
Abstract
Objectives (i) To explore the relation between greyscale intravascular ultrasound (IVUS) plaque qualitative classification and IVUS radiofrequency data (RFD) analysis tissue types; (ii) to evaluate if plaque composition as assessed by RFD analysis can be predicted by visual assessment of greyscale IVUS images. Methods In 120 IVUS-RFD cross-sections, a sector of the plaque with homogenous tissue composition (e.g., fibrous, fibrofatty, necrotic core, and dense calcium) was selected. Two experienced observers analyzed twice the corresponding greyscale IVUS images to: (1) classify the selected sectors according to greyscale IVUS plaque type classification and (2) predict the tissue type expected in the sector by RFD analysis. Results In the greyscale IVUS plaque type classification, the observers agreed in 90/120 sectors (κ = 0.64). Calcified, soft and mixed plaques by greyscale IVUS classification were mainly composed of dense calcium, fibrofatty, and necrotic core, respectively, in the RFD analysis. The plaques classified in greyscale IVUS as fibrous were actually fibrous tissue by IVUS RFD in only 30% of the cases. Overall, high interobserver variability in the prediction of RFD results by visual assessment of greyscale IVUS images (κ = 0.23 for observer 1 and 0.55 for observer 2) was found. Sensitivities for detection of calcified tissue and NC by greyscale IVUS visual assessment were 88% and 58%, respectively. Conclusions High interobserver variability in the prediction of tissue type by visual assessment of greyscale IVUS images was observed. This underlines the need of quantitative methods for the analysis of the ultrasound characteristics of coronary plaque components.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Greyscale coronary intravascular ultrasound (IVUS) is a useful technique for the evaluation of the extent and distribution of coronary atherosclerotic plaques [1] but it has a lot of limitations for the identification of its tissue composition [2, 3]. Soft (echolucent) plaques have been related either to high lipid content [4–8] or presence of smooth muscle cells [9]. While fibrous plaques usually have an intermediate echogenicity, but sometimes very dense fibrous plaques can also appear as calcified lesions [10]. Traditionally, acoustic shadowing has been considered as a sign of calcification, but necrotic tissue can also cause shadowing [9]. These limitations of the greyscale IVUS visual plaque assessment have lead to the development of quantitative techniques for analysis of the ultrasound characteristics of plaque components such as the automated echogenicity analysis of IVUS images [9] or the spectral analysis of IVUS radiofrequency data (RFD). This last technology allows the identification of four tissue types [11, 12] and it has been validated with histopathology ex vivo and in vivo showing high predictive accuracies [13, 14]. Due to its high accuracy and bearing in mind that it can only be a surrogate of pathology, we have used RFD analysis for tissue identification in the present study.
So far, to our knowledge, there are no studies comparing the relation between tissue composition by RFD analysis and greyscale IVUS visual assessment. The objective, of this study was two-fold: (i) to explore the relation between the greyscale IVUS plaque qualitative classification and the IVUS RFD analysis tissue types; (ii) to evaluate if the plaque composition as assessed by RFD analysis can be predicted by visual assessment of greyscale IVUS images.
Methods
Study population
Patients older than 18 years admitted to our hospital for cardiac catheterization due to stable angina or an acute coronary syndrome in whom IVUS with RFD acquisition was performed in a non-treated vessel were included. Informed written consent was signed by all the patients.
IVUS imaging protocol
For IVUS acquisition the Eagle Eye 20 MHz catheter (Volcano Corporation, Rancho Cordova, USA) and a dedicated console were used. The IVUS examination was performed using an automatic continuous speed pullback at a rate of 0.5 mm/s. The image data was stored on DVD for off-line analysis.
RFD acquisition and analysis
Both greyscale and RFD were acquired during the same pullback. The IVUS RFD acquisition was gated to the peak R-wave. The processing of the RFD was performed with pcVH software, version 2.1, which allows a semi-automatic contour detection of the lumen and media-adventitia border. The borders were corrected manually for all cross sections. The spectral analysis of IVUS RFD classifies tissue components of the atherosclerotic plaque in four types and overlays a colour coded map [14]: fibrous tissue as detected by RFD (dark green) corresponds in pathology to densely packed bundles of collagen fibers with no evidence of intra-fiber lipid accumulation and without macrophage infiltration. Fibrofatty tissue by RFD (green light) identifies loosely packed bundles of collagen fibers and cells with high lipid content, without cholesterols clefts or necrosis areas. Necrotic core (NC) as detected by RFD (red) corresponds to lipid areas containing remnants of foam cells and dead lymphocytes, cholesterol clefts and microcalcifications. Dense calcium by RFD analysis (white) identifies focal areas of calcification in pathology.
