: Consequence = short-term: leaving the church and instant ease of symptoms, feeling ashamed and irrational, long-term: anticipatory anxiety, avoiding situations (crowded places) that might trigger panic attacks.
-
3.
Set therapy goals
Focus on one or two realistic goals that refer to the most pressing complaints and describe them as detailed as possible.
HZ and the therapist identified two main goals:
-
1.
Reduce number and intensity of panic attacks. A complete absence of panic attacks might not be achievable.
-
2.
Integration of impairment and deficits in everyday life. For HZ this meant primarily to be able to care in a compassionate way for her family despite changes in emotional perception.
-
1.
-
4.
Psychoeducation
Provide information on current neuropsychological knowledge about the psychological condition.
HZ was educated on the connection of brain state and emotional state, the emotional networks in the brain and probable changes in brain functioning (i.e. emotion perception or memory function) due to TLE surgery.
-
5.
Cognitive therapy
Develop skills for reviewing one’s own perception and the interpretation of physical symptoms or behaviour.
Cognitive restructuring with HZ included the following instruments and exercises:
-
1.
Cognitive triad (Thoughts, Emotions, Behaviour) (Beck, 2002) and SORC model (Kanfer et al., 1969).
-
2.
The vicious circle of fear and the possibility to interrupt (Hagena & Gebauer, 2014).
-
3.
The concept of a benevolent companion and inner critic (Stinckens et al., 2013)
-
4.
Training of perception and body reactions, mindfulness of own feelings and needs.
-
1.
-
6.
Developing mental and behavioural strategies for occurring panic attacks
Choose and exercise strategies to regain a sense of control when panic attacks occur.
HZ was instructed with exercises to increase stress tolerance and self-regulation. She identified individual stress releasing actions such as squeezing a stress ball, imagination techniques (i.e. save space exercise (Reddemann, 2017) as well as muscle relaxation techniques (Margraf & Schneider, 2018) and techniques to actively redirect attention (i.e. mental arithmetic).
-
7.
Creating awareness for patients’s impairments in the patient’s social environment
Enable the patient to talk about his or her impairments and needs and offer sessions with family, partners or friends if necessary.
This step included supporting HZ in communicating with family and close friends about the effects of the TLE-brain surgery, about the resulting disability to interpret facial expression and about the fact that this might cause irritation in social contacts. HZ was encouraged to talk openly about her condition and the changes in emotional perception that she experienced.
-
8.
Gradual exposure therapy for panic inducing situations
Apply the developed strategies for extinction learning to gradually decrease the fear-response.
HZ was encouraged to try different strategies for stress reduction and attention-redirection techniques (see 6.) until she had identified the strategies that would help her to stay in the situation and tolerate the situation. Leaving the situation was the last choice.
Current Status
HZ is free from epileptic seizures and takes no anticonvulsive medication or psychiatric drugs. According to HZ and her therapist, she developed acceptance and management of the consequences of the MTL-resectomy. Her perception of facial expressions of emotions remains impaired and she reports having difficulties to sense emotions and moods of others in every-day life. In the beginning, the lack of this ability made her feel insufficient especially when interacting with her own children and insecure when interacting with others. Throughout therapy HZ acquired a better understanding about the links between brain functioning and emotions and the probable changes due to her brain surgery. Learning about the neuronal networks of emotion regulation enabled her to explain her difficulties to close family and friends who reacted in an understanding and supportive way. HZ says, she is now more ready to directly ask someone about his or her emotional state. HZ’s reduced experience of fear considerably changed her behaviour towards dangerous situations: for instance, she described that she would now be very much interested in trying out bungee jumping, an experience she had found to be rather life-threatening than thrilling before the surgery. Over the course of her therapy her panic attacks have become gradually less frequent. One year after the start of therapy the panic attacks have disappeared completely and have not re-emerged until now despite the fact that HZ exposes herself regularly to situations where she either has had panic attacks in the past or was worried about having one. HZ reports to still feel nervous in some situations occasionally, but these symptoms do not meet the criteria for a panic disorder. She no longer avoids crowded places and applies stress-reducing techniques effectively. She schedules time for relaxation and recreation for each day. Currently, HZ schedules therapeutic sessions on demand. At least twice a year a meeting takes place to monitor her progress.
Discussion
We presented the case of HZ who received unilateral amygdala resection for epilepsy treatment. This case offers helpful information for therapists working with TLE surgery patients and new insights on the effect of TLE surgery on emotion regulating networks.
Post-operation HZ displayed two distinct changes in emotional perception and processing: an impaired emotional face perception and increased inadequate fearful responses. HZ’s limited abilities in interpreting facial emotions in both experimental conditions and in every-day life are in accordance with earlier findings from patients with amygdala lesions that demonstrate the important role of the amygdala for recognizing and appropriately reacting to fear-inducing stimuli (Anderson, 2007). Indeed, several studies on patients with damage to the amygdala found an impaired ability to correctly recognize emotional facial expressions, especially in the case of fearful faces (Adolphs et al., 1994, 1999, 2003; Brierley et al., 2004; Calder, 1996; Pishnamazi et al., 2016). One of the most intensively studied patients with bilateral amygdala damage is S.M. This patient suffered from Urbach-Wiethe disease (Tranel & Hyman, 1990). S.M. showed absence of fear in the presence of fear inducing stimuli (i.e. venomous snakes or spiders) (Feinstein et al., 2011; Lilienfeld et al., 2018). Amygdala damage may affect not only visual perception but also the recognition of emotional voices (Dellacherie et al., 2011). The physiological reactions to arousing stimuli also seem to be altered by amygdala lesion according to some studies (Anderson & Phelps, 2002; Gläscher & Adolphs, 2003). Table 2 presents results from face-emotion tests of our patient in comparison to those from three other patients with amygdala damage (Broks et al., 1998). As can be seen HZ performed particularly poorly in that domain even in comparison with other patients.
