
Abstract
Serum copper (Cu) and zinc (Zn), essential micronutrients that have important immunomodulatory and antimicrobial properties, are biomarkers of ageing. Serum Cu/Zn-ratio may be a more reliable marker for age-related degenerative conditions compared with serum Cu or Zn alone. We aimed to assess the association between Cu/Zn-ratio and the risk of incident pneumonia in a prospective cohort study. Serum levels of Cu and Zn were measured at baseline using atomic absorption spectrometry in 2503 men aged 42–61 years in the Kuopio Ischemic Heart Disease prospective cohort study. Hazard ratios (HRs) with confidence intervals (CIs) were calculated for incident pneumonia using Cox regression models. A total of 599 cases of pneumonia occurred during a median follow-up of 26.1 years. Serum Cu/Zn-ratio and Cu were each linearly associated with incident pneumonia. A unit increase in Cu/Zn-ratio was associated with an increased risk of pneumonia in analysis adjusted for potential confounders including C-reactive protein (HR 1.65; 95% CI 1.17–2.33). The corresponding adjusted HR (95% CI) was 2.04 (1.22–3.40) for serum Cu. The association between serum Zn and pneumonia was curvilinear. Compared to the bottom tertile of Zn, the multivariable adjusted HRs (95% CIs) for incident pneumonia were 0.68 (0.55–0.83) and 0.96 (0.79–1.16) for the middle and top tertiles of Zn, respectively. Further analysis in the same participants showed that Cu/Zn-ratio might be a stronger risk indicator for pneumonia than serum C-reactive protein. In middle-aged and older Finnish men, increased serum Cu/Zn-ratio and Cu concentrations are each linearly associated with an increased risk of incident pneumonia.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pneumonia, an inflammatory condition of the lung tissue commonly caused by bacteria or viruses, can be acquired in the community (community acquired pneumonia, CAP) or in the hospital environment (hospital acquired pneumonia). (Cilloniz et al. 2016b) Community-acquired pneumonia is a leading cause of hospitalization, morbidity, mortality, and associated with significant health care costs. (Nair and Niederman 2011)The Global Burden of Disease Study 2019 reported that lower respiratory infections ranked as the fourth leading cause of disability-adjusted life-years. (GBD Collaborators 2020) Despite the development of newer molecular tests for microbial identification of pathogens, pulmonary imaging facilities and antimicrobial therapies for the management of pneumonia over the last decade, the incidence of pneumonia persistently remains high. (Cillóniz et al. 2018) Major contributors to the growing incidence of pneumonia include increased life expectancy, smoking, excessive alcohol consumption, respiratory conditions such as asthma and chronic obstructive pulmonary disease (COPD), other chronic conditions such as diabetes, kidney and liver disease, and immunosuppression. Cillóniz and others 2018; Nair and Niederman 2011).
Though pneumonia constitutes a substantial global public health burden, it is a preventable cause of death and disability. Older age is a major risk factor for pneumonia, (Torres et al. 2013) which is a leading cause for hospitalization and subsequent mortality among this population group. (Jackson et al. 2004) This is due to the physiological changes associated with aging such as age-related weakening of the immune system (immunosenescence)(Haase and Rink 2009) as well as the high prevalence of chronic disease in older people. (Cilloniz et al. 2016a) With increasing life expectancy, there is increasing research focussed on identifying biomarkers of ageing,(Engelfriet et al. 2013) which could be clinically relevant for preventing aging-related diseases such as pneumonia. Copper (Cu) and zinc (Zn), essential micronutrients involved in several cellular processes such as nucleic acid synthesis, enzymatic reactions, oxidoreductases, inflammation, mitochondrial electron transport, cell replication and repair,(Chimienti 2013; Festa and Thiele 2011) have been identified as biomarkers related to aging as they appear to be mostly related to inflammatory parameters than the nutritional ones. (Malavolta et al.2010) They have important immunomodulatory and antimicrobial properties(Malavolta et al. 2015) and are relevant for the development, regulation and maintenance of the immune and antioxidative defence system. (Stafford et al. 2013) Copper is involved in various biological processes, and its insufficiency, deficiency, or toxic levels can lead to many disease states. (DiNicolantonio et al. 2018) Zinc deficiency contributes to frailty, disability and an increased incidence of age-related degenerative diseases such as cancer, infections and atherosclerosis. (Mocchegiani 2007).
