
Abstract
To evaluate feasibility, frequency and severity of peri-procedural complications and post-procedural adverse events (AEs) in patients with advanced cholangiocarcinoma or liver metastasis of uveal melanoma and prior hemihepatectomy undergoing chemosaturation percutaneous hepatic perfusion (CS-PHP) and to analyze therapy response and overall survival compared to a matched group without prior surgery. CS-PHP performed between 10/2014 and 02/2018 were retrospectively assessed. To determine peri-procedural safety and post-procedural adverse events, hospital records and hematological, hepatic and biliary function were categorized using Common Terminology Criteria for Adverse Events (CTCAE) v5.0 (1–5; mild-death). Significance was tested using Wilcoxon signed-rank and Mann–Whitney U test. Kaplan–Meier estimation and log-rank test assessed survival. Overall 21 CS-PHP in seven patients (4/7 males; 52 ± 10 years) with hemihepatectomy (grouphemihep) and 22 CS-PHP in seven patients (3/7 males; 63 ± 12 years) without prior surgery (groupnoresection) were included. No complications occurred during the CS-PHP procedures. Transient changes (CTCAE grade 1–2) of liver enzymes and blood cells followed all procedures. In comparison, grouphemihep presented slightly more AEs grade 3–4 (e.g. thrombocytopenia in 57% (12/21) vs. 41% (9/22; p = 0.37)) 5–7 days after CS-PHP. These AEs were self-limiting or responsive to treatment (insignificant difference of pre-interventional to 21–45 days post-interventional values (p > 0.05)). One patient in grouphemihep with high tumor burden died eight days following CS-PHP. No deaths occurred in groupnoresection. In comparison, overall survival after first diagnosis was insignificantly shorter in groupnoresection (44.7(32–56.1) months) than in grouphemihep (48.3(34.6–72.8) months; p = 0.48). The severity of adverse events following CS-PHP in patients after hemihepatectomy was comparable to a matched group without prior liver surgery. Thus, the performance of CS-PHP is not substantially compromised by a prior hemihepatectomy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Surgical resection is an important treatment option for intrahepatic cholangiocarcinoma (iCCA) and metastatic uveal melanoma (UM) [1]. Determined by extent of tumor and anatomical location, liver resections vary from atypical resection to hemihepatectomy. Despite the curative intent of surgical resection, tumor recurrence in iCCA is a common problem with reported rates of up to 50% [2, 3] and in metastatic UM, recurrence rates of up to 80% are described [4, 5]. Tumor relapse is often challenging, as re-resection might not be suitable due to small fraction of left functional liver tissue and due to more challenging anatomical situs. According to current guidelines for iCCA, locoregional therapies can be considered after first-line chemotherapy and chemosaturation percutaneous hepatic perfusion (CS-PHP) already showed encouraging results in early studies [1, 6]. Concerning inoperable metastasized UM, no standard of care is available and current guidelines recommend ablation, infusion, perfusion and/or embolization therapies tailored to number and location of the metastases [7]. As in metastatic UM the liver is often the first and only site of metastases [8], liver directed therapies such as CS-PHP are of increasing relevance. Nonetheless, dedicated research investigating CS-PHP following liver resection is missing.
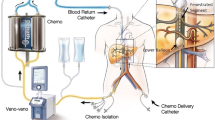
CS-PHP with melphalan is an innovative locoregional therapy for hepatic malignancies. The aim of CS-PHP is to control tumor growth, palliate symptoms and extent survival. Several studies have demonstrated efficacy in iCCA and UM and confirmed safety of the procedure [1, 9,10,11]. CS-PHP is taking advantage of the unique hepatic anatomy: high dose melphalan is administered via a catheter placed in the hepatic artery and thus, provides a non-diluted chemoperfusion of the diseased liver parenchyma. To prevent systemic damage caused by the melphalan-enriched blood, a double balloon catheter is placed in the inferior vena cava (IVC), which occludes the IVC above and below the confluens of the liver veins. The venous hepatic blood is extracted through the double balloon catheter, filtered via an extracorporeal melphalan specific filtration system and returned to the circulation through a sheath in the right jugular vein [11, 12].
