
Abstract
The UJA Covid-19 Jewish Impact Study constitutes a random sample of 4403 adults in Jewish households in the New York area. Collected between February and May 2021, the data include symptoms of depression and anxiety and the use of professional help. Via respondents’ zip code tabulation areas (ZCTAs), these data are linked to contextual measures of mental health care access from two data sources: the SAMHSA Locator on specialty community treatment clinics, and the Zip Code Business Patterns database on solo and small group practices. Both treatment facilities and office practices are added to multilevel logistic regression models as density rates (per 10,000 people) and as binary indicators of presence. While we find no meaningful relationship between the general presence of mental health care services and help-seeking behavior, the ZCTA-level density of office practices is significantly associated with service utilization among the socially isolated, foreign-born and Hispanics or non-white respondents.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Local mental health treatment infrastructure likely affects an individual’s likelihood to seek help, but the extent to which the availability of professional mental health services affects treatment utilization is still unclear, especially during the Covid-19 pandemic, when individuals are increasingly mentally burdened but are also seeking and finding more help online.
Association between people’s access to mental health care providers, either measured through distance (Fortney et al., 1999) or the general presence within a certain neighborhood or radius, and help-seeking behavior, is well documented. For instance, research dating back to the nineteenth century shows that there was an inverse relationship between distance to and use of mental hospitals (Jarvis, 1852). In the following years, this relationship was confirmed by other researchers, demonstrating that limited access to mental health care can impact people’s likelihood to seek help (S. Allard et al., 2003), to receive treatment, to experience successful treatment (McCarthy et al., 2007) and in the most severe cases, it can affect suicide rates resulting from mental health issues (Hung et al., 2020; Johnson & Brookover, 2020). Other studies have demonstrated that patients with access to free transportation services do not experience the negative effect of distance to providers (Whetten et al., 2006), pointing to the importance of local mental health care that is easy to reach.
In general, access to mental health services affects people in poverty the most since the mental health care density tends to be lower in less affluent areas (Ellis et al., 2009; Hendryx, 2008; Sharma et al., 2017). As researchers have pointed out, “we might expect such programs to be located farther away from higher-poverty areas in order to attract fee-paying clients. […] Access to outpatient mental health service providers is almost twice as great in low-poverty areas as in high- or extremely high-poverty areas” […] (Allard, 2009, p. 68). In addition, research has demonstrated that the “complexity of their physical and mental health problems, low reimbursement for Medicaid-insured populations, or no reimbursement for uninsured individuals” could be factors influencing the lower density of treatment in less affluent areas (Cook et al., 2017).
There are several ways in which access to local mental health care might impact individuals’ mental health outcomes and likelihood to seek help for symptoms of anxiety and depression (Allard et al., 2003). Individuals might not be willing to or able to commute to mental health care providers, especially if they have children, no access to transportation, inflexible job situations and other factors that might complicate such a commute. Furthermore, local outreach and information networks within communities are important factors that shape individuals’ likelihoods to seek and use help. In other words, limited mental health care infrastructure might mean less knowledge about where to find help and about mental health in general.
In trying to explain help-seeking behavior, most research has either focused on individual-level explanatory factors or taken a geographic perspective focusing on association at the neighborhood-, county- or state-level (Ellis et al., 2009; Goldsmith et al., 1997). Few studies (Cook et al., 2013; Cook et al., 2017; McCarthy et al., 2007) have integrated individual-level survey data with contextual mental health care information to understand how systematic barriers can influence individual behavior.
This study distinguishes itself by examining the relationship between individual help-seeking behavior and contextual access measured at a relatively low level of geography. Most importantly, given that the data were collected between February and May 2021, these recent data shed light on contextual effects of mental health care provider density during the Covid-19 pandemic, when strict measures such as lockdown and stay-at-home orders negatively impacted mental health and help-seeking behaviors, and aggravated socio-demographic disparities across different socio-economic groups. The Covid-19 pandemic is also a time when an increasing share of people rely on online psychological help, potentially rendering local access to mental health care less important or even obsolete. However, we hypothesize that the local mental health treatment infrastructure will still play a crucial role given that recent research has demonstrated older people and people in rural areas are significantly less likely to use telehealth services (most of which are mental health related) (Jaffe et al., 2020).
To our knowledge, this is also the first study that includes predictors for both.
-
(a)
specialty community MH treatment clinics, and
-
(b)
solo and small group mental health practices,
which serve different populations and purposes, and therefore should not be lumped together into one contextual measure of mental health care availability. In addition, we also offer a broader definition of mental health care availability: Instead of just relying on binary indicators of whether a ZCTA had any mental health care providers (Cummings et al., 2017) or just relying on standardized rates (Cook et al., 2017), we conduct separate analyses for these different measures. In this study, a dichotomous predictor points to the role of the general presence of mental health care providers in a ZCTA, while population-standardized mental health care rates refer to the role of provider density.
To sum up, we address the following research question: How is local mental health care infrastructure, measured through care density and presence of treatment clinics and small health practices, associated with individual help-seeking behavior?
Data and Methods
Data
To answer the research question, we merge three sets of data.