Among serum micronutrients, concentrations of Cu and Zn are strictly regulated by compensatory mechanisms that act to stabilize them within certain ranges of nutritional intake.(Malavolta et al. 2015) Serum concentrations of Cu and Zn are only slightly affected by nutritional changes unless during severe deficiency or supplementation use.(Malavolta et al. 2015) However, in the presence of pathological changes such as inflammatory conditions, there is a decrease in serum Zn concentrations and an increase in serum Cu concentrations, and thus they are biologically interrelated.(Sullivan et al. 1979) The typical presentation of several age-related chronic diseases is an increase in the Cu-to-Zn ratio (Cu/Zn-ratio).(Malavolta et al. 2015) It has been suggested that the serum Cu/Zn-ratio may be a more reliable marker of pathological outcomes, compared to the use of Cu or Zn alone.(Malavolta et al. 2015) High serum Cu/Zn-ratio has been shown to be associated with an increased risk of cardiovascular mortality, (Leone et al. 2006) cancer, (Leone et al. 2006) all-cause mortality(Malavolta et al. 2010) as well as infectious disease. (Laine et al. 2020) Though the previous study by Laine and colleagues evaluated infection outcomes, the specific outcome of pneumonia was not assessed. (Laine et al. 2020) To our knowledge, the prospective association between serum Cu/Zn-ratio and the risk of the specific outcome of pneumonia has not been previously explored. Our principal aim was to assess the nature and magnitude of the prospective association of serum Cu/Zn-ratio with pneumonia risk, using a population-based prospective cohort of 2503 middle-aged and older Finnish men. A secondary aim was to assess the individual associations of serum Cu and Zn with incident pneumonia risk. Furthermore, given that C-reactive protein (CRP) is a major inflammatory marker, we also evaluated the association of serum high sensitivity CRP (hsCRP) with pneumonia risk in the same set of participants to make comparisons.
Methods
This study was conducted in accordance with STROBE (STrengthening the Reporting of OBservational studies in Epidemiology) guidelines for reporting observational studies in epidemiology (Supplementary File 1).
Study design and participants
The Research Ethics Committee of the University of Kuopio approved the study protocol and each study participant provided written informed consent. All study procedures adhered to the Declaration of Helsinki. Participants included in this study were part of the Kuopio Ischaemic Heart Disease Risk Factor Study (KIHD), a population-based prospective cohort study that was set up to investigate risk factors for atherosclerotic cardiovascular disease and other related diseases. The study design and recruitment methods have been described in detail in previous reports. (Kunutsor et al. 2016b, c; Laukkanen et al. 2018) Briefly, participants included in the KIHD comprised a representative sample of men aged 42, 48, 54 or 60 years living in the city of Kuopio and its surrounding rural communities in eastern Finland. During recruitment, a total of 3433 men were potentially eligible and of these, 3235 were found to be eligible for inclusion into study. Of this number, 2682 volunteered to participate and 553 did not respond to the invitation or declined to give informed consent. Baseline examinations were performed between March 1984 and December 1989. From this analysis, we excluded those with missing data on the exposures and potential confounders (n = 179). The current analysis included 2503 men with complete information on serum measurements of Cu and Zn, relevant covariates, and incident pneumonia events.
Measurement of covariates and outcome ascertainment
Blood sample collection and measurement of blood biomarkers, physical measurements, and assessment of lifestyle characteristics, medical history and dietary intakes have been described in detail in previous reports. (Abdollahi et al. 2019; Kunutsor and others 2016a; Kunutsor and Laukkanen 2016; Salonen et al. 1992) Participants fasted overnight and abstained from drinking alcohol for at least 3 days and from smoking for at least 12 h before blood samples were taken between 8 and 10 a.m. Serum hsCRP measurements were made with an immunometric assay (Immulite High Sensitivity C-Reactive Protein Assay; DPC, Los Angeles, CA, USA). Measurements of serum Cu and Zn concentrations were made from frozen serum samples stored at −20° C for 1–5 years, using the PerkinElmer 306 atomic absorption spectrophotometer (Norwalk, Connecticut, USA). Self-administered questionnaires were used to assess medical history and lifestyle characteristics such as smoking and alcohol consumption. (Salonen et al. 1992) Socioeconomic status (SES) was assessed using self-reported questionnaires via a summary index that combined income, education, occupational prestige, material standard of living and housing conditions. The composite SES index ranged from 0 to 25, with higher values indicating lower SES. (Jae et al. 2020) The consumption of foods was assessed with the use of a 4-day guided food record, during three weekdays and one weekend day using household measures. Instructions were provided and completed food records were checked by a nutritionist together with the participant, to ensure accuracy. Leisure-time physical activity was assessed from a 12 month physical activity history modified from the Minnesota Leisure-Time Physical Activity Questionnaire. (Taylor et al. 1978).
Incident cases of pneumonia that occurred from study entry to 2018 were included in this analysis. The diagnoses of pneumonia cases were made by qualified physicians based on the International Classification of Diseases (ICD) codes used in clinical practice (ICD-8 codes 485; ICD-9 codes 480–483, and 485; ICD-10 codes J15, and J18) and were collected by linkage to the National Hospital Discharge Register (THL/93/5.05.00/2013). (Kunutsor et al. 2016a; Kunutsor et al. 2016b).
