
Abstract
To evaluate the anatomical aspects and relations of a modified tissue passage with the tension-free vaginal tape obturator (TVT-O) needle, designed for the purpose of reduction of the thigh pain, related with this anti-urinary incontinence operation. The distances between the modified TVT-O surgically inserted needle and obturator nerve branches were measured in fresh cadaver. The introduced surgical needle caused no trauma to any of the adjacent cadaveric organs, and the distances between the surgical needle and the obturator nerve branches was 4 cm. The modified TVT-O needle route is shown to be safe and remote from the obturator nerve branches, thus conduction of a clinical study for evaluation of related pain reduction is recommended.
Similar content being viewed by others


Introduction
The tension-free vaginal tape (TVT) has been used since described by Ulmsten at 1996 for the treatment of female stress urinary incontinence. This mid-urethral Prolene tape support operation is now accepted worldwide as an easy-to-learn, effective, and safe surgical procedure [1–5]. However, the TVT harbors few typical operative complications such as bladder penetration (4–8%), urinary outlet obstruction (2%–5%), and rare occurrence of bowel penetration, intra-operative bleeding, and postoperative infections [2, 3, 5–10]. That reality led Delorme to design a novel mid-urethral sling in the form of a trans-obturator TVT-like procedure (2001). In such, the TVT needle bypasses the retro-pubic area, which is in proximity with the bladder, bowel, and blood vessels, by making the needle pass through the relatively safe medial compartment of the obturator fossa area, remote from the pelvic viscera and vessels [11]. This trans-obturator tape (TOT) outside-in operation was shown to be safe minimally invasive anti-incontinence procedure, yet related bladder injuries were reported [12–16]. Two years later, De Leval presented an inside-out approach, the tension-free vaginal tape obturator (TVT-O), aimed to reduce the bladder injury rate [17, 18]. This TVT-O was later claimed to cause perioperative thigh pain [19, 20]. Flam then raised the idea that the TVT-O-related thigh pain might be attributed to the oblique, thus long, path of the TVT-O needle through muscles and connective tissue at the obturator foramen. Long needle path was thought to entail heavy tissue damage and cause high related pain levels. Additionally, the rather close proximity of the surgical TVT-O needle to the obturator nerve branches might aggravate the perioperative pain. Flam designed a perpendicular TVT-O needle passage through the obturator foramen to yield a shorter route for this inside-out procedure. Flam passed the TVT-O needle as close as possible to the inferior pubic ramus and with a skin exit at the outer aspect of the labia majora rather than laterally to the inguinal fold, as described by De Leval earlier [21]. This alternative route was aimed to extend the distance between the needle and the obturator nerve branches as well.
Methods
The second author performed the TVT-O with the Flam method (TVT-O FM) in an anatomic laboratory on a fresh cadaver (legs positioned at 90° flexion and 30° abduction with the hip joint). The TVT-O FM differs from the De Leval method with the needle passage, being as close to the inferior pubic ramus as possible, exiting the skin not laterally to the inguinal fold as with De Leval but at the major labia. The obturator area crossing is perpendicular rather than tangential, making the throughway shorter. Achieving these required changes with De Leval’s angle of the needle handle: instead of introducing it at a 30° angle to penetrating the obturator membrane, it is inserted at 75° (see Figs. 1, 2, 3, 4). The distances between the needle and the obturator nerve and vessels branches were measured at the fresh cadaver right after dissection of the adductor region.

De Leval’s TVT-O technique

Flam’s TVT-O FM technique

TVT-O FM procedural steps: (1, 2) insertion, (3, 4) advancing and exiting the surgical needle