Covid-19 Jewish Impact Study
First, individual data come from the 2021 UJA Covid-19 Jewish Impact Study,Footnote 1 which constitutes a random sample of roughly 4400 Jewish and non-Jewish adults living in Jewish households in the New York region (five counties in New York City, Westchester, Nassau and Suffolk). The survey asked respondents about their current mental health and whether they were seeking help to deal with mental health problems. Among the few studies on help-seeking, some have demonstrated that treatment hesitancy and negative attitudes toward professional mental health treatment are more prevalent in Jewish communities (Schlosser et al., 2013). In general, the focus has been on the Orthodox Jewish population (Loewenthal, 2006; Pirutinsky et al., 2009; Schnitzer et al., 2011). For instance, Loewenthal’s (2006) research in England points to cultural and religious barriers that negatively impact the search and use of mental healthcare services, such as Jewish values, high levels of stigma, and concerns about violating Jewish religious law.
Mental Health Care Infrastructure
As a second step, we combine data from Substance Abuse and Mental Health Services Administration (SAMHSA) Behavioral Health Treatment Services Locator and 2019 Zip Code Business Patterns database, which provide information on the location of mental health service providers. The SAMHSA Locator provides a database of specialty mental health treatment facilities in the United States that is updated annually from facility responses to SAMHSA’s National Mental Health Services Survey (N-MHSS).Footnote 2 Moreover, new facilities meeting the survey qualifications are added monthly and facility information such as name, address and services provided has been updated on a weekly basis.Footnote 3 We downloaded the data from the SAMHSA Locator on June 25, 2021, and for this study, we mainly use the location of each facility as it is geocoded to the zip code level. Using the Missouri Census Data Center 2010 crosswalk file,Footnote 4 we aggregate the zip code level measures of mental health care resources into Zip code tabulation areas (ZCTAs), which are a preferable unit of analysis because they “are considerably smaller than counties, allowing for the examination of how mental health treatment resources are distributed across more local areas” (Cummings et al., 2017).
Since data from the SAMHSA Locator do not include small-group and solo practices but mainly focus on mental health clinics, we also include the most recent data from the 2019 Zip Code Business Patterns database, which is readily available at the zip-code level. These data include information on office-based physician and non-physician specialist like psychologists and psychiatrists. Again, we aggregate these data to the ZCTA level. This approach, using both data sources, has been shown to sufficiently cover mental health care access (Cummings et al., 2017).
As explained above, we choose a dual approach to assessing the effect of mental health care access on individual help-seeking behavior. In the first set of regression models, the main predictor is a dichotomous measure of whether there was at least one (a) mental health care facility and (b) at least one small-group or solo practice in a ZCTA. In the second set of models, we control for standardized provider density. These mental health care provider density rates are calculated using 2019 ACS 5-year-average population estimates in each ZCTA as the denominator, multiplied by 10,000, indicating the number of (a) mental health care facilities and (b) small-group or solo practices per 10,000 people in the neighborhood (Cook et al., 2017).
Dependent Variable
The UJA study contains information on symptoms of anxiety and depression rather than clinically diagnosed disorders, especially since it was not the primary objective of this study to monitor health-risk behaviors. The prevalence and severity of anxiety and depression symptoms are based on the Patient Health Questionnaire (PHQ-2) and Generalized Anxiety Disorder (GAD-2) questionnaires, which are short yet highly predictive measures of mental health (Hughes et al., 2018; Löwe et al., 2005). By focusing on four current symptoms (having little interest or pleasure in doing things; feeling down, depressed, or hopeless; feeling nervous, anxious, or on edge; not being able to stop or control worrying), individuals are included that “qualify” as showing symptoms of mental health issues but might not be aware of those symptoms as a mental illness. The questions refer to the past week, using a 4-point Likert scale (0 = Nearly every day, 1 = More than half the days, 2 = Several days, and 3 = Not at all). Reversing these scores, we calculate a total depression score using the first two symptoms and another total score for anxiety using the last two symptoms, respectively. Individuals scoring a total of 3 points or higher on either scale show symptoms of depression or anxiety.
Our main outcome variable, help-seeking, was assessed by asking “Have you sought professional help, or are you planning to seek professional help, for symptoms of depression or anxiety?”, with ‘yes’ and ‘no’ as response options. This dependent variable is included in the analysis in two ways (Table 1): the dataset contains information on help-seeking behavior for any respondent with an indication of mental health problems (anxiety and/or depression), leaving us with a sample size of 1360 responses (Sample 1). As a robustness check, we rerun the models relying only on those 765 respondents that “qualify” as having symptoms of depression and/or anxiety as described above and provide valid answers to the help seeking question (Sample 2). In other words, Sample 2 only includes respondents who had a combined anxiety or depression score that was higher than 3 points. As we can see below, respondents in Sample 2 had slightly higher rates of seeking help.
Independent Variables
Main Explanatory Variables
As explained above, our main independent variable is the availability of mental health services in a local ZCTA, which is measured using two types of mental health care services:
-
(1)
Specialty mental health treatment clinics, and
-
(2)
Solo and small group practices of mental health specialists—including psychiatrists and therapists.
These two represent the “two systems of mental health care” (Cummings et al., 2017), and they are operationalized in two ways. The first one is service density, reflecting the number of total service providers per 10,000 people in the neighborhood. In the second approach, we use a dichotomous measure of service presence instead.
