
Abstract
A 73-year-old male was admitted because of recurrent syncope. He was diagnosed with transient bradycardia caused by a 2:1 atrioventricular block, and he underwent cardiac computed tomography (CT) using 320 detector-row CT to screen for coronary artery disease. Significant coronary artery stenosis was not detected, but diffuse late iodinate enhancement was found on the epi-myocardium and endo-myocardium of the interventricular septum, and endo-myocardium of the anterior and lateral left ventricular (LV) myocardium (LVM) on CT. The ejection fraction and global longitudinal strain (LS) of LVM were 53.97% and − 9.87% on CT. Apical sparing was present, meaning the LS of LV apical segments were preserved compared with basal segments on CT. Pathological findings of LVM demonstrated loss of myocardial cells and extra-cellular amyloid deposition on the direct fast scarlet staining. He was finally diagnosed with transthyretin amyloidosis.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
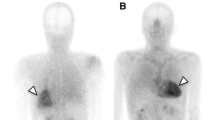
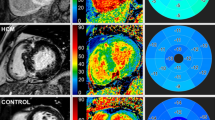
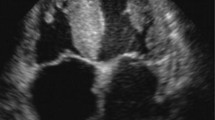
A 73-year-old male was admitted because of recurrent syncope. He was diagnosed with transient bradycardia caused by a 2:1 atrioventricular block, and he underwent cardiac computed tomography (CT) using 320 detector-row CT (Aquilion ONE/ViSION Edition, Canon Medical Systems, Japan) to screen for coronary artery disease. We performed a non-contrast scan using a prospective electrocardiography (ECG) gating technique and an early-phase scan using a retrospective ECG gating technique for the precise evaluation of coronary arteries [1]. A late-phase scan using a prospective ECG gating technique was performed six minutes after the injection of contrast media. Contrast material was injected using a triphasic protocol as described previously. During the first contrast phase, we injected 70 mL of undiluted iodinated contrast agent (370 mg/mL) at four mL/s, followed by 50 mL of a 50%/50% saline-to-contrast material mixture at four mL/s and 16 mL of pure saline at two mL/s, intravenously [1]. Significant coronary artery stenosis was not detected (Figure A), but diffuse late iodinate enhancement was found on the epi-myocardium and endo-myocardium of the interventricular septum (Figure B - D), and endo-myocardium of the anterior and lateral left ventricular (LV) myocardium (LVM) on CT. The ejection fraction and global longitudinal strain (LS) of LVM were calculated using a new software (Medis Suite CT QStrain 4.2, Medis Medical Imaging, The Netherlands and they were 53.97% and − 9.87% (Figures E - G) (The polar map of LS was presented according to the 17 LVM segments model of the American Heart Association [AHA]). Apical sparing was present, meaning preserved LS of LV apical segments compared with basal segments on CT. LS of LVM was also evaluated using transthoracic echocardiography (Figure H) (The LVM segments of the polar maps for LS were presented with slightly rotated positioning from the 17 LVM segments model of the AHA). Pathological findings of LVM demonstrated loss of myocardial cells and extra-cellular amyloid deposition on the direct fast scarlet staining (Figure 1). He was finally diagnosed with transthyretin amyloidosis.

(A) Significant coronary artery stenosis was not detected on computed tomography (CT). (B–D) Diffuse late iodinate enhancement was found on the epi-myocardium and endo-myocardium of the interventricular septum, and endo-myocardium of the anterior and lateral left ventricular (LV) myocardium (LVM) on CT. (E–G) The ejection fraction and global longitudinal strain (LS) of LVM were calculated using new software (Medis Suite CT QStrain 4.2, Medis Medical Imaging, The Netherlands), and they were 53.97% and − 9.87%. Apical sparing was present, meaning the LS of LV apical segments was preserved compared with basal segments on CT (The polar map of LS was presented according to the 17 LVM segments model of the American Heart Association [AHA]). (H) LS of LVM was also evaluated using transthoracic echocardiography (The LVM segments of the polar maps for LS were presented with slightly rotated positioning from the 17 LVM segments model of the AHA). (I) Pathological findings of LVM demonstrated loss of myocardial cells and extra-cellular amyloid deposition on the direct fast scarlet staining
Scanning images in a whole cardiac phase differs from the usual protocol of cardiac CT, but scanning images in an entire cardiac phase becomes necessary in cases of arrhythmia. Myocardial strain analysis has been available on CT, and a good correlation was reported between the strain data on CT and echocardiography [2]. Apical sparing is a typical abnormality in patients with cardiac amyloidosis [3]. Furthermore, recent technological innovations in CT equipment have made it possible to significantly reduce radiation doses during cardiac imaging, even with complete cardiac cycle acquisition [4].
References
Takaoka H, Funabashi N, Uehara M, Fujimoto Y, Kobayashi Y (2013) Diagnostic accuracy of coronary 320 slice CT angiography using retrospective electrocardiogram gated acquisition compared with virtual prospective electrocardiogram gated acquisition with and without padding. Int J Cardiol 168:2811–2815
Bernhard B, Grogg H, Zurkirchen J, Demirel C, Hagemeyer D, Okuno T, et al (2022) Reproducibility of 4D cardiac computed tomography feature tracking myocardial strain and comparison against speckle-tracking echocardiography in patients with severe aortic stenosis. J Cardiovasc Comput Tomogr 16:309–318
Phelan D, Collier P, Thavendiranathan P, Popović ZB, Hanna M, Plana JC, et al (2012) Relative apical sparing of longitudinal strain using two-dimensional speckle-tracking echocardiography is both sensitive and specific for the diagnosis of cardiac amyloidosis. Heart 98:1442–1448
Chen CM, Liu YC, Chen CC, Wen MS, Hung CF, Wan YL (2012) Radiation dose exposure of patients undergoing 320-row cardiac CT for assessing coronary angiography and global left ventricular function. Int J Cardiovasc Imaging 28:1–5
Funding
This work was partially supported by the JSPS KAKENHI Grant Number JP23K11891.
Author information
Authors and Affiliations
Contributions
“M.K., H.T., and JI.I., wrote the main manuscript text. M.K., H.T., and JI.I., prepared figures A to H. The other authors critically reviewed and edited this manuscript. All authors reviewed the manuscript.”
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Disclosure
We have nothing to disclose related to this article.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kinoshita, M., Takaoka, H., Ota, J. et al. Four-dimensional computed tomography is useful for detection of apical sparing of cardiac amyloidosis. Int J Cardiovasc Imaging (2024). https://doi.org/10.1007/s10554-024-03127-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10554-024-03127-6