One particularly interesting aspect of HZ’s post-operative clinical picture is the development of panic attacks. This exaggerated fear response occurred in objectively harmless situations, while in potentially life-threatening situations (e.g. great height) HZ showed no emotional response. The panic attacks unsettled and worried HZ so much that she sought therapeutic help. This provided us with the opportunity to examine an interesting question: Is it possible to treat panic disorder using CBT in a patient with damage to the amygdala?
The amygdala is a critical part of the fear and anxiety circuits. In laboratory settings these networks are frequently studied by using classical conditioning experiments (LaBar et al., 1998). According to LeDoux this procedure can only provide information on one of the two critical systems, namely it provides information on the system that leads to an adequate fearful response but it provides no information on the system that cognitively evaluates and generates the feeling of fear (LeDoux & Brown, 2017; Mobbs et al., 2019).
However, the role of the fear and anxiety circuits in generating panic is still not clear. Intuitively one might assume that an exaggerated fear-response is a neural correlate of anxiety and panic disorder. In fact, this presumption received support in fMRI studies with panic disorder patients. It was found in those patients that fear and anxiety related regions were hyper activated (de Carvalho et al., 2010a; Kircher et al., 2013). Kircher et al. described the influence of CBT on brain responses of patients with panic disorder during a fear conditioning experiment. Moreover, the study by Kircher et al. reported that successful CBT treatment is associated with activity-reduction in the fear and anxiety circuits. They described the influence of CBT on patients with panic disorder. Their pre–post comparison (t1 > t2) revealed a reduced activation in the amygdala, bilateral anterior insula, in parts of the cingulate cortices as well as in the inferior frontal gyrus (IFG) after successful CBT. Because the IFG is involved in the experience and cognitive regulation of emotions, the authors speculate that therapy could lower activation in fear and anxiety circuits that is caused by negative cognitions represented in frontal cortex. Another study on the impact of CBT found that successful treatment was related to an increase in right hippocampal activation and an inhibitory functional coupling between the anterior cingulate cortex and the amygdala (Lueken et al., 2013).
These findings imply that structurally intact fear-and-anxiety circuits are critically involved in the pathogenesis of panic disorder and may also constitute an essential precondition for the successful treatment of panic attacks. However, this conclusion is challenged by an interesting case report about a patient who developed panic attacks despite extensive, bilateral damage to the amygdalae (Wiest et al., 2006). Wiest and colleagues described the case of a patient who suffered from intense panic attacks at age 38 despite bilateral amygdala damage through Urbach-Wiethe disease since age 4. The patient had a normal emotional development and an appropriate range of mood and affect. Panic attacks occurred spontaneously without any identifiable external trigger. The patient also became depressive. The patient was treated with anti-depressive medication and both the symptoms of depression and frequency of panic attacks decreased. However, for this patient no attempts at psychotherapeutic treatment were reported. That intact amygdalae are not required for a panic attack was also shown by a study of Feinstein and colleagues who induced panic attacks in three patients with amygdala lesions (Feinstein et al., 2013). This view is supported by functional studies that found abnormal activation mainly in the brainstem, anterior and midcingulate cortex, insula, and lateral as well as medial parts of the prefrontal cortex (for a review see Sobanski & Wagner, 2017).
Thus, while it seems clear that panic disorders can arise in the absence of an intact fear and anxiety network, it is still unclear whether psychotherapeutic treatment will be successful under those conditions. This is the question that we wish to address in our current report.
The idea to offer CBT to patients with neurological impairment is not new but studies investigating its effectiveness for this patient group showed mixed results. CBT can be suitable for treating post-brain-injury depression, anxiety and emotional distress and is also applicable to different groups of patients with cognitive deficits (Bradbury et al., 2008; Exner et al., 2021; Gallagher et al., 2019; Hodgson et al., 2005; Khan-Bourne & Brown, 2003; Waldron et al., 2013). Although CBT can be effective after acquired brain injury, psychological distress could not be decreased in all cases (Hodgson et al., 2005; Rasquin et al., 2009) and even worsened in some (Lincoln & Flannaghan, 2003; Ramaratnam et al., 2008). However, altogether the evidence is encouraging: the majority of published studies report positive effects. Nevertheless, the specific question of whether an intact emotion-network is a critical precondition for successful CBT has not been answered by previous reports. Those previous studies used patient samples that were heterogenous with respect to the type of lesions (local or diffuse) and its causes (i.e. traumatic brain injury, tumor, hemorrhage or stroke). Thus, cases such as HZ, with defined lesions, affecting specifically the fear-network, are particularly interesting to shed more light on the preconditions for successful CBT.
The following two aims were pursued with the CBT of patient HZ: to help her manage life despite her partial emotional blunting and to reduce the frequency of panic attacks. The outcome suggests that both aims were achieved. However, we have to be cautious in our interpretation. Given the single-case nature of this report with its inherent lack of a control group it is impossible to rule out that the observed improvements were the result of spontaneous recovery. Nevertheless, the tight coupling between the observed improvement and therapy support a causal role of CBT in the observed recovery. Symptoms were largely stable prior to therapy but decreased significantly during therapy. It is also remarkable that those aspects of the disorder improved most that were the target of the treatment during the time of observed improvement.