As people are likely to search for health care beyond their residential neighborhoods, we also construct the service density and presence measures for their surrounding neighborhoods. Here, we use a contiguity-based approach and define neighbors (i.e., neighboring ZCTAs) for a focal zip code tabulation area as those ZCTAs that share at least a vertex with the focal neighborhood (Lloyd, 2010). For the service density measure, we sum up the total service providers and total population in the surrounding neighborhoods first and, relying on the same approach used for the focal neighborhood, calculate a standardized measure. For the service presence measure, the dichotomous variable indicates whether at least one service provider is present in the surrounding neighborhoods.
As Table 2 demonstrates, 66% of the survey respondents live in a neighborhood that has at least one specialty mental health treatment facility and 75% of them have at least one solo or small group practice in their neighborhood. On average, there are only 0.28 treatment facilities per 10,000 residents, while the rate for private practices is much higher at 3.11. Most respondents can also access treatment facilities (93%) or private services (90%) in their surrounding ZCTAs. The prevalence of treatment facilities in these surrounding neighborhoods (0.30 per 10,000 residents) is as high as it is in their residential neighborhood, though in the case of private practices, the rate is much lower (1.66 per 10,000 residents).
Other Socio-demographic Controls
The analysis also includes socio-demographic control variables that might influence the likelihood of an individual to seek help when struggling with a mental health problem.Footnote 5
When studying help-seeking behavior, controlling for the severity of anxiety or depression is an important prerequisite since people with stronger symptoms are more likely to seek help (Magaard et al., 2017; Rickwood & Braithwaite, 1994; Sherwood et al., 2007). In this paper, we add up individual depression and anxiety scores, with a higher value indicating more severe symptoms of anxiety or depression.
We also control for an urban/sub-urban divide in our study design. Research has shown that people living in less urban environments are more reluctant to seek care due to more stigmatized attitudes (Hoyt et al., 1997) and lack of access (Ellis et al., 2009).
Much research has focused on how gender influences people’s propensity to seek professional help for mental health problems. Overall, studies seem to agree that women are more likely to seek help when compared to their male counterparts (Biddle et al., 2004; Eisenberg et al., 2009; Goldsmith et al., 1997; Oliver et al., 2005), often pointing to a large number of barriers that prevent men from seeking and accessing the help they need (Doherty & Kartalova-O’Doherty, 2010). Studies have also documented the relationship between age and usage of professional mental health services. In an analysis of 17 different datasets, about half of the datasets showed a significant association between the likelihood to seek help and age (Magaard et al., 2017; Tijhuis et al., 1990), even though the relationship pointed in different directions. Some studies show that younger people are more likely to seek help for mental problems (Mackenzie et al., 2008), while other studies show that middle-aged or older respondents are seeking help at higher rates (Biddle et al., 2004; Oliver et al., 2005) and it is the young who are most reluctant and hard-to-reach when it comes to mental health issues (Aguirre Velasco et al., 2020). Race has also been found to affect the individual propensity to find help. Several studies have shown that, in comparison to white respondents, non-whites were less likely to seek help when facing mental health challenges. In particular, black (Snowden, 1998; Taylor & Kuo, 2019; Woodward, 2011) and Asian individuals (Kim & Zane, 2016; Masuda et al., 2009) have been shown to seek needed help at much lower rates than their white counterparts. These findings have also been closely linked to nativity; in general, immigrants to the U.S. have been shown to access help at lower rates than native born Americans (Abe-Kim et al., 2007; Na et al., 2016; Shin, 2002).
Socio-economic status, which we control for as education and poverty in this paper, has been shown to be another important factor in influencing the use of mental health related services. After controlling for other socio-demographic and situational factors, individuals with higher levels of education were more likely to seek help, especially in the U.S. and Canada (Magaard et al., 2017; Tijhuis et al., 1990). Poverty is another factor influencing mental health care access (Ellis et al., 2009). Studies have even demonstrated that the poverty effect can be so strong that it “explains away” any observed differences in race and ethnicity when it comes to help-seeking and might be the actual underlying reason for differential help-seeking behavior (Chow et al., 2003).
Finally, we control for social connection, measured by including marital status and social network size. While we do not find any direct evidence in the literature suggesting that marital status influences the use of mental health services, social support and family ties have been shown to promote better health behaviors (Umberson, 1987). In addition, being embedded in bigger social circles has been shown to affect help-seeking behavior (Horwitz, 1978; Kawachi & Berkman, 2001).
Statistical Analysis
-
a.
Descriptive statistics are computed to describe the outcome variable and the independent variables.
-
b.
Next, two sets of multilevel logistic regression modelsFootnote 6 are constructed to estimate the association between seeking professional mental help and access to care (measured through service density and presence), controlling for age, race/ethnicity, gender, nativity, education and poverty status, and social connections. In the first set of models, the dichotomized dependent variable is the willingness to seek help for mental health when facing symptoms of depression and anxiety for any respondent who indicated at any point having little interest or pleasure in doing things, feeling down, depressed, or hopeless, feeling nervous, anxious, or on edge, or not being able to stop or control worrying. In the second set of models, the analysis is redone relying only on respondents that qualified as having a symptom of anxiety or depression based on the PHQ-2 or GAD-2 guidelines.