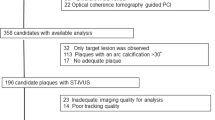
Selection and analysis of the areas of interest (Fig. 1)
Twenty-seven IVUS RFD pullbacks in non-stented vessels were included in this study. By evaluation of the IVUS RFD images, one independent analyst, (who did not participate in the final analysis), selected cross sections (CSS) that contained plaque areas with a homogeneous tissue composition of one of the four tissue types defined by RFD analysis (Fig. 1). An area was considered homogeneous when one tissue type represented more than 60% of its composition. These homogeneous areas were delimited inside a sector using dedicated in house developed software that allows selective analysis and quantification of the geometrical and compositional parameters (MATLAB MathWorks, Natick, MA). The angle of the sector, defined from the centre of gravity of the lumen, was variable depending on the size of the homogenous area. Eventually, 30 sectors for each type of tissue based on the RFD analysis were selected (Fig. 2). The corresponding 120 sectors in the greyscale IVUS images were categorized twice by two independent highly experienced observers. They were blinded for the observations of the other analyst and for the RFD processing results. For the first analysis, they categorized the plaque type in each sector, according to the greyscale IVUS plaque classification recommended in the IVUS Consensus Document of the American College of Cardiology: (1) soft plaque (lesion echogenicity less than the surrounding adventitia), (2) fibrous plaque [intermediate echogenicity between soft (echolucent) atheromas and highly echogenic calcified plaques], (3) calcified plaque (echogenicity higher than the adventitia with acoustic shadowing), and (4) mixed plaques (when they contain more than one acoustical subtype) [10]. One week later they analyzed again the greyscale IVUS sectors to guess the predominant tissue type (fibrous, fibrofatty, NC or dense calcium) expected in the RFD analysis of these greyscale images. They could only provide one tissue type per sector.

Flow-chart showing the areas of interest selection and analysis. By evaluation of the IVUS (intravascular ultrasound) radiofrequency data (RFD) images, one independent analyst selected cross sections that contained plaque areas with a homogeneous tissue composition of one of the four tissue types identified by RFD analysis (A). These homogeneous areas were delimited inside a sector (angle from the gravity center of the lumen, indicated by the red lines in A). In total, 30 sectors for each tissue type (fibrotic, fibrofatty, necrotic core, and dense calcium) based on the RFD analysis were selected. The corresponding sectors were identified in the greyscale (GS) images (indicated by the red lines in B). Eventually 120 GS sectors were analyzed by two observers

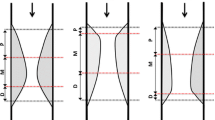
Examples of the sectors chosen for each tissue type. IVUS greyscale and the corresponding RFD analysis images are shown. The red lines indicate the sector selected for the analysis. (a) fibrous tissue, (b) fibrofatty tissue, (c) necrotic core, and (d) dense calcium
Statistical analysis
Data are expressed as percentages for categorical variables. Agreement between observers was measured by calculating the κ-value that takes into account the proportion of agreements occurring by chance. A negative value of κ indicate a worse than chance agreement, a value of zero indicates agreement no better than chance, and a value of 1 indicates perfect agreement [15]. Comparison of the IVUS RFD analysis data and the observers’ classification was made by calculating the sensitivity, specificity, and global accuracy for each tissue type.
Results
The mean age of the population was 58 ± 12 years, 87% were males. Regarding the clinical presentation, 56% of the patients were admitted to the hospital due to ST elevation myocardial infarction, 13% presented with non-ST elevation myocardial infarction and 31% with stable angina.
The interrogated vessel was the LAD in 44%, the LCX in 19% and the RCA in 37% of the patients. In the selected 120 CSS, the mean vessel and lumen cross sectional areas were 18.4 ± 5.8 mm2 and 8.9 ± 3.5 mm2, respectively, with a plaque burden of 51 ± 11%. The median angle of the analyzed sectors was 51 degrees.
Greyscale IVUS classification
Observer 1 classified the sectors as fibrous in 12.5%, calcified in 20%, soft in 55% and mixed in 12.5% of the cases. Whereas observer 2, classified them as fibrous in 21%, calcified in 23%, soft in 38% and mixed in 18% of the cases. The two observers agreed on 90 out of 120 sectors (κ = 0.64). The maximum level of concordance was on the classification of the calcified sectors, while the lower level of concordance was observed in the fibrous sectors (Table 1).