In patients following resection of hepatic tissue, CS-PHP might be more complex and potentially hazardous. First, the anatomical changes following liver resection due to scarring, compensatory hypertrophy and changes of the venous drainage to the vena cava might compromise a safe positioning of the catheters. Second, the toxic effect of melphalan on the overall reduced liver parenchyma after hepatic resection might be increased. Thus, the purpose of this study was to evaluate frequency and severity of peri-procedural complications and post-procedural adverse events in patients with right hemihepatectomy undergoing CS-PHP and to compare these to a matched group without prior surgery.
Material and methods
Patient selection
The local ethics committee approved this retrospective study. In our tertiary care referral center, an interdisciplinary liver tumor board reaches treatment decisions for all patients with primary or secondary intrahepatic malignancies. From 10/2014 to 02/2018, 52 patients were scheduled for CS-PHP as last line treatment option and underwent 112 procedures (patient characteristics see Table 1). Among these 52 patients were seven patients with prior hemihepatectomy, who underwent 21 CS-PHP (grouphemihep), and were included in this study. No patient with prior hemihepatectomy undergoing CS-PHP was excluded.
Additionally, we defined seven patients (undergoing 22 CS-PHP) without hepatic resection as control group (groupnoresection). In order to achieve comparable patient collectives, grouphemihep and groupnoresection were matched by primary tumor, age, sex, number of consecutive CS-PHP and pre-interventional level of lactate dehydrogenase (LDH). Requirements for CS-PHP were sufficient hematological (haemoglobin > 8 g/dL; white blood count > 2 thsd/μL; platelets > 50 thsd/μL), hepatic (bilirubin ≤ 3 × upper limit of normal, maximum Child–Pugh A) and renal function (serum creatinine > 60 µmol/L). Contraindications included a recent history of transient ischemic attacks, heart failure with a left ventricular ejection fraction < 40% or significant chronic obstructive or restrictive pulmonary disorder. LDH, indicating tumor burden, should not exceed 500 IU/L. ECOG performance status must score 0 or 1 before CS-PHP. All patients gave written consent before CS-PHP.
Part of this study population has previously been reported [11, 13]. These articles dealt with safety and efficacy of the second-generation CS-PHP, whereas this study focuses on peri- and post-interventional adverse events and therapy response of patients with previous right hemihepatectomy compared to a matched group without prior liver surgery.
Data acquisition
Complications were observed during defined periods. In the peri-procedural period (start of general anesthesia to transfer to intensive care unit, adverse events (AEs) are more likely to be linked directly to the CS-PHP procedure. During the post-procedural period (1–2 days on intensive care unit), 5–7 days following CS-PHP (in-patient stay on regular ward) and during the subsequent 21–45 days (first control as outpatient), AEs are more likely to be related to systemic exposure of chemotherapeutic melphalan. Clinical reports regarding the hospital stay and follow up examinations were screened. Haematological parameters including full blood count and international normalized ratio (INR) as well as alanine transferase, aspartate transferase, gamma-glutamyl-transferase, alkaline phosphatase, total bilirubin and albumin indicating the liver function, LDH, creatinine as kidney function parameter, c-reactive protein and MELD-Scores were analysed. Values were assessed and classified using Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0. CTCAE is a descriptive terminology used for AE reporting. A severity scale is provided for each AE term (grades 1–5; mild-death). The assessment was performed by one radiologist (C.L.A.D.), blinded to the patient allocation to grouphemihep/groupnoresection. Pre-interventional measurements were considered baseline.
Either CT or MRI was performed before and within three months after CS-PHP. Treatment response was measured according to the RECIST 1.1 [14]. Overall survival (OS) was determined from initial diagnosis and first CS-PHP until last follow-up or death, whichever occurred first.