Results of the multivariate logistic regression models are expressed as adjusted odds ratio (OR) with a 95% confidence interval (CI); p-values < 0.05 are considered statistically significant, though we identify results significant at 0.1 level.
Finally, to control for the spatial spillover effect from neighboring ZCTAs, we include the service density and presence measures in the surrounding neighborhoods of a focal zip code tabulation area.
Results
As we can see from Map 1 and 2 below, treatment facilities and private practices offering professional mental health care are not equally distributed across the New York area under study. In general, specialty mental health treatment facilities (Map 1) are more equally distributed when compared to solo and small group practices of mental health specialists (Map 2). Still, standardized rates of treatment facilities are higher in the city, when compared to more suburban areas. In Map 2, we see that small practice density rates are among the highest in Manhattan.

Treatment facility density in 8-County New York Area

Private practice density in 8-County New York Area
Descriptive Statistics
Unweighted descriptive statistics are used to explore sample characteristics including all variables used in the models below. As pointed out before, 46 percent of respondents with symptoms of anxiety or depression had sought help or were planning to seek help. For this sample, the total anxiety/depression score ranges from 3 to 12, with the average being 5.3. While age is evenly distributed, the sample skews slightly female (63 percent). Roughly 90 percent of respondents are non-Hispanic white, and the remaining 10 percent are Hispanic, non-Hispanic Asian, non-Hispanic black, or other. 18 percent of the sample indicated they were foreign-born. In terms of socio-economic status, 11 percent of respondents are poor and there is a relatively high share with at least a bachelor’s degree (83 percent). Most respondents had at least three friends, and 45 percent were married (Table 3).
Multilevel Logistic Regression Model Results
Finally, we run multivariate logistic regression models to estimate the link between help seeking and access to care, while controlling for a host of socio-demographic and situation variables hypothesized to influence help-seeking. Odds ratios (OR) and significance are checked for model-building. While there is no general agreement on how to measure model fit, the McKelvey & Zavoina Pseudo R-squared is found to be the most appropriate in evaluating the goodness of fit of the multivariate logistic models (Langer, 2017). We have tried to find the most straight-forward model which could explain as much variance as possible and kept theoretically important independent variables at significance level below 0.05.
For each model, respondents living in ZCTAs with a higher provider density would be expected to be more likely to access services, all things being equal. To test this hypothesis, we construct four different models. Model 1 only includes individual-level controls (total anxiety and depression score, gender, age, education, race/ethnicity, nativity, poverty, marital status, urban/rural status, and social connectedness). Combining an individual’s probability of seeking help with their nativity, race/ethnicity and level of social connectedness, creates an interaction term that is included in Models 2–4 to discern whether access differentially impacts service utilization for these three groups. Model 2 includes interaction effects for foreign-born respondents, Model 3 focuses on Hispanic or non-white respondents, and Model 4 interacts social ties (number of friends, family and neighbors to rely on) with access.
Prior to the discussion of the different model outcomes, we discuss the different decisions that are made with regards to model design:
-
(a)
We run two different model versions relying on 1360 responses (Sample 1) and 765 respondents (Sample 2) depending on whether they “qualify” as having symptoms of depression and/or anxiety based on PHQ-2 and GAD-2 standards. Since results based on Sample 2 are not statistically significant, we only report the major findings for Sample 1. After deleting 42 cases with missing values on the independent variables, we include 1318 cases in the final analysis.
-
(b)
We control for spatial spillover effects and do not find these to be significant. These controls are therefore not included in the findings below.
-
(c)
As discussed above, we propose both running models using a dichotomous measure of service presence, and an alternative model controlling for service density, reflecting the number of total service providers per 10,000 people in the neighborhood. All models below do not show a significant relationship for service presence and therefore, these results are not included. Instead, Models 2–4 rely on service density as the main predictor. We conclude that density is a better measure as it offers more variability, especially in a context where most respondents live in areas that have access to a mental health care provider. Density is also more sensitive to the level of access a respondent has in their neighborhood.
-
(d)
Finally, we conduct separate analyses for the two kinds of mental health service providers: specialty mental health treatment facilities, and solo and small group practices of mental health specialists (psychiatrists, therapists, etc.). The models below only include findings for small private practices, since mental health treatment clinics do not show a significant relationship to the outcome for both density and presence measures. This could be partially explained by the fact that people are more likely to seek private services for their mental health issues.Footnote 7
The first model (Table 4) shows the relationship between help seeking and a range of sociodemographic controls. Not surprisingly, the overall level of mental problems measured by a total anxiety/depression score is highly predictive of help seeking; people who struggle more with their psychological health search for help at higher levels when compared to people who struggle less. Neither age nor gender show significant relationships with the outcome. The same holds true for poverty and urban/suburban status. Consistent with prior studies, our findings show that foreign-born respondents were significantly less likely than whites to seek help. While bivariate disparities in service utilization also exist for non-Hispanic whites and their diverse counterparts, those differences seem to be “explained away” by the other socio-demographic controls. In line with past research, married respondents were less likely to seek help when compared to single, divorced, separated, or widowed adults. Finally, we account for social network size (measured by the number of relatives, friends, or neighbors respondents can call on for help) and find this to be an important factor in shaping help seeking behavior: relative to the isolated (those with no or few social ties), respondents with bigger social circles are more likely to seek mental health help. Most of these individual-level relationships hold across Models 1–4, irrespective of whether access to mental health service is included in the analysis. The McKelvey & Zavoina R2 value of 0.207 shows that roughly 21% of the variance in professional help seeking for a mental health problem was explained by this model.
