
Abstract
Aim
This paper aims to better understand the relationship between homicide and other public health outcomes, by studying their trends over time.
Subject and methods
Research in both criminology and public health has long identified that crime and violence tend to cluster together with adverse phenomena in the social and health domains. However, such work has relied primarily on cross-sectional analyses. Here, we instead study trends over time. We take data from the Netherlands, between 2000 and 2020, and ask whether homicide shows similar trends over time as other public health phenomena – such as smoking behaviour, alcohol use, child mortality, adolescent pregnancies, and suicide.
Results
We observe, first, that all of the phenomena – with the exception of suicide – declined over the period under study. We then employ a time series analysis to examine whether these trends arise independently, or whether they are the result of structural similarities between phenomena. Results showed that the decline in homicide rates is linked to a similar decline in adolescent pregnancies – the rates of these phenomena ‘move together’ during the period under study.
Conclusion
This work shows that the phenomenon of homicide shares structural similarities with teenage pregnancies – a decline in one is linked to a similar decline in the other. More generally, the current work furthers our understanding of the place of homicide in the domain of (public) health.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Research in both criminology and public health has long shown that crime and violence tend to cluster together with adverse phenomena in the social and health domains. Where levels of crime and violence are high, other adverse outcomes also tend to be more prevalent. This basic observation that different adverse outcomes have a tendency to ‘cluster together’ has been observed in many different forms. It has been observed in the lives of individuals (Gottfredson and Hirschi 1990), at the level of communities (Wilson 1987) and counties (Ousey 2017). It has been observed in the form of crime and delinquency in general (van Nieuwenhuijzen et al. 2009), and in terms of violence and homicide more specifically (van Breen & Liem 2022). It has been observed in Europe (van Breen & Liem 2022), in the United States (Ousey 2017), in South America (Murray et al. 2013) and in South Africa (Gilbert 1996), as well as cross-nationally (Pickett et al. 2005).
In this paper, we aim to extend our understanding of the overlap between criminal violence (specifically homicide) and adverse outcomes in the social and health domain. Past literature on this topic has focused primarily on cross-sectional relationships (for an exception see Mark and Torrats-Espinosa 2022). We instead study time trends of homicide and other adverse health phenomena. We are interested in the extent to which homicide trends ‘moves together’ over time with trends in adverse phenomena outside the realm of crime. Specifically, based on previous literature, we compare rates of homicide to suicide (Unnithan et al. 1994), child mortality (Ousey 2017), adolescent pregnancy (Pickett et al. 2005), smoking behaviour (van Nieuwenhuijzen et al. 2009) and alcohol use (Ritter and Stompe 2013).
The benefit of studying time trends include, first, the fact that they offer a different perspective than cross-sectional analyses. Employing varied methods allows for a fuller understanding of the phenomena we are interested in. Second, specifically in the domain of adverse health outcomes and violence, time trends have perhaps more relevance than in other domains. Public health and violence are priority areas for policy, and areas of concern for the general public. As such, researchers and policy makers are particularly attuned to questions of whether these phenomena are increasing or decreasing over time, and if so, how these trends can be understood. For instance, in the criminological literature, much has been written about the decline in rates of homicide over recent decades, and how such evidence should be interpreted (Eisner 2003; Aebi and Linde 2014; Suonpää et al. 2022). Important for the current work is the fact that the criminological literature has also made use of formalised models to test and interpret these crime trends, by the use of time series models (Liu 2006; Cook and Cook 2011). Time series models are highly formalised, and allow us to formally separate random fluctuations in the data, from structural effects – thereby facilitating more robust interpretation. Here, we apply a time series model to better understand how trends in homicide overlap with trends in adverse health outcomes such as suicide, child mortality, adolescent pregnancy, smoking behaviour and alcohol use.
The current study
We take data from the Netherlands, between 2000 and 2020, to examine the relationships between the trends in homicide, and other adverse health outcomes in the social and health domains. We employ a time series analysis, specifically a co-integration test (Liu 2006). Time series analysis differentiates three main types of relationships between different trends. First, trends may converge (become more similar) over time. Second, trends may diverge (become less similar) over time. Third, trends may be in equilibrium, or ‘co-integrated’. Co-integration reflects a scenario where two trends move together over time, in other words, the difference between the trends is stable over time. For the purposes of the current study, then, we are interested in whether the different trends show evidence of co-integration.