The successful outcome in this patient raises an interesting question with respect to the role of the fear and anxiety circuits in the emergence and treatment of panic disorders. There seems to be a conflict between claims that assign an important role to the intact amygdala for the occurrence and treatability of panic disorders on the one hand and findings that suggest that such disorders can emerge and can be successfully treated despite damage to the amygdala.
One explanation would be that the relevant network for these processes is not really compromised in HZ. However, this account is implausible. While the damage in patient HZ is restricted to only one hemisphere, she displays nevertheless significant emotion-related impairments. In fact, as detailed above, some of her deficits are as pronounced as those found in patients with bilateral amygdala lesions.
Therefore, we favour a different explanation. Let’s assume the amygdala plays a critical role in assigning the correct emotion, that is, reacting fearful to appropriate situations but not in generating the fear-response itself. Under this assumption it is not surprising that following amygdala lesions fear and even panic responses are still present but assigned inappropriately. This is exactly what we observed in HZ. She seems relaxed in dangerous situations but developed panic in harmless settings. The question is whether the automatic assignment provided by the amygdala might be overruled or replaced by a more knowledge-driven, cognitive assignment process. The CBT applied in the case of HZ tested this possibility. HZ’s positive outcome suggests that a cognitive ability to assign appropriate emotions to given situations can be acquired. The success of CBT treatment also suggests that this ability is not reliant on an intact amygdala and that CBT provides a promising avenue to address emotion disorders also in other patients with damage to the brain’s emotion network.
This second explanation concurs with the view that the amygdala is setting the appropriate preconditions for emotion expression by “enhancing attention and associated perceptual encoding of emotional events” (Anderson, 2007; but see also Anderson & Phelps, 2002). It also concurs with the model of two systems regulating fear and anxiety responses, where the amygdala controls immediate fear response and the frontal areas are engaged when the conscious feeling arises (LeDoux & Pine, 2016).
Moreover, the fact that CBT can be effective despite damage to the amygdala suggests (tentatively given that HZ has still one intact amygdala) that effective control over the fear-response from frontal areas does not depend on intact amygdala system but that this frontal control can bypath the amygdala system. We suggest that a knowledge-based, cognitive system compensates for the more automatic, but compromised amygdala-based system and allows CBT to work also in patients with damage to the amygdala. Support for such an interpretation comes also from HZ who has good cognitive insight into her deficit (more on this issue below) and is now able to assess the objective danger of situations correctly even though this ability eluded her in the first months after surgery. Such a cognitive pathway to emotion control might also play an important role in CBT for brain-healthy patients. This is also suggested by neuroimaging studies showing how CBT impacts on the activity of posterior cingulate cortex, prefrontal medial cortex, ventral anterior cingulate cortex, pons and hippocampus but not the amygdala itself (Beutel et al., 2010; Kircher et al., 2013; Prasko et al., 2004; Sakai et al., 2006).
Apart from the theoretical implications, this report might be of clinical relevance. HZ’s case suggests a useful role for CBT in patients with amygdala lesions. This single case might also offer practical implications about how treatment should be adapted and for which patients such a treatment might be successfully applied. For the therapeutic treatment of anxiety, CBT guidelines recommend two steps: psychoeducation on fear responses and behaviour-emotion interaction. Building on this, gradual exposure is combined with relaxation training to practise the regulation of physiological arousal. These strategies were developed to achieve both the extinction of conditioned fear and the cognitive regulation of emotions. If therapists follow the guidelines for CBT when working with this special patient group, details such as frequency, the selection of exercises as well as documentation (if the patient has memory impairment) must be modified to the individual requirements of the patient. In our experience the following four points are useful to bear in mind: (1) basic neuropsychological knowledge is helpful for therapists and of particular importance to meet the specific concerns of this particular patient group. Apart from addressing behavior-emotion interactions, psychoeducation should focus on explaining the emotion regulatory circuits. Therapists need to address that these networks are partially disrupted by brain TLE surgery. Patients need to be informed that the current state of science does not yet offer conclusive answers on the recovery of cognitive and emotional processes after TLE surgery. However, studies on traumatic brain injury patients that benefit from CBT interventions are promising. (2) In TLE-surgery patients, memory function might be impaired due to lesions of hippocampal areas (Baxendale et al., 2006; Binder et al., 2010). In this case, therapist and patient should make use of external memory aids in the therapeutic progress, for example to minute the outcome for each therapeutic session (possibly even audiotape the entire session) and to write down exercises for the patient to practice at home. Patient HZ used a diary to keep track of her condition and any changes, which she brought to each session. (3) Therapy should aim at supporting the patient in coping and adjusting to new circumstances in everyday life. Patients might struggle to communicate their distress and needs with their families, partners or friends. In this case, therapists should help patients to find good ways to explain the patients’ psychological problems to friends and family and practice that type of communication with patients during their therapy sessions. For this part of the therapy, it might be helpful to invite relatives or friends to a session. As always, therapy should be resource oriented, focussing on helpful factors for recovery. For HZ it was helpful to remind her of her positive internal resources (her positive attitude or open-mindedness) and positive external resources (her supporting family and her work life). (4) It is important to first establish that the patient is aware of and able to evaluate his or her own emotional state, as CBT is relying on the introspective abilities of a patient. Good insight into one’s own psychological state is a key factor for successful therapy and influences the patient’s motivation (Lynch, 2012). The question of insight is of particular concern in the case of patients with amygdala lesions. Can such patients develop sufficient awareness for their own emotional state as is required for the successful implementation of CBT? Ammerlaan et al. (2008) investigated how emotion-perception impairments interfere with interpersonal behaviour in patients with amygdalohippocampectomy. While they found subtle impairments in recognition of fear and disgust, these deficits did not extend to the patients’ self-reports of social intercourse. The Scale for Interpersonal Behaviour (SIB) (Arrindell et al., 2001) was used as an index of the participants’ social behaviour and skills. As the SIB showed no group differences, the authors concluded that patients with amygdalohippocampectomy are unaware of their emotion recognition deficits and have only limited insight into their own mental states and their own behaviour (Ammerlaan et al., 2008). However, we observed a different behaviour in HZ. She was highly distressed by changes in emotional perception post-surgery and could describe the pre-post changes of her emotional experience with great precision. Interestingly, she was also able to evaluate situations as dangerous and predict a “normal” reaction and behaviour, while she herself could not experience the expected reaction. This suggests that lesions in the amygdala-hippocampal region do not necessarily results in patients having a lack of awareness for their own psychological problems or having reduced awareness of their own emotional state.