Controlling for all socio-demographic factors included in Model 1, the second model (R2 = 0.216) considers the relationship between mental health care utilization and density of mental health service providers including interaction effects for foreign-born respondents. While the ZCTA-level number of private services per 10,000 residents overall is not significant for native-born adults, an increase in service density by one unit of measure increases the odds of seeking help by a factor of 1.2 among the foreign-born.
Similar to Model 2, higher mental health care density is a strong predictor of help seeking for Hispanic or non-white respondents in Model 3 (OR 1.266, p < 0.01). In contrast to non-Hispanic whites, Hispanics or non-whites were more likely to seek help as the number of small and solo mental health care practices increased in each neighborhood.
Model 4 shows that, for the isolated, service density is also a significant predictor of professional help-seeking. As a reminder, we measured the size of social networks by asking respondents to provide the number of family members, friends and neighbors they could rely on in times of need. Taking service density out of the equation, bigger social networks are associated with more help-seeking. Including an interaction effect for density and social ties, however, shows that the isolated benefit the most from a larger number of private services per 10,000 in ZCTA: as density increases, those with 3–4, 5–9 and more than 10 social ties are less likely (OR 0.8) to seek help, compared to those with just few social ties (0–2 social ties).
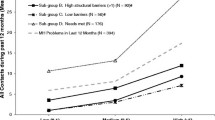
Figures 1, 2 and 3 show the predicted probabilities of seeking help by service density in each ZCTA. Controlling for overall mental health status and socio-demographic variables, Fig. 1 depicts a strong density effect for foreign-born adults. Foreign-born respondents in ZCTAs with no small or solo practices had a likelihood of around 20 percent to utilize professional help, compared to roughly 80 percent among those foreign-born respondents with 20 practices in their neighborhood. A similar pattern can be observed for Hispanic or non-white respondents (Fig. 2), where we see an almost logarithmic relationship. The benefit of increased service density is particularly strong in neighborhoods with lower levels of density. Only a third of respondents with 0–2 close social ties in areas with no small or solo practices were likely to seek help, versus almost three quarters of respondents in areas with very high practice density (Fig. 3).

Predicted probabilities of seeking help by mental health care density, among native-born and foreign-born population (based on postestimation results of Model 2)

Predicted probabilities of seeking help by mental health care density, among non-Hispanic whites and Hispanics or non-whites (based on postestimation results of Model 3)

Predicted probabilities of seeking help by mental health care density, for different levels of social connection (based on postestimation results of Model 4)
Discussion
Our findings demonstrate that almost half of respondents do not seek professional help when experiencing psychological distress. The main goal of this paper is understanding how access to help predicts help seeking for self-reported mental health problems. This cross-sectional analysis of help seeking behavior through a services access perspective reveals findings that are relevant for policy makers and planners, professional therapists, and counselors. We show that for some of the most vulnerable groups in society, place matters with regards to mental health care service utilization and help seeking is not only impacted by individual-level factors such as the severity of mental health problem and socio-demographic characteristics, but also by the contextual environment.
Higher service provider density overall, whether in the residential neighborhood or surrounding neighborhoods, is not associated with overall help-seeking behavior, all things being equal. Instead, our findings demonstrate that the neighborhood-level density of solo and small group practices of mental health specialists is an important determinant of service utilization among those with few or no social ties, the foreign-born and Hispanics or non-white respondents. The multilevel analyses (Models 2–4) suggest that when accounting for individual characteristics introduced in Model 1, isolated, foreign-born, and Hispanic/non-white respondents with more access to private practices were more likely to utilize mental health services when compared to respondents living in areas with low service density. This relationship is particularly striking for the foreign-born, who are significantly less likely to utilize mental health care services overall but respond positively to higher levels of and therefore easier access to mental health care practices when compared to their native-born counterparts.
As pointed out before, the Covid-19 pandemic led an increasing share of people to rely on online mental help. Our findings, especially as they pertain to the isolated, foreign-born, and Hispanic/non-white respondents, show the important role physical and local access to mental health care still plays. Further research is needed to discern whether local access overall does not play a role for other population groups due to the increased reliance on telehealth.
While we controlled for both mental health care density and the presence of treatment clinics and small health practices, we only found density to be significantly related to the outcome. We argue that a dichotomous measure of presence is not sufficient, given that this analysis was conducted at the ZCTA-level. In New York City, the largest ZCTAs are inhabited by more than 100,000 people; in such an instance, a binary measure of mere presence does not suffice. Density measures are sensitive to population size and therefore preferable.
In addition, several socio-demographic factors were included in all models to capture individual-level characteristics that could impact service utilization. We include age, race/ethnicity, gender, nativity, education, poverty status, and social ties. Unsurprisingly, overall mental health status strongly impacts the likelihood of seeking help. Furthermore, nativity, marital status, and social network size are predictive of help seeking. To improve access to care for people with symptoms of anxiety or depression, policy makers and health clinicians need to continue to focus efforts on individual-level factors associated with help seeking.
