
Abstract
This systematic review and meta-analysis aims to compare the effects of couple-based prevention interventions against individual-level interventions on HIV prevention in randomized controlled trials (RCTs), identify potential moderators, and assess study quality. Eleven RCTs were included, comprising 3933 couples in the intervention group and 7125 individuals in the individual control group, predominantly in heterosexual couples from the USA and Africa. Couple-based interventions had a more significant effect in promoting condom use and HIV testing. Education levels of high school or above, residence in low- and middle-income countries, and intervention design incorporating HIV counseling and testing were associated with higher odds of condom use. The quality assessment analysis identified methodological and theoretical heterogeneity factors. Evidence of couple-based HIV prevention RCTs among men who have sex with men, injecting drug users, sex workers, and transgender women warrant further investigation. Recommendations are made to improve the quality and replicability of future intervention studies.
Resumen
Esta revista sistemática y metanálisis tiene por objeto comparar los efectos de las intervenciones de prevención basadas en pareja con las a nivel individual en la prevención del VIH en ensayos controlados aleatorios (ECA), identificar posibles moderadores y evaluar la calidad de los estudios. Se incluyeron once ECA, que comprendían 3.933 parejas en el grupo de intervención y 7.125 personas en el grupo de control individual, la mayoría de las cuales eran heterosexuales de EE.UU. y de África. Las intervenciones basadas en pareja son más eficaces para promover el uso de preservativos y pruebas del VIH. Los niveles de educación secundaria o superior, los países de ingresos bajos y medianos, y los diseños de intervención que incluyen pruebas y asesoramiento sobre el VIH se relacionan con más uso de preservativos. El análisis de evaluación de la calidad ha identificado factores de heterogeneidad metodológica y teórica. Las pruebas de ECA basadas en pareja para la prevención del VIH en hombres que tienen sexo con hombres, consumidores de drogas inyectables, trabajadoras sexuales y mujeres transgénero necesitan más investigación. Se hacen recomendaciones para mejorar la calidad y replicabilidad de futuros estudios de intervención.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Sexual transmission of HIV between two sexually intimate partners remains the primary cause of the HIV epidemic in many parts of the world [1]. In this specific micro-social situation, dissonance between partners emerges in the liaison of interaction and interdependence [2]. This creates a variegated picture of the sexual risks driving HIV transmission among couples [3]. Partner bonds may be resilient through shared resources and coping efforts conducive to one or both individuals’ improved health outcomes [4]. However, the intimate bond between couples can complicate efforts to sustain HIV transmission prevention methods. A good illustration is HIV prevention between serodiscordant partners in which one partner has positive HIV status; even though HIV transmission is a persistent health threat to serodiscordant couples, they may not use condoms consistently [5] because condom use delegitimizes the trust and intimacy of a romantic relationship [6]. In such situations where individual resources are overwhelmed, partners can prevent HIV transmission while promoting trust and intimacy by calling on shared resources and efforts, including sexual negotiation [7,8,9], virus load suppression for the HIV positive partner (i.e., the outlook of “undetectable equals untransmittable” status; i.e., U = U) [8, 10, 11], as well as HIV counseling and testing [12], and access to pre-exposure prophylaxis (PrEP) [13] for the HIV-negative partner.
The past two decades have witnessed growing advancement in couple-based HIV prevention programs. Recent empirical evidence supports the credibility of couple-based interventions, particularly when compared to individual-level interventions with large base sizes. A recent meta-analysis suggested that couple-based interventions are more effective than individual-level interventions in promoting HIV-protective behaviors to prevent HIV transmission and infection [14]. Dyadic perspectives may increase couples’ sense of shared responsibility for HIV and sexually transmitted infections (STI) prevention, motivating them to work together to stay healthy and reinforcing intimate partner bonding by treating two partners as an intervention unit. This approach is advantageous in offering preventive interventions for HIV and other STI because it delivers practical skills in communication and negotiation for safer sex.
Parallel to this, the development of HIV-prevention randomized controlled trials (RCTs) in key populations (i.e., injecting drug users, sex workers, gay men and other men who have sex with men [MSM], and transgender populations) and their sexual partners has become an overarching public health issue. One important observation is that in recent years, more than 60% of new adult HIV cases worldwide occurred in key populations [1]. However, because they face persistent health inequities, these populations have no, or very limited, access to HIV-related health resources [1]. It therefore becomes important that intervention programs not only help to mobilize resources or encourage the use of shared resources amongst key populations, but also ascertain the socioenvironmental factors that may inhibit these populations from implementing them. Another important point is that, with RCTs as the gold standard of evidence for intervention studies in the twenty-first century [15], using RCTs to evaluate the intervention effects of improving the health and well-being of key populations in the face of widespread global health inequities is now one of many pressing public health concerns [16].
To date, five systematic reviews and meta-analyses of HIV couple-based intervention and prevention studies have been published, which primarily provide qualitative and quantitative assessments of key intervention elements and study outcomes [14, 16,17,18]. However, there are two significant issues of heterogeneity limiting these studies: issues in the methodological design of empirical intervention studies and quality assessments of the meta-studies.
