
Abstract
An increasing number of intermediate risk asymptomatic subjects benefit from measures of atherosclerosis burden like coronary artery calcification studies with non-contrast heart computed tomography (CT). However, additional information can be derived from these studies, looking beyond the coronary arteries and without exposing the patients to further radiation. We report a semi-automatic method that objectively assesses ascending, arch and descending aorta dimension and shape from non-contrast CT datasets to investigate the effect of aging on thoracic aorta geometry. First, the segmentation process identifies the vessel centerline coordinates following a toroidal path for the curvilinear portion and axial planes for descending aorta. Then, reconstructing oblique planes orthogonal to the centerline direction, it iteratively fits circles inside the vessel cross-section. Finally, regional thoracic aorta dimensions (diameter, volume and length) and shape (vessel curvature and tortuosity) are calculated. A population of 200 normotensive men was recruited. Length, mean diameter and volume differed by 1.2 cm, 0.13 cm and 21 cm3 per decade of life, respectively. Aortic shape uncoiled with aging, reducing its tortuosity and increasing its radius of curvature. The arch was the most affected segment. In conclusion, non-contrast cardiac CT imaging can be successfully employed to assess thoracic aorta 3D morphometry.




Similar content being viewed by others


References
Agmon, Y., B. K. Khandheria, I. Meissner, G. L. Schwartz, J. D. Sicks, A. J. Fought, W. M. O’Fallon, D. O. Wiebers, and A. J. Tajik. Is aortic dilatation an atherosclerosis-related process? Clinical, laboratory, and transesophageal echocardiographic correlates of thoracic aortic dimensions in the population with implications for thoracic aortic aneurysm formation. J. Am. Coll. Cardiol. 42(6):1076–1083, 2003.
Behrens, T., K. Rohr, and H. S. Stiehl. Robust segmentation of tubular structures in 3-D medical images by parametric object detection and tracking. IEEE Trans. Syst. Man Cybern. B Cybern. 33(4):554–561, 2003.
Budoff, M. J., and K. M. Gul. Expert review on coronary calcium. Vasc. Health Risk Manag. 4(2):315–324, 2008.
Chironi, G., L. Orobinskaia, J. L. Megnien, M. E. Sirieix, S. Clement-Guinaudeau, M. Bensalah, A. Azarine, E. Mousseaux, and A. Simon. Early thoracic aorta enlargement in asymptomatic individuals at risk for cardiovascular disease: determinant factors and clinical implication. J. Hypertens. 28(10):2134–2138, 2010.
Choi, G., C. Cheng, N. Wilson, and C. Taylor. Methods for quantifying three-dimensional deformation of arteries due to pulsatile and nonpulsatile forces: implications for the design of stents and stent grafts. Ann. Biomed. Eng. 37(1):14–33, 2009.
Chyu, K. Y., and P. K. Shah. Emerging therapies for atherosclerosis prevention and management. Cardiol. Clin. 29(1):123–135, 2011.
de Bruijne, M., B. van Ginneken, M. A. Viergever, and W. J. Niessen. Adapting active shape models for 3D segmentation of tubular structures in medical images. Inf. Process. Med. Imaging 18:136–147, 2003.
Dotter, C. T., D. J. Roberts, and I. Steinberg. Aortic length: angiocardiographic measurements. Circulation 2(6):915–920, 1950.
Elefteriades, J. A., and E. A. Farkas. Thoracic aortic aneurysm clinically pertinent controversies and uncertainties. J. Am. Coll. Cardiol. 55(9):841–857, 2010.
Frangi, A. F., W. J. Niessen, R. M. Hoogeveen, T. van Walsum, and M. A. Viergever. Model-based quantitation of 3-D magnetic resonance angiographic images. IEEE Trans. Med. Imaging 18(10):946–956, 1999.
Funka-Lea, G., Y. Boykov, C. Florin, M. P. Jolly, R. Moreau-Gobard, R. Ramaraj, and D. Rinck. Automatic heart isolation for CT coronary visualization using graph-cuts. In: Biomedical Imaging: Nano to Macro, 2006. 3rd IEEE International Symposium on, 2006, pp. 614–617.