This study has several limitations. First and foremost, our analysis takes place at the ZCTA-level due to limited information on respondents’ address. Most scholars, who study contextual effects, recognize that the use of administratively drawn boundaries, such as ZCTAs, is limited but use these boundaries out of necessity. Future research could examine the role of care access in shaping help seeking using more individualized measures of context. While non-overlapping territorial boundaries are usually administratively defined, overlapping egocentric neighborhoods could be used to depict the individual’s living environment more realistically.
Second, due to the cross-sectional study design, we cannot assume this relationship is causal; instead, this study provides evidence that an increase in mental health care density is associated with increased help seeking for the groups discussed above. Further experimental or quasi-experimental research is needed to confirm this finding.
Finally, the data from the UJA Covid-19 Impact Study mainly focus on adults in Jewish households in the New York 8-county area, including both Jewish and non-Jewish respondents. We still believe that the findings from this study provide important contributions to the debate around access to mental health care during the pandemic. The Jewish population covered in this study is highly diverse in terms of gender identity and sexual orientation, place of birth, race and ethnicity, socio-economic background and the level of commitment and identification with Judaism, and therefore offers an interesting study “object”. In addition, the 2011 UJA demographic studyFootnote 8 shows that the population in NY Jewish households is large (roughly 1.54 million residents) and constitutes a large share of the general population: 16 percent of all households in the eight-county New York area are Jewish. Given the size, share, and diversity of the population studied in this random sample, the UJA Covid-19 Impact Study provides an important study context. The importance of local private practice density suggests that mental health care providers, social workers, neighborhood organizations and other groups seeking to promote the use of mental health care services need to focus on areas with low provider density. In areas with low levels of provider density, individuals in need of mental health care should be directed to nearby available services through outreach efforts. The research findings here also call for policy to increase mental health care access, in particular in areas with high concentration of foreign-born, Hispanic or non-white and socially isolated people. This is even more important when we consider that based on prior research (Johnson & Brookover, 2020), vulnerable populations are often affected the most by lack of mental health care access as they tend to live in underserved areas. Because our research finds no effect for community treatment clinics, and only shows a significant relationship for solo and small group practices of mental health specialists, this is even more important: Cummings et al. (2017) demonstrate that smaller practices—including therapists and psychiatrists—are often situated in higher income communities. Not only are vulnerable populations underserved, but our findings also demonstrate that they benefit most from access. In addition, there’s a myriad of research showing that stigma surrounding mental illness is a major reason for not seeking help, especially in non-white and foreign-born communities. A higher density and visibility of mental health practices could thus alleviate some of this stigma and increase acceptance of psychological problems overall.
Notes
See https://www.samhsa.gov/data/data-we-collect/n-mhss-national-mental-health-services-survey. The most recent one was conducted in 2019.
It should be noted that we wanted to account for whether respondents had access to insurance; most study respondents were covered by insurance, which is why this variable is not included. We also exclude denomination as it is not significantly associated with the outcome variable.
To accommodate the hierarchical structure of the survey data as well as its sampling design, we use the “melogit” command in Stata (16.1) to fit these models.
94% of respondents who sought or are planning to seek help in the UJA survey report private services as the most common option they would like to take.
References
Abe-Kim, J., Takeuchi, D. T., Hong, S., Zane, N., Sue, S., Spencer, M. S., Appel, H., Nicdao, E., & Alegría, M. (2007). Use of mental health-related services among immigrant and US-born Asian Americans: Results from the National Latino and Asian American Study. American Journal of Public Health, 97(1), 91–98. https://doi.org/10.2105/AJPH.2006.098541
Aguirre Velasco, A., Cruz, I. S. S., Billings, J., Jimenez, M., & Rowe, S. (2020). What are the barriers, facilitators and interventions targeting help-seeking behaviours for common mental health problems in adolescents? A systematic review. BMC Psychiatry, 20(1), 293. https://doi.org/10.1186/s12888-020-02659-0
Allard, S., Tolman, R., & Rosen, D. (2003). Proximity to service providers and service utilization among welfare recipients: The interaction of place and race. Journal of Policy Analysis and Management: the Journal of the Association for Public Policy Analysis and Management, 22, 599–613. https://doi.org/10.1002/pam.10157
Allard, S. W. (2009). Out of reach: Place, poverty, and the New American welfare state. Yale University Press.
Biddle, L., Gunnell, D., Sharp, D., & Donovan, J. L. (2004). Factors influencing help seeking in mentally distressed young adults: A cross-sectional survey. British Journal of General Practice, 54(501), 248–253.
Chow, J.C.-C., Jaffee, K., & Snowden, L. (2003). Racial/ethnic disparities in the use of mental health services in poverty areas. American Journal of Public Health, 93(5), 792–797.
Cook, B. L., Doksum, T., Chen, C. N., Carle, A., & Alegría, M. (2013). The role of provider supply and organization in reducing racial/ethnic disparities in mental health care in the US. Social Science & Medicine, 84, 102–109.