Statistical analysis
Variables with skewed distributions (e.g., alcohol consumption, physical activity, and hsCRP) were natural log transformed to achieve approximately symmetrical distributions. Baseline characteristics were presented as means ± standard deviation (SD) or median (interquartile range, IQR) for continuous variables and n (percentages) for categorical variables. In linear regression models adjusted for age, Pearson correlation coefficients were calculated to assess the cross-sectional associations of serum Cu/Zn-ratio with various continuous risk markers; for categorical variables, the percentage differences in mean values of serum Cu/Zn-ratio for a category versus its reference were calculated. Hazard ratios (HRs) with 95% confidence intervals (CIs) for incident pneumonia were estimated using Cox proportional hazard models and these were adjusted for in three models: (Model 1) age; (Model 2) Model 1 plus body mass index (BMI), smoking status, history of type 2 diabetes, prevalent coronary heart disease (CHD), history of asthma, history of chronic bronchitis, history of tuberculosis, alcohol consumption, SES, leisure-time physical activity, total energy intake, intake of fruits, berries and vegetables, and intake of processed and unprocessed red meat; and (Model 3) Model 2 plus hsCRP (a potential mediator of the association). The selected confounders were based on their previously established roles as risk factors for pneumonia, evidence from previous research, or their potential as confounders based on known associations with incident pneumonia and observed associations with the exposures using the available data. (Groenwold et al. 2011) To explore potential nonlinear dose–response relationships between the exposures and incident pneumonia risk, we constructed multivariable restricted cubic splines (RCSs) with knots at the 5th, 35th, 65th, and 95th percentiles of the distribution of the exposures as recommended by Harrell. (Harrell 2001) Serum Cu/Zn-ratio and Cu were modeled as both continuous (per unit increase) and categorical (tertiles) variables given evidence of linear relationships with pneumonia risk using multivariable RCS curves; serum Zn was modeled as tertiles given evidence of a nonlinear relationship. We constructed Kaplan–Meier curves for tertiles of serum Cu/Zn-ratio and compared them using the log rank test. We used formal tests of interaction tests to assess statistical evidence of effect modification by clinically relevant characteristics. To minimize any bias due to reverse causation, sensitivity analysis involved excluding the first two years of follow-up. All statistical analyses were conducted using Stata version MP 17 (Stata Corp, College Station, Texas).
Results
Baseline characteristics
The overall mean (SD) age of study participants at recruitment was 53 (5) years. The means (SDs) of serum Cu/Zn-ratio, Cu and Zn were 1.21 (0.27), 1.11 (0.18) and 0.94 (0.12), respectively. Significant weak and positive correlations were observed between serum Cu/Zn-ratio and age, alcohol consumption, and SES; whereas, the correlation was stronger for hsCRP (r = 0.42). Significant weak and inverse correlations were observed with physical activity and intake of fruits, berries and vegetables. Values of serum Cu/Zn-ratio were significantly higher in men who smoked compared with men who did not smoke (Table 1).
Association of serum Cu/Zn-ratio with pneumonia
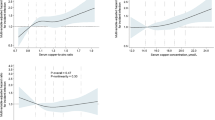
A total of 599 incident cases of pneumonia were recorded (annual rate 10.33/1000 person-years at risk; 95% CI 9.53–11.19) during a median (IQR) follow-up of 26.1 (16.7–30.8) years. A multivariable RCS curve showed that the risk of pneumonia increased linearly with increasing serum Cu/Zn-ratio across the range 1.50–3.10 (p-value for nonlinearity = 0.16) (Fig. 1A). The HR (95% CI) for incident pneumonia per unit increase in serum Cu/Zn-ratio was 2.07 (1.51–2.84) in analysis adjusted for age, BMI, smoking status, history of type 2 diabetes, prevalent CHD, history of asthma, chronic bronchitis or tuberculosis, alcohol consumption, SES, leisure-time physical activity, total energy intake, intake of fruits, berries and vegetables, and intake of processed and unprocessed red meat, which was attenuated to 1.65 (1.17–2.33) after further adjustment for hsCRP (Table 2). The corresponding adjusted HRs (95% CIs) were 1.32 (1.08–1.62) and 1.15 (0.92–1.42) comparing the top versus bottom tertiles of serum Cu/Zn-ratio. Cumulative hazard curves showed an increased risk of pneumonia among men in the top tertile of serum Cu/Zn-ratio compared with the other Cu/Zn-ratio groups (p-value for log-rank test < 0.001; Fig. 2).