First, the scarcity of couple-based HIV prevention interventions has led to notable heterogeneity in study designs and outcomes in these five systematic reviews and meta-analyses. Although one of the five systematic reviews and meta-analyses compares couple-based and individual-level interventions [14], it achieves this only by mixing controlled trials and prospective cohort designs, thereby obfuscating the underlying intervention effects due to considerable selection bias in study design. However, RCTs may counter the heterogeneity seen in previous systematic reviews and meta-analyses more effectively by controlling self-selection and self-reporting bias in study design. Therefore, a meta-analysis of RCTs involving couple-based HIV prevention interventions will help clarify the effects of couple-based interventions over individual-level interventions.
Furthermore, methodological heterogeneity in HIV prevention intervention research may also be perceived on a theoretical level. Couple-based research frequently relies on individual-level theories as design and interpretation frameworks [16], potentially diminishing significant moderators and health outcomes of dyadic interactions and decision-making. Therefore, the development of dyad-level theories may more accurately explain inter- and intrapersonal interaction as well as the influence of health behaviors in couples [3, 19] by considering both partners’ emotions, cognition, and behaviors. These dyadic models may provide a more robust theoretical underpinning for research and intervention in addressing the needs of an intimate-partner relationship [20].
Second, there is distinct heterogeneity in the quality assessments used to substantiate each study’s internal validity among these five meta-studies. Only Jiwatram-Negrón and El-Bassel’s study [16] used an adapted assessment tool to provide quality assessment. A scarcity of accredited quality assessment guidelines may contribute to the lack of quality assessments conducted in the additional four studies. The Template for Intervention Description and Replication (TIDieR) guide published in 2014 clarifies intervention reporting to ensure the quality and replicability of intervention studies [21]. However, the five meta-studies above were conducted before the release of the TIDieR guide, potentially contributing to their lack of rigorous and uniform quality assessment. Thus, the present study facilitates the development of future intervention studies of couple-based HIV prevention by implementing a more comprehensive quality assessment framework through the integration of methodological and reporting quality assessments.
Considering the heterogeneity within the design, outcome, and quality assessment variables of previous meta-studies, this systematic review and meta-analysis aims to (a) estimate the relative magnitude of couple-based interventions over individual-level interventions’ effects on HIV preventive behaviors of sexual-risk reduction through direct comparison of RCTs; (b) identify potential moderators, particularly intervention- and relationship-specific factors of the intervention effect; and (c) assess the methodological and reporting quality of the intervention. This paper expands on existing systematic reviews and meta-analyses, integrating more recent literature with more robust methodological support and making suggestions for quality assessment.
Methods
Protocol Registration
This systematic review and meta-analysis was registered in the PROSPERO database (CRD42020222819, https://www.crd.york.ac.uk/PROSPERO/). We conducted and reported our systematic review and meta-analysis according to Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA, [22]; Table A in Online Attachment).
Searching Strategy
The first two authors (RF & JH) independently searched five electronic databases (Web of Science, PubMed/Medline, PsycInfo, CINAHL, and clinicaltrials.gov). The keywords combined participant (Couple OR dyad OR partner OR married), intervention-related terms (training OR intervention OR prevention), and disease-related terms (HIV OR AIDS) (See detailed search strings in Table B in Online Attachment). We also searched the reference lists of the published systematic review and original articles. All searches were limited to English peer-reviewed journal articles.
Study Eligibility
Studies were eligible if they met the following criteria: (1) used RCT study design; (2) evaluated a couple-based preventive intervention compared to an individual-level control, including biobehavioral components (i.e., skills-building, HIV voluntary testing and counseling and antiretroviral therapy [ART] adherence) as previously categorized by Jiwatram-Negrón and El-Bassel [16]; (3) conducted in same-sex or heterosexual couples; and (4) measured pre- and post-intervention changes in at least one HIV-preventive behavior. Studies were excluded if they were: (1) a theoretical article or research protocol or (2) not peer-reviewed (i.e., an unpublished thesis, dissertation, or book chapter).
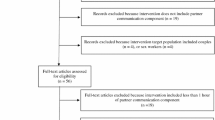
Two authors (RF & JH) independently screened the results based on titles, abstracts, and full texts. RF & JH held three discussion meetings with the corresponding author (NXY) to resolve any discrepancies during the screening phase. The full texts were excluded if they (1) lacked RCT design, (2) lacked a couple-based or couple-focused intervention or control group, (3) lacked couple vs. individual comparison, (4) used the same dataset published in a previous paper, (5) used a secondary analysis, (6) provided only baseline data, (7) randomized only HIV-negative partners, (8) described study outcomes that were not related to sexual-risk reduction or HIV/AIDS, or (9) invited study participants who were not in a sexual relationship (Table C in Online Attachment). The selection process is shown in Fig. 1.

The flow chart of the included studies
Data Coding and Extraction
The outcomes of interest are HIV-preventive behaviors, including condom use (defined as consistent condom use or no condomless sex), HIV testing, STI reduction, and ART adherence. ART adherence can be measured by either a self-report scale or blood-based tests.
We (RF & JH) coded the adjusted odds ratios (aOR) with 95% confidential interval, means and standard deviations (SD) in each arm before and after interventions, and mean changes with variance in each arm or other data format used to calculate odds ratio.
We (RF & JH) also used a Shimo spreadsheet (https://shimo.im/desktop) to extract participant-related information (i.e., age, education attainment, sex distribution, type of couple, and relationship status), intervention-related data (i.e., sessions, frequency, total hours, intervention content, the format of control, and type of control), and implementation-related characteristic (i.e., fidelity and tailoring).