Relation between greyscale IVUS plaque classification and IVUS RFD analysis tissue types
Of the 90 sectors in which there was agreement between the two observers, ten were classified as fibrous, 23 as calcified, 46 as soft and 11 as mixed. The ten fibrous sectors by greyscale (as classified by two observers) were composed of fibrous tissue in RFD analysis in only 3/10 (30%). The 23 calcified were constituted by dense calcium in RFD analysis in 16/23 (70%) of the cases. The soft sectors were composed more commonly of fibrofatty tissue in 29/46 (63%), and lastly the mixed sectors were constituted mainly by NC core in 9/11 (82%) (Table 2).
Prediction of the tissue type expected in RFD analysis by qualitative assessment of greyscale IVUS
When predicting the tissue type expected by RFD analysis, observer 1 classified the 120 greyscale sectors as follows: 37% fibrous, 25% dense calcium, 19% NC and 19% fibrofatty tissue; a total of 51 sectors were correctly classified when compared to RFD analysis (κ = 0.23). While observer 2 classified them as fibrous in 22%, dense calcium in 22%, NC in 23%, and fibrofatty in 33% of the cases. A total of 82 sectors were correctly classified when compared with RFD analysis (κ = 0.55) (Table 3).
The two observers classified similarly 44/120 sectors, which was 36.7% of concordance (κ = 0.16). These 44 sectors were classified by both analysts as fibrous in 15.8%, dense calcium in 45.5%, NC in 27.3%, and fibrofatty in 11.4% of the cases. Thirty out of these 44 sectors were correctly categorized according to IVUS RFD (κ = 0.53) (Table 3). A high sensitivity for the detection of calcified tissue by greyscale IVUS visual assessment was observed (88%), while the sensitivity for the other three types of tissue, (50%, 50%, and 58% for fibrous, fibrofatty, and NC, respectively) was lower. The specificity of the two observers was above 80% for all the tissues. The global predictive accuracy was also above 80% for fibrous, fibrofatty, and dense calcium, while for the NC was 79% (Table 4).
Discussion
In the present study the main findings were: (1) For the greyscale IVUS classification, the agreement between observers was high (κ = 0.64). (2) Calcified, soft and mixed plaques by greyscale IVUS classification were mainly composed of dense calcium, fibrofatty and NC respectively in the RFD analysis. The plaques classified in greyscale IVUS as fibrous were actually fibrous tissue by IVUS RFD in only 30% of the cases. (3) Overall, high interobserver variability in the prediction of RFD results by visual assessment of greyscale images (κ = 0.23 for observer 1 and 0.55 for observer (2) was obtained. (4) Sensitivity for detection of calcified tissue by greyscale IVUS visual assessment was high while for NC was low.
Greyscale IVUS variability for plaque type identification
The interobserver variability in the plaque type assessment by greyscale IVUS reported in the literature varies considerably, with percentages of concordance between observers ranging from 88% to only 47% [16–18]. In the present study a good agreement was found.
Specifically, the best agreement was in the classification of the calcified plaques (82%). This is in line with the results of Palmer et al. [16], who reported an interobserver concordance of 87% for this type of plaques. This high level of agreement can be explained because the IVUS features for calcification (high echoreflectivity with acoustic shadowing and reverberations) are well defined and easier to identify in greyscale IVUS.
Greyscale IVUS plaque classification and IVUS RFD analysis relationship
The sensitivity for the detection of fibrous and fibrofatty tissue by greyscale IVUS visual assessment was low (around 50%) in the present study. The plaques classified as soft by the observers were composed of fibrofatty tissue in 29/46 but 16/46 were fibrous tissue by RFD analysis. This is in concordance with histological examinations that showed low sensitivity of greyscale IVUS compared with pathology in discriminating fibrous and fatty tissue, 50% and 40%, respectively [19]. In another in-vitro study that compared 104 matching intracoronary ultrasound images and histological cross-sections, the sensitivity to detect lipid deposits was only 46% [20].
These findings are of clinical relevance, because soft plaques have been related to acute coronary syndromes [18, 21] and in this study these happen to be constituted mainly by fibrous and fibrofatty tissue and not by NC which is the substrate of the ruptured plaques.