Cook, B. L., Zuvekas, S. H., Chen, J., Progovac, A., & Lincoln, A. K. (2017). Assessing the individual, neighborhood, and policy predictors of disparities in mental health care. Medical Care Research and Review, 74(4), 404–430. https://doi.org/10.1177/1077558716646898
Cummings, J. R., Allen, L., Clennon, J., Ji, X., & Druss, B. G. (2017). Geographic access to specialty mental health care across high- and low-income US communities. JAMA Psychiatry, 74(5), 476–484. https://doi.org/10.1001/jamapsychiatry.2017.0303
Doherty, D. T., & Kartalova-O’Doherty, Y. (2010). Gender and self-reported mental health problems: Predictors of help seeking from a general practitioner. British Journal of Health Psychology, 15(1), 213–228. https://doi.org/10.1348/135910709X457423
Eisenberg, D., Downs, M. F., Golberstein, E., & Zivin, K. (2009). Stigma and help seeking for mental health among college students. Medical Care Research and Review, 66(5), 522–541. https://doi.org/10.1177/1077558709335173
Ellis, A. R., Konrad, T. R., Thomas, K. C., & Morrissey, J. P. (2009). County-level estimates of mental health professional supply in the United States. Psychiatric Services (Washington, D.C.), 60(10), 1315–1322. https://doi.org/10.1176/ps.2009.60.10.1315
Fortney, J., Rost, K., Zhang, M., & Warren, J. (1999). The impact of geographic accessibility on the intensity and quality of depression treatment. Medical Care, 37(9), 884–893. https://doi.org/10.1097/00005650-199909000-00005
Goldsmith, H. F., Wagenfeld, M. O., Manderscheid, R. W., & Stiles, D. (1997). Specialty mental health services in metropolitan and nonmetropolitan areas: 1983 and 1990. Administration and Policy in Mental Health, 24(6), 475–488. https://doi.org/10.1007/BF02042826
Hendryx, M. (2008). mental health professional shortage areas in rural Appalachia. The Journal of Rural Health, 24(2), 179–182. https://doi.org/10.1111/j.1748-0361.2008.00155.x
Horwitz, A. (1978). Family, kin, and friend networks in psychiatric help-seeking. Social Science & Medicine. Part a: Medical Psychology & Medical Sociology, 12, 297–304. https://doi.org/10.1016/0271-7123(78)90069-X
Hoyt, D. R., Conger, R. D., Valde, J. G., & Weihs, K. (1997). Psychological distress and help seeking in rural America. American Journal of Community Psychology, 25(4), 449–470. https://doi.org/10.1023/A:1024655521619
Hughes, A. J., Dunn, K. M., Chaffee, T., Bhattarai, J., & Beier, M. (2018). Diagnostic and clinical utility of the GAD-2 for screening anxiety symptoms in individuals with multiple sclerosis. Archives of Physical Medicine and Rehabilitation, 99(10), 2045–2049. https://doi.org/10.1016/j.apmr.2018.05.029
Hung, P., Busch, S. H., Shih, Y.-W., McGregor, A. J., & Wang, S. (2020). Changes in community mental health services availability and suicide mortality in the US: A retrospective study. BMC Psychiatry, 20(1), 188. https://doi.org/10.1186/s12888-020-02607-y
Jaffe, D. H., Lee, L., Huynh, S., & Haskell, T. P. (2020). Health inequalities in the use of Telehealth in the United States in the lens of COVID-19. Population Health Management, 23(5), 368–377. https://doi.org/10.1089/pop.2020.0186
Jarvis, E. (1852). On the supposed increase of insanity. American Journal of Psychiatry, 8(4), 333–364. https://doi.org/10.1176/ajp.8.4.333
Johnson, K. F., & Brookover, D. L. (2020). Counselors’ role in decreasing suicide in mental health professional shortage areas in the United States. Journal of Mental Health Counseling, 42(2), 170–186. https://doi.org/10.17744/mehc.42.2.06
Kawachi, I., & Berkman, L. F. (2001). Social ties and mental health. Journal of Urban Health: Bulletin of the New York Academy of Medicine, 78(3), 458–467. https://doi.org/10.1093/jurban/78.3.458
Kim, J. E., & Zane, N. (2016). Help-seeking intentions among Asian American and White American students in psychological distress: Application of the health belief model. Cultural Diversity and Ethnic Minority Psychology, 22(3), 311–321. https://doi.org/10.1037/cdp0000056
Langer, W. (2017). How to assess the fit of multilevel logit models with Stata? German Stata Users’ Group Meetings, 2017, 05.
Lloyd, C. (2010). Spatial data analysis: An introduction for GIS users. Oxford University Press.
Loewenthal, K. (2006). Strictly orthodox Jews and their relations with psychotherapy and psychiatry.