Specifically, we coded the type of couple into same-sex, heterosexual, and mixed. Relationship status is operationalized as the median or mean years of partnership or percentage of participants who regarded themselves as in a relationship.
Statistical Analysis
First, a random-effects model was conducted using the odds ratio (OR) to estimate the comparative effect of the couple-based intervention on HIV preventive behavior. An OR higher than 1 indicated greater odds of condom use in the couple-based intervention than in the individual-level control. Forest plots illustrate the effect sizes for individual and pooled studies.
Second, we used Cochrane Q tests and I2 to assess the significance and proportion of the between-study heterogeneity [23]. Regarding publication bias, we utilized Egger’s intercept test to assess the asymmetry of the funnel plot [24].
Third, subgroup analysis and meta-regression were used to evaluate the source of heterogeneity if more than 10 comparisons were analyzed in any outcomes. In addition to a continuous variable of age, moderators of categorical variables included the education level (high school or above vs. below high school), intervention component (skills-building vs. HIV testing and counseling), type of couple (i.e., heterosexual, same-sex, or mixed), study quality (high vs. low; we compared studies with high bias against those with low bias to check the robustness of our findings [25]), total sessions (< 6 sessions vs. ≥ 6 sessions), tailoring (no or unclear vs. yes), fidelity (no or unclear vs. yes), HIV status (serodiscordant couple vs. negative or unknown), and country (high-income vs. low- and middle-income). Because the studies have relatively small sample sizes and/or are few, a p value of 0.1 was used, as suggested by the Cochrane handbook [26], to detect the significance of heterogeneity and subgroup analyses. Additionally, subgroup analysis was conducted after we found 10 or more comparisons of outcomes of interest [26].
All analyses were conducted in Comprehensive Meta-analysis Version 3 (CMA 3.0).
Study Quality
Referring to previous meta-analyses concerning the effect of psychological interventions [25, 27], we used a modified Physiotherapy Evidence Database (PEDro) scale to evaluate the study quality, including participant eligibility, randomization, the comparable baseline in key outcomes, concealment, retention rate (> 85%) intention-to-treat (ITT), blindness to participants, between-group comparisons, and point estimates with variance [32]. Studies were regarded as high-quality if they scored 7 or higher (maximum score = 9). The first two authors independently checked the study quality point-to-point (Table D in Online Attachment). We also used a modified template for intervention description and replication (TIDieR) checklist to label whether the researchers have reported their intervention properly, which is crucial for study replication [21].
Results
Characteristics of Included Studies
Altogether, 11 eligible RCTs [28,29,30,31,32,33,34,35,36,37,38] were included in this meta-analysis (Table 1), comprising 3933 couples in the intervention group and 7125 individuals in the individual-level control, with heterosexual couples in the USA and Africa predominating. The mean participant age ranged from 18 to 45. Heterosexual couples were recruited exclusively in 10 out of 11 RCT studies, of which only one study covered injecting drug users and their sexual partners. Apart from this, only one of the 11 studies recruited male couples [38]. Three studies recruited serodiscordant couples [31, 35, 38] whereas others recruited seroconcordant HIV-negative or couples with unknown HIV status. The education level varied across studies, and the female proportion ranged from 0 to 72.8%. Six studies defined a couple by the length of the relationship (i.e., a minimum of being together for six months [28, 30,31,32,33, 35]). Only three of the included RCTs reported significant effects on HIV-preventive behaviors [29, 31, 36].
Comparing Couple-Based Versus Individual-Based Intervention on HIV-Preventive Behaviors
Condom Use
Eleven comparisons reported condom use during anal or vaginal sex acts. The composite effect size for the change of condom use between the two groups was 1.431 (95% CI 1.133–1.808, p = 0.003, random-effects model, Fig. 2, Panel A). No significant heterogeneity was detected across comparisons [Q(10) = 17.625, p = 0.062, I2 = 43.261%]. No significant asymmetry was detected from the funnel plot (Intercept = − 0.277, p = 0.742).

The forest plot for HIV preventive behaviors. Panel A: The pooled effect size for condom use. Panel B: The pooled effect sizefor HIV testing. Panel C: The pooled effect size for STI reduction. Panel D: The pooled effect size for ARTadherence
HIV Testing
Three comparisons reported HIV testing rates between the two groups. The composite effect size for the change in HIV testing between the two groups was 1.308 (95% CI 1.061–1.612, p = 0.012, Fig. 2, Panel B). No significant heterogeneity was detected across comparisons [Q(2) = 1.538, p = 0.464, I2 = 0]. No significant asymmetry was detected from the funnel plot (Intercept = 24.183, p = 0.120).
STI Reduction and ART Adherence
Two comparisons reported STI rates between the two groups. The composite effect size for the change of STI between the two groups was 1.638 (95% CI 0.509–5.270, p = 0.408; Fig. 2, Panel C). A significant heterogeneity was detected across comparisons [Q(1) = 3.318, p = 0.069, I2 = 69.86]. Only one study reported ART adherence between two groups with a non-significant effect size (OR 1.230, 95% CI 0.729–2.076, p = 0.438; Fig. 2, Panel D).
Moderating Effects
Participants with an education level of high school or above showed a higher odds of condom use [Q(1) = 4.401, p = 0.036], compared to those had received less than a high school education. Compared to skills-building, interventions incorporating an HIV counseling and testing component were more effective in improving condom use [Q(1) = 3.275, p = 0.070]. Improvements in condom use were higher in low- and middle-income countries (LMICs) compared to studies conducted in high-income countries [Q(1) = 3.679, p = 0.054].