There are several case-dependent factors that had a positive impact on the outcome. Her very supporting family and intact social network, her positive and optimistic mind-set, her high motivation and her sense of self-responsibility were probably important facilitating factors during HZ’s therapy. Additionally, in learning to deal with the impairments HZ was sustained in her efforts by her conviction that the TLE surgery, despite causing new psychological problems, was an overall success. TLE surgery effectively cured her epilepsy and thus offered her the hope of a more normal life. Moreover, due to its abrupt post-surgery onset the emotional problems were clearly seen by both HZ and her clinicians as the consequence of the brain-surgery. This meant the pathological nature of those problems and the need to address was never in doubt. This contrasts with the more typical situation in brain-healthy patients suffering from panic disorders where symptoms develop slowly and no obvious trigger can be identified. Consequently, many patients struggle with the fact, that their emotional reaction seems irrational or pathological. Thus, paradoxically, in this respect patients with psychological problems following brain damage may sometimes be more open to therapy and thus more promising candidates for CBT than some brain-healthy patients.
Conclusion
To conclude, the case of patient HZ confirms that TLE surgery can lead to substantial changes in emotion processing and experience. Paradoxically it can also lead to heightened fears in inappropriate situations, leading to panic attacks. This case suggests standard CBT, customized to the specific resources and difficulties of the patient, as a valuable intervention for the growing number of TLE surgery patients who may show de-novo psychiatric impairments after surgery. Both the presence of panic attacks and the success of CBT therapy despite damage to the amygdala should prompt us to re-think the role of the amygdala in the pathogenesis and treatment of this disorder. Future research in form of group studies including functional neuroimaging is needed to further illuminate the cognitive, functional and neuronal mechanisms underlying effective psychotherapy in patients with damage to their emotion-regulating network.
References
Adolphs, R., Tranel, D., & Damasio, A. R. (2003). Dissociable neural systems for recognizing emotions. Brain and Cognition, 52(1), 61–69.
Adolphs, R., Tranel, D., Damasio, H., & Damasio, A. (1994). Impaired recognition of emotion in facial expressions following bilateral damage to the human amygdala. Nature, 372(6507), 669–672.
Adolphs, R., Tranel, D., Hamann, S., Young, A. W., Calder, A. J., Phelps, E. A., et al. (1999). Recognition of facial emotion in nine individuals with bilateral amygdala damage. Neuropsychologia, 37(10), 1111–1117.
Al-Otaibi, F., Baeesa, S. S., Parrent, A. G., Girvin, J. P., & Steven, D. (2012). Surgical techniques for the treatment of temporal lobe epilepsy. Epilepsy Research and Treatment.
American Psychiatric Association, D. S., & American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders: DSM-5 (Vol. 5). Washington, DC: American psychiatric association.
Ammerlaan, E. J., Hendriks, M. P., Colon, A. J., & Kessels, R. P. (2008). Emotion perception and interpersonal behavior in epilepsy patients after unilateral amygdalohippocampectomy. Acta Neurobiologiae Experimentalis, 68(2), 214–218.
Anderson, A. K. (2007). Feeling emotional: The amygdala links emotional perception and experience. Social Cognitive and Affective Neuroscience, 2(2), 71–72.
Anderson, A. K., & Phelps, E. A. (2002). Is the human amygdala critical for the subjective experience of emotion? Evidence of intact dispositional affect in patients with amygdala lesions. Journal of Cognitive Neuroscience, 14(5), 709–720.
Anhoury, S., Brown, R. J., Krishnamoorthy, E., & Trimble, M. R. (2000). Psychiatric outcome after temporal lobectomy: A predictive study. Epilepsia, 41(12), 1608–1615.
Arrindell, W. A., Bridges, K. R., Van der Ende, J., Lawrence, J. S. S., Gray-Shellberg, L., Harnish, R., et al. (2001). Normative studies with the Scale for Interpersonal Behaviour (SIB): II. US students: a cross-cultural comparison with Dutch data. Behaviour Research and Therapy, 39(12), 1461–1479.
Bandelow, B., Lichte, T., Rudolf, S., Wiltink, J., & Beutel, M. (Eds.). (2014). S3-Leitlinie Angststörungen. Springer.
Barrett, L. (2017). How Emotions Are Made. New York, Houghton Mifflin, Harcourt. Berridge KC, Kringelbach ML (2008) Affective neuroscience of pleasure: Reward in humans and animals. Psychopharmacology (Berlin), 199, 457–480.
Baxendale, S., Thompson, P., Harkness, W., & Duncan, J. (2006). Predicting memory decline following epilepsy surgery: A multivariate approach. Epilepsia, 47(11), 1887–1894.
