
Abstract
Novel insights in the biology of cancer have switched the paradigm of a “one-size-fits-all” cancer treatment to an individualized biology-driven treatment approach. In recent years, a diversity of biomarkers and targeted therapies has been discovered. Although these examples accentuate the promise of personalized cancer treatment, for most cancers and cancer subgroups no biomarkers and effective targeted therapy are available. The great majority of patients still receive unselected standard therapies with no use of their individual molecular characteristics. Better knowledge about the underlying tumor biology will lead the way toward personalized cancer treatment. In this review, we summarize the evidence for a promising cancer biomarker: checkpoint with forkhead and ring finger domains (CHFR). CHFR is a mitotic checkpoint and tumor suppressor gene, which is inactivated in a diverse group of solid malignancies, mostly by promoter CpG island methylation. CHFR inactivation has shown to be an indicator of poor prognosis and sensitivity to taxane-based chemotherapy. Here we summarize the current knowledge of altered CHFR expression in cancer, the impact on tumor biology and implications for personalized cancer treatment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Over the last 20 years, there has been a revolution in the perspective of cancer treatment. Improvement of molecular profiling techniques such as next generation sequencing and whole genome methylation analysis made it possible to compare thousands of molecules simultaneously with high accuracy and speed. These studies have allowed novel and meaningful insights in the biology of cancer. Lung, breast, colorectal and many other cancers have shown to be heterogeneous diseases, which develop through specific molecular alterations that influence the clinical presentation, prognosis and response to therapy [1]. The diversity of molecular background and resultant biological behavior can be harnessed into an individualized biology-driven treatment, instead of the present “one-size-fits-all” approach. For some cancers, personalized cancer treatment is already implemented in daily practice.
In breast cancer treatment, for instance, it is now standard to test and target increased human epidermal growth factor receptor 2 (HER2) with both monoclonal antibodies such as trastuzumab or small molecule inhibitors such as lapatinib [2]. In non-small cell lung cancer (NSCLC) patients, testing for mutations in EGFR and KRAS, and EML4-anaplastic lymphoma kinase (ALK) gene rearrangements to select appropriately targeted therapy occurs on a routine basis. Mutations in the kinase domain of EGFR have shown to be a strong predictor of response to EGFR tyrosine kinase inhibitors (TKIs) erlotinib and gefitinib [3]. These patients respond better to EGFR TKIs than to chemotherapeutic agents carboplatin/paclitaxel, reflected by a significantly improved progression-free survival [4]. Furthermore, patients with NSCLC harboring the ALK rearrangement, which occurs in about 7 % of NSCLCs, benefit from ALK inhibitor crizotinib [5]. A recent prospective randomized phase III study compared crizotinib therapy to chemotherapy, pemetrexed or docetaxel, in 347 locally advanced or metastatic ALK-positive lung cancers, and clearly showed that crizotinib therapy is associated with a higher response rate 65 % (95 % CI, 58 to 72) versus 20 % (95 % CI, 14 to 26) (P < 0.001) but also an improved quality of life compared to chemotherapy. The relatively low incidence of EGFR and ALK aberrations in non-Asian patients, however, account for the fact that ∼87 % of patients with NSCLC still receive conventional chemotherapy with no suitable biomarkers for therapy selection. The same accounts for women with triple-negative breast cancer who do not benefit from anti-hormonal therapy or trastuzumab and for whom effective treatment is limited [6].
Other examples of useful biomarkers are KRAS mutation testing to predict benefit from monoclonal antibodies against EGFR, cetuximab and panitumumab, in metastatic colon cancer [7] and BRAF V600E mutation analysis in metastatic melanoma in order to predict responsiveness to BRAF inhibitors such as vemurafenib [8]. Salient to this review, testing for promoter CpG island methylation of DNA repair gene O6-methylguanine-DNA methyltransferase, MGMT, guides the clinical management of glioblastoma. MGMT is able to reverse the damage acquired by alkylating agents and therefore promotes methylation, and subsequent silencing of MGMT is associated with increased progression-free and overall survival after therapy with alkylating agents such as temozolomide [9, 10].
Although these examples display the promise of personalized cancer treatment and more biomarkers are being discovered, work is still in progress. For most cancers and cancer subgroups, no biomarkers and effective targeted therapy are available and therefore the great majority of patients still receive standard therapies with no individualization based on their tumor’s molecular characteristics.
In this review, we highlight a promising novel biomarker for which multiple lines of evidence are emerging: checkpoint with FHA and ring finger domains (CHFR). CHFR is a mitotic checkpoint- and tumor suppressor gene and is inactivated in a diverse number of solid malignancies. CHFR is most frequently inactivated by promoter CpG island methylation and has shown to be a marker of poor prognosis and increased sensitivity to treatment with taxanes. Here we summarize literature on the relevance of altered CHFR expression in cancer.
2 CHFR: an important regulator of cell cycle progression
CHFR is an early mitotic checkpoint gene that functions as a key player in controlling chromosomal integrity [11].
CHFR is expressed in the cytoplasm of all normal tissues and accumulates in the nucleus in response to microtubule poisoning or radiation damaging stress. After localization into the nucleus, CHFR becomes phosphorylated by protein kinase B (PKB/AKT), a member of the PI3K signaling pathway [12]. The nuclear distribution, mobility and function of CHFR are dependent upon interaction with promyelocytic leukemia protein (PML) bodies [13, 14]. CHFR expression levels fluctuate greatly during different stages of the cell cycle. Microtubule stress will lead to an elevation of CHFR expression levels and a mitotic arrest. To the contrary, auto-ubiquitination activity and degradation of CHFR, which is stimulated by AKT, are a prerequisite for mitotic entry [15]. Thereby, CHFR controls cell cycle progression at the G2/M transition as well.
It is not known how CHFR senses microtubule stress, but it has been shown that CHFR localizes to the mitotic spindle by an interaction with TCTP, a protein involved in microtubule stabilization and β-tubulin [16]. Disruption of the spindle causes CHFR to deliberate from TCTP and the mitotic spindle, which will enable the activation of signaling pathways and ultimately delay cell cycle progression [17].
These signaling pathways prevent entry into mitosis by inhibiting the activation of Cdc25 phosphatases that are able to activate the cyclin B1-Cdk1 kinase.