Other moderators—such as age, type of couple, HIV status, study quality, intervention sessions, tailoring, and fidelity—were not significantly associated with the intervention effect of condom use (Table 2). The number of trials was not sufficient to conduct a moderating analysis for the outcomes of HIV testing, STI reduction and ART adherence.
Methodological and Reporting Quality
Online Table D summarizes the methodological quality of the included studies. All the included studies provided clear information on their eligibility criteria, randomization, similar baseline, and utilized appropriate statistical analysis for between-group comparisons [28,29,30,31,32,33,34,35,36,37,38]. However, six of the 11 studies lacked concealed allocation [28, 32,33,34,35, 37], seven studies did not blind the assessors [28,29,30, 32,33,34, 37], three studies did not analyze their data following ITT strategies [33, 37, 38], one study failed to obtain data from more than 85% of the participants initially allocated to both groups [38], and one study did not report the point estimate and its variance [28].
Table 3 summarizes the reporting quality of the included studies. Only one study reported the intervention as per the TIDieR checklist [36]. Seven out of 11 studies articulated their research aims using theoretical frameworks—social cognitive theory and combined ecological theory being the most frequently adopted [30,31,32,33,34,35, 37]. All studies except one did not report the provider(s) (e.g., trained counselor or facilitator) of the intervention [37]. Three studies were conducted in LMICs [28, 36, 37], seven in one high-income country (i.e., the USA [30,31,32,33,34,35, 38]), and one comprising data from three countries [29].
Different from Jiwatram-Negrón and El-Bassel’s categorization of couple-based HIV prevention and intervention biobehavioral studies [16], we identified two main HIV prevention intervention components: couple-based skills-building and couple-based HIV counseling and testing (CHCT). The couple-based skill-building component incorporated relationship-enhancing, risk-reduction, joint decision-making, and collaborative problem-solving skills, which also integrated with ART adherence education in one RCT study [35]. The CHCT component provided a single-session 30–60 min counseling and testing service based on couples’ gender roles, sexual orientation, sexual or drug use history, and risk assessment, or ethnicity. For instance, the CHCT component for male couples discussed HIV risks and how they wish to approach HIV prevention and skills-building around sexual agreements in the future [38]. From the individual-based control arms, we also differentiated two components: individual-based health education that promotes participants’ overall health or provides HIV/STD information, and individual-based usual care that covers standard clinical care providing ART medication adherence or standard HIV counseling and testing.
The intervention ranged from one to 14 sessions, apart from three interventions that offered a one-off CHCT session [28, 29, 38]. Six interventions were conducted with one session per week [30,31,32,33,34, 36]. Six studies tailored interventions to the couple’s dyadic risk features, findings from previous couple-based interventions, and characteristics of the key populations [29, 31, 32, 34, 37, 38]. However, modifications of intervention content or implementation procedure were not reported in any of the 11 studies. In addition, seven studies adopted strategies (e.g., fidelity check by on-site supervisor) to maintain or improve fidelity [30,31,32,33,34,35,36].
Discussion
This meta-analysis is the first to synthesize existing RCTs, and it finds that couple-based interventions are more efficacious in promoting condom use and HIV testing (i.e., biobehavioral prevention) than individual-level interventions. As moderators for intervention effect, participants with higher education levels, couple-based interventions utilizing HIV testing and counseling strategies, and interventions conducted in low-income countries showed more significant improvement in condom use. This suggests that, despite the potential to reduce sexual risks and enhance HIV testing, many couple-based HIV prevention interventions conducted worldwide remain inadequate. Therefore, the following discussion also highlights significant methodological constraints of RCTs that are critical for facilitating advancements in couple-based HIV prevention interventions.
Relative Effect of Couple-Based Interventions on HIV-Preventive Behaviors
This systematic review suggests that couple-based interventions have a stronger effect than individual-level interventions to boost condom use and encourage HIV testing among couples in RCTs. One possibility is that behavioral cooperation may help couples establish common goals in initiating healthy behaviors and developing a partnership based on joint decision-making and collective action toward reducing HIV transmission risks [13]. When both partners participate in couple-based interventions, they decrease discrepant perceptions of HIV transmission risks and increase their health literacy regarding HIV [39].
Another possible consideration is that enhanced communicative skills may enable couples to discuss complex or private sexual issues more openly. However, such inter-couple discussions are hard to implement without proper guidance [37, 40]. Couple-based intervention offers a promising platform to promote “open” discussions with a trained counselor or psychologist to help discuss sexual issues in a safe and constructive environment [41].
Communication-based intervention techniques may help couples to acknowledge sexual consent and shift their normative perceptions of their sexual relationships [42], thereby enhancing their dyadic resilience and relationship health as a whole [4]. In particular, interventions emphasizing a healthy sexuality, a healthy couple relationship, power-balancing, negotiating power, and joint decision-making may provide opportunities for cultivating open discussions. One example is that CHCT service offers a room for couples to learn about HIV risk for individuals and couples, to find out couples’ HIV status, and form a collaborative HIV prevention plan with help from a counselor who can facilitate couple discussion to reduce fears and possible negative consequences before and after disclosure [43, 44].