Prediction of the tissue type expected in RFD analysis by qualitative assessment of greyscale IVUS
The individual prediction of RFD results by visual assessment of greyscale IVUS images was low and the interobserver variability was high (the κ value ranged from 0.23 for observer 1 to 0.56 for observer 2). Collectively, when the two observers agreed on IVUS RFD classification, they could predict the results of the RFD analysis in 56% of the cases (κ = 0.53). However, the accuracy of the greyscale IVUS visual assessment to predict the type of tissue depends highly on the plaque type [22]. In our study, the observers had the best sensitivity (88%) with 81% specificity for the detection of dense calcium. Detection of calcium depends on the histological pattern, but with the exception of multiple scattered microcalcification, greyscale IVUS analysis can be considered highly specific and sensitive for the detection of calcium in a plaque [3]. Indeed, other postmortem studies have demonstrated 90% sensitivity and 100% specificity for the detection of dense calcified plaques [16, 23]. Nevertheless, it is striking that 30% of the plaques classified as calcified by the two observers in our study were composed predominantly of NC in the RFD analysis. This is a learning point from this study: not all the greyscale IVUS “calcified-looking” plaques were dense calcium in IVUS RFD, but roughly one out of three sectors was NC. This misclassification may be due to the fact that sometimes NC areas are hyperechogenic and can cause some acoustic shadowing [9].
In our study, the sensitivity of the observers for the detection of the NC was low (58%). This has also been previously reported, the NC could not be characterized by greyscale IVUS visual assessment [13]. The possible explanation is the heterogeneous pathological nature of the NC that translates into a mixed appearance in greyscale IVUS. In fact, NC composition combines lipid necrotic areas, with foam cells and dead lymphocytes, cholesterol clefts and microcalcifications [14]. Indeed, when the NC was the main component of the plaque, it was classified by the two observers mainly as mixed plaque (43%) in our study. This highlights the necessity of a more specific tissue characterization by a dedicated imaging technique such as IVUS RFD analysis.
Limitations
IVUS RFD analysis has demonstrated in ex vivo and in vivo human coronary comparisons with histological specimens, high predictive accuracies. Nevertheless, it is only a surrogate of pathology for tissue identification. The choosen criterion of 60% homogeneity by RFD may have introduced an important bias in this analysis, as plaques could be indeed rather heterogeneous. We acknowledge that further analysis with a more strict (of different) criterion for homogeneity by RFD may find different correlation and variability between RFD and GS. It is clear that IVUS RFD technology may offer better qualitative and quantitative tissue characterization than GS IVUS, but its definite role is yet to be determined.
Conclusions
High interobserver variability in the prediction of tissue type by visual assessment of greyscale IVUS images was observed. This underlines the need of quantitative methods for the analysis of the ultrasound characteristics of plaque components.
Abbreviations
- CSS:
-
Cross sections
- IVUS:
-
Intravascular ultrasound
- NC:
-
Necrotic core
- RFD:
-
Radiofrequency data
References
Rasheed QDP, Anderson J, Hodgson JM (1995) Intracoronary ultrasound-defined plaque composition: computer-aided plaque characterization and correlation with histologic samples obtained during directional coronary atherectomy. Am Heart J 129:631–637. doi:10.1016/0002-8703(95)90307-0
Di Mario CTS, Madretsma S, van Suylen RJ et al (1992) Detection and characterization of vascular lesions by intravascular ultrasound: an in vitro study correlated with histology. J Am Soc Echocardiogr 5:135–146
Di Mario C, Gorge G, Peters R et al (1998) Clinical application and image interpretation in intracoronary ultrasound. Study Group on Intracoronary Imaging of the Working Group of Coronary Circulation and of the Subgroup on Intravascular Ultrasound of the Working Group of Echocardiography of the European Society of Cardiology. Eur Heart J 19:207–229. doi:10.1053/euhj.1996.0433
Honda O, Sugiyama S, Kugiyama K et al (2004) Echolucent carotid plaques predict future coronary events in patients with coronary artery disease. J Am Coll Cardiol 43:1177–1184. doi:10.1016/j.jacc.2003.09.063