CHFR is able to influence the mitotic checkpoint by a proteosomal-dependent and a proteosomal-independent mechanism (Fig. 1).

CHFR delays entry into metaphase in respons to microtubular stress by effecting target proteins in a proteosome-dependent and a proteosome-independent manner
CHFR was first described to function as an E3 ubiquitin ligase, which ubiquitinates and targets proteins for degradation by the S26 proteosome [15, 18]. One of the target proteins is polo-like kinase 1 (PLK1). PLK1 is a serine/threonine kinase that is involved in the phosphorylation of Cdc25, thereby regulating cyclin B1-cdk activity. PLK1 phosphorylation and activation are established by another kinase, Aurora A [19–22]. By ubiquitination and degradation of both PLK1 and Aurora A, CHFR is able to inhibit the formation of the cyclin B1-Cdk complex and thereby promote cell cycle arrest [20, 23]. Although in vitro data are appealing, evidence that CHFR targets PLK1 for degradation in vivo as well is weak. There are conflicting studies that did not observe a decrease in PLK1 and Aurora A protein expression in response to microtubule poison [24–26]. Differences in study design and molecular environment make it difficult to compare results and therefore more studies are needed to clarify this inconsistency.
Other targets for ubiquitination and protein degradation by CHFR are chromokinesine protein Kif22[27], histone deacetylase HDAC1[28] and poly(ADP-ribose) 1 PARP1[29]. Kif22 plays a role in the organization of spindle microtubules and chromosome movement and regulation of Kif22 activity by CHFR is important for maintaining chromosomal stability [27]. HDAC1 is a histone deacetylase that is able to inhibit the expression of cell cycle genes such as p21. By ubiquitination of HDAC1, CHFR is able to reverse HDAC1-induced repression of p21 and thereby restore the p21-G1 checkpoint [28, 30, 31]. Interestingly, CHFR was also shown to inhibit invasiveness and metastatic potential caused by HDAC1 expression by the regulation of metastasis suppressors, KAI1 and E-cadherin [28].
PARP1 plays a role in the DNA damage response and is involved in the recruitment of CHFR to DNA damage sites immediately after DNA damage has occurred [29, 32]. CHFR then participates in a cascade of protein ubiquitination. One of the proteins that becomes ubiquitinated and degraded is PARP-1 itself. Thereby, CHFR is able to detach PARP-1 from the chromatin, which is an important step in the DNA damage repair response [29].
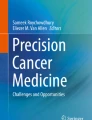
CHFR binds to PARP-1 via the RAR-binding zinc finger domain, which is situated in the cysteine region of CHFR. As the name illustrates, CHFR contains a N-terminal FHA domain, a central RING finger domain, and a C-terminal cysteine-rich domain (Fig. 2). The function of the FHA domain is largely unknown but is required for the checkpoint function and might be involved in the binding to phosphorylated proteins [19]. The RING finger domain is important for the ubiquitinating activity of CHFR and is able to form lysine 48- and lysine 63-linked polyubiquitination chains [25]. The cysteine-rich domain is important for the interaction between CHFR and target proteins [19–22]. Inside the cysteine-rich region, the RAR-binding zinc-finger (PBZ) is situated which is able to bind poly(ADP-ribose)PARP family members such as PARP-1.

CHFR gene and protein. Schematic representation of promoter CpG island methylation, mutation and polymorphisms with functional significance. of a CHFR gene encompassing 18 exons. CpG island is enlarged with CpG dinucleotides as vertical lines. TSS: transcription start site * mutation. # polymorphism. b CHFR protein consisting of 664 aminoacids. FHA: forhead-associated domain. RING: ringfinger domain. CR: cysteine-rich domain. PBZ: RAR-binding zinc-finger domain. Mutations in black, polymorphism in red
Recently, it was shown that CHFR also ubiquitinates and regulates the expression of TOPK [33]. TOPK is a promitotic serine/threonine kinase that phosphorylates and inactivates downstream substrate PTEN, which will lead to activation of AKT. By inhibiting TOPK, CHFR prevents the TOPK-induced activation of AKT and thereby blocks G2/M progression.
CHFR can also influence the mitotic checkpoint by functioning as an ubiquitin ligase that targets proteins not for degradation but for activation of signal transduction. By catalyzing the formation of noncanonical Lys63-linked polyubiquitin chains [25], CHFR was shown to activate the p38 stress kinase pathway, which will reverse chromosome condensation and induce a mitotic arrest [34]. Furthermore, CHFR indirectly inhibits the nuclear accumulation of cyclin B [24], thereby preventing the formation of the cyclin B1/cdk complex by the same mechanism, and also interacts with mitotic arrest deficient 2 (MAD2). MAD2 is a key protein in the spindle assembly checkpoint by its ability to sense improper spindle attachment and inhibit the anaphase-promoting-complex [35]. MAD2 is dependent upon binding to CHFR for its activation and transport to the kinetochore. In the absence of CHFR, MAD2 is not able to inhibit anaphase progression, which will result in mitotic defects [36].
Above-summarized data clearly show that CHFR is an important regulator of cell cycle progression. Since inactivation of CHFR promotes chromosomal defects and via activation of HDAC1 tissue invasion [28], CHFR malfunction is thought to play an important role in cancer progression and metastasis.
3 CHFR inactivation in cancer and its role as tumor suppressor
CHFR is more frequently inactivated in cancer than all other mitotic checkpoint control genes together [11]. Scolnick et al. were the first to report lack of CHFR expression in neuroblastoma and colorectal cancer cell lines [11]. Absence of CHFR in these cell lines resulted in a high mitotic index when exposed to microtubule stress compared to wild-type cancer cells, which was restored by reintroduction of functional CHFR. In a breast cancer cell line model, decreased CHFR expression resulted in an accelerated growth rate, enhanced invasiveness and amplified colony formation.