Gentile, B. J., D. R. Gross, C. J. Chuong, and N. H. Hwang. Segmental volume distensibility of the canine thoracic aorta in vivo. Cardiovasc. Res. 22(6):385–389, 1988.
Giulini, S. M., and S. Bonardelli. Post-traumatic lesions of the aortic isthmus. Ann. Ital. Chir. 80(2):89–100, 2009.
Greenland, P., J. S. Alpert, G. A. Beller, E. J. Benjamin, M. J. Budoff, Z. A. Fayad, E. Foster, M. A. Hlatky, J. M. Hodgson, F. G. Kushner, et al. ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 56(25):e50–e103, 2010.
Greenland, P., S. C. Smith, Jr., and S. M. Grundy. Improving coronary heart disease risk assessment in asymptomatic people: role of traditional risk factors and noninvasive cardiovascular tests. Circulation 104(15):1863–1867, 2001.
Kannel, W. B., R. B. D’Agostino, L. Sullivan, and P. W. Wilson. Concept and usefulness of cardiovascular risk profiles. Am. Heart J. 148(1):16–26, 2004.
Kovács, T. Automatic segmentation of the vessel lumen from 3D CTA images of aortic dissection. In: Selected Readings in Vision and Graphics, edited by L. Van Gool, G. Székely, M. Gross, and B. Schiele. Konstanz: Hartung-Gorre Verlag, 2010.
Kurkure, U., O. C. Avila-Montes, and I. A. Kakadiaris. Automated segmentation of thoracic aorta in non-contrast CT images. In: Biomedical Imaging: From Nano to Macro, 2008. ISBI 2008. 5th IEEE International Symposium on, 2008, pp. 29–32.
Mao, S. S., N. Ahmadi, B. Shah, D. Beckmann, A. Chen, L. Ngo, F. R. Flores, Y. L. Gao, and M. J. Budoff. Normal thoracic aorta diameter on cardiac computed tomography in healthy asymptomatic adults: impact of age and gender. Acad. Radiol. 15(7):827–834, 2008.
Muntendam, P., C. McCall, J. Sanz, E. Falk, and V. Fuster. The BioImage Study: novel approaches to risk assessment in the primary prevention of atherosclerotic cardiovascular disease—study design and objectives. Am. Heart J. 160(1):49–57e41, 2010.
O’Rourke, M., A. Farnsworth, and J. O’Rourke. Aortic dimensions and stiffness in normal adults. JACC Cardiovasc. Imaging 1(6):749–751, 2008.
Patel, D. J., A. J. Mallos, and D. L. Fry. Aortic mechanics in the living dog. J. Appl. Physiol. 16:293–299, 1961.
Roger, V. L., A. S. Go, D. M. Lloyd-Jones, R. J. Adams, J. D. Berry, T. M. Brown, M. R. Carnethon, S. Dai, G. de Simone, E. S. Ford, et al. Heart disease and stroke statistics–2011 update: a report from the American Heart Association. Circulation 123(4):e18–e209, 2011.
Rueckert, D., P. Burger, S. M. Forbat, R. D. Mohiaddin, and G. Z. Yang. Automatic tracking of the aorta in cardiovascular MR images using deformable models. IEEE Trans. Med. Imaging 16(5):581–590, 1997.
Rumberger, J. A. Using noncontrast cardiac CT and coronary artery calcification measurements for cardiovascular risk assessment and management in asymptomatic adults. Vasc. Health Risk Manag. 6:579–591, 2010.
Schwartz, E., R. Gottardi, J. Holfeld, C. Loewe, M. Czerny, and G. Langs. Evaluating deformation patterns of the thoracic aorta in gated CTA sequences. In: Biomedical Imaging: From Nano to Macro, 2010 IEEE International Symposium on, 2010, pp. 21–24.
Shah, P. K. Screening asymptomatic subjects for subclinical atherosclerosis: can we, does it matter, and should we? J. Am. Coll. Cardiol. 56(2):98–105, 2010.
Sugawara, J., K. Hayashi, T. Yokoi, and H. Tanaka. Age-associated elongation of the ascending aorta in adults. J. Am. Coll. Cardiol. Imaging 1(6):739–748, 2008.