Löwe, B., Kroenke, K., & Gräfe, K. (2005). Detecting and monitoring depression with a two-item questionnaire (PHQ-2). Journal of Psychosomatic Research, 58, 163–171. https://doi.org/10.1016/j.jpsychores.2004.09.006
Mackenzie, C. S., Scott, T., Mather, A., & Sareen, J. (2008). Older adults’ help-seeking attitudes and treatment beliefs concerning mental health problems. The American Journal of Geriatric Psychiatry, 16(12), 1010–1019. https://doi.org/10.1097/JGP.0b013e31818cd3be
Magaard, J. L., Seeralan, T., Schulz, H., & Brütt, A. L. (2017). Factors associated with help-seeking behaviour among individuals with major depression: A systematic review. PLoS ONE, 12(5), e0176730. https://doi.org/10.1371/journal.pone.0176730
Masuda, A., Anderson, P. L., Twohig, M. P., Feinstein, A. B., Chou, Y.-Y., Wendell, J. W., & Stormo, A. R. (2009). Help-seeking experiences and attitudes among African American, Asian American, and European American college students. International Journal for the Advancement of Counselling, 31(3), 168–180. https://doi.org/10.1007/s10447-009-9076-2
McCarthy, J. F., Blow, F. C., Valenstein, M., Fischer, E. P., Owen, R. R., Barry, K. L., Hudson, T. J., & Ignacio, R. V. (2007). Veterans affairs health system and mental health treatment retention among patients with serious mental illness: Evaluating accessibility and availability barriers. Health Services Research, 42(3 Pt 1), 1042–1060. https://doi.org/10.1111/j.1475-6773.2006.00642.x
Na, S., Ryder, A. G., & Kirmayer, L. J. (2016). Toward a culturally responsive model of mental health literacy: Facilitating help-seeking among East Asian immigrants to North America. American Journal of Community Psychology, 58(1–2), 211–225. https://doi.org/10.1002/ajcp.12085
Oliver, M. I., Pearson, N., Coe, N., & Gunnell, D. (2005). Help-seeking behaviour in men and women with common mental health problems: Cross-sectional study. The British Journal of Psychiatry, 186(4), 297–301. https://doi.org/10.1192/bjp.186.4.297
Pirutinsky, S., Rosmarin, D. H., & Pargament, K. I. (2009). Community attitudes towards culture-influenced mental illness: Scrupulosity vs. nonreligious OCD among orthodox jews. Journal of Community Psychology, 37(8), 949–958. https://doi.org/10.1002/jcop.20341
Rickwood, D. J., & Braithwaite, V. A. (1994). Social-psychological factors affecting help-seeking for emotional problems. Social Science & Medicine, 39(4), 563–572. https://doi.org/10.1016/0277-9536(94)90099-X
Schlosser, L. Z., Safran, R. S., Suson, R. A., Dettle, K., & Dewey, J. J. H. (2013). The assessment, diagnosis, and treatment of mental disorders among American jews. In F. A. Paniagua, & A.-M. Yamada (Eds.), Handbook of multicultural mental health (pp. 347–366). Academic Press.
Schnitzer, G., Loots, G., Escudero, V., & Schechter, I. (2011). Negotiating the pathways into care in a globalizing world: Help-seeking behaviour of ultra-orthodox jewish parents. International Journal of Social Psychiatry, 57(2), 153–165. https://doi.org/10.1177/0020764009105291
Sharma, R. N., Casas, R. N., Crawford, N. M., & Mills, L. N. (2017). Geographic distribution of California mental health professionals in relation to sociodemographic characteristics. Cultural Diversity and Ethnic Minority Psychology, 23(4), 595–600. https://doi.org/10.1037/cdp0000147
Sherwood, C., Salkovskis, P. M., & Rimes, K. A. (2007). Help-seeking for depression: The role of beliefs, attitudes and mood. Behavioural and Cognitive Psychotherapy, 35(5), 541–554. https://doi.org/10.1017/S1352465807003815
Shin, J. K. (2002). Help-seeking behaviors by Korean immigrants for depression. Issues in Mental Health Nursing, 23(5), 461–476. https://doi.org/10.1080/01612840290052640
Snowden, L. R. (1998). Racial differences in informal help seeking for mental health problems. Journal of Community Psychology, 26(5), 429–438. https://doi.org/10.1002/(SICI)1520-6629(199809)26:5%3c429::AID-JCOP3%3e3.0.CO;2-M
Taylor, R. E., & Kuo, B. C. H. (2019). Black American psychological help-seeking intention: An integrated literature review with recommendations for clinical practice. Journal of Psychotherapy Integration, 29(4), 325–337. https://doi.org/10.1037/int0000131
Tijhuis, M. A., Peters, L., & Foets, M. (1990). An orientation toward help-seeking for emotional problems. Social Science & Medicine, 31(9), 989–995. https://doi.org/10.1016/0277-9536(90)90108-5
Umberson, D. (1987). Family status and health behaviors: Social control as a dimension of social integration. Journal of Health and Social Behavior, 28(3), 306–319. https://doi.org/10.2307/2136848
Whetten, R., Whetten, K., Pence, B. W., Reif, S., Conover, C., & Bouis, S. (2006). Does distance affect utilization of substance abuse and mental health services in the presence of transportation services? AIDS Care, 18(Suppl 1), S27-34. https://doi.org/10.1080/09540120600839397
Woodward, A. T. (2011). Discrimination and help-seeking: Use of professional services and informal support among African Americans, Black Caribbeans, and Non-Hispanic Whites with a mental disorder. Race and Social Problems, 3(3), 146. https://doi.org/10.1007/s12552-011-9049-z
Funding
No funding was received to assist with the preparation of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose. The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Research Involving Human and/or Animal Participants
This study utilizes public-use data and does not directly involve human participants or animals.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Jacoby, A., Li, Y. Mental Health Care Access and Individual Help-Seeking During the Covid-19 Pandemic. Community Ment Health J 58, 1572–1583 (2022). https://doi.org/10.1007/s10597-022-00973-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10597-022-00973-3