In order to study the physiological role of CHFR and its function in tumorigenesis, Chfr knockout mice have been generated [20]. Chfr knockout mice develop invasive lymphomas and solid tumors (lung, liver, gastrointestinal) after 40 weeks and have an increased susceptibility to chemical carcinogenesis [20]. Embryonic fibroblasts from Chfr-deficient mice show substantial aneuploidy and polyploidy. Therefore, CHFR inactivation is expected to participate in the acquisition of chromosomal defects and a chromosomal instability phenotype in cancer. In primary colorectal and breast cancer tissue, however, CHFR inactivation is not associated with chromosomal instability [37]. In colorectal cancer (CRC) and gastric cancer, CHFR inactivation is associated, however, with microsatellite instability (MSI) and MLH1 promoter CpG island methylation. The mechanism underlying the association between CHFR inactivation and MSI is unknown but might be due to an underlying DNA methylation defect that causes promoter CpG island methylation of both CHFR and MLH1. Murine studies, however, demonstrated that simultaneous loss of Chfr and Mlh1 synergistically increased predisposition to cancer development, which implicates a more functional interaction [38].
Furthermore, a recent study shows an additional role for CHFR in regulating expression of pro-inflammatory chemokine interleukin-8 (IL-8). CHFR is able to inhibit the NFκB signaling pathway and IL-8, which subsequently resulted in decreased angiogenesis and cell migration [39–41]. Inactivation of CHFR triggers NFκB signaling activity and thereby accelerates angiogenesis and a metastatic phenotype, which is associated with a poor prognosis.
4 Genetic and epigenetic mechanisms of CHFR transcriptional silencing
In the last decade, disrupted CHFR expression has been described in multiple cancer tissues (Table 1). Although promoter CpG island methylation is the most frequently occurring alteration leading to CHFR inactivation, genetic alterations have been observed occasionally. Scolnick and Halazonetis were the first to describe a sequence variation in the cysteine-rich domain of CHFR in osteosarcoma cell line U2OS [11] (Fig. 2). The variation consisted of a G to A transition leading to substitution of valine 539 by methionine and was initially interpreted as a missense mutation with functional impairment but turned out to be a polymorphism [42]. The relevance of variant genotypes was further studied in a series of 462 colorectal cancer patients and 245 healthy controls [43]. This study showed that the A allele of the GA variant was associated with a reduced CRC risk (P = 0.02; OR, 0.496; 95 % CI, 0.279–0.883). Thereby, it was shown that polymorphisms in the CHFR gene can be used as indicator for colorectal cancer susceptibility.
Additional studies to identify structural variations in the CHFR coding sequence led to the identification of three missense mutations in non-small cell lung cancer (NSCLC); all three were associated with a defective mitotic checkpoint [44]. Two mutations target the FHA and RING finger domain and the third is located in the cysteine-rich region (Fig. 2b). These mutations, however, were observed in only 3 out of 53 patients. Loss of the chromosomal region harboring CHFR, 12q24.33, occurs more frequently. In esophageal adenocarcinomas (EAC), CHFR DNA copy number loss appears to occur in 59 % (17/27) of esophageal cancers and is associated with reduced CHFR expression [45].
In most cancers, however, CHFR expression is reduced due to promoter CpG island methylation (Fig. 2a). The promoter region of CHFR contains a CpG island spanning −905 to +783 bp relative to the transcription start site. CHFR promoter CpG island methylation and subsequent transcriptional silencing was first described in esophageal cancer [46], of which 16.3 % (7/43) was hypermethylated while this was absent in adjacent normal tissues. Later it became clear that CHFR promoter CpG island methylation occurs in other cancers as well, among which CRC (24–53 %) and gastric cancer (35–52 %) (Table 1). In NSCLC, CHFR promoter CpG island methylation occurs in approximately 10–40 % of NSCLCs characterized by wild-type EGFR and KRAS in absence of ALK gene rearrangement, which implicates that CHFR promoter CpG island methylation occurs in a specific NSCLC subgroup [47].
Multiple studies have shown that CHFR promoter CpG island methylation can be detected not only in the primary cancers but also in blood (NSCLC) [47], stool (CRC) [48] and peritoneal fluid (gastric cancer) [49, 50]. This lends support to CHFR having promise as a diagnostic marker.
5 CHFR promoter methylation is associated with a poor prognosis and increased sensitivity to microtubule inhibitors
5.1 CHFR promoter CpG island methylation as prognostic marker
In recent years, it has become clear that CHFR promoter CpG island methylation is associated with a poor prognosis in multiple cancer types. In NSCLC, CHFR promoter CpG island methylation is associated with an increased risk of disease recurrence and poor survival [51–53]. In a series of 165 NSCLCs in which the CHFR promoter CpG island was methylated in 10 % of patients and KRAS and EGFR mutation were found in 8 % and 29 % of cases, CHFR promoter CpG island methylation was the only molecular alteration that was associated with a shorter survival (log-rank test, P = 0.0017) [52]. In colorectal cancer, an association between CHFR promoter CpG island methylation and poor prognosis has been reported in two independent studies. Tanake et al. [54] showed in a retrospective study of 82 resected high-risk stage II or III CRC that CHFR promoter CpG island methylation (assessed by pyrosequencing) was associated with a shorter recurrence free survival (log-rank test, P = 0.006) and a reduced overall survival (log-rank test, P = 0.07). We also recently showed that CHFR promoter CpG island methylation is an indicator of poor survival in stage II BRAF wild type microsatellite stable CRC (n = 66, P < 0.01, HR = 3.89, 95 % CI = 1.58–9.60) and validated these results in an independent prospective cohort study (n = 136, P = 0.07, HR = 2.11, 95 % CI = 0.95–4.59) (Cleven et al., submitted).
Together, these studies indicate that CHFR promoter CpG island methylation is an indicator of an aggressive phenotype characterized by a high risk of disease recurrence and a shorter overall survival. Testing for CHFR promoter CpG island methylation may help to select patients with a poor prognosis. Future studies are needed to investigate which treatment or screenings approaches will improve survival for patients with CHFR inactivated cancers.
5.2 CHFR promoter CpG island methylation as predictor of taxane sensitivity
Although CHFR promoter CpG island methylation is associated with a poor prognosis, CHFR inactivation predisposes to an increased sensitivity to microtubule inhibitors (Table 2). Microtubule inhibitors such as docetaxel and paclitaxel disrupt normal microtubule dynamics during cell division by binding to the beta-tubulin subunits. This will lead to a failure of microtubule separation and apoptosis. As CHFR is able to block entry into prophase until chromosomal alignment is restored, CHFR inhibits the effect of taxanes. Accordingly, cells expressing CHFR are more viable upon treatment with microtubule inhibitors compared to cells not expressing CHFR [55].