We consider relationships between homicide and various adverse health outcomes, specifically adolescent pregnancies, alcohol use and smoking behaviour, as well as child mortality and suicide. In European literature, the relationship between homicide and child mortality tends to be less pronounced than it is in the U.S. (Chen et al. 2016; van Breen & Liem 2022). Still, we include child mortality for the purposes of clearer comparisons with U.S. work. Similar reasoning applies for suicide. While there is good reason to consider homicide and suicide as conceptually related (Unnithan et al. 1994), the empirical relationships between homicide and suicide tend to be less straightforward. For example, previous research has shown that homicide and suicide do not cluster together at the macro-level (van Breen & Liem 2022). Similarly, at the individual-level of analysis, recent work has shown that there is limited overlap between aggressive behaviour towards others and self-harm behaviours (Shafti et al. 2022). In sum, previous work has generated limited evidence for an empirical relationship between homicide and suicide, but we include it for the sake of completeness.
Based on these considerations, then, we hypothesise that there will be evidence for co-integration between rates of homicide and rates of (H1a) adolescent pregnancies, (H1b) heavy smoking, (H1c) heavy alcohol use, but not (H1d) child mortality or (H1e) suicide. Co-integration between the trends suggests that the different phenomena have a shared component and are responding to similar external influences.
Method
Time frame
In this work, we focus on a period of 21 years, from 2000 to 2020. For the purposes of time series analysis this is relatively short (but see Liu 2006). Data availability played a role in our choice for this timeframe. In more recent timeframes, more extensive and better quality data are available. To counter-balance this issue we chose to apply a relatively conservative test, which reduces the risk of false-positives and over-interpretation. The details of the test are given in the section Analytical Procedure below.
Variables and corresponding data sources
The data consists of population-level incidence data in aggregate form. For each of the indicators of central interest (outlined in detail below) we calculate rates per 100,000 of the population. The majority of the data is taken from Statistics Netherlands (Centraal Bureau voor Statistiek) – who offer an open data portal. The homicide data was taken from the Dutch Homicide Monitor (details below). Below, we describe each of the variables in turn.
Homicide
We obtained the homicide data for the period under study from the Dutch Homicide Monitor (DHM). The DHM draws on police sources triangulated with archival searches, to identify homicide incidents across the Netherlands from 1992 onwards. We extracted aggregate data showing the total number of people who were the victim of homicide in a given year between 2000 and 2020. We then calculate rates of homicide per 100,000 of the population in each year.
Suicide
We used suicide mortality per 100,000 of the population. These data were taken from Statistics Netherlands – reflecting individuals for whom the registered cause of death was suicide, in a given year. As before, we used general population statistics to calculate the suicide rate per 100,000.
Child mortality
Child mortality data was taken from Statistics Netherlands – reflecting all children who died at 5 years or younger in a given year. From this total we exclude child deaths as a result of homicide to prevent double counting of these cases.
Heavy smoking
Data on the prevalence of (heavy) smoking was taken from Statistics Netherlands. Heavy smokers are those individuals who smoke at least 20 cigarettes a day. Unlike suicide, homicide and adolescent pregnancies variables, the smoking variable is an estimate rather than an observation. Health surveys are distributed each year to a representative sample of the population, and those observations are then extrapolated to the whole population. We extracted the estimates of heavy smokers in the population, and then, as before, we used general population statistics to calculate the rate of heavy smokers per 100,000 of the population.
Heavy alcohol use
Data on the prevalence of (heavy) alcohol use, was also taken from Statistics Netherlands. Similar to the smoking variable, rates of heavy alcohol use are based on estimates rather than observations. There is one further aspect of this variable that requires elaboration. As for smoking, the cut-off for what is considered ‘heavy’ alcohol use is based on government guidelines. Up to 2011, the guideline is the same for everyone, after that it was revised downward by half for women – accordingly this creates a jump in heavy alcohol use in 2012 among women. That is, for women, we applied a correction to ensure comparability over the whole time frame. Details on the correction we applied are available in the Appendix.