Moderators of Intervention Effect in Promoting Condom Use
We identified three moderators of the intervention effect in promoting condom use: (1) intervention design incorporating HIV counseling and testing, (2) low- and middle-income countries, and (3) high school or above education level. First, HIV counseling and testing showed a stronger intervention effect than skills-building in promoting condom use. Although we did not conduct subgroup analyses on HIV testing due to limited comparisons, one 2020 RCT study found that the skills-building component of a couple-based intervention resulted in comparable effects on both condom use and HIV testing [36]. It is worth noting that interventions containing a skills-building strategy showed smaller, but significant, effects on condom use. Therefore, an additional question merits further examination: Will a combined-component couple-based intervention (i.e., CHCT plus skills-building) outperform a single-component couple-based intervention (i.e., CHCT or skills-building alone) in promoting more significant and longer-lasting effects on HIV-preventive behaviors? Some individual-level multi-component interventions may shed light on the answer to this question [45, 46]. For example, an RCT study demonstrated that MSM exposed to combined behavioral (e.g., interpersonal communication) and biomedical (e.g., HIV testing and counseling) components were more likely to use condoms during anal sex compared to those in the single-component group [45].
Second, adapting intervention material to participants’ education levels may increase the effectiveness of HIV transmission prevention interventions. As previously mentioned, participants with a high school education or above were more likely to use condoms than those with a lower education level. Intervention research that incorporates a skills-building component and typically takes several hours of training [31, 32, 47] may be too pedantically saturated to benefit participants with lower education levels. Therefore, we recommend a simplified version of the implementation protocols for participants with lower education levels that highlight the practical features of HIV transmission prevention and use layman’s language in combination with suggestions to practice behavioral and habitual changes at home.
Third, couple-based HIV prevention interventions may be more beneficial to reducing sexual risks when implemented in areas where resources are more constrained, such as in LMICs. Evidence from prior research supports our findings that CHCT has been recognized as one of the most cost-effective intervention strategies in resource-constrained settings and is particularly strong in HIV-serodiscordant couples [43]. This may be explained by the mobilizing of shared resources within a couple that were previously rarely considered, including the awareness of the importance of sexual negotiation, and supporting once-scarce environmental resources such as the space for an open and private conversation with a trained counselor for CHCT and/or access to PrEP [12, 13]. Although the evidence for cost-effectiveness analyses of skill-building intervention components remains to be clarified, future public health intervention strategies need to be weighted more toward resource-constrained areas with the objective to more effectively reduce HIV risk among couples.
Methodological and Theoretical Barriers and Recommendations
Several methodological and theoretical barriers must be highlighted because they risk impacting the advancement of couple-based HIV prevention interventions. First, although study quality did not appear to moderate the intervention effect in RCTs, seven of the 11 studies (63.6%) failed to conceal allocation or blind the assessor. Consequently, a low-quality or inadequately designed study may still distort the verifiability of the study’s effects because of these two issues. We suggest that the allocation of quality assessment measures be executed by off-site third parties or by using sequentially numbered, sealed, opaque envelopes to establish better methodological and reporting quality.
Moreover, because eight of the 11 studies (72.7%) were published before 2014, only one study reported its intervention following the TIDieR checklist for better reporting and replication [36]. By utilizing TIDieR, we found that six out of 11 studies reported tailoring the intervention content to the study participants, mainly in risk-assessment and risk-reduction plans that seldom consider embedded sociocultural contexts.
Regrettably, most (six out of seven) of the reviewed couple-based HIV preventive intervention RCTs reported using theoretical frameworks were guided by individual-based theories focusing on behavioral changes at the individual level, such as social cognitive theory and combined ecological theory, rather than dyadic-level theories [31, 34]. As a result, many aspects involving dyads, interactions, and relationships were frequently overlooked in the theoretical models applied in the interventions [33, 35]. These irregularities in quality assessment signify that two improvements are needed for better reporting and replication across intervention studies, namely sociocultural sensitivity and theoretical context of relationship dynamics.
We first recommend that interventions adapt a more socioculturally sensitive approach by considering both partners’ cumulative education levels in coordination with other demographic characteristics of the local target populations, such as income level and sexual orientation. Although heterosexual couples are disproportionately represented in these 11 interventions, the target participants were often subgroups of populations impacted by low income, poor housing (including homelessness), or domestic violence [32, 33]. Moreover, only a few past and ongoing studies focus on partner concurrency [18] and male couples [38, 48], and even fewer on drug users and their sexual partners [32, 33] or transgender women and their sexual partners [49, 50]. The scarcity of couple-based RCTs in key populations has become a pressing research concern given the central role that HIV prevention plays in these key populations’ partnerships. Although researchers need to design intervention protocols with clear linkages to outcome variables, it is also critical to incorporate participants’ backgrounds and interpersonal relationships within intervention strategies and customize protocols to meet couple-based participants’ specific needs.
We also suggest that interventions may benefit from more thoroughly considering relationship dynamics in a broader theoretical context. One way to do this is to identify appropriate outcome measures based on the couple’s interdependence within dyadic coping perspectives [4]. To date, intervention studies have mainly used outcome measures and statistical methods to indicate individual-level behavioral change. Although researchers have made enormous efforts to design and implement core behavioral intervention components (e.g., skills-building for couples), none of the studies included in this review evaluated the dyadic outcomes, such as relationship quality [51] and sexual agreement [52] between partners. However, it is reassuring to note that in a recent dyadic intervention for improvement of HIV care engagement among HIV-serodiscordant male couples, Stephenson and colleagues (2017) [53] adopted a framework grounded in Couple’s Interdependence Theory [19] and selected dyadic measures of behavioral change within the couple.