The association between CHFR expression and decreased sensitivity to microtubule inhibitors was first shown by Satoh et al. in gastric cancer cell lines [56]. Docetaxel or paclitaxel is a standard treatment option for gastric cancer, though not all patients will respond to this therapy. CHFR promoter CpG island methylation was hypothesized to be an important determinant of response to therapy. In a small study of 12 patients with advanced stage gastric cancer that received adjuvant paclitaxel, CHFR promoter CpG island methylation was associated with a better clinical response compared to cancers with unmethylated CHFR of which the majority showed progressive disease [57]. These results could, however, not be confirmed in a larger study of 41 gastric cancers in which promoter CpG island methylation was not associated with response to docetaxel or paclitaxel [58]. Of note, clinical response, however, was measured in metastatic lesions where the methylation status of CHFR was not assessed.
Stronger support for the potential role for CHFR promoter CpG island methylation in predicting response to microtubule inhibitors has been described in other cancer types. Cervical adenocarcinoma cell lines (n = 6) with CHFR promoter CpG island methylation, for instance, are sensitive to treatment with docetaxel and paclitaxel [59]. Treatment with 5-Aza-2′-deoxycytidine recovered CHFR expression and decreased the sensitivity to these agents immediately, an effect that was not observed for treatment with 5-fluorouracil, etoposide, cisplatin and doxorubicin. The same accounts for CHFR promoter CpG island methylation and treatment with paclitaxel in endometrial cancer cell lines [60, 61] and in NSCLCs [62].
Other preclinical evidence for CHFR as marker of taxane sensitivity comes from a recent retrospective study that analyzed CHFR inactivation and response to paclitaxel in metastatic NSCLC [63]. CHFR promoter CpG island methylation was assessed with MSP and validated by methylation microarray and nuclear expression of CHFR was analyzed by immunohistochemistry. Although CHFR promoter CpG island methylation was observed in only 1/32 (3.1 %) patients, 16/41 (37 %) patients showed reduced nuclear staining of CHFR, indicating the presence of a CHFR repressive event other than promoter CpG island methylation that still needs to be elucidated. In this study diminished nuclear CHFR expression was associated with a better response to therapy (19 % versus 52 % progression at first restaging, P = 0.033) and a prolonged overall survival (9.1 versus 5.1 months, HR 0.28, 95 % CI = 0.14–0.56) compared to patients with high CHFR nuclear expression.
Finally, in colorectal cancer, a recently reported preclinical study showed increased sensitivity to taxanes in colorectal cancer cell lines both in vitro and in vivo. The correlation between CHFR expression and resistance to docetaxel was statistically significant (P = 0.033), with a 20-fold increase in median IC50 for cell lines that had measurable CHFR expression versus silenced cell lines [64].
Although randomized prospective clinical trials are needed before implementation into clinical practice, these studies together strongly support the evidence for CHFR inactivation as marker of taxane sensitivity.
6 Conclusion
In the last decade, a substantial number of studies have been performed to investigate CHFR inactivation, usually due to promoter CpG island methylation, as biomarker to predict prognosis and response to microtubule inhibitors in a diversity of cancers. There is compelling evidence that reduced CHFR expression is a promising biomarker that can improve the management of multiple tumor types.
The clinical impact of CHFR promoter CpG island methylation as prognostic marker will be in the selection of patients with an aggressive phenotype. In stage II CRC, CHFR promoter CpG island methylation can help to identify patients with a worse prognosis that might benefit from adjuvant therapy. The same accounts for CHFR inactivation as predictive marker of taxane sensitivity where CHFR inactivation can help to select patients for taxane treatment. Furthermore, these results can be a rationale for studying the effect of taxane treatment in cancers with CHFR inactivation. A prospective trial to test this hypothesis in CRC is presently ongoing.
The clinical value of any biomarker, however, depends on the accuracy of the test. The majority of candidate biomarkers reported in literature do not reach clinical use mostly because they fail to pass the validation phase. This can be explained by intra- and inter-tumor heterogeneity, a technical inability to consistently verify the presence of the biomarker in patient’s material, and the lack of specificity for a particular disease. In most studies, CHFR promoter CpG island methylation is assessed by methylation-specific PCR (MSP). MSP is a very sensitive qualitative method that is able to detect aberrant methylation in minute amounts of DNA [65]. One important aspect of the technique is the region selected to be analyzed since not all regions within the CpG island have biological and clinical relevance [66]. In the literature, however, different locations within the promoter CpG island of CHFR have been analyzed (Table 1), which makes it difficult to compare results. CpG methylation within region −240 to −73 bp relative to the transcription start site of CHFR has shown to result in gene silencing [46] and is therefore proposed as core region of promoter methylation [67].
One of the technical challenges of MSP is a false positive result due to inadequacy of bisulfite treatment and mispriming especially when nested PCR or high numbers of PCR cycles are used [65]. Several alternative methods are available among which pyrosequencing [68]. Pyrosequencing permits a quantitative methylation analysis with single nucleotide resolution of the amplified region but also relies on amplification of bisulfite-converted DNA. One of the challenges of pyrosequencing, however, is that the technique requires a numeric cutoff value to define a positive methylation status, which is difficult in a clinical setting that is dependent upon biopsy specimens that are usually small and do not allow correction for tumor heterogeneity or involvement of normal tissues. The same accounts for other quantitative (q)MSP techniques.
Besides MSP, pyrosequencing and qMSP, recently also ultra-deep next-generation-based bisulfite sequencing has become available. Future studies are needed to evaluate the performance of the different techniques in assessing CHFR methylation status in a clinical setting. Since all associations between CHFR promoter methylation and clinical variables (Table 2) until now are consistently found with MSP, at present MSP is the more promising method of choice.
Furthermore, large, independent cohort studies and clinical trials are needed to validate the prognostic and predictive value of CHFR inactivation. These trials will need to be compared to established clinical markers such as Tumor-Node-Metastasis (TNM) classification system. Simon et al. have proposed a less time consuming design in which archival material of prospective trials is used to investigate the performance of a single biomarker [69].
In conclusion, the combination of the crucial role of CHFR in mitotic checkpoint control and a clear prognostic and predictive power highlights the clinical potential of CHFR as biomarker. Although work is still in progress, currently available results all point into the same direction and make CHFR inactivation, mostly due to promoter CpG island methylation, a biomarker with great potential and the development of clinical trials to validate its predictive and prognostic value, a priority.