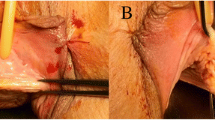
Relations between the surgical needle with TVT-O FM and the obturator nerve branches. RA Right anterior, RP right posterior, LA left anterior, LP left posterior
Results
Introducing the TVT-O surgical needles by Flam’s modification to the obturator foramen did not endanger the surrounding organs. The passage through the muscular and connective tissue was perpendicular for shortening the path. The distances measured between the surgical needle passed by the TVT-O FM technique and the obturator nerve and vessels branches were 40 mm on both sides.
Discussion
Delorme and De Leval launched outside-in (TOT) and inside-out (TVT-O) trans-obturator submid-urethral supportive tape anti-incontinence procedures to avoid the TVT aforementioned complications. This included bladder penetration, intra-operative bleeding, postoperative field infection, and bowel injury [1–3, 5–10]. The TVT-O was thought to be less hazardous than the TOT to the bladder, yet it was accused to induce postoperative thigh neuralgia [19, 20]. The close similarity with the accurate needle passage of the TOT, which was not reported to cause postoperative pain, and the TVT-O FM grounded the hypothesis of thigh pain reduction with the proposed surgical method. Thus, the TVT-O FM [21] proposes an alternative to the original TVT-O inside-out needle passage for the reduction of the tissue damage and related pain. Since 2005, Dr. Flam has performed about 2,500 such procedures, with no clinical evidence of nerve or large vessel damage and with reduced postoperative thigh pain occurrence (personal communications). This might be explained now by a shorter pass through the obturator tissues as well as by an increased distance between the TVT-O FM surgical needle and the obturator nerve branches (4 cm) in comparison with De Leval’s technique (2 cm) [17].The present cadaveric study results proves the TVT-O FM safety and indicates a clinical trial. Usually, more than one cadaver study would be recommended for showing reasonable surgical safety bounders, yet the definitely large safety margins found with this single cadaver overcame potential individual anatomical variations.
Conclusion
Our data support the notion that the TVT-O FM procedure draws safety margins for this procedure in terms of the hazards to obturator bundle branches, thus a clinical study is recommended here.
References
Ulmsten U, Henriksson L, Johnson P, Varhos G (1996) An ambulatory surgical procedure under local anesthesia for treatment of female urinary incontinence. Int Urogynecol J 7:81–86
Olsson I, Kroon U (1999) A three-year postoperative evaluation of tension-free vaginal tape. Gynecol Obstet Investig 48(4):267–269
Kuuva N, Nilsson CG (2002) A nationwide analysis of complications associated with the tension-free vaginal tape (TVT) procedure. Acta Obstet Gynecol Scand 81:72–77
Paraiso MFR, Muir TW, Sokol AI (2002) Are midurethral slings the gold standard surgical treatment for primary genuine stress incontinence? J Am Assoc Gynecol Laparosc 9(4):405–407
Waetjen LE, Subak LL, Shen H et al (2003) Stress urinary incontinence surgery in the United States. Obstet Gynecol 101:671–676
Neuman M (2004) Tension-free vaginal tape bladder penetration and long-lasting trans-vesical Prolene material. J Pelvic Med Surg 10(6):307–309
Neuman M (2004) Post tension-free vaginal tape voiding difficulties – prevention and management. J Pelvic Med Surg 10:19–21
Neuman M (2002) Infected hematoma following tension-free vaginal tape implantation. J Urol 168(6):2549
Grise P, Lobel B, Grall J (2003) Les complicasions du TVT. Prog Urol 13(1):144–146
Nygaard IE, Heit M (2004) Stress urinary incontinence. Obstet Gynecol 104:607–620
Delorme E (2001) Transobturator urethral suspension: a minimally invasive procedure to treat female stress urinary incontinence. Prog Urol 11:1306–1313
Hermieu JF, Messas A, Delmas V et al (2003) Bladder injury after TVT transobturator. Prog Urol 13(1):115–117
Minaglia S, Ozel B, Klutke C et al (2004) Bladder injury during transobturator sling. Urology 64(2):376–377
Deval B, Ferchaux J, Berry R et al (2006) Objective and subjective cure rates after trans-obturator tape (OBTAPE) treatment of female urinary incontinence. Eur Urol 49(2):373–377
Fischer A, Fink T, Zachmann S et al (2005) Comparison of retro-pubic and outside-in trans-obturator sling systems for the cure of female genuine stress urinary incontinence. Eur Urol 48(5):799–804
Roumeguere T, Quackels T, Bollens R et al (2005) Trans-obturator vaginal tape (TOT) for female stress incontinence: one year follow-up in 120 patients. Eur Urol 48(5):805–809
De Leval J (2003) Novel surgical technique for the treatment of female stress urinary incontinence: transobturator vaginal tape inside-out. Eur Urol 44:724–730
Neuman M (2007) TVT and TVT-obturator: comparison of two operative procedures. Eur J Obstet Gynecol Reprod Biol 131(1):89–92
Debodinance P (2007) Trans-obturator urethral sling for the surgical correction of female stress urinary incontinence: outside-in (Monarc) versus inside-out (TVT-O). Are the two ways reassuring? Eur J Obstet Gynecol Reprod Biol 133(2):232–238
Wang W, Zhu L, Lang J (2009) Trans-obturator tape procedure versus tension free vaginal for treatment of stress urinary incontinence. Int J Gynecol Obstet 104(2):113–116
Neuman M, Sosnovski V, Bornstein J et al (2009) Avoiding thigh pain in trans-obturator anti-incontinence slings. Pelviperineology 28(3):69
Conflicts of interest
M. Neuman and A. Martan are consultants for Gynecare
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Neuman, M., Hubka, P., Martan, A. et al. Modified needle route for potential reduction of the trans-obturator inside-out-related thigh pain: a cadaveric study. Gynecol Surg 8, 171–174 (2011). https://doi.org/10.1007/s10397-010-0635-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10397-010-0635-7