CS-PHP-Procedure
All procedures were performed in an angio suite under general anaesthesia due to the lengths of the intervention (mean 164 ± 52 min) and due to the haemodynamic changes, which are common with the transient inferior vena cava (IVC) occlusion and blood filtration [15]. In CS-PHP, an appropriate sheath is inserted through the femoral artery and a catheter is placed in the hepatic artery to provide a chemoperfusion with high dose melphalan of the supplied liver parenchyma. In order to prevent systemic exposure of the toxic melphalan, a double balloon catheter, inserted through the femoral vein, is placed in the IVC. The cranial balloon is inflated close to the cavoatrial junction and the caudal balloon is inflated in the subhepatic segment of the IVC, below the confluens of the hepatic veins (Fig. 1). The double balloon catheter is equipped with multiple side holes. An extracorporeal pump extracts the melphalan-enriched blood into a dedicated filtration system (Delcath system’s second-generation hemofiltration system), which separates melphalan from the venous blood with a filtration rate of up to 93–96% [15,16,17]. The extracorporeal circuit is completed by the return of the blood via a sheath in the jugular vein. In order to maintain an activated clotting time above 500 s, which is essential for safe extracorporeal hemofiltration, heparin is administered as needed. The melphalan dosage used in boths grouphemihep and groupnoresection was bodyweight dependent, 2,5–3 mg/kg ideal body weight up to a maximum dose of 220 mg of melphalan, dissolved in a 500 cc solution. The chemotherapeutic agent is infused in aliquots of each 100 cc at a rate of 0.4 ml/s, in between which an angiogram is performed to ascertain proper flow in the hepatic artery of interest.

Gd-EOB DTPA-enhanced MRI of a patient with prior right hemihepatectomy. The multifocal hepatic metastasis of uveal melanoma in the left liver (black arrows) are clearly depicted in the delayed transversal T1 weighted phase (a, b). A coronal CT scan (c) gives an overview of the postoperative situs following right hemihepatectomy. The star (*) marks the confluens of the liver veins (white arrow) close to the resection margin. d Displays the retrograde injection of contrast agent during CS-PHP to verify correct placement of the double balloon catheter. The cranial balloon of the double balloon catheter is placed in the cavoatrial junction in close proximity to the resection margin. The caudal balloon is placed below the confluens of the liver veins. No leakage is visible while the left liver vein is opacified (white arrow). e Presents an overview angiography of the celiac trunk with a small left hepatic artery. The catheter used for administration of melphalan is advanced to the left hepatic artery (f). IVC = inferior vena cava
24–72 h following CS-PHP, patients received single-shot antibiotics and granulocyte-colony stimulating factor.
Statistical analysis
Descriptive statistical analysis of the study data was performed. Survival was assessed using Kaplan–Meier estimation and log-rank test. Related data were tested for significance using non-parametric pairwise Wilcoxon signed-rank test and Mann–Whitney U test was performed for group comparison. Contingency table analysis was performed using chi-square test. Level of significance was set to p < 0.05. Statistical analyses were performed using commercially available software (JMP 15, SAS Institute). Values are presented in mean (and standard deviation) or median (and interquartile range).
Results
Overall, 21 CS-PHP in seven patients (52 ± 10 years, four men and three women) with prior right hemihepatectomy as well as 22 CS-PHP in seven patients (63 ± 12 years, three men and four women) without prior hepatic resection were included in this study. Prevalence of the underlying tumor entities were as follows: in grouphemihep, five patients with consecutive 14 CS-PHP suffered from iCCA and two patients underwent six CS-PHP in consequence of a metastasized UM. In groupnoresection, five patients with iCCA and 17 conducted CS-PHP as well as two patients with UM and five successful interventions were included. The patients median LDH values prior to the first CS-PHP were 320 (232–378) U/L in grouphemihep and 242 (236–333) U/L in groupnoresection (p = 0.95). Detailed patients` demographics, clinical and interventional parameters are displayed in Table 2.