References
Dienstmann, R., Rodon, J., Barretina, J., & Tabernero, J. (2013). Genomic medicine frontier in human solid tumors: prospects and challenges. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology, 31(15), 1874–1884.
Olopade, O. I., Grushko, T. A., Nanda, R., & Huo, D. (2008). Advances in breast cancer: pathways to personalized medicine. Clinical Cancer Research : an Official Journal of the American Association for Cancer Research, 14(24), 7988–7999.
Fukuoka, M., Wu, Y. L., Thongprasert, S., Sunpaweravong, P., Leong, S. S., Sriuranpong, V., et al. (2011). Biomarker analyses and final overall survival results from a phase III, randomized, open-label, first-line study of gefitinib versus carboplatin/paclitaxel in clinically selected patients with advanced non-small-cell lung cancer in Asia (IPASS). Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology, 29(21), 2866–2874.
Mok, T. S. (2011). Personalized medicine in lung cancer: what we need to know. Nature Reviews Clinical Oncology, 8(11), 661–668.
Shaw, A. T., Yeap, B. Y., Solomon, B. J., Riely, G. J., Gainor, J., Engelman, J. A., et al. (2011). Effect of crizotinib on overall survival in patients with advanced non-small-cell lung cancer harbouring ALK gene rearrangement: a retrospective analysis. The Lancet Oncology, 12(11), 1004–1012.
Andre, F., & Zielinski, C. C. (2012). Optimal strategies for the treatment of metastatic triple-negative breast cancer with currently approved agents. Annals of Oncology : Official Journal of the European Society for Medical Oncology/ESMO, 23(Suppl 6), vi46–vi51.
Karapetis, C. S., Khambata-Ford, S., Jonker, D. J., O’Callaghan, C. J., Tu, D., Tebbutt, N. C., et al. (2008). K-ras mutations and benefit from cetuximab in advanced colorectal cancer. The New England Journal of Medicine, 359(17), 1757–1765.
Flaherty, K. T., Puzanov, I., Kim, K. B., Ribas, A., McArthur, G. A., Sosman, J. A., et al. (2010). Inhibition of mutated, activated BRAF in metastatic melanoma. The New England Journal of Medicine, 363(9), 809–819.
Hegi, M. E., Diserens, A. C., Gorlia, T., Hamou, M. F., de Tribolet, N., Weller, M., et al. (2005). MGMT gene silencing and benefit from temozolomide in glioblastoma. The New England Journal of Medicine, 352(10), 997–1003.
Hegi, M. E., Liu, L., Herman, J. G., Stupp, R., Wick, W., Weller, M., et al. (2008). Correlation of O6-methylguanine methyltransferase (MGMT) promoter methylation with clinical outcomes in glioblastoma and clinical strategies to modulate MGMT activity. Journal of Clinical Oncology : official journal of the American Society of Clinical Oncology, 26(25), 4189–4199.
Scolnick, D. M., & Halazonetis, T. D. (2000). Chfr defines a mitotic stress checkpoint that delays entry into metaphase. Nature, 406(6794), 430–435.
Shtivelman, E. (2003). Promotion of mitosis by activated protein kinase B after DNA damage involves polo-like kinase 1 and checkpoint protein CHFR. Molecular Cancer Research : MCR, 1(13), 959–969.
Daniels, M. J., Marson, A., & Venkitaraman, A. R. (2004). PML bodies control the nuclear dynamics and function of the CHFR mitotic checkpoint protein. Nature Structural & Molecular Biology, 11(11), 1114–1121.
Fukuda, T., Kondo, Y., & Nakagama, H. (2008). The anti-proliferative effects of the CHFR depend on the forkhead associated domain, but not E3 ligase activity mediated by ring finger domain. PLoS ONE, 3(3), e1776.
Kim, J. S., Park, Y. Y., Park, S. Y., Cho, H., & Kang, D. (2011). The auto-ubiquitylation of E3 ubiquitin-protein ligase Chfr at G2 phase is required for accumulation of polo-like kinase 1 and mitotic entry in mammalian cells. The Journal of Biological Chemistry, 286(35), 30615–30623.
Yarm, F. R. (2002). Plk phosphorylation regulates the microtubule-stabilizing protein TCTP. Molecular and Cellular Biology, 22(17), 6209–6221.
Burgess, A., Labbe, J. C., Vigneron, S., Bonneaud, N., Strub, J. M., Van Dorsselaer, A., et al. (2008). Chfr interacts and colocalizes with TCTP to the mitotic spindle. Oncogene, 27(42), 5554–5566.
van Vugt, M. A., & Medema, R. H. (2005). Getting in and out of mitosis with Polo-like kinase-1. Oncogene, 24(17), 2844–2859.
Li, J., Williams, B. L., Haire, L. F., Goldberg, M., Wilker, E., Durocher, D., et al. (2002). Structural and functional versatility of the FHA domain in DNA-damage signaling by the tumor suppressor kinase Chk2. Molecular Cell, 9(5), 1045–1054.
Yu, X., Minter-Dykhouse, K., Malureanu, L., Zhao, W. M., Zhang, D., Merkle, C. J., et al. (2005). Chfr is required for tumor suppression and Aurora A regulation. Nature Genetics, 37(4), 401–406.
Privette, L. M., Weier, J. F., Nguyen, H. N., Yu, X., & Petty, E. M. (2008). Loss of CHFR in human mammary epithelial cells causes genomic instability by disrupting the mitotic spindle assembly checkpoint. Neoplasia, 10(7), 643–652.
Vader, G., & Lens, S. M. (2008). The Aurora kinase family in cell division and cancer. Biochimica et Biophysica Acta, 1786(1), 60–72.
Kang, D., Chen, J., Wong, J., & Fang, G. (2002). The checkpoint protein Chfr is a ligase that ubiquitinates Plk1 and inhibits Cdc2 at the G2 to M transition. The Journal of Cell Biology, 156(2), 249–259.
Summers, M. K., Bothos, J., & Halazonetis, T. D. (2005). The CHFR mitotic checkpoint protein delays cell cycle progression by excluding cyclin B1 from the nucleus. Oncogene, 24(16), 2589–2598.