Another method is to explore theories that integrate relationship dynamics and HIV prevention. There is a large gap between theories construing the relationship dynamics that may influence the transformation of motivation and health behavior, especially among same-sex couples in an HIV-serodiscordant relationship. A recent qualitative study revealed how “viral load agreements” facilitate the practice of different strategies in undetectable viral load for prevention among gay male couples [8], shedding new light on the development of theoretical constructs. Future RCTs may integrate renewed dyadic constructs into their interventions [54] following dyadic theoretical models such as the systemic transactional model [55] and the dyadic health model [56]. Researchers may also consider the relational dynamic characteristics of other key populations when tailoring interventions for the specific groups, such as interpersonal dynamics-based detoxification of injecting drug users [57], gender roles of transgender women [49], and intimate partner violence experienced by female sex workers [58].
Limitations
There are some limitations to this study. First, a relatively small number of RCTs are available, limiting the statistical power for subgroup meta-analysis and meta-regression. Second, because all 11 studies were conducted in the USA and Africa, the conclusions drawn in this study may not be generalizable to, or adequately representative of, other world regions. Third, given that most studies have been exclusively targeted at heterosexual couples, there is an urgent need for more robust bodies of evidence on the effect of intervention studies on more diverse populations. In the future, with more original RCTs assessing intervention effects among key populations from more global perspectives, an updated meta-analysis would provide more evidence of the sustainable impact of couple-based interventions.
Conclusions
In this systematic review and meta-analysis, couple-based interventions are more efficacious than individual-level interventions in biobehavioral HIV prevention. The intervention effect of couple-based HIV prevention RCTs will be improved by considering sociocultural sensitivities and theoretical contexts in relationship dynamics. Finally, couple-based HIV prevention RCTs are still in their infancy, and studies among key populations (i.e., MSM, injecting drug users, sex workers, and transgender women) warrant further investigation.
Data Availability
The study was pre-registered at the PROSPERO database (CRD42020222819, https://www.crd.york.ac.uk/PROSPERO/). Materials used to conduct the study are publically available at Open Science Framework (Identifier: https://doi.org/10.17605/OSF.IO/7NBJK, https://osf.io/7nbjk/?view_only=eb5a91ea50b74c90b6999237c8795f85).
Change history
23 May 2023
A Correction to this paper has been published: https://doi.org/10.1007/s10461-023-04080-6
References
UNAIDS. Seizing the moment: tackling entrenched inequalities to end epidemics. Geneva: UNAIDS; 2020.
Rusbult CE, Van Lange PAM. Interdependence, interaction, and relationships. Annu Rev Psychol. 2003;54:351–75.
Karney BR, Hops H, Redding CA, Reis HT, Rothman AJ, Simpson JA. A framework for incorporating dyads in models of HIV-prevention. AIDS Behav. 2010;14:189–203.
Gamarel KE, Revenson TA. Dyadic adaptation to chronic illness: the importance of considering context in understanding couples’ resilience. In: Skerrett K, Fergus K, editors. Couple resilience. Berlin: Springer; 2015. p. 83–105.
Koff A, Goldberg C, Ogbuagu O. Condomless sex and HIV transmission among serodifferent couples: current evidence and recommendations. Ann Med. 2017;49:534–44.
Remien RH, Carballo-Dieguez A, Wagner G. Intimacy and sexual risk behaviour in serodiscordant male couples. AIDS Care. 1995;7:429–38.
Hoff CC, Chakravarty D, Beougher SC, Darbes LA, Dadasovich R, Neilands TB. Serostatus differences and agreements about sex with outside partners among gay male couples. AIDS Educ Prev. 2009;21:25–38.
Philpot SP, Prestage G, Ellard J, Grulich AE, Bavinton BR, Grulich AE, et al. How do gay serodiscordant couples in Sydney, Australia negotiate undetectable viral load for HIV prevention? AIDS Behav. 2018;22:3981–90.
Villar-Loubet OM, Bruscantini L, Shikwane ME, Weiss S, Peltzer K, Jones DL. HIV disclosure, sexual negotiation and male involvement in prevention-of-mother-to-child-transmission in South Africa. Cult Health Sex. 2013;15:253–68.
Rodger AJ, Cambiano V, Bruun T, Vernazza P, Collins S, Degen O, et al. Risk of HIV transmission through condomless sex in serodifferent gay couples with the HIV-positive partner taking suppressive antiretroviral therapy (PARTNER): final results of a multicentre, prospective, observational study. Lancet. 2019;393:2428–38.
Ngure K, Ongolly F, Dolla A, Awour M, Mugwanya KK, Irungu E, et al. “I just believe there is a risk” understanding of undetectable equals untransmissible (U = U) among health providers and HIV-negative partners in serodiscordant relationships in Kenya. J Int AIDS Soc. 2020;23: e25466.
Krakowiak D, Kinuthia J, Osoti AO, Asila V, Gone MA, Mark J, et al. Home-based HIV testing among pregnant couples increases partner testing and identification of serodiscordant partnerships. J Acquir Immune Defic Syndr. 2016;72:S167–73.