Restricted cubic splines of the hazard ratios of incident pneumonia with serum Cu/Zn-ratio, Cu and Zn A Serum Cu/Zn-ratio and pneumonia; B Serum Cu and pneumonia; C Serum Zn and pneumonia Dashed lines represent the 95% confidence intervals for the spline model (solid line). Models were adjusted for age, body mass index, smoking status, history of type 2 diabetes, prevalent coronary heart disease, history of asthma, history of chronic bronchitis, history of tuberculosis, alcohol consumption, socioeconomic status, leisure-time physical activity, total energy intake, intake of fruits, berries and vegetables, and intake of processed and unprocessed red meat Cu, copper; Zn, zinc

Cumulative Kaplan–Meier curves for pneumonia during follow-up according to tertiles of serum Cu/Zn-ratio
Association of serum hsCRP with pneumonia
Direct comparisons were made to the association of serum hsCRP with pneumonia risk in the same set of participants. Serum hsCRP was independently associated with pneumonia risk (Supplementary File 2).
Association of serum Cu/Zn-ratio with pneumonia in subgroups
The association between serum Cu/Zn-ratio and pneumonia risk remained consistent across several clinically relevant subgroups except for marginal evidence of interaction by SES (p for interaction = 0.05); the association between serum Cu/Zn-ratio and pneumonia risk was strong and positive in men with low SES but was modest in men with high SES (Fig. 3).

Association between serum Cu/Zn-ratio and pneumonia risk across several clinically relevant subgroups CHD coronary heart disease; CI confidence interval; Cu copper; HR hazard ratio; Zn zinc
Associations of serum Cu and Zn with pneumonia
A multivariable RCS curve showed that the risk of pneumonia increased linearly with increasing serum Cu across the range 1.60–2.30 (p-value for nonlinearity = 0.36) (Fig. 1B). The HR (95% CI) for incident pneumonia per unit increase in serum Cu was 2.89 (1.83–4.56) in analysis adjusted for age, BMI, smoking status, history of type 2 diabetes, prevalent CHD, history of asthma, chronic bronchitis or tuberculosis, alcohol consumption, SES, leisure-time physical activity, total energy intake, intake of fruits, berries and vegetables, and intake of processed and unprocessed red meat, which was attenuated to 2.04 (1.22–3.40) following further adjustment for hsCRP (Table 2). The corresponding adjusted HRs (95% CIs) were 1.44 (1.18–1.77) and 1.25 (1.00–1.55) comparing the top versus bottom tertiles of serum Cu.
A multivariable RCS curve showed a curvilinear relationship between serum Zn and pneumonia risk (p-value for nonlinearity = 0.009) (Fig. 1C). Compared to the bottom tertile of Zn, the HRs (95% CIs) for incident pneumonia were 0.67 (0.55–0.82) and 0.94 (0.77–1.14) for the middle and top tertiles of Zn, respectively, in analysis that adjusted for age, BMI, smoking status, history of type 2 diabetes, prevalent CHD, history of asthma, chronic bronchitis or tuberculosis, alcohol consumption, SES, leisure-time physical activity, total energy intake, intake of fruits, berries and vegetables, and intake of processed and unprocessed red meat (Table 2). The respective HRs (95% CIs) were 0.68 (0.55–0.83) and 0.96 (0.79–1.16) in further analysis adjusted for hsCRP. The associations of serum Cu/Zn-ratio, Cu and Zn with risk of pneumonia remained similar in analyses that excluded the first two years of follow-up (Supplementary File 3).
Discussion
Key findings
In this prospective evaluation of the relationship between serum Cu/Zn-ratio and risk of incident pneumonia using a cohort of middle-aged and older Finnish men, elevated serum Cu/Zn-ratio was associated with an increased risk of incident pneumonia in a linear dose–response manner. The association did not differ across several clinically relevant subgroups, except for evidence of effect modification by SES; the association appeared to be stronger in men with low SES. In separate evaluations of serum Cu and Zn, Cu was positively associated with pneumonia in a linear dose–response manner, whereas serum Zn was inversely associated with pneumonia risk in a curvilinear manner. When serum Cu/Zn-ratio and Cu were modelled as categorical variables, the associations were attenuated on further adjustment for hsCRP, reflecting the fact that inflammatory pathways are involved in the development of pneumonia and hence confirms the fact that inflammation is a potential mediator of the observed association. Furthermore, correlation analysis demonstrated a strong positive correlation between serum Cu/Zn-ratio and hsCRP. If serum hsCRP is a potential mediator, then adjusting for it constitutes an overadjustment. Findings therefore suggest independent associations of serum Cu/Zn-ratio, Cu and Zn with pneumonia risk. Furthermore, the associations remained persistent when the first two years of follow-up were excluded. In further analysis that assessed the association of serum hsCRP with pneumonia risk in the same set of participants, a relatively weaker association was demonstrated in the analysis that modeled serum hsCRP as a continuous variable; which implies that serum Cu/Zn-ratio may be a stronger risk indicator than serum hsCRP for pneumonia risk.