CS-PHP and peri-interventional complications
There were no AEs of grade 3–5 recorded during the interventions. Hypotension and tachycardia were recorded during all procedures following inflation of the double balloon catheter and initiation of the veno-venous bypass including the filtration system and successfully managed by the anaesthesiologists. Overall, the cardiovascular fluctuations were self-limiting at the end of the procedures. Before administration of melphalan, the double balloon catheter had to be repositioned due to leakage of the cranial balloon in 3/21 interventions of three patients in grouphemihep and in 3/21 consecutive interventions of one patient in groupnoresection. The mean melphalan dose was 174 ± 24 mg in grouphemihep and 174 ± 30 mg in groupnoresection (p = 0.47). The mean procedure time was 169 ± 27 min in grouphemihep and 176 ± 52 min in groupnoresection (p = 0.69).
Toxicity and complications
In total, 114 AEs (grade 1–5) occurred in grouphemihep (5.5 AEs per intervention) and 106 AEs in groupnoresection (4.8 AEs per intervention; p = 0.68). The percentage distribution (Table 3) of the AEs grade 1–4 was comparable between grouphemihep and groupnoresection with the majority of AEs being rated mild (grade one; grouphemihep 32% (32/114) and groupnoresection 35% (37/106)) or moderate (grade two; grouphemihep 38% (44/114) and groupnoresection 38% (40/106)).
All interventions were followed by thrombocytopenia, anemia and an increase of liver enzymes. Most clinically relevant AEs accounted for toxicity-related hematologic and liver parameter changes (refer to Table 4): post-interventional thrombocytopenia grade three was common (52% (11/21) in grouphemihep and 36% (8/22) in groupnoresection; p = 0.36). Grade four thrombocytopenia with need for thrombocyte concentrates was observed after one procedure (5%) in each group. A reduced white blood count (WBC) equivalent to AE grade three was noted after 5–7 days in 24% (5/21) of the CS-PHP in grouphemihep and in 9% (2/22) of the CS-PHP in groupnoresection (p = 0.24). Increase of liver enzymes (AE grade three) was frequent in both groups (29% (6/21) in grouphemihep and 18% (4/22) in groupnoresection; p = 0.73). Whereas aspartate transferase values were elevated post-interventionally, alkaline phosphatase values showed an early decrease and an increase on day 5–7. The above-mentioned changes in blood count and liver enzymes were transient in both groups–no statistical significance was found when comparing baseline values to late post-interventional (21–45 days after CS-PHP) measurements. Detailed courses of laboratory parameters are displayed in Fig. 2.

Hematological and hepatic parameters of grouphemihep and groupnoresection pre, post, 5–7 days and 21–45 days after CS-PHP in a tabular overview (median and interquartile range); simplified course of laboratory parameters below. Statistical significance of parameter changes within grouphemihep and groupnoresection has been tested (p ≥ .05). HGB hemoglobin, PLT = platelet, WBC white blood count, ALB albumin, ALT alanine transferase, AST aspartate transferase, GGT gamma-glutamyl transferase, ALP alkaline phosphatase, LDH lactate dehydrogenase, CRP c-reactive protein, INR international normalized ratio, Crea creatinine, T BIL = total bilirubin, MELD-Score model of end stage liver disease-score
Non-toxic AEs grade three compromised inflammatory or infectious complications on day 5–7 after 5% (1/21) of the CS-PHP in grouphemihep and after 38% (8/22) of the interventions in groupnoresection (for details refer to Table 3). Non-toxic AEs grade 4 were: cholangitis (5%;1/21) after 5–7 days and post-interventional hypotension (5%;1/21) in grouphemihep and a post-interventional anaphylactic reaction to protamine (5%;1/22) in groupnoresection.