Adolescent pregnancies
The variable reflecting the rate of adolescent pregnancies was composed of two indicators, namely (1) births to adolescent women and (2) abortions among adolescent women, in a given year. Data on births to adolescent mothers were accessed from Statistics Netherlands, reflecting the total number of births to mothers under 20 years of age. Data on abortions among adolescents were extracted from the yearly report of the Health Inspectorate, the organisation that regulates national health care (https://toezichtdocumenten.igj.nl). For each year, these two variables were summed to create an index of adolescent pregnancies (ending in either birth or abortion).
Analytical procedure
As noted above, we apply a co-integration test to examine whether the trends in the different phenomena share structural similarities. Our analytical procedure followed Liu (2006) and is composed of two stages. First, we create differences scores for each pair of phenomena. To create the difference scores, we first log the rates of the individual phenomena so that the different rates of the phenomena are transformed to more comparable scales. We then create difference indices between each pair of adverse outcomes, by subtracting one from the other. In the second stage, we apply the unit root test or augmented Dickey Fuller test. A full description of unit root processes is beyond the scope of this paper (for further information see Patterson 2010) – the key issue is that the alternative hypothesis of the test is that the difference score is stationary, and does not change over time. Those interested in the model specifications can refer to the Appendix.
We use R to apply the test (https://www.r-project.org) using the function boot_sqt in the package boot.ur (Smeekes and Wilms 2020). The function boot_sqt automatically sets the lag length to the minimum length required to eliminate auto-correlation from each series’ residuals. The advantage of this function over other similar functions offered in R is that it allows testing multiple time series at once, and corrects for the inflated type error I associated with multiple testing. Here we test for the co-integration between six phenomena, generating 15 tests in total (see Table 1 below). The multiple testing correction we apply results in a fairly conservative test. We consider this appropriate for the current study given the fact that we could include only a relatively short timeframe. As outlined above, including fewer observations makes for a less robust analysis, which we counterbalance in part by applying a more conservative procedure at the testing stage.
Results
Descriptive analysis
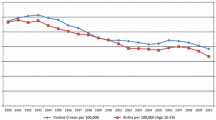
The trends in the individual phenomena are represented visually in Fig. 1. In general, all phenomena decline over time, and in 2020 reach roughly 50% of their 2000 rates. The exception to this is suicide – which in 2020 has increased a little compared to 2000. More specifically, we see that suicide first declines along with the other phenomena, but from 2007 onwards starts to rise again, while the other phenomena continue to decline.

Trends in rates of homicide, suicide, child mortality, heavy smoking, heavy alcohol use and adolescent pregnancies between 2000 and 2020
In sum, for each of the individual phenomena (aside from suicide) there is evidence for a decline over time. We now examine whether these declines arise independently of one another or as a result of structural similarities.
Co-integration
The results of the unit root tests are shown in Table 1. There was evidence of co-integration between trends in homicide and adolescent pregnancies, t(24) = –5.40, p = .003. That is, hypothesis H1a was supported: between the years 2000 and 2020, the decline in the homicide rate is linked to the decline in the rate of adolescent pregnancies. There was no evidence for co-integration of homicide trends with trends in alcohol use, smoking behaviour, child mortality or suicide. The hypotheses for child mortality (H1d) and suicide (H1e) had postulated the absence of co-integration, and as such, these hypotheses are also supported.
Having established the evidence for co-integration between homicide and each of the other phenomena, we now turn to the relationships among the other phenomena, disregarding homicide for a moment. The lower half of Table 1 provides an overview of the findings. As can be seen in the table – there was some evidence for co-integration between adolescent pregnancies and heavy alcohol use, but this evidence was not strong enough to lead to a rejection of the null hypothesis when correcting for multiple testing.
Discussion
In this project we examine how trends in homicide overlap with trends in adverse health outcomes such as suicide, child mortality, adolescent pregnancy, smoking behaviour and alcohol use. Visual inspection of the trends (in Fig. 1) showed that all these phenomena – with the exception of suicide – now occur less frequently than before, by 2020 they had declined to approximately 50% of their 2000 rate. More importantly, results of the co-integration test indicate that the trend in homicide rates was co-integrated with the trend in adolescent pregnancies – that is, rates of homicide and adolescent pregnancy ‘move together’ over time, indicating that there are structural similarities between the homicide trend and the trend in adolescent pregnancies.