Bothos, J., Summers, M. K., Venere, M., Scolnick, D. M., & Halazonetis, T. D. (2003). The Chfr mitotic checkpoint protein functions with Ubc13-Mms2 to form Lys63-linked polyubiquitin chains. Oncogene, 22(46), 7101–7107.
Welchman, R. L., Gordon, C., & Mayer, R. J. (2005). Ubiquitin and ubiquitin-like proteins as multifunctional signals. Nature Reviews Molecular Cell Biology, 6(8), 599–609.
Maddika, S., Sy, S. M., & Chen, J. (2009). Functional interaction between Chfr and Kif22 controls genomic stability. The Journal of Biological Chemistry, 284(19), 12998–13003.
Oh, Y. M., Kwon, Y. E., Kim, J. M., Bae, S. J., Lee, B. K., Yoo, S. J., et al. (2009). Chfr is linked to tumour metastasis through the downregulation of HDAC1. Nature Cell Biology, 11(3), 295–302.
Kashima, L., Idogawa, M., Mita, H., Shitashige, M., Yamada, T., Ogi, K., et al. (2012). CHFR protein regulates mitotic checkpoint by targeting PARP-1 protein for ubiquitination and degradation. The Journal of Biological Chemistry, 287(16), 12975–12984.
Vidal, A., & Koff, A. (2000). Cell-cycle inhibitors: three families united by a common cause. Gene, 247(1–2), 1–15.
Kim, J. H., Kim, B., Cai, L., Choi, H. J., Ohgi, K. A., Tran, C., et al. (2005). Transcriptional regulation of a metastasis suppressor gene by Tip60 and beta-catenin complexes. Nature, 434(7035), 921–926.
Ahel, I., Ahel, D., Matsusaka, T., Clark, A. J., Pines, J., Boulton, S. J., et al. (2008). Poly(ADP-ribose)-binding zinc finger motifs in DNA repair/checkpoint proteins. Nature, 451(7174), 81–85.
Shinde, S. R., Gangula, N. R., Kavela, S., Pandey, V., & Maddika, S. (2013). TOPK and PTEN participate in CHFR mediated mitotic checkpoint. Cellular Signalling, 25(12), 2511–2517.
Matsusaka, T., & Pines, J. (2004). Chfr acts with the p38 stress kinases to block entry to mitosis in mammalian cells. The Journal of Cell Biology, 166(4), 507–516.
Fang, G., Yu, H., & Kirschner, M. W. (1998). The checkpoint protein MAD2 and the mitotic regulator CDC20 form a ternary complex with the anaphase-promoting complex to control anaphase initiation. Genes and Development, 12(12), 1871–1883.
Keller, J. A., & Petty, E. M. (2011). CHFR binds to and regulates MAD2 in the spindle checkpoint through its cysteine-rich domain. Biochemical and Biophysical Research Communications, 409(3), 389–393.
Bertholon, J., Wang, Q., Falette, N., Verny, C., Auclair, J., Chassot, C., et al. (2003). Chfr inactivation is not associated to chromosomal instability in colon cancers. Oncogene, 22(55), 8956–8960.
Fu, Z., Regan, K., Zhang, L., Muders, M. H., Thibodeau, S. N., French, A., et al. (2009). Deficiencies in Chfr and Mlh1 synergistically enhance tumor susceptibility in mice. The Journal of Clinical Investigation, 119(9), 2714–2724.
Kashima, L., Toyota, M., Mita, H., Suzuki, H., Idogawa, M., Ogi, K., et al. (2009). CHFR, a potential tumor suppressor, downregulates interleukin-8 through the inhibition of NF-kappaB. Oncogene, 28(29), 2643–2653.
Nurnberg, W., Tobias, D., Otto, F., Henz, B. M., & Schadendorf, D. (1999). Expression of interleukin-8 detected by in situ hybridization correlates with worse prognosis in primary cutaneous melanoma. The Journal of Pathology, 189(4), 546–551.
Lee, K. H., Bae, S. H., Lee, J. L., Hyun, M. S., Kim, S. H., Song, S. K., et al. (2004). Relationship between urokinase-type plasminogen receptor, interleukin-8 gene expression and clinicopathological features in gastric cancer. Oncology, 66(3), 210–217.
Mizuno, K., Osada, H., Konishi, H., Tatematsu, Y., Yatabe, Y., Mitsudomi, T., et al. (2002). Aberrant hypermethylation of the CHFR prophase checkpoint gene in human lung cancers. Oncogene, 21(15), 2328–2333.
Kang, H. C., Kim, I. J., Jang, S. G., Hong, S. H., Hwang, J. A., Shin, H. R., et al. (2008). Coding region polymorphisms in the CHFR mitotic stress checkpoint gene are associated with colorectal cancer risk. Cancer Letters, 260(1–2), 170–179.
Mariatos, G., Bothos, J., Zacharatos, P., Summers, M. K., Scolnick, D. M., Kittas, C., et al. (2003). Inactivating mutations targeting the chfr mitotic checkpoint gene in human lung cancer. Cancer Research, 63(21), 7185–7189.
Soutto, M., Peng, D., Razvi, M., Ruemmele, P., Hartmann, A., Roessner, A., et al. (2010). Epigenetic and genetic silencing of CHFR in esophageal adenocarcinomas. Cancer, 116(17), 4033–4042.
Shibata, Y., Haruki, N., Kuwabara, Y., Ishiguro, H., Shinoda, N., Sato, A., et al. (2002). Chfr expression is downregulated by CpG island hypermethylation in esophageal cancer. Carcinogenesis, 23(10), 1695–1699.
Salazar, F., Molina, M. A., Sanchez-Ronco, M., Moran, T., Ramirez, J. L., Sanchez, J. M., et al. (2011). First-line therapy and methylation status of CHFR in serum influence outcome to chemotherapy versus EGFR tyrosine kinase inhibitors as second-line therapy in stage IV non-small-cell lung cancer patients. Lung Cancer, 72(1), 84–91.
Bosch, L. J., Mongera, S., Terhaar Sive Droste, J. S., Oort, F. A., van Turenhout, S. T., Penning, M. T., et al. (2012). Analytical sensitivity and stability of DNA methylation testing in stool samples for colorectal cancer detection. Cellular Oncology, 35(4), 309–315.