A case of death (AE grade five) occurred in grouphemihep in a patient with hepatic metastases from uveal melanoma and a high pre-interventional tumor burden (LDH 1559 U/I) (Table 1; patient seven). The patient developed multi-organ failure as well as pancytopenia and deceased eight days after his second CS-PHP despite intensive care treatment. There was no AE grade five in groupnoresection.
Therapy response and overall survival
In grouphemihep, the median time from initial diagnosis to first CS-PHP was 27 (14.5–80.5) months compared to 35 (11–42) in groupnoresection (p = 0.4). The median time from right hemihepatectomy to first CS-PHP was 10.5 (6–52) months. Following CS-PHP, the first follow up exam was performed 47 (42–60) days following CS-PHP in grouphemihep and 49 (43–71) days in groupnoresection (p = 0.78). The first therapy response according to RECIST 1.1 was 100% stable disease (SD) in groupnoresection (7/7). In the first response assessment of grouphemihep, 43% of patients presented with SD (3/7), 14% with complete remission (1/7), 14% with partial response (1/7) and 29% (2/7) with progressive disease; one of these two patients had extrahepatic progress. Taking into account not only the first but all therapy responses, the best response was 47% SD in grouphemihep (4/7), 71% SD in groupnoresection (5/7), 14% complete remission in both groups (1/7), 14% partial response in both groups (1/7) and 14% progressive disease (extrahepatic progression) in grouphemihep (1/7).
The median overall survival (OS) after first CS-PHP in groupnoresection was longer (19.7 (7.5–23.8) months) than in grouphemihep with 9.3 (4.2–17) months (p = 0.53). When comparing mean OS (months) from initial diagnosis, groupnoresection (44.7 (32–56.1)) had a shorter OS than grouphemihep (48.3 (34.6–72.8)) (p = 0.48).
Discussion
Chemosaturation percutaneous hepatic perfusion delivers high doses of chemotherapy directly to the liver while limiting systemic toxicity via hemofiltration of the hepatic venous blood [11]. In this retrospective study, we compared the peri- and post-interventional adverse events and therapy response of CS-PHP in seven patients with prior hemihepatectomy undergoing 21 procedures (grouphemihep) to a matched cohort of seven patients without hepatic surgery and 22 conducted interventions (groupnoresection). Our data show, that CS-PHP after hemihepatectomy has manageable toxicity comparable to a group of non-resected patients. Therefore, CS-PHP might serve as a potential last-line palliative treatment option for selected patients with cholangiocarcinoma and liverdominant metastatic uveal melanoma even after prior liver surgery.
The potential merit of locoregional liver therapies in metastatic uveal melanoma is controversially discussed and is of high importance as favorable systemic therapies are still lacking [18]. Khoja et. al analysed 29 phase II studies based on the original survival and response data and concluded, that locoregional therapy approaches present a clear numeric advantage compared to systemic therapies [19]. The use of CS-PHP in patients with liverdominant UM is based on the results of a landmark phase III randomized controlled study [9], which showed an improved progression free survival after CS-PHP versus best alternative care (BAC). Unfortunately, a high crossover of BAC patients to the CS-PHP group confounded any possible survival advantage in this study.
In the setting of unresectable iCCA, guidelines suggest locoregional therapy approaches in patients with tumor progression under first-line systemic chemotherapy [6]. CS-PHP in iCCA has so far only been evaluated in small cohorts, but presented long-lasting tumor stabilization in selected patients [1, 13, 20]. In order to provide optimal patient tailored treatment options, possible benefits over other locoregional therapy approaches (e.g. transarterial radioembolization (TARE)) need to be further evaluated.