Fonner VA, Ntogwisangu J, Hamidu I, Joseph J, Fields J, Evans E, et al. “We are in this together:” dyadic-level influence and decision-making among HIV serodiscordant couples in Tanzania receiving access to PrEP. BMC Public Health. 2021;21:1–1.
Crepaz N, Tungol-Ashmon MV, Vosburgh HW, Baack BN, Mullins MM. Are couple-based interventions more effective than interventions delivered to individuals in promoting HIV protective behaviors? A meta-analysis. AIDS Care. 2015;27:1361–6.
Bothwell LE, Greene JA, Podolsky SH, Jones DS. Assessing the gold standard lessons from the history of RCTs. N Engl J Med. 2016;374:2175–81.
Jiwatram-Negrón T, El-Bassel N. Systematic review of couple-based HIV intervention and prevention studies: advantages, gaps, and future directions. AIDS Behav. 2014;18:1864–87.
Burton J, Darbes LA, Operario D. Couples-focused behavioral interventions for prevention of HIV: systematic review of the state of evidence. AIDS Behav. 2010;14:1.
LaCroix JM, Pellowski JA, Lennon CA, Johnson BT. Behavioural interventions to reduce sexual risk for HIV in heterosexual couples: a meta-analysis. Sex Transm Infect. 2013;89:620–7.
Lewis MA, McBride CM, Pollak KI, Puleo E, Butterfield RM, Emmons KM. Understanding health behavior change among couples: an interdependence and communal coping approach. Soc Sci Med. 2006;62:1369–80.
Ryff CD, Singer B. Interpersonal flourishing: a positive health agenda for the new millennium. Pers Soc Psychol Rev. 2000;4:30–44.
Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. 2014;348:g1687–97.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88: 105906.
Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21:1539–58.
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34.
Hou J, Jiang T, Fu J, Su B, Wu H, Sun R, et al. The long-term efficacy of working memory training in healthy older adults: a systematic review and meta-analysis of 22 randomized controlled trials. J Gerontol Ser B. 2020;75:e174–88.
Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane handbook for systematic reviews of interventions. London: Wiley; 2019.
Jiang T, Hou J, Sun R, Dai L, Wang W, Wu H, et al. Immunological and psychological efficacy of meditation/yoga intervention among people living with HIV (PLWH): a systematic review and meta-analyses of 19 randomized controlled trials. Ann Behav Med. 2021;55:505–19.
Becker S, Mlay R, Schwandt HM, Lyamuya E. Comparing couples’ and individual voluntary counseling and testing for HIV at antenatal clinics in Tanzania: a randomized trial. AIDS Behav. 2010;14:558–66.
Coates TJ, Grinstead OA, Gregorich SE, Sweat M, Kamenga M, Sangiwa G, et al. Efficacy of voluntary HIV-1 counselling and testing in individuals and couples in Kenya, Tanzania, and Trinidad: a randomised trial. Lancet. 2000;356:103.
El-Bassel N, Witte SS, Gilbert L, Wu E, Chang M, Hill J, et al. The efficacy of a relationship-based HIV/STD prevention program for heterosexual couples. Am J Public Health. 2003;93:963–9.
El-Bassel N, Jemmott JB, Landis JR, Pequegnat W, Wingood GM, Wyatt GE, et al. National Institute of Mental Health Multisite Eban HIV/STD prevention intervention for African American HIV serodiscordant couples: a cluster randomized trial. Arch Intern Med. 2010;170:1594–601.
El-Bassel N, Gilbert L, Wu E, Witte SS, Chang M, Hill J, et al. Couple-based HIV prevention for low-income drug users from New York city: a randomized controlled trial to reduce dual risks. J Acquir Immune Defic Syndr. 2011;58:198–206.
Jones DL, Kashy D, Villar-Loubet OM, Cook R, Weiss SM. The impact of substance use, sexual trauma, and intimate partner violence on sexual risk intervention outcomes in couples: a randomized trial. Ann Behav Med. 2013;45:318–28.
McMahon JM, Tortu S, Pouget ER, Torres L, Rodriguez W, Hamid R. Effectiveness of couple-based HIV counseling and testing for women substance users and their primary male partners: a randomized trial. Adv Prev Med. 2013;2013:1–5.
Remien RH, Stirratt MJ, Dolezal C, Dognin JS, Wagner GJ, Carballo-Dieguez A, et al. Couple-focused support to improve HIV medication adherence: a randomized controlled trial. AIDS. 2005;19:807–14.
Sharma V, Leight J, Verani F, Tewolde S, Deyessa N. Effectiveness of a culturally appropriate intervention to prevent intimate partner violence and HIV transmission among men, women, and couples in rural Ethiopia: findings from a cluster-randomized controlled trial. PLoS Med. 2020;17: e1003274.
Speizer IS, Zule WA, Carney T, Browne FA, Ndirangu J, Wechsberg WM. Changing sex risk behaviors, gender norms, and relationship dynamics among couples in Cape Town, South Africa: efficacy of an intervention on the dyad. Soc Sci Med. 2018;209:95–103.
Sullivan PS, White D, Rosenberg ES, Barnes J, Jones J, Dasgupta S, et al. Safety and acceptability of couples HIV testing and counseling for US men who have sex with men: a randomized prevention study. J Int Assoc Provid AIDS Care. 2014;13:135–44.