Comparison with previous studies
To our knowledge, this is the first study to evaluate the prospective association between serum Cu/Zn-ratio and pneumonia risk, hence, we are unable to compare the current findings in the context of previous work. However, several epidemiological observational studies have demonstrated associations between serum Cu/Zn-ratio and several age-related degenerative conditions such as cardiovascular mortality (Leone et al. 2006; Reunanen and others 1996), HIV-1 mortality (Lai et al. 2001), cancer (Leone et al. 2006), knee chondrocalcinosis (He et al. 2020), and all-cause mortality (Malavolta et al. 2010). In a recent prospective evaluation, Laine and colleagues demonstrated an increased serum Cu/Zn-ratio and Cu concentration to be each associated with an increased risk of incident infections; there was no evidence of an association of Zn with incident infection, except when the analysis was limited to the first 10 years of follow-up (Laine et al. 2020). However, the outcome used in this evaluation comprised a comprehensive list of infectious conditions including intestinal infectious diseases, other bacterial diseases, viral diseases, diseases of the ear, other forms of heart disease, acute respiratory infections, influenza, pneumonia, diseases of the urinary system and male genital organs, and infections of skin and subcutaneous tissue. Though the commonest infection was pneumonia,(Laine et al. 2020) it is uncertain which specific outcome/outcomes could be driving the observed association, as estimates for cause-specific infections were not reported. In a number of case–control studies that were based on patients with bacterial, viral and parasitic infections, serum Cu/Zn-ratio was demonstrated to be a potential prognostic marker (Asemota et al. 2018; Kassu et al. 2006; Van Weyenbergh et al. 2004). Given that this is the first prospective study to evaluate the association between serum Cu/Zn-ratio and pneumonia, other large-scale prospective studies are still needed to confirm the current findings.
Explanations for findings
Several mechanistic pathways may underline the observed associations of serum Cu/Zn-ratio and Cu and Zn concentrations with the risk of incident pneumonia. In addition to their roles in almost every cellular process in the human body,(Chimienti 2013; Festa and Thiele 2011) Cu and Zn play important roles in the optimal functioning of the immune system. (Stafford et al. 2013) Though Cu plays a beneficial role in numerous biological processes, it can exhibit toxic effects in high amounts. High levels of Cu could increase the risk of infections such as pneumonia via increased inflammation, given its close relationship with ceruloplasmin, which is elevated during an acute phase response,(Uriu-Adams and Keen 2005) in addition to the ability of Cu to serve as a nutrient for infectious microbes. (Besold et al. 2016) For almost six decades, Zn has been known as an important factor for the immune system;(Prasad et al. 1963) its role in immune function has been consistently demonstrated in several cellular studies. (Haase and Rink 2014) The immune defence system relies on two major groups of cells (innate and adaptive immune cells), which also depend on Zn availability at multiple levels. (Wellinghausen et al. 1997) The major roles played by Zn in immunity include (i) signal transduction of immune cells; (ii) its impact on immune cell function such as suppression of several T cell-mediated immune reactions and formation of neutrophil extracellular traps; and (iii) “nutritional immunity”, a host response designed to starve pathogens of essential metals. (Haase and Rink 2014) Consequently, Zn deficiency leads to impaired immune function and an increased risk of infections. With advancing age, there is a decrease in serum Zn concentrations due to insufficient dietary Zn consumption, reduced intestinal absorption or increased losses (due to diarrhoea or use of diuretics) (Mocchegiani et al. 2013) and/or an increase in serum Cu concentrations (Baudry et al. 2020) due to the presence of inflammatory conditions commonly seen in old age. (Sullivan et al. 1979) This consequently leads to an increase in the serum Cu/Zn-ratio. Given that an increased serum Cu/Zn-ratio is commonly seen in older people, there is also a possibility that our findings of an increased risk of pneumonia with an increased serum Cu/Zn-ratio could be due to reverse causation. However, this may be unlikely given that the findings were essentially similar on excluding the first two years of follow-up.
Implications of findings
The overall evidence suggests that serum Cu/Zn-ratio, Cu and Zn could be risk markers for incident pneumonia. Whether there is a causal relevance to these presented relationships would need to be proved using appropriate study designs such as randomised controlled trials and Mendelian randomisation studies. Nevertheless, the findings are clinically relevant. It has previously been suggested that the serum Cu/Zn-ratio may be a valuable predictive marker for pathological outcomes, and might be comparable or even superior to other well established inflammatory markers such as CRP and erythrocyte sedimentation rate. (Malavolta et al. 2015) Indeed, our analysis showed that serum Cu/Zn-ratio might be a potentially stronger risk indicator for pneumonia risk than hsCRP. An increment of the serum Cu/Zn-ratio above 2.0 in older people has been reported to commonly reflect an inflammatory response or decreased nutritional Zn status. (Malavolta et al. 2010) Measurement of the serum Cu/Zn-ratio as well as serum Cu and Zn concentrations could be used to identify individuals at high risk of serious infections such as pneumonia. However, formal risk prediction analyses are needed to assess the value of these potential risk predictors. Since Zn deficiency in old age is commonly due to insufficient dietary Zn consumption, reduced intestinal absorption or increased losses,(Mocchegiani et al. 2013) its supplementation could help alleviate the deficiencies, which could ultimately provide optimal levels of serum Cu/Zn-ratio in at-risk individuals. There is consistent evidence that preventive Zn supplementation reduces the risk of morbidity and mortality from infectious diseases such as pneumonia, diarrhoea and malaria. (Bates et al. 1993; Yakoob et al. 2011).