Gronholdt ML (1999) Ultrasound and lipoproteins as predictors of lipid-rich, rupture-prone plaques in the carotid artery. Arterioscler Thromb Vasc Biol 19:2–13
Prati F, Arbustini E, Labellarte A et al (2001) Correlation between high frequency intravascular ultrasound and histomorphology in human coronary arteries. Heart 85:567–570. doi:10.1136/heart.85.5.567
Wickline SA (2004) Plaque characterization: surrogate markers or the real thing? J Am Coll Cardiol 43:1185–1187. doi:10.1016/j.jacc.2004.01.009
DeMaria AN, Narula J, Mahmud E et al (2006) Imaging vulnerable plaque by ultrasound. J Am Coll Cardiol 47(Suppl 8):C32–C39. doi:10.1016/j.jacc.2005.11.047
Bruining N, Verheye S, Knaapen M et al (2007) Three-dimensional and quantitative analysis of atherosclerotic plaque composition by automated differential echogenicity. Catheter Cardiovasc Interv 70:968–978. doi:10.1002/ccd.21310
Mintz GS, Nissen SE, Anderson WD et al (2001) American College of Cardiology Clinical Expert Consensus Document on Standards for Acquisition, Measurement and Reporting of Intravascular Ultrasound Studies (IVUS). A report of the American College of Cardiology Task Force on Clinical Expert Consensus Documents. J Am Coll Cardiol 37:1478–1492. doi:10.1016/S0735-1097(01)01175-5
Rodriguez-Granillo GA, Garcia-Garcia HM, Wentzel J et al (2006) Plaque composition and its relationship with acknowledged shear stress patterns in coronary arteries. J Am Coll Cardiol 47:884–885. doi:10.1016/j.jacc.2005.11.027
Rodriguez-Granillo GA, Vaina S, Garcia-Garcia HM et al (2006) Reproducibility of intravascular ultrasound radiofrequency data analysis: implications for the design of longitudinal studies. Int J Cardiovasc Imaging 22:621–631. doi:10.1007/s10554-006-9080-0
Nasu K, Tsuchikane E, Katoh O et al (2006) Accuracy of in vivo coronary plaque morphology assessment: a validation study of in vivo virtual histology compared with in vitro histopathology. J Am Coll Cardiol 47:2405–2412. doi:10.1016/j.jacc.2006.02.044
Nair A, Margolis P, Kuban BD et al (2007) Automated coronary plaque characterization with intravascular ultrasound backscatter: ex vivo validation. Eurointervention 3:113–130
Munoz SR (1997) Interpretation of kappa and B-statistics measures of agreement. J Appl Stat 24:105–111. doi:10.1080/02664769723918
Palmer ND, Northridge D, Lessells A et al (1999) In vitro analysis of coronary atheromatous lesions by intravascular ultrasound; reproducibility and histological correlation of lesion morphology. Eur Heart J 20:1701–1706. doi:10.1053/euhj.1999.1627
Hiro T, Leung CY, Russo RJ et al (1996) Variability in tissue characterization of atherosclerotic plaque by intravascular ultrasound: a comparison of four intravascular ultrasound systems. Am J Card Imaging 10:209–218
Hodgson JM, Reddy KG, Suneja R et al (1993) Intracoronary ultrasound imaging: correlation of plaque morphology with angiography, clinical syndrome and procedural results in patients undergoing coronary angioplasty. J Am Coll Cardiol 21:35–44
Hiro T, Leung CY, De Guzman S et al (1997) Are soft echoes really soft? Intravascular ultrasound assessment of mechanical properties in human atherosclerotic tissue. Am Heart J 133(1):1–7. doi:10.1016/S0002-8703(97)70241-2
Peters RJ, Kok WE, Havenith MG et al (1994) Histopathologic validation of intracoronary ultrasound imaging. J Am Soc Echocardiogr 7:230–241
Yamagishi M, Terashima M, Awano K et al (2000) Morphology of vulnerable coronary plaque: insights from follow-up of patients examined by intravascular ultrasound before an acute coronary syndrome. J Am Coll Cardiol 35:106–111. doi:10.1016/S0735-1097(99)00533-1
Potkin BN, Bartorelli AL, Gessert JM et al (1990) Coronary artery imaging with intravascular high-frequency ultrasound. Circulation 81:1575–1585
Friedrich GJ, Moes NY, Muhlberger VA et al (1994) Detection of intralesional calcium by intracoronary ultrasound depends on the histologic pattern. Am Heart J 128:435–441. doi:10.1016/0002-8703(94)90614-9
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Gonzalo, N., García-García, H.M., Ligthart, J. et al. Coronary plaque composition as assessed by greyscale intravascular ultrasound and radiofrequency spectral data analysis. Int J Cardiovasc Imaging 24, 811–818 (2008). https://doi.org/10.1007/s10554-008-9324-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10554-008-9324-2