Hiraki, M., Kitajima, Y., Sato, S., Nakamura, J., Hashiguchi, K., Noshiro, H., et al. (2010). Aberrant gene methylation in the peritoneal fluid is a risk factor predicting peritoneal recurrence in gastric cancer. World journal of gastroenterology : WJG, 16(3), 330-338.
Hiraki, M., Kitajima, Y., Koga, Y., Tanaka, T., Nakamura, J., Hashiguchi, K., et al. (2011). Aberrant Gene Methylation Is a Biomarker for the Detection of Cancer Cells in Peritoneal Wash Samples from Advanced Gastric Cancer Patients. Annals of surgical oncology.
Koga, T., Takeshita, M., Yano, T., Maehara, Y., & Sueishi, K. (2011). CHFR hypermethylation and EGFR mutation are mutually exclusive and exhibit contrastive clinical backgrounds and outcomes in non-small cell lung cancer. International Journal of Cancer. Journal International du Cancer, 128(5), 1009–1017.
Koga, T., Takeshita, M., Ijichi, K., Yano, T., Maehara, Y., & Sueishi, K. (2013). CHFR aberrant methylation involves a subset of human lung adenocarcinoma associated with poor clinical outcomes. Human pathology.
Takeshita, M., Koga, T., Takayama, K., Kouso, H., Nishimura-Ikeda, Y., Yoshino, I., et al. (2008). CHFR expression is preferentially impaired in smoking-related squamous cell carcinoma of the lung, and the diminished expression significantly harms outcomes. International Journal of Cancer. Journal International du Cancer, 123(7), 1623–1630.
Tanaka, M., Chang, P., Li, Y., Li, D., Overman, M., Maru, D. M., et al. (2011). Association of CHFR Promoter Methylation with Disease Recurrence in Locally Advanced Colon Cancer. Clinical Cancer Research : an Official Journal of the American Association for Cancer Research, 17(13), 4531–4540.
Chaturvedi, P., Sudakin, V., Bobiak, M. L., Fisher, P. W., Mattern, M. R., Jablonski, S. A., et al. (2002). Chfr regulates a mitotic stress pathway through its RING-finger domain with ubiquitin ligase activity. Cancer Research, 62(6), 1797–1801.
Satoh, A., Toyota, M., Itoh, F., Sasaki, Y., Suzuki, H., Ogi, K., et al. (2003). Epigenetic inactivation of CHFR and sensitivity to microtubule inhibitors in gastric cancer. Cancer Research, 63(24), 8606–8613.
Koga, Y., Kitajima, Y., Miyoshi, A., Sato, K., Sato, S., & Miyazaki, K. (2006). The significance of aberrant CHFR methylation for clinical response to microtubule inhibitors in gastric cancer. Journal of Gastroenterology, 41(2), 133–139.
Yoshida, K., Hamai, Y., Suzuki, T., Sanada, Y., Oue, N., & Yasui, W. (2006). DNA methylation of CHFR is not a predictor of the response to docetaxel and paclitaxel in advanced and recurrent gastric cancer. Anticancer Research, 26(1A), 49–54.
Banno, K., Yanokura, M., Kawaguchi, M., Kuwabara, Y., Akiyoshi, J., Kobayashi, Y., et al. (2007). Epigenetic inactivation of the CHFR gene in cervical cancer contributes to sensitivity to taxanes. International Journal of Oncology, 31(4), 713–720.
Yanokura, M., Banno, K., Kawaguchi, M., Hirao, N., Hirasawa, A., Susumu, N., et al. (2007). Relationship of aberrant DNA hypermethylation of CHFR with sensitivity to taxanes in endometrial cancer. Oncology Reports, 17(1), 41–48.
Wang, X., Yang, Y., Xu, C., Xiao, L., Shen, H., Zhang, X., et al. (2011). CHFR suppression by hypermethylation sensitizes endometrial cancer cells to paclitaxel. International Journal of Gynecological Cancer : official journal of the International Gynecological Cancer Society, 21(6), 996–1003.
Takeshita, M., Koga, T., Takayama, K., Yano, T., Maehara, Y., Nakanishi, Y., et al. (2010). Alternative efficacy-predicting markers for paclitaxel instead of CHFR in non-small-cell lung cancer. Cancer Biology and Therapy, 10(9), 933–941.
Pillai, R. N., Brodie, S. A., Sica, G. L., Shaojin, Y., Li, G., Nickleach, D. C., et al. (2013). CHFR protein expression predicts outcomes to taxane-based first line therapy in metastatic NSCLC. Clinical Cancer Research: An Official Journal of the American Association for Cancer Research, 19(6), 1603–1611.
Pelosof, L., Yerram, S. R., Ahuja, N., Delmas, A., Danilova, L., Herman, J. G., et al. (2013). CHFR silencing or microsatellite instability is associated with increased anti-tumor activity of docetaxel or gemcitabine in colorectal cancer. International Journal of Cancer. Journal International du Cancer
Herman, J. G., Graff, J. R., Myohanen, S., Nelkin, B. D., & Baylin, S. B. (1996). Methylation-specific PCR: a novel PCR assay for methylation status of CpG islands. Proceedings of the National Academy of Sciences of the United States of America, 93(18), 9821–9826.
van Vlodrop, I. J., Niessen, H. E., Derks, S., Baldewijns, M. M., van Criekinge, W., Herman, J. G., et al. (2011). Analysis of promoter CpG island hypermethylation in cancer: location, location, location! Clinical Cancer Research: An Official journal of the American Association for Cancer Research, 17(13), 4225–4231.
Brandes, J. C., van Engeland, M., Wouters, K. A., Weijenberg, M. P., & Herman, J. G. (2005). CHFR promoter hypermethylation in colon cancer correlates with the microsatellite instability phenotype. Carcinogenesis, 26(6), 1152–1156.
Tost, J., & Gut, I. G. (2007). DNA methylation analysis by pyrosequencing. Nature Protocols, 2(9), 2265–2275.
Simon, R. M., Paik, S., & Hayes, D. F. (2009). Use of archived specimens in evaluation of prognostic and predictive biomarkers. Journal of the National Cancer Institute, 101(21), 1446–1452.