When interpreting this finding, we might consider lifestyle theories (Hindelang et al. 1978). Aebi and Linde (2014) describe homicide trends across 15 European countries between 1960 and 2010 and suggest that trends in homicide rates reflect lifestyle changes in the population. Applying this perspective to the current findings we might consider lifestyle changes that have occurred since 2000 that may similarly affect homicide and adolescent pregnancies, but not the other phenomena under study. The rise of social media and the internet seems to be an obvious candidate, which may have reduced time spent in live interpersonal interaction (e.g. Winstone et al. 2021), thereby reducing specifically those phenomena that require a physical interpersonal component (pregnancy; homicide) but not the non-interpersonal outcomes (suicide; heavy alcohol use; heavy smoking; child mortality). In this way, the current findings can help us ‘disentangle’ clusters of adverse health outcomes in such a way that possible explanatory mechanisms come into clearer focus.
Contributions & limitations
The limitations associated with this study include several methodological issues surrounding data availability and quality. First, rates of homicide and child mortality are quite low. This affects the stability of the trends over time – time trends based on low counts can sometimes behave erratically as small fluctuations in the number of observations represent large percentage differences. Further, as discussed above, we study a relatively short timeframe of 21 years. As such, these findings certainly do not represent the final word on this topic.
Instead we suggest the contribution of this work lies in two key points: First, in unpacking clusters of adverse health outcomes in a way that offers insight into the societal factors that contribute to these clusters. Second, in applying a formalised test to the patterns observed. Note that many of the phenomena seemed to show similar time trends upon visual inspection (in Fig. 1). However, the more formal analysis forces us to temper that assessment. The trends observed there seem to arise (relatively) independently of one another, even if they look similar. Finally, this work has relevant implications for policy. By showing that empirical findings in criminology and public health may implicate similar factors, we stand a better chance of creating effective social policies, and thereby contribute to a safer and healthier society.
Conclusion
Homicide rates in Western Europe have declined in recent years (Suonpää et al. 2022). Interestingly, a similar decline is evident in a number of other adverse health phenomena, such as child mortality, adolescent pregnancies, smoking behaviour and heavy alcohol use. Here, we analysed whether these similar trends arise independently, or whether there is evidence for structural similarities between them. Results indicated similarities between rates of homicide and adolescent pregnancies in particular – the rates of these phenomena ‘move together’ during the period under study, suggesting that these two phenomena are responding similarly to a changing societal landscape. This work, then, furthers our understanding of the place of homicide in the domain of (public) health. Moreover, this work has implications for policy. By showing that empirical findings in criminology and public health may implicate similar factors, we stand a better chance of creating effective social policy.