The overall OS of our study collective is in line with the original phase III study of Hughes et al. and other current studies reporting OS ranging from 10 to 27 months [9, 20,21,22,23]. There was a trend for a shorter median overall survival in grouphemihep, which was 9.3 months after first CS-PHP in grouphemihep compared to 19.7 months in groupnoresection (p = 0.53). Of note, patients in grouphemihep were younger than in groupnoresection and the first CS-PHP was performed earlier after first diagnosis than in groupnoresection. The rapid disease progression of grouphemihep might reflect a more aggressive tumor biology and thus might explain the trend for a shorter OS.
Comparable numbers of AEs grade 1–5 were detected in both study groups. The mainly hematological AEs might be explained by incomplete extracorporeal filtration and delayed hepatic release of melphalan [9, 17]. Furthermore, leakages alongside the double balloon catheter (used to occlude the IVC) might increase systemic melphalan [12]. We detected a higher rate of leakages per patient in grouphemihep (3 leakages in 3/7 patients) than in groupnoresection (3 leakages in 1/7 patients), indicating that postsurgical anatomy makes positioning of the balloons more challenging. Nonetheless, in all patients an appropriate occlusion of the IVC was achieved before administration of melphalan. The liver-related AEs (reflecting direct toxicity of melphalan to the hepatocytes) were insignificantly higher in grouphemihep, presumably explained by the overall lower number of hepatocytes after hemihepatectomy. The monitored hematological and hepatic toxic effects were responsive to therapy and normalized towards the end of the observational period in both groups – indicating that reduced liver volume after hemihepatectomy does not impact long term results and underlining the safety of the procedure. Thus, the relevance of slightly more short-term toxicity-related AEs in grouphemihep seems negligible.
The clinically relevant AEs grade 3–4 recorded in our study were comparable to the results of recent studies. Kaydis et al. [21] examined the safety and efficacy of CS-PHP in 51 patients with metastasized UM receiving 134 CS-PHP. Comparable to our results, post-procedural hematological toxicities were common. Moreover, the AEs were comparable to those reported in the original Phase III study [9].
We found an equal percentage distribution of AEs grade 1–4 in grouphemihep and groupnoresection, but one death in grouphemihep. The deceased patient underwent surgery 172 months after first diagnosis of UM. Relapse occurred with disseminated intrahepatic metastasis and a high tumor burden (LDH 1559 U/I, norm: ≤ 250 U/I). SD was the response after the first procedure. After the second CS-PHP, the patient developed a neutropenic bacterial peritonitis and subsequent septic shock with multi organ failure and deceased eight days after CS-PHP. Of note, one patient in groupnoresection with high pre-interventional LDH (1064 U/I) suffered from pancytopenia and sepsis and deceased 2.8 months after the first and only CS-PHP. In both cases, the adverse outcome was most likely related to high tumor burden, which has been described to have a negative correlation to survival [11]. Both patients were aware of their high-risk profile and were treated due to a strong therapeutic wish of the patients. Consequently to these events, further patients with a high tumor burden were more carefully discussed in our institution.
There are several limitations to this study. We performed a single center study including only a small number of patients. Patient data was retrospectively evaluated for complications and adverse events. As a transregional center, we treat patients from across Germany and some patients received their follow up examinations outside our center. As a result, 19% of laboratory data were unavailable for day 21–45 of the observational period. Nevertheless, we acquired the laboratory results for up to 7 days for all treatments. According to other studies, this might be adequate to assess the toxicity of melphalan [11]. Overall, the number of interventions and the number of patients included in this study is limited. The patients included in groupnoresection did not match the patients in grouphemihep in all characteristics due to a lack of possible options, as CS-PHP is a rarely conducted procedure for selected patients only. This might lead to a limited comparability.
The severity of adverse events following chemosaturation percutaneous hepatic perfusion in patients after right hemihepatectomy was comparable to a matched group without prior liver surgery. Therefore, chemosaturation percutaneous hepatic perfusion with melphalan might be safely performed in patients following hemihepatectomy.