Strengths and limitations
Apart from being the first prospective evaluation of the association between serum Cu/Zn-ratio and the specific outcome of pneumonia, other strengths include (i) the representativeness of the general Finnish middle-aged to older male population, (ii) employment of a relatively large cohort, (iii) the long-term follow-up of the cohort, and (iv) the comprehensive analyses including adjustment for a panel of potential confounders, assessment of the dose–response relationships, evaluation for effect modification on the association using several clinically relevant characteristics and sensitivity analysis. Several limitations of this study deserve consideration. They include (i) the inability to generalise findings to other populations, women and other age groups; furthermore, evidence suggests that there may be gender differences in the concentrations of Cu and Zn;(Olsen et al. 2012) (ii) the possibility that regression dilution bias could have underestimated the associations due to the use of single baseline measurements of the exposures and the long-term follow-up period; (iii) serum Cu concentrations may not accurately reflect actual Cu status, given that leucocyte Cu measurement is considered to be a more reliable index of Cu status in the body;(DiNicolantonio et al. 2018) and (iv) the potential for biases such as residual confounding and reverse causation as with all observational cohort studies.
Conclusions
An increased serum Cu/Zn-ratio and serum Cu concentrations are associated with an increased risk of incident pneumonia in middle-aged and older Finnish men, consistent with linear dose–response relationships. The relationship between serum Zn and pneumonia is inverse and curvilinear. Furthermore, serum Cu/Zn-ratio might be a stronger risk indicator for pneumonia than hsCRP, a major inflammatory marker.
Data availability
The data that support the findings of this study are available from the Principal Investigator (J.A.L.) upon reasonable request.
Abbreviations
- BMI:
-
Body mass index
- CAP:
-
Community acquired pneumonia
- CHD:
-
Coronary heart disease
- CI:
-
Confidence interval
- COPD:
-
Chronic obstructive pulmonary disease
- Cu:
-
Copper
- HDL-C:
-
High-density lipoprotein cholesterol
- HR:
-
Hazard ratio
- hsCRP:
-
High-sensitivity C-reactive protein
- IQR:
-
Interquartile range
- KIHD:
-
Kuopio Ischemic Heart Disease
- SD:
-
Standard deviation
- SES:
-
Socioeconomic status
- Zn:
-
Zinc
References
Abdollahi AM, Virtanen HEK, Voutilainen S, Kurl S, Tuomainen TP, Salonen JT, Virtanen JK (2019) Egg consumption, cholesterol intake, and risk of incident stroke in men: the kuopio ischaemic Heart disease risk factor study. Am J Clin Nutr 110:169–176
Asemota EA, Okafor IM, Okoroiwu HU, Ekong ER, Anyanwu SO, Efiong EE, Udomah F (2018) Zinc, copper, CD4 T-cell count and some hematological parameters of HIV-infected subjects in Southern Nigeria. Integr Med Res 7:53–60
Bates CJ, Evans PH, Dardenne M, Prentice A, Lunn PG, Northrop-Clewes CA, Hoare S, Cole TJ, Horan SJ, Longman SC et al (1993) A trial of zinc supplementation in young rural gambian children. Br J Nutr 69:243–255
Baudry J, Kopp JF, Boeing H, Kipp AP, Schwerdtle T, Schulze MB (2020) Changes of trace element status during aging: results of the EPIC-potsdam cohort study. Eur J Nutr 59:3045–3058
Besold AN, Culbertson EM, Culotta VC (2016) The Yin and Yang of copper during infection. J Biol Inorg Chem 21:137–144
Chimienti F (2013) Zinc, pancreatic islet cell function and diabetes: new insights into an old story. Nutr Res Rev 26:1–11
Cilloniz C, Ceccato A, San Jose A, Torres A (2016) Clinical management of community acquired pneumonia in the elderly patient. Expert Rev Respir Med 10:1211–1220
Cilloniz C, Martin-Loeches I, Garcia-Vidal C, San Jose A, Torres A (2016) Microbial etiology of pneumonia: epidemiology diagnosis and resistance patterns. Int J Mol Sci. https://doi.org/10.3390/ijms17122120
Cillóniz C, Cardozo C, García-Vidal C (2018) Epidemiology, pathophysiology, and microbiology of communityacquired pneumonia. Annals Res Hosp. https://doi.org/10.21037/arh.2017.12.03
DiNicolantonio JJ, Mangan D, O’Keefe JH (2018) Copper deficiency may be a leading cause of ischaemic heart disease. Open Heart 5:e000784