Data availability
The data and materials associated with this project will be available through the Open Science Framework at https://osf.io/7dgpz/
Code availability
The code associated with this project will be available through the Open Science Framework at https://osf.io/7dgpz/
References
Aebi MF, Linde A (2014) The persistence of lifestyles: Rates and correlates of homicide in Western Europe from 1960 to 2010. Eur J Criminol 11(5):552–577. https://doi.org/10.1177/1477370814541178
Chen A, Oster E, Williams H (2016) Why is infant mortality higher in the United States than in Europe? Am Econ J: Econ Policy 8(2):89–124. https://doi.org/10.1257/pol.20140224
Cook J, Cook S (2011) Are US crime rates really unit root processes? J Quant Criminol 27(3):299–314. https://doi.org/10.1007/s10940-010-9124-4
Eisner M (2003) Long-term historical trends in violent crime. Crime Justice 30:83–142. https://doi.org/10.1086/652229
Gilbert L (1996) Urban violence and health—South Africa 1995. Soc Sci Med 43(5):873–886. https://doi.org/10.1016/0277-9536(96)00131-1
Gottfredson M, Hirschi T (1990) A general theory of crime. California, United States, Standford University Press, Stanford, Stanford
Hindelang MJ, Gottfredson MR, Garofalo J (1978) Victims of personal crime: An empirical foundation for a theory of personal victimization. Ballinger Cambridge, MA
Liu J (2006) Modernization and crime patterns in China. J Crim Justice 34(2):119–130. https://doi.org/10.1016/j.jcrimjus.2006.01.009
Mark ND, Torrats-Espinosa G (2022) Declining violence and improving birth outcomes in the US: evidence from birth certificate data. Soc Sci Med 294:114595. https://doi.org/10.1016/j.socscimed.2021.114595
Murray J, de Castro Cerqueira DR, Kahn T (2013) Crime and violence in Brazil: systematic review of time trends, prevalence rates and risk factors. Aggress Violent Behav 18(5):471–483. https://doi.org/10.1016/j.avb.2013.07.003
Ousey GC (2017) Crime is not the only problem: examining why violence and adverse health outcomes co-vary across large US counties. J Crim Justice 50:29–41. https://doi.org/10.1016/j.jcrimjus.2017.03.003
Patterson K (2010) A primer for unit root testing. PallGrave MacMillan, Basingstoke. https://doi.org/10.1057/9780230248458
Pickett KE, Mookherjee J, Wilkinson RG (2005) Adolescent birth rates, total homicides, and income inequality in rich countries. Am J Public Health 95(7):1181–1183. https://doi.org/10.2105/AJPH.2004.056721
Ritter K, Stompe T (2013) Unemployment, suicide-and homicide-rates in the EU countries. Neuropsychiat: Klin Diagnost Therap Rehabilitat 27(3):111–118
Shafti M, Steeg S, de Beurs D et al (2022) The inter-connections between self-harm and aggressive behaviours: a general network analysis study of dual harm. Front Psychiatry 13:1570. https://doi.org/10.3389/fpsyt.2022.953764
Smeekes S, Wilms I (2020) bootUR: Bootstrap Unit Root Tests. https://cris.maastrichtuniversity.nl/en/publications/bootur-bootstrap-unit-root-tests. Accessed 12 Apr 2023
Suonpää K, Kivivuori J, Aarten P et al (2022) Homicide drop in seven European countries: General or specific across countries and crime types?. Eur J Criminol (online first):1-28. https://doi.org/10.1177/14773708221103799
Unnithan NP, Huff-Corzine L, Corzine J, Whitt HP (1994) The currents of lethal violence: an integrated model of suicide and homicide. SUNY Press, San Diego
van Breen JA, Liem M (2022) Clustering of homicide with other adverse health outcomes in the Netherlands. Prev Med Rep 30(101988)
van Nieuwenhuijzen M, Junger M, Velderman MK et al (2009) Clustering of health-compromising behavior and delinquency in adolescents and adults in the Dutch population. Prev Med 48(6):572–578
Wilson WJ (1987) The truly disadvantaged: the inner city, the underclass, and public policy. University of Chicago Press, Chicago
Winstone L, Mars B, Haworth C, Kidger J (2021) Social media use and social connectedness among adolescents in the United Kingdom: a qualitative exploration of displacement and stimulation. BMC Public Health 21(1):1–15. https://doi.org/10.1186/s12889-021-11802-9
Acknowledgement
We would like to thank prof. Gary LaFree for helpful comments on an earlier draft of this manuscript.
Funding
This research was supported by the Social Resilience and Security Interdisciplinary programme at Leiden University
Author information
Authors and Affiliations
Contributions
JB and ML developed the project. ML secured funding for the project. JB gathered the data, conducted the analysis, and wrote the first manuscript draft. ML gave feedback.
Corresponding author
Ethics declarations
Ethics approval
The work reported in this manuscript was approved by the institutional ethics board at Leiden University.
Consent to participate
Not applicable
Consent for publication
Not applicable
Conflicts of Interest
The authors declare that they have no conflicts of interest relating to the work reported in this manuscript
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
van Breen, J., Liem, M. When it rains it pours? A time-series approach to the relationship between homicide and other adverse health phenomena. J Public Health (Berl.) (2023). https://doi.org/10.1007/s10389-023-01929-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10389-023-01929-x