Abbreviations
- AE:
-
Adverse event
- BAC:
-
Best available care
- CS-PHP:
-
Chemosaturation percutaneous hepatic perfusion
- CTCAE:
-
Common terminology criteria for adverse events
- ECOG:
-
Eastern cooperative oncology group
- iCCA:
-
Intrahepatic cholangiocarcinoma
- INR:
-
International normalized ratio
- IVC:
-
Inferior vena cava
- LDH:
-
Lactate dehydrogenase
- MELD:
-
Model for end-stage liver disease
- OS:
-
Overall survival
- RECIST:
-
Response evaluation criteria in solid tumors
- SD:
-
Stable disease
- TARE:
-
Transarterial radioembolization
- UM:
-
Uveal melanoma
References
Marquardt S, Kirstein MM, Brüning R, Zeile M, Ferrucci PF, Prevoo W et al (2019) Percutaneous hepatic perfusion (chemosaturation) with melphalan in patients with intrahepatic cholangiocarcinoma: european multicentre study on safety, short-term effects and survival. Eur Radiol 29(4):1882–1892
Tian M-X, Zhou Y-F, Qu W-F, Liu W-R, Jin L, Jiang X-F et al (2019) Histopathology-based immunoscore predicts recurrence for intrahepatic cholangiocarcinoma after hepatectomy. Cancer Immunol Immunother 68(8):1369–1378
Sulpice L, Rayar M, Boucher E, Pracht M, Meunier B, Boudjema K (2012) Treatment of recurrent intrahepatic cholangiocarcinoma. Br J Surg Dezember 99(12):1711–1717
Aghayan DL, Kazaryan AM, Fretland ÅA, Sahakyan MA, Røsok BI, Bjørnbeth BA et al (2018) Laparoscopic liver resection for metastatic melanoma. Surg Endosc 32(3):1470–1477
Pawlik TM, Zorzi D, Abdalla EK, Clary BM, Gershenwald JE, Ross MI et al (2006) Hepatic resection for metastatic melanoma: distinct patterns of recurrence and prognosis for ocular versus cutaneous disease. Ann Surg Oncol 13(5):712–720
Valle JW, Borbath I, Khan SA, Huguet F, Gruenberger T, Arnold D (2016) Biliary cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol 27:v28–37
S3-Leitlinie zur Diagnostik, Therapie und Nachsorge des Melanoms, Version 3.2, AWMF, Register-Nummer: 032/024OL. 2019.
Jovanovic P, Mihajlovic M, Djordjevic-Jocic J, Vlajkovic S, Cekic S, Stefanovic V (2013) Ocular melanoma: an overview of the current status. Int J Clin Exp Pathol 6(7):1230–1244
Hughes MS, Zager J, Faries M, Alexander HR, Royal RE, Wood B et al (2016) Results of a randomized controlled multicenter phase III trial of percutaneous hepatic perfusion compared with best available care for patients with melanoma liver metastases. Ann Surg Oncol 23(4):1309–1319
Pingpank JF, Libutti SK, Chang R, Wood BJ, Neeman Z, Kam AW et al (2005) Phase I study of hepatic arterial melphalan infusion and hepatic venous hemofiltration using percutaneously placed catheters in patients with unresectable hepatic malignancies. JCO 23(15):3465–3474
Kirstein MM, Marquardt S, Jedicke N, Marhenke S, Koppert W, Manns MP et al (2017) Safety and efficacy of chemosaturation in patients with primary and secondary liver tumors. J Cancer Res Clin Oncol 143(10):2113–2121
Dewald CLA, Meine TC, Winther HMB, Kloeckner R, Maschke SK, Kirstein MM et al (2019) Chemosaturation percutaneous hepatic perfusion (CS-PHP) with melphalan: evaluation of 2D-perfusion angiography (2D-PA) for leakage detection of the venous double-balloon catheter. Cardiovasc Intervent Radiol 42(10):1441–1448
Schönfeld L, Hinrichs JB, Marquardt S, Voigtländer T, Dewald C, Koppert W et al (2020) Chemosaturation with percutaneous hepatic perfusion is effective in patients with ocular melanoma and cholangiocarcinoma. J Cancer Res Clin Oncol. https://doi.org/10.1007/s00432-020-03289-5