Privette, L. M., Gonzalez, M. E., Ding, L., Kleer, C. G., & Petty, E. M. (2007). Altered expression of the early mitotic checkpoint protein, CHFR, in breast cancers: implications for tumor suppression. Cancer Research, 67(13), 6064–6074.
Erson, A. E., & Petty, E. M. (2004). CHFR-associated early G2/M checkpoint defects in breast cancer cells. Molecular Carcinogenesis, 39(1), 26–33.
Agundez, M., Grau, L., Palou, J., Algaba, F., Villavicencio, H., & Sanchez-Carbayo, M. (2011). Evaluation of the methylation status of tumour suppressor genes for predicting bacillus calmette-guerin response in patients with T1G3 high-risk bladder tumours. European Urology, 60(1), 131–140.
Toyota, M., Sasaki, Y., Satoh, A., Ogi, K., Kikuchi, T., Suzuki, H., et al. (2003). Epigenetic inactivation of CHFR in human tumors. Proceedings of the National Academy of Sciences of the United States of America, 100(13), 7818–7823.
Corn, P. G., Summers, M. K., Fogt, F., Virmani, A. K., Gazdar, A. F., Halazonetis, T. D., et al. (2003). Frequent hypermethylation of the 5′ CpG island of the mitotic stress checkpoint gene Chfr in colorectal and non-small cell lung cancer. Carcinogenesis, 24(1), 47–51.
Derks, S., Postma, C., Carvalho, B., van den Bosch, S. M., Moerkerk, P. T., Herman, J. G., et al. (2008). Integrated analysis of chromosomal, microsatellite and epigenetic instability in colorectal cancer identifies specific associations between promoter methylation of pivotal tumour suppressor and DNA repair genes and specific chromosomal alterations. Carcinogenesis, 29(2), 434–439.
Morioka, Y., Hibi, K., Sakai, M., Koike, M., Fujiwara, M., Kodera, Y., et al. (2006). Aberrant methylation of the CHFR gene is frequently detected in non-invasive colorectal cancer. Anticancer Research, 26(6B), 4267–4270.
Kawasaki, T., Ohnishi, M., Nosho, K., Suemoto, Y., Kirkner, G. J., Meyerhardt, J. A., et al. (2008). CpG island methylator phenotype-low (CIMP-low) colorectal cancer shows not only few methylated CIMP-high-specific CpG islands, but also low-level methylation at individual loci. Modern Pathology: An Official Journal of the United States and Canadian Academy of Pathology, Inc, 21(3), 245–255.
Honda, T., Tamura, G., Waki, T., Kawata, S., Nishizuka, S., & Motoyama, T. (2004). Promoter hypermethylation of the Chfr gene in neoplastic and non-neoplastic gastric epithelia. British Journal of Cancer, 90(10), 2013–2016.
Kang, H. C., Kim, I. J., Park, J. H., Shin, Y., Park, H. W., Ku, J. L., et al. (2004). Promoter hypermethylation and silencing of CHFR mitotic stress checkpoint gene in human gastric cancers. Oncology Reports, 12(1), 129–133.
Cheung, H. W., Ching, Y. P., Nicholls, J. M., Ling, M. T., Wong, Y. C., Hui, N., et al. (2005). Epigenetic inactivation of CHFR in nasopharyngeal carcinoma through promoter methylation. Molecular Carcinogenesis, 43(4), 237–245.
Hutajulu, S. H., Indrasari, S. R., Indrawati, L. P., Harijadi, A., Duin, S., Haryana, S. M., et al. (2011). Epigenetic markers for early detection of nasopharyngeal carcinoma in a high risk population. Molecular Cancer, 10, 48.
Morioka, Y., Hibi, K., Sakai, M., Koike, M., Fujiwara, M., Kodera, Y., et al. (2006). Aberrant methylation of the CHFR gene in digestive tract cancer. Anticancer Research, 26(3A), 1791–1795.
Sakai, M., Hibi, K., Kanazumi, N., Nomoto, S., Inoue, S., Takeda, S., et al. (2005). Aberrant methylation of the CHFR gene in advanced hepatocellular carcinoma. Hepato-Gastroenterology, 52(66), 1854–1857.
Tozawa, T., Tamura, G., Honda, T., Nawata, S., Kimura, W., Makino, N., et al. (2004). Promoter hypermethylation of DAP-kinase is associated with poor survival in primary biliary tract carcinoma patients. Cancer Science, 95(9), 736–740.
Ogi, K., Toyota, M., Mita, H., Satoh, A., Kashima, L., Sasaki, Y., et al. (2005). Small interfering RNA-induced CHFR silencing sensitizes oral squamous cell cancer cells to microtubule inhibitors. Cancer Biology & Therapy, 4(7), 773–780.
Baba, S., Hara, A., Kato, K., Long, N. K., Hatano, Y., Kimura, M., et al. (2009). Aberrant promoter hypermethylation of the CHFR gene in oral squamous cell carcinomas. Oncology Reports, 22(5), 1173–1179.
van Doorn, R., Zoutman, W. H., Dijkman, R., de Menezes, R. X., Commandeur, S., Mulder, A. A., et al. (2005). Epigenetic profiling of cutaneous T-cell lymphoma: promoter hypermethylation of multiple tumor suppressor genes including BCL7a, PTPRG, and p73. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology, 23(17), 3886–3896.
Chen, K., Sawhney, R., Khan, M., Benninger, M. S., Hou, Z., Sethi, S., et al. (2007). Methylation of multiple genes as diagnostic and therapeutic markers in primary head and neck squamous cell carcinoma. Archives of Otolaryngology–Head & Neck Surgery, 133(11), 1131–1138.
Acknowledgments
This work was performed within the framework of CTMM, the Center for Translational Molecular Medicine, project DeCoDe (grant 03O-101). SD is financially supported by the Dutch Cancer Society (VU 2012-5351). JB is supported by the Department of Veterans Affairs Career Development Award-2 (7IK2BX001283-2).
Conflict of interest
JH is consultant for MDx Health and receives research funding from MDx Health.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
About this article
Cite this article
Derks, S., Cleven, A.H.G., Melotte, V. et al. Emerging evidence for CHFR as a cancer biomarker: from tumor biology to precision medicine. Cancer Metastasis Rev 33, 161–171 (2014). https://doi.org/10.1007/s10555-013-9462-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10555-013-9462-4