Diseases GBD, Injuries C (2020) Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet 396:1204–1222
Engelfriet PM, Jansen EH, Picavet HS, Dolle ME (2013) Biochemical markers of aging for longitudinal studies in humans. Epidemiol Rev 35:132–151
Festa RA, Thiele DJ (2011) Copper: an essential metal in biology. Curr Biol 21:R877-883
Groenwold RH, Klungel OH, Grobbee DE, Hoes AW (2011) Selection of confounding variables should not be based on observed associations with exposure. Eur J Epidemiol 26:589–593
Haase H, Rink L (2009) The immune system and the impact of zinc during aging. Immun Ageing 6:9
Haase H, Rink L (2014) Multiple impacts of zinc on immune function. Metallomics 6:1175–1180
Harrell FE Jr (2001) Regression modeling strategies: with applications to linear models, logistic regression, and survival analysis. Springer, New York
He H, Wang Y, Yang Z, Ding X, Yang T, Lei G, Li H, Xie D (2020) Association between serum zinc and copper concentrations and copper/zinc ratio with the prevalence of knee chondrocalcinosis: a cross-sectional study. BMC Musculoskelet Disord 21:97
Jackson ML, Neuzil KM, Thompson WW, Shay DK, Yu O, Hanson CA, Jackson LA (2004) The burden of community-acquired pneumonia in seniors: results of a population-based study. Clin Infect Dis 39:1642–1650
Jae SY, Kurl S, Bunsawat K, Franklin BA, Choo J, Kunutsor SK, Kauhanen J, Laukkanen JA (2020) Impact of cardiorespiratory fitness on survival in men with low socioeconomic status. Eur J Prev Cardiol. https://doi.org/10.1177/2047487319901057
Kassu A, Yabutani T, Mahmud ZH, Mohammad A, Nguyen N, Huong BT, Hailemariam G, Diro E, Ayele B, Wondmikun Y, Motonaka J, Ota F (2006) Alterations in serum levels of trace elements in tuberculosis and HIV infections. Eur J Clin Nutr 60:580–586
Kunutsor SK, Laukkanen JA (2016) Serum zinc concentrations and incident hypertension: new findings from a population-based cohort study. J Hypertens 34:1055–1061
Kunutsor SK, Khan H, Laukkanen JA (2016) gamma-glutamyltransferase and risk of sudden cardiac death in middle-aged finnish men: a new prospective cohort study. J Am Heart Assoc. https://doi.org/10.1161/JAHA.115.002858
Kunutsor SK, Khan H, Nyyssonen K, Laukkanen JA (2016a) Lipoprotein(a) and risk of sudden cardiac death in middle-aged finnish men: a new prospective cohort study. Int J Cardiol 220:718–725
Kunutsor SK, Kurl S, Zaccardi F, Laukkanen JA (2016b) Baseline and long-term fibrinogen levels and risk of sudden cardiac death: a new prospective study and meta-analysis. Atherosclerosis 245:171–180
Kunutsor SK, Laukkanen T, Laukkanen JA (2017a) Cardiorespiratory fitness and future risk of pneumonia: a long-term prospective cohort study. Ann Epidemiol 27:603–605
Kunutsor SK, Laukkanen T, Laukkanen JA (2017b) Frequent sauna bathing may reduce the risk of pneumonia in middle-aged caucasian men: the KIHD prospective cohort study. Respir Med 132:161–163
Kunutsor SK, Whitehouse MR, Blom AW, Laukkanen JA (2017c) Low serum magnesium levels are associated with increased risk of fractures: a long-term prospective cohort study. Eur J Epidemiol 32:593–603
Lai H, Lai S, Shor-Posner G, Ma F, Trapido E, Baum MK (2001) Plasma zinc, copper, copper: zinc ratio, and survival in a cohort of HIV-1-infected homosexual men. J Acquir Immune Defic Syndr 27:56–62
Laine JT, Tuomainen TP, Salonen JT, Virtanen JK (2020) Serum copper-to-zinc-ratio and risk of incident infection in men: the kuopio ischaemic heart disease risk factor study. Eur J Epidemiol 35:1149–1156
Laukkanen T, Kunutsor SK, Zaccardi F, Lee E, Willeit P, Khan H, Laukkanen JA (2018) Acute effects of sauna bathing on cardiovascular function. J Hum Hypertens 32:129–138
Leone N, Courbon D, Ducimetiere P, Zureik M (2006) Zinc, copper, and magnesium and risks for all-cause, cancer, and cardiovascular mortality. Epidemiology 17:308–314
Malavolta M, Giacconi R, Piacenza F, Santarelli L, Cipriano C, Costarelli L, Tesei S, Pierpaoli S, Basso A, Galeazzi R, Lattanzio F, Mocchegiani E (2010) Plasma copper/zinc ratio: an inflammatory/nutritional biomarker as predictor of all-cause mortality in elderly population. Biogerontology 11:309–319