Thomas, J. B., L. Antiga, S. L. Che, J. S. Milner, D. A. Steinman, J. D. Spence, and B. K. Rutt. Variation in the carotid bifurcation geometry of young versus older adults: implications for geometric risk of atherosclerosis. Stroke 36(11):2450–2456, 2005.
Vasan, R. S., M. G. Larson, and D. Levy. Determinants of echocardiographic aortic root size. The Framingham Heart Study. Circulation 91(3):734–740, 1995.
Wolak, A., H. Gransar, L. E. J. Thomson, J. D. Friedman, R. Hachamovitch, A. Gutstein, L. J. Shaw, D. Polk, N. D. Wong, R. Saouaf, et al. Aortic size assessment by noncontrast cardiac computed tomography: normal limits by age, gender, and body surface area. JACC Cardiovasc. Imaging 1(2):200–209, 2008.
Wood, N. B., S. Z. Zhao, A. Zambanini, M. Jackson, W. Gedroyc, S. A. Thom, A. D. Hughes, and X. Y. Xu. Curvature and tortuosity of the superficial femoral artery: a possible risk factor for peripheral arterial disease. J. Appl. Physiol. 101(5):1412–1418, 2006.
Worz, S., H. von Tengg-Kobligk, V. Henninger, F. Rengier, H. Schumacher, D. Bockler, H. U. Kauczor, and K. Rohr. 3-D quantification of the aortic arch morphology in 3-D CTA data for endovascular aortic repair. IEEE Trans. Biomed. Eng. 57(10):2359–2368, 2010.
Zhao, F., H. Zhang, A. Wahle, M. T. Thomas, A. H. Stolpen, T. D. Scholz, and M. Sonka. Congenital aortic disease: 4D magnetic resonance segmentation and quantitative analysis. Med. Image Anal. 13(3):483–493, 2009.
Acknowledgments
This work was supported by the project PIP number 112-200901-00734 (CONICET) and the Houssay post-doctoral program (CONICET).
Author information
Authors and Affiliations
Corresponding author
Additional information
Associate Editor Joan Greve oversaw the review of this article.
Appendix
Appendix
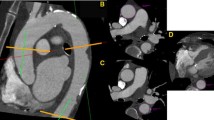
The curvilinear portion of the thoracic aorta was analyzed reconstructing oblique planes that turned around the mid-point between centerline coordinates C A and C D as shown in Fig. 1b. Starting from an axial plane P 0, that contain C A and C D, the algorithm makes a fixed translation-rotation and a subsequent dynamic rotation pivoting around the center of the aortic arch.
The plane P 0 was defined as:
where \( \hat{x}, \hat{y} \) and \( \hat{z} \) are the unit vectors of the 3D euclidean space along the coronal, sagital and axial directions of the CT volume, \( z_{{C_{\text{A}} ,C_{\text{D}} }} \) is the z-coordinate of the slice containing C A and C D and parameters λ, ɛ are such that:
P 0 was first translated and rotated with the following transformation
where \( \left\langle {P_{0} } \right\rangle \) is the center-point of the plane P 0 and \( R_{{\alpha ,\hat{z}}} \) is the rotation matrix
that aligns P 0 with the vector connecting C A and C D. Accordingly, angle α was calculated as:
Finally, the resulting plane was sequentially rotated in 2° steps, using the transformation
where \( R_{{\theta_{i},u}} \) is the rotation matrix:
which performs a rotation of θ degrees around the axis u, orthogonal to the segment \( \overline{{C_{\text{A}} - C_{\text{D}} }} \) and the unit vector \( \hat{z} \), calculated from the following a vector product:
The curvilinear path of the thoracic aorta was covered assigning values of θ i angle from 0° to 240°.
Rights and permissions
About this article
Cite this article
Craiem, D., Chironi, G., Redheuil, A. et al. Aging Impact on Thoracic Aorta 3D Morphometry in Intermediate-Risk Subjects: Looking Beyond Coronary Arteries with Non-Contrast Cardiac CT. Ann Biomed Eng 40, 1028–1038 (2012). https://doi.org/10.1007/s10439-011-0487-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10439-011-0487-y