Beougher SC, Gómez W, Hoff CC. The couple as context: Latino gay male couples and HIV. Cult Health Sex. 2011;13:299.
Mitchell JW. Characteristics and allowed behaviors of gay male couples’ sexual agreements. J Sex Res. 2014;51:316.
Karim QA, Karim SS, Soldan K, Zondi M. Reducing the risk of HIV infection among South African sex workers: socioeconomic and gender barriers. Am J Public Health. 1995;85:1521–5.
Garcia-Moreno C, Jansen HA, Ellsberg M, Heise L, Watts CH. Prevalence of intimate partner violence: findings from the WHO multi-country study on women’s health and domestic violence. Lancet. 2006;368:1260–9.
Painter TM. Voluntary counseling and testing for couples: a high-leverage intervention for HIV/AIDS prevention in sub-Saharan Africa. Soc Sci Med. 2001;53:1397–411.
Desgrées-du-Loû A, Orne-Gliemann J. Couple-centred testing and counselling for HIV serodiscordant heterosexual couples in sub-Saharan Africa. Reprod Health Matters. 2008;16:151–61.
Firestone R, Rivas J, Lungo S, Cabrera A, Ruether S, Wheeler J, et al. Effectiveness of a combination prevention strategy for HIV risk reduction with men who have sex with men in Central America: a mid-term evaluation. BMC Public Health. 2014;14:1244.
Corbett EL, Makamure B, Cheung YB, Dauya E, Matambo R, Bandason T, et al. HIV incidence during a cluster-randomized trial of two strategies providing voluntary counselling and testing at the workplace Zimbabwe. AIDS. 2007;21:483–9.
Sharma A, Kahle E, Sullivan S, Stephenson R. Relationship characteristics associated with perceptions of partners’ HIV testing behavior among male couples. AIDS Behav. 2020;24:516–31.
Stephenson R, Garofalo R, Sullivan PS, Hidalgo MA, Bazzi AR, Hoehnle S, et al. Stronger together: results from a randomized controlled efficacy trial of a dyadic intervention to improve engagement in HIV care among serodiscordant male couples in three US cities. AIDS Behav. 2021;25:2369–81.
Operario D, Gamarel KE, Iwamoto M, Suzuki S, Suico S, Darbes L, et al. Couples-focused prevention program to reduce HIV risk among transgender women and their primary male partners: feasibility and promise of the couples HIV intervention program. AIDS Behav. 2017;21:2452–63.
Gamarel KE, Sevelius JM, Neilands TB, Kaplan RL, Johnson MO, Nemoto T, et al. Couples-based approach to HIV prevention for transgender women and their partners: study protocol for a randomised controlled trial testing the efficacy of the “It Takes Two” intervention. BMJ Open. 2020;10: e038723.
Hahlweg K. Fragebogen zur partnerschaftsdiagnostik: (FPD); handanweisung. 1996. p. 45.
Hoff CC, Beougher SC. Sexual agreements among gay male couples. Arch Sex Behav. 2010;39:774–87.
Stephenson R, Suarez NA, Garofalo R, Hidalgo MA, Hoehnle S, Thai J, et al. Project stronger together: protocol to test a dyadic intervention to improve engagement in HIV care among sero-discordant male couples in three US cities. JMIR Res Protoc. 2017;6: e7884.
Salazar LF, Stephenson RB, Sullivan PS, Tarver R. Development and validation of HIV-related dyadic measures for men who have sex with men. J Sex Res. 2013;50:164–77.
Bodenmann G, Randall AK, Falconier MK. Coping in couples: the systemic transactional model (STM). London: Routledge/Taylor & Francis Group; 2016. p. 5–22.
Newcomb ME. Romantic relationships and sexual minority health: a review and description of the Dyadic Health Model. Clin Psychol Rev. 2020;82: 101924.
Simmons J, Singer M. I love you … and heroin: care and collusion among drug-using couples. Subst Abuse Treat Prev Policy. 2006;1:7.
Ulibarri MD, Strathdee SA, Lozada R, Magis-Rodriguez C, Amaro H, O’Campo P, et al. Intimate partner violence among female sex workers in two Mexico. S. Border cities: partner characteristics and HIV risk behaviors as correlates of abuse. Psychol Trauma. 2010;2:318–25.
Acknowledgements
We thank Runsong Sun of the National Key Laboratory of Cognitive Neuroscience and Learning, Beijing Normal University for his contribution to data search and technical support.
Funding
This study was funded by a Grant from the Research Grants Council of the Hong Kong Special Administrative Region, P. R. China (Project No. CityU 11600617).
Author information
Authors and Affiliations
Contributions
RF, JH, and NXY conceived of the study; RF and JH did data coding, conducted analyses, and provided technical and material support; NXY, YG, RF, and JH contributed to interpretation of results and conclusions; RF and JH drafted the manuscript; all authors contributed to manuscript review and editing. We confirm that the manuscript has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed. We further confirm that the order of authors listed in the manuscript has been approved by all of us.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised: Author has opted for open access on 27th April 2023.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Fu, R., Hou, J., Gu, Y. et al. Do Couple-Based Interventions Show Larger Effects in Promoting HIV Preventive Behaviors than Individualized Interventions in Couples? A Systematic Review and Meta-analysis of 11 Randomized Controlled Trials. AIDS Behav 27, 314–334 (2023). https://doi.org/10.1007/s10461-022-03768-5
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-022-03768-5