Beck, A. T. (2002). Cognitive models of depression. Clinical Advances in Cognitive Psychotherapy: Theory and Application, 14(1), 29–61.
Beck, A. T., Sokol, L., Clark, D. A., Berchick, R., & Wright, F. (1992). A crossover study of focused cognitive therapy for panic disorder. The American Journal of Psychiatry.
Berridge, K. C., & Kringelbach, M. L. (2008). Affective neuroscience of pleasure: Reward in humans and animals. Psychopharmacology (berl), 199(3), 457–480.
Berridge, K. C., & Kringelbach, M. L. (2011). Building a neuroscience of pleasure and well-being. Psychology of Well-Being: Theory, Research and Practice, 1(1), 1–26.
Beutel, M. E., Stark, R., Pan, H., Silbersweig, D., & Dietrich, S. (2010). Changes of brain activation pre-post short-term psychodynamic inpatient psychotherapy: An fMRI study of panic disorder patients. Psychiatry Research: Neuroimaging, 184(2), 96–104.
Binder, J. R., Swanson, S. J., Sabsevitz, D. S., Hammeke, T. A., Raghavan, M., & Mueller, W. M. (2010). A comparison of two fMRI methods for predicting verbal memory decline after left temporal lobectomy: Language lateralization versus hippocampal activation asymmetry. Epilepsia, 51(4), 618–626.
Bornemann, B., Winkielman, P., & van der Meer, E. (2012). Can you feel what you do not see? Using internal feedback to detect briefly presented emotional stimuli. International Journal of Psychophysiology, 85(1), 116–124.
Bradbury, C. L., Christensen, B. K., Lau, M. A., Ruttan, L. A., Arundine, A. L., & Green, R. E. (2008). The efficacy of cognitive behavior therapy in the treatment of emotional distress after acquired brain injury. Archives of Physical Medicine and Rehabilitation, 89(12), S61–S68.
Brandt, C., Schoendienst, M., Trentowska, M., May, T. W., Pohlmann-Eden, B., Tuschen-Caffier, B., et al. (2010). Prevalence of anxiety disorders in patients with refractory focal epilepsy—A prospective clinic based survey. Epilepsy & Behavior, 17(2), 259–263.
Brierley, B., Medford, N., Shaw, P., & David, A. (2004). Emotional memory and perception in temporal lobectomy patients with amygdala damage. Journal of Neurology, Neurosurgery & Psychiatry, 75(4), 593–599.
Broks, P., Young, A. W., Maratos, E. J., Coffey, P. J., Calder, A. J., Isaac, C. L., et al. (1998). Face processing impairments after encephalitis: Amygdala damage and recognition of fear. Neuropsychologia, 36(1), 59–70.
Calder, A. J. (1996). Facial emotion recognition after bilateral amygdala damage: Differentially severe impairment of fear. Cognitive Neuropsychology, 13(5), 699–745.
Clark, D. M. (1986). A cognitive approach to panic. Behaviour Research and Therapy, 24(4), 461–470.
Cleary, R. A., Thompson, P. J., Fox, Z., & Foong, J. (2012). Predictors of psychiatric and seizure outcome following temporal lobe epilepsy surgery. Epilepsia, 53(10), 1705–1712.
Clum, G. A., Clum, G. A., & Surls, R. (1993). A meta-analysis of treatments for panic disorder. Journal of Consulting and Clinical Psychology, 61(2), 317.
Coplan, J. D., & Lydiard, R. B. (1998). Brain circuits in panic disorder. Biological Psychiatry, 44(12), 1264–1276.
de Araujo Filho, G. M., Rosa, V. P., Lin, K., Caboclo, L. O. S. F., Sakamoto, A. C., & Yacubian, E. M. T. (2008). Psychiatric comorbidity in epilepsy: A study comparing patients with mesial temporal sclerosis and juvenile myoclonic epilepsy. Epilepsy & Behavior, 13(1), 196–201.
de Carvalho, M. R., Dias, G. P., Cosci, F., de-Melo-Neto, V. L., Bevilaqua, M. C. N., Gardino, P. F., & Nardi, A. E. (2010). Current findings of fMRI in panic disorder: Contributions for the fear neurocircuitry and CBT effects. Expert Review of Neurotherapeutics, 10(2), 291–303.
de Carvalho, M. R., Rozenthal, M., & Nardi, A. E. (2010b). The fear circuitry in panic disorder and its modulation by cognitive-behaviour therapy interventions. The World Journal of Biological Psychiatry, 11(2–2), 188–198.
Dellacherie, D., Hasboun, D., Baulac, M., Belin, P., & Samson, S. (2011). Impaired recognition of fear in voices and reduced anxiety after unilateral temporal lobe resection. Neuropsychologia, 49(4), 618–629.
Devinsky, O. (2004). Diagnosis and treatment of temporal lobe epilepsy. Reviews in Neurological Diseases, 1(1), 2–9.
Devinsky, O., Barr, W., Vickrey, B., Berg, A., Bazil, C., Pacia, S., et al. (2005). Changes in depression and anxiety after resective surgery for epilepsy. Neurology, 65(11), 1744–1749.
Engel, J., McDermott, M. P., Wiebe, S., Langfitt, J. T., Stern, J. M., Dewar, S., et al. (2012). Early surgical therapy for drug-resistant temporal lobe epilepsy: A randomized trial. JAMA, 307(9), 922–930.
Erba, G., Moja, L., Beghi, E., Messina, P., & Pupillo, E. (2012). Barriers toward epilepsy surgery. A Survey among Practicing Neurologists. Epilepsia, 53(1), 35–43.