Schwartz LH, Litière S, de Vries E, Ford R, Gwyther S, Mandrekar S et al (2016) RECIST 1.1—update and clarification: from the RECIST committee. Eur J Cancer 62:132–137
Vogel A, Gupta S, Zeile M, von Haken R, Brüning R, Lotz G et al (2016) Chemosaturation percutaneous hepatic perfusion: a systematic review. Adv Ther 33(12):2122–2138
Moeslein FM, McAndrew EG, Appling WM, Hryniewich NE, Jarvis KD, Markos SM et al (2014) Evaluation of delcath systems’ generation 2 (GEN 2) melphalan hemofiltration system in a porcine model of percutaneous hepatic perfusion. Cardiovasc Intervent Radiol 37(3):763–769
de Leede EM, Burgmans MC, Meijer TS, Martini CH, Tijl FGJ, Vuyk J et al (2017) Prospective clinical and pharmacological evaluation of the delcath system’s second-generation (GEN2) hemofiltration system in patients undergoing percutaneous hepatic perfusion with melphalan. Cardiovasc Intervent Radiol 40(8):1196–1205
Triozzi PL, Singh AD (2015) Adjuvant therapy of uveal melanoma: current status. Ocul Oncol Pathol 1(1):54–62
Khoja L, Atenafu EG, Suciu S, Leyvraz S, Sato T, Marshall E et al (2019) Meta-analysis in metastatic uveal melanoma to determine progression free and overall survival benchmarks: an international rare cancers initiative (IRCI) ocular melanoma study. Ann Oncol 30(8):1370–1380
Vogl T, Zangos S, Scholtz J, Schmitt F, Paetzold S, Trojan J et al (2014) Chemosaturation with percutaneous hepatic perfusions of melphalan for hepatic metastases: experience from two european centers. Fortschr Röntgenstr 186(10):937–944
Karydis I, Gangi A, Wheater MJ, Choi J, Wilson I, Thomas K et al (2018) Percutaneous hepatic perfusion with melphalan in uveal melanoma: a safe and effective treatment modality in an orphan disease. J Surg Oncol 117(6):1170–1178
Abbott AM, Doepker MP, Kim Y, Perez MC, Gandle C, Thomas KL et al (2018) Hepatic progression-free and overall survival after regional therapy to the liver for metastatic melanoma. Am J Clin Oncol 41(8):747–753
Artzner C, Mossakowski O, Hefferman G, Grosse U, Hoffmann R, Forschner A et al (2019) Chemosaturation with percutaneous hepatic perfusion of melphalan for liver-dominant metastatic uveal melanoma: a single center experience. Cancer Imaging 19(1):31
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
All authors substantially contributed to the conception and design, acquisition of data or analysis and interpretation of data for this work. All authors drafted the article or substantially revised it due to the important intellectual content. All authors gave final approval of this version of the manuscript to be published.
Corresponding author
Ethics declarations
Conflict of interest
The authors of this manuscript declare relationships with the following companies: Siemens Healthcare and ProMedicus (Bernhard Meyer and Frank Wacker; outside the submitted work). The remaining authors declare no relationships with any companies whose products or services may be related to the subject matter of the article. All authors declare no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Dewald, C.L.A., Becker, L.S., Maschke, S.K. et al. Percutaneous isolated hepatic perfusion (chemosaturation) with melphalan following right hemihepatectomy in patients with cholangiocarcinoma and metastatic uveal melanoma: peri- and post-interventional adverse events and therapy response compared to a matched group without prior liver surgery. Clin Exp Metastasis 37, 683–692 (2020). https://doi.org/10.1007/s10585-020-10057-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10585-020-10057-9