Malavolta M, Piacenza F, Basso A, Giacconi R, Costarelli L, Mocchegiani E (2015) Serum copper to zinc ratio: relationship with aging and health status. Mech Ageing Dev 151:93–100
Mocchegiani E (2007) Zinc and ageing: third Zincage conference. Immun Ageing 4:5
Mocchegiani E, Romeo J, Malavolta M, Costarelli L, Giacconi R, Diaz LE, Marcos A (2013) Zinc: dietary intake and impact of supplementation on immune function in elderly. Age (dordr) 35:839–860
Nair GB, Niederman MS (2011) Community-acquired pneumonia: an unfinished battle. Med Clin North Am 95:1143–1161
Olsen L, Lind PM, Lind L (2012) Gender differences for associations between circulating levels of metals and coronary risk in the elderly. Int J Hyg Environ Health 215:411–417
Prasad AS, Miale A, Jr., Farid, Z., Sandstead, H.H., Schulert, A.R. (1963) Zinc metabolism in patients with the syndrome of iron deficiency anemia, hepatosplenomegaly, dwarfism, and hypognadism. J Lab Clin Med 61:537–549
Reunanen A, Knekt P, Marniemi J, Maki J, Maatela J, Aromaa A (1996) Serum calcium, magnesium, copper and zinc and risk of cardiovascular death. Eur J Clin Nutr 50:431–437
Salonen JT, Nyyssonen K, Korpela H, Tuomilehto J, Seppanen R, Salonen R (1992) High stored iron levels are associated with excess risk of myocardial infarction in eastern finnish men. Circulation 86:803–811
Stafford SL, Bokil NJ, Achard ME, Kapetanovic R, Schembri MA, McEwan AG, Sweet MJ (2013) Metal ions in macrophage antimicrobial pathways: emerging roles for zinc and copper. Biosci Rep. https://doi.org/10.1042/BSR20130014
Sullivan JF, Blotcky AJ, Jetton MM, Hahn HK, Burch RE (1979) Serum levels of selenium, calcium, copper magnesium, manganese and zinc in various human diseases. J Nutr 109:1432–1437
Taylor HL, Jacobs DR Jr, Schucker B, Knudsen J, Leon AS, Debacker G (1978) A questionnaire for the assessment of leisure time physical activities. J Chronic Dis 31:741–755
Torres A, Peetermans WE, Viegi G, Blasi F (2013) Risk factors for community-acquired pneumonia in adults in Europe: a literature review. Thorax 68:1057–1065
Uriu-Adams JY, Keen CL (2005) Copper, oxidative stress, and human health. Mol Aspects Med 26:268–298
Van Weyenbergh J, Santana G, D’Oliveira A Jr, Santos AF Jr, Costa CH, Carvalho EM, Barral A, Barral-Netto M (2004) Zinc/copper imbalance reflects immune dysfunction in human leishmaniasis: an ex vivo and in vitro study. BMC Infect Dis 4:50
Wellinghausen N, Kirchner H, Rink L (1997) The immunobiology of zinc. Immunol Today 18:519–521
Yakoob MY, Theodoratou E, Jabeen A, Imdad A, Eisele TP, Ferguson J, Jhass A, Rudan I, Campbell H, Black RE, Bhutta ZA (2011) Preventive zinc supplementation in developing countries: impact on mortality and morbidity due to diarrhea, pneumonia and malaria. BMC Public Health 11(Suppl 3):S23
Acknowledgements
We thank the staff of the Kuopio Research Institute of Exercise Medicine and the Research Institute of Public Health and University of Eastern Finland, Kuopio, Finland for the data collection in the study.
Funding
JAL acknowledges support from The Finnish Foundation for Cardiovascular Research, Helsinki, Finland.
Author information
Authors and Affiliations
Contributions
S.K.K. conceived and planned the study and methodology, conducted data curation, carried out the statistical analysis and prepared an original draft; S.Y.J. conceived and planned the study; J.A.L. conceived and planned the study and methodology; all authors contributed to writing, reviewing, and editing of the manuscript, provided insights on the topic, discussed the results and critically revised the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare there are no competing interests.
Ethical approval
The Research Ethics Committee of the University of Eastern Finland approved the study (reference #:143/97), and each participant gave written informed consent. All study procedures were conducted according to the Declaration of Helsinki.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kunutsor, S.K., Voutilainen, A. & Laukkanen, J.A. Serum copper-to-zinc ratio and risk of incident pneumonia in caucasian men: a prospective cohort study. Biometals 35, 921–933 (2022). https://doi.org/10.1007/s10534-022-00414-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10534-022-00414-4