Etkin, A., & Wager, T. D. (2007). Functional neuroimaging of anxiety: A meta-analysis of emotional processing in PTSD, social anxiety disorder, and specific phobia. American Journal of Psychiatry, 164(10), 1476–1488.
Exner, C., Doering, B. K., Conrad, N., Künemund, A., Zwick, S., Kühl, K., et al. (2021). Integrated neuropsychological and cognitive behavioural therapy after acquired brain injury: A pragmatic randomized clinical trial. Neuropsychological Rehabilitation.
Feinstein, J. S., Adolphs, R., Damasio, A., & Tranel, D. (2011). The human amygdala and the induction and experience of fear. Current Biology, 21(1), 34–38.
Feinstein, J. S., Buzza, C., Hurlemann, R., Follmer, R. L., Dahdaleh, N. S., Coryell, W. H., et al. (2013). Fear and panic in humans with bilateral amygdala damage. Nature Neuroscience, 16(3), 270–272.
Feldker, K., Heitmann, C. Y., Neumeister, P., Bruchmann, M., Vibrans, L., Zwitserlood, P., & Straube, T. (2016). Brain responses to disorder-related visual threat in panic disorder. Human Brain Mapping, 37(12), 4439–4453.
Gallagher, M., McLeod, H. J., & McMillan, T. M. (2019). A systematic review of recommended modifications of CBT for people with cognitive impairments following brain injury. Neuropsychological Rehabilitation, 29(1), 1–21.
Gläscher, J., & Adolphs, R. (2003). Processing of the arousal of subliminal and supraliminal emotional stimuli by the human amygdala. Journal of Neuroscience, 23(32), 10274–10282.
Glosser, G., Zwil, A. S., Glosser, D. S., O’Connor, M. J., & Sperling, M. R. (2000). Psychiatric aspects of temporal lobe epilepsy before and after anterior temporal lobectomy. Journal of Neurology, Neurosurgery & Psychiatry, 68(1), 53–58.
Golouboff, N., Fiori, N., Delalande, O., Fohlen, M., Dellatolas, G., & Jambaqué, I. (2008). Impaired facial expression recognition in children with temporal lobe epilepsy: Impact of early seizure onset on fear recognition. Neuropsychologia, 46(5), 1415–1428.
Gorman, J. M., Kent, J. M., Sullivan, G. M., & Coplan, J. D. (2000). Neuroanatomical hypothesis of panic disorder, revised. American Journal of Psychiatry, 157(4), 493–505.
Gould, R. A., Ott, M. W., & Pollack, M. H. (1995). A meta-analysis of treatment outcome for panic disorder. Clinical Psychology Review, 15(8), 819–844.
Haby, M. M., Donnelly, M., Corry, J., & Vos, T. (2006). Cognitive behavioural therapy for depression, panic disorder and generalized anxiety disorder: A meta-regression of factors that may predict outcome. Australian & New Zealand Journal of Psychiatry, 40(1), 9–19.
Hagena, S., & Gebauer, M. (2014). Therapie-Tools Angststörungen. Belz Verlag.
Halley, S. A., Wrench, J. M., Reutens, D. C., & Wilson, S. J. (2010). The amygdala and anxiety after epilepsy surgery. Epilepsy & Behavior, 18(4), 431–436.
Heinrichs, N., Alpers, G. W., & Gerlach, A. L. (2009). Evidenzbasierte Leitlinie zur Psychotherapie der Panikstörung und Agoraphobie. Hogrefe Verlag.
Hermann, B. P., Seidenberg, M., Bell, B., Woodard, A., Rutecki, P., & Sheth, R. (2000). Comorbid psychiatric symptoms in temporal lobe epilepsy: Association with chronicity of epilepsy and impact on quality of life. Epilepsy & Behavior, 1(3), 184–190.
Hodgson, J., McDonald, S., Tate, R., & Gertler, P. (2005). A randomised controlled trial of a cognitive-behavioural therapy program for managing social anxiety after acquired brain injury. Brain Impairment, 6(3), 169.
Hoppenbrouwers, S. S., Bulten, B. H., & Brazil, I. A. (2016). Parsing fear: A reassessment of the evidence for fear deficits in psychopathy. Psychological Bulletin, 142(6), 573.
Inman, C. S., Bijanki, K. R., Bass, D. I., Gross, R. E., Hamann, S., & Willie, J. T. (2020). Human amygdala stimulation effects on emotion physiology and emotional experience. Neuropsychologia, 145, 106722.
Kanfer, F., Saslow, G., & Franks, C. (1969). Behavior therapy: Appraisal and status. McGraw-Hill.
Kanner, A. M. (2016). Management of psychiatric and neurological comorbidities in epilepsy. Nature Reviews Neurology, 12(2), 106.
Kennedy, S. H., Konarski, J. Z., Segal, Z. V., Lau, M. A., Bieling, P. J., McIntyre, R. S., & Mayberg, H. S. (2007). Differences in brain glucose metabolism between responders to CBT and venlafaxine in a 16-week randomized controlled trial. American Journal of Psychiatry, 164(5), 778–788.
Khan-Bourne, N., & Brown, R. (2003). Cognitive behaviour therapy for the treatment of depression in individuals with brain injury. Neuropsychological Rehabilitation, 13(1–2), 89–107.
Kircher, T., Arolt, V., Jansen, A., Pyka, M., Reinhardt, I., Kellermann, T., et al. (2013). Effect of cognitive-behavioral therapy on neural correlates of fear conditioning in panic disorder. Biological Psychiatry, 73(1), 93–101.
Kwan, P., & Brodie, M. J. (2000). Epilepsy after the first drug fails: Substitution or add-on? Seizure, 9(7), 464–468.
LaBar, K. S., Gatenby, J. C., Gore, J. C., LeDoux, J. E., & Phelps, E. A. (1998). Human amygdala activation during conditioned fear acquisition and extinction: A mixed-trial fMRI study. Neuron, 20(5), 937–945.
Lai, C.-H. (2011). Gray matter deficits in panic disorder: A pilot study of meta-analysis. Journal of Clinical Psychopharmacology, 31(3), 287–293.
Lang, P. J. (1969). The mechanics of desensitization and the laboratory study of human fear. Behavior therapy: Appraisal and status. New York: McGraw-Hill, 160–191.
LeDoux, J. E. (2020). Thoughtful feelings. Current Biology, 30(11), R619–R623.
LeDoux, J. E., & Brown, R. (2017). A higher-order theory of emotional consciousness. Proceedings of the National Academy of Sciences, 114(10), E2016–E2025.
LeDoux, J. E., & Pine, D. S. (2016). Using neuroscience to help understand fear and anxiety: A two-system framework. American Journal of Psychiatry, 173, 1083–1093.
LeDoux, K., & Gordon, B. (2011). Disruption of spelling-to-sound correspondence mapping during single-word reading in patients with temporal lobe epilepsy. Brain and Language, 118(1–2), 1–8.
Lilienfeld, S. O., Sauvigné, K. C., Reber, J., Watts, A. L., Hamann, S., Smith, S. F., et al. (2018). Potential effects of severe bilateral amygdala damage on psychopathic personality features: A case report. Personality Disorders: Theory, Research, and Treatment, 9(2), 112.
Lincoln, N., & Flannaghan, T. (2003). Cognitive behavioral psychotherapy for depression following stroke: A randomized controlled trial. Stroke, 34(1), 111–115.
Lueken, U., Straube, B., Konrad, C., Wittchen, H.-U., Ströhle, A., Wittmann, A., et al. (2013). Neural substrates of treatment response to cognitive-behavioral therapy in panic disorder with agoraphobia. American Journal of Psychiatry, 170(11), 1345–1355.
Lynch, M. M. (2012). Factors influencing successful psychotherapy outcomes. (Unpublished master’s thesis). University of St. Thomas, St. Paul, Minnesota.
Margraf, J., & Schneider, S. (2018). Lehrbuch der Verhaltenstherapie – Grundlagen, Diagnostik, Verfahren und Rahmenbedingungen psychologischer Therapie. Springer.
Massana, G., Serra-Grabulosa, J. M., Salgado-Pineda, P., Gastó, C., Junqué, C., Massana, J., et al. (2003). Amygdalar atrophy in panic disorder patients detected by volumetric magnetic resonance imaging. NeuroImage, 19(1), 80–90.
McIntosh, A. M., Kalnins, R. M., Mitchell, L. A., Fabinyi, G. C., Briellmann, R. S., & Berkovic, S. F. (2004). Temporal lobectomy: Long-term seizure outcome, late recurrence and risks for seizure recurrence. Brain, 127(9), 2018–2030.
McNally, R. J. (2007). Mechanisms of exposure therapy: How neuroscience can improve psychological treatments for anxiety disorders. Clinical Psychology Review, 27(6), 750–759.
Messina, I., Sambin, M., Palmieri, A., & Viviani, R. (2013). Neural correlates of psychotherapy in anxiety and depression: A meta-analysis. PloS one, 8(9), e74657.
Mobbs, D., Adolphs, R., Fanselow, M. S., Barrett, L. F., LeDoux, J. E., Ressler, K., & Tye, K. M. (2019). Viewpoints: Approaches to defining and investigating fear. Nature Neuroscience, 22(8), 1205–1216.
Mula, M., Pini, S., Preve, M., Masini, M., Giovannini, I., & Cassano, G. B. (2009). Clinical correlates of depersonalization symptoms in patients with bipolar disorder. Journal of Affective Disorders, 115(1–2), 252–256.
Öhman, A. (2005). The role of the amygdala in human fear: Automatic detection of threat. Psychoneuroendocrinology, 30(10), 953–958.
Otte, C. (2011). Cognitive behavioral therapy in anxiety disorders: Current state of the evidence. Dialogues in Clinical Neuroscience, 13(4), 413.
Ougrin, D. (2011). Efficacy of exposure versus cognitive therapy in anxiety disorders: Systematic review and meta-analysis. BMC Psychiatry, 11(1), 1–13.
Pintor, L., Bailles, E., Fernández-Egea, E., Sánchez-Gistau, V., Torres, X., Carreno, M., et al. (2007). Psychiatric disorders in temporal lobe epilepsy patients over the first year after surgical treatment. Seizure, 16(3), 218–225.
Pishnamazi, M., Tafakhori, A., Loloee, S., Modabbernia, A., Aghamollaii, V., Bahrami, B., & Winston, J. S. (2016). Attentional bias towards and away from fearful faces is modulated by developmental amygdala damage. Cortex, 81, 24–34.
Porto, P. R., Oliveira, L., Mari, J., Volchan, E., Figueira, I., & Ventura, P. (2009). Does cognitive behavioral therapy change the brain? A systematic review of neuroimaging in anxiety disorders. The Journal of Neuropsychiatry and Clinical Neurosciences, 21(2), 114–125.
Prasko, J., Horácek, J., Zalesky, R., Kopecek, M., Novak, T., Paskova, B., et al. (2004). The change of regional brain metabolism (18FDG PET) in panic disorder during the treatment with cognitive behavioral therapy or antidepressants. Neuroendocrinology Letters, 25(5), 340–348.
Ramaratnam, S., Baker, G. A., & Goldstein, L. H. (2008). Psychological treatments for epilepsy. Cochrane Database of Systematic Reviews.
Rasquin, S., Van De Sande, P., Praamstra, A., & Van Heugten, C. (2009). Cognitive-behavioural intervention for depression after stroke: Five single case studies on effects and feasibility. Neuropsychological Rehabilitation, 19(2), 208–222.
Reddemann, L. (2017). Imagination als heilsame Kraft (Vol. 5). Klett-Cotta.
Roffman, J. L., Marci, C. D., Glick, D. M., Dougherty, D. D., & Rauch, S. L. (2005). Neuroimaging and the functional neuroanatomy of psychotherapy. Psychological Medicine, 35(10), 1385–1398.
Sakai, Y., Kumano, H., Nishikawa, M., Sakano, Y., Kaiya, H., Imabayashi, E., et al. (2005). Cerebral glucose metabolism associated with a fear network in panic disorder. NeuroReport, 16(9), 927–931.
Sakai, Y., Kumano, H., Nishikawa, M., Sakano, Y., Kaiya, H., Imabayashi, E., et al. (2006). Changes in cerebral glucose utilization in patients with panic disorder treated with cognitive–behavioral therapy. NeuroImage, 33(1), 218–226.
Schuele, S. U., & Lüders, H. O. (2008). Intractable epilepsy: Management and therapeutic alternatives. The Lancet Neurology, 7(6), 514–524.
Sobanski, T., & Wagner, G. (2017). Functional neuroanatomy in panic disorder: Status quo of the research. World Journal of Psychiatry, 7(1), 12.
Spencer, S. S. (2002). When should temporal-lobe epilepsy be treated surgically? The Lancet Neurology, 1(6), 375–382.
Stinckens, N., Lietaer, G., & Leijssen, M. (2013). Working with the inner critic: Therapeutic approach. Person-Centered & Experiential Psychotherapies, 12(2), 141–156.
Sylvester, C. M., Corbetta, M., Raichle, M., Rodebaugh, T., Schlaggar, B., Sheline, Y., et al. (2012). Functional network dysfunction in anxiety and anxiety disorders. Trends in Neurosciences, 35(9), 527–535.
Taschereau-Dumouchel, V., Kawato, M., & Lau, H. (2020). Multivoxel pattern analysis reveals dissociations between subjective fear and its physiological correlates. Molecular Psychiatry, 25(10), 2342–2354.
Tranel, D., & Hyman, B. T. (1990). Neuropsychological correlates of bilateral amygdala damage. Archives of Neurology, 47(3), 349–355.
Waldron, B., Casserly, L. M., & O’Sullivan, C. (2013). Cognitive behavioural therapy for depression and anxiety in adults with acquired brain injury: What works for whom? Neuropsychological Rehabilitation, 23(1), 64–101.
Wiebe, S. (2000). Epidemiology of temporal lobe epilepsy. Canadian Journal of Neurological Sciences, 27(S1), S6–S10.
Wieser, H. G., Ortega, M., Friedman, A., & Yonekawa, Y. (2003). Long-term seizure outcomes following amygdalohippocampectomy. Journal of Neurosurgery, 98(4), 751–763.
Wiest, G., Lehner-Baumgartner, E., & Baumgartner, C. (2006). Panic attacks in an individual with bilateral selective lesions of the amygdala. Archives of Neurology, 63(12), 1798–1801.
Williamson, P., French, J., Thadani, V., Kim, J., Novelly, R., Spencer, S., et al. (1993). Characteristics of medial temporal lobe epilepsy: II. Interictal and ictal scalp electroencephalography, neuropsychological testing, neuroimaging, surgical results, and pathology. Annals of Neurology, 34(6), 781–787.
Wrench, J. M., Rayner, G., & Wilson, S. J. (2011). Profiling the evolution of depression after epilepsy surgery. Epilepsia, 52(5), 900–908.
Young, A., Perrett, D., Calder, A., Sprengelmeyer, R., & Ekman, P. (2002). Facial expressions of emotion: Stimuli and tests (FEEST). Thames Valley Test Company.
Zeman, A., Kapur, N., & Jones-Gotman, M. (2012). Epilepsy and memory. Oxford University Press.
Zhao, F., Kang, H., You, L., Rastogi, P., Venkatesh, D., & Chandra, M. (2014). Neuropsychological deficits in temporal lobe epilepsy: A comprehensive review. Annals of Indian Academy of Neurology, 17(4), 374.
Acknowledgements
We wish to thank HZ for her cooperation. This research was supported by grants from the German Research Foundation (Deutsche Forschungsgemeinschaft: DFG-SCHE 735/3-1; DFG-SCHE 735/3-2).
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Theresa Halder, Petra Michl, Virginia Flanagin and Thomas Schenk declare that they have no conflict of interest.
Informed Consent
The brain surgery was not part of this study and research, we therefore can not provide you with the informed consent concerning the brain surgery.
Animal rights
No animal studies were carried out by the authors for this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Halder, T., Michl, P., Flanagin, V. et al. Impaired Emotion Processing and Panic Disorder After Left Anterior Temporal Lobectomy: A Case Report of Successful Psychotherapeutic Intervention. Cogn Ther Res 46, 838–851 (2022). https://doi.org/10.1007/s10608-022-10301-